
Association of Muscle Mass, Muscle Strength, and Muscle Function with Gait Ability Assessed Using Inertial Measurement Unit Sensors in Older Women






Abstract
1. Introduction
2. Materials and Methods
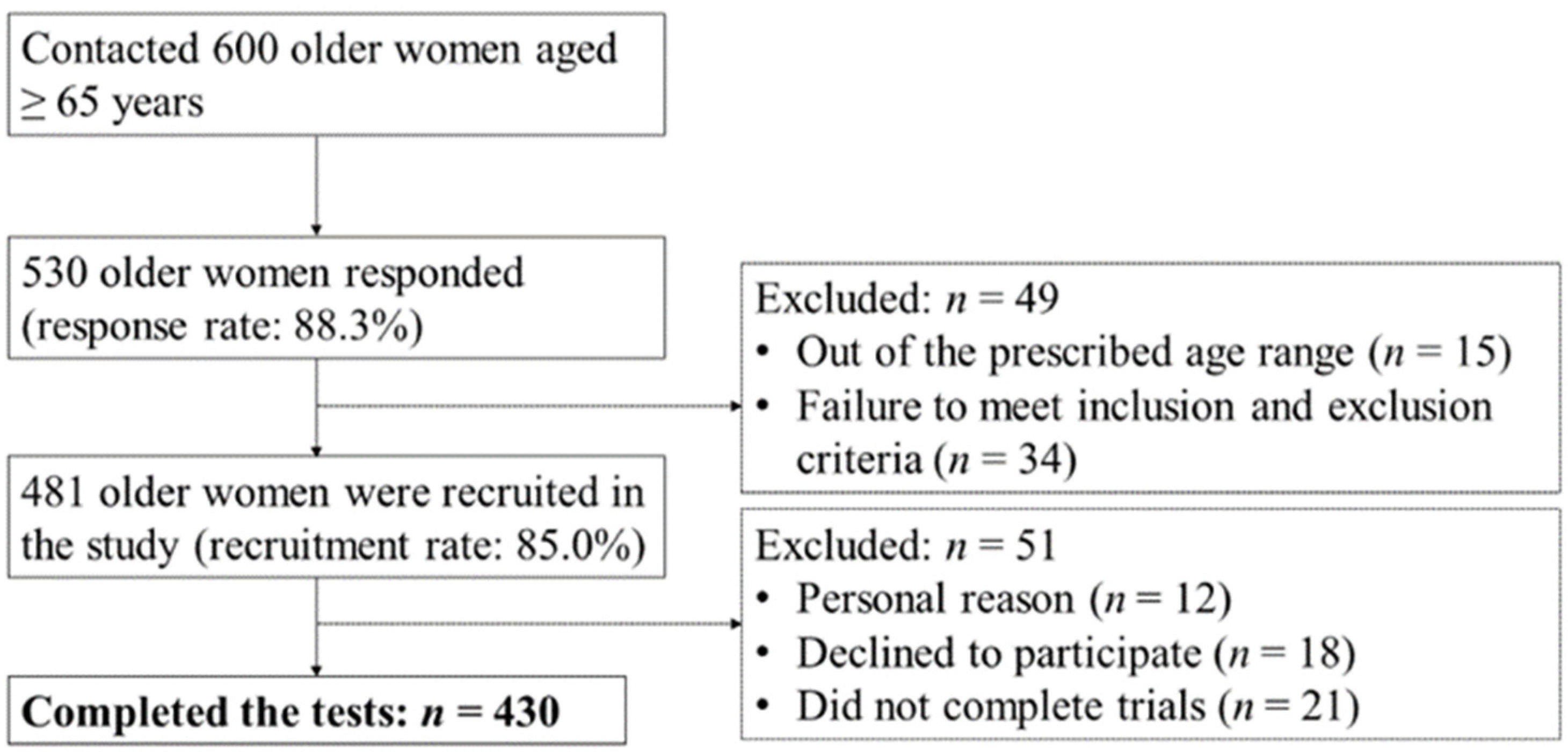
2.1. Participants
2.2. Assessment of MM, MS, and MF
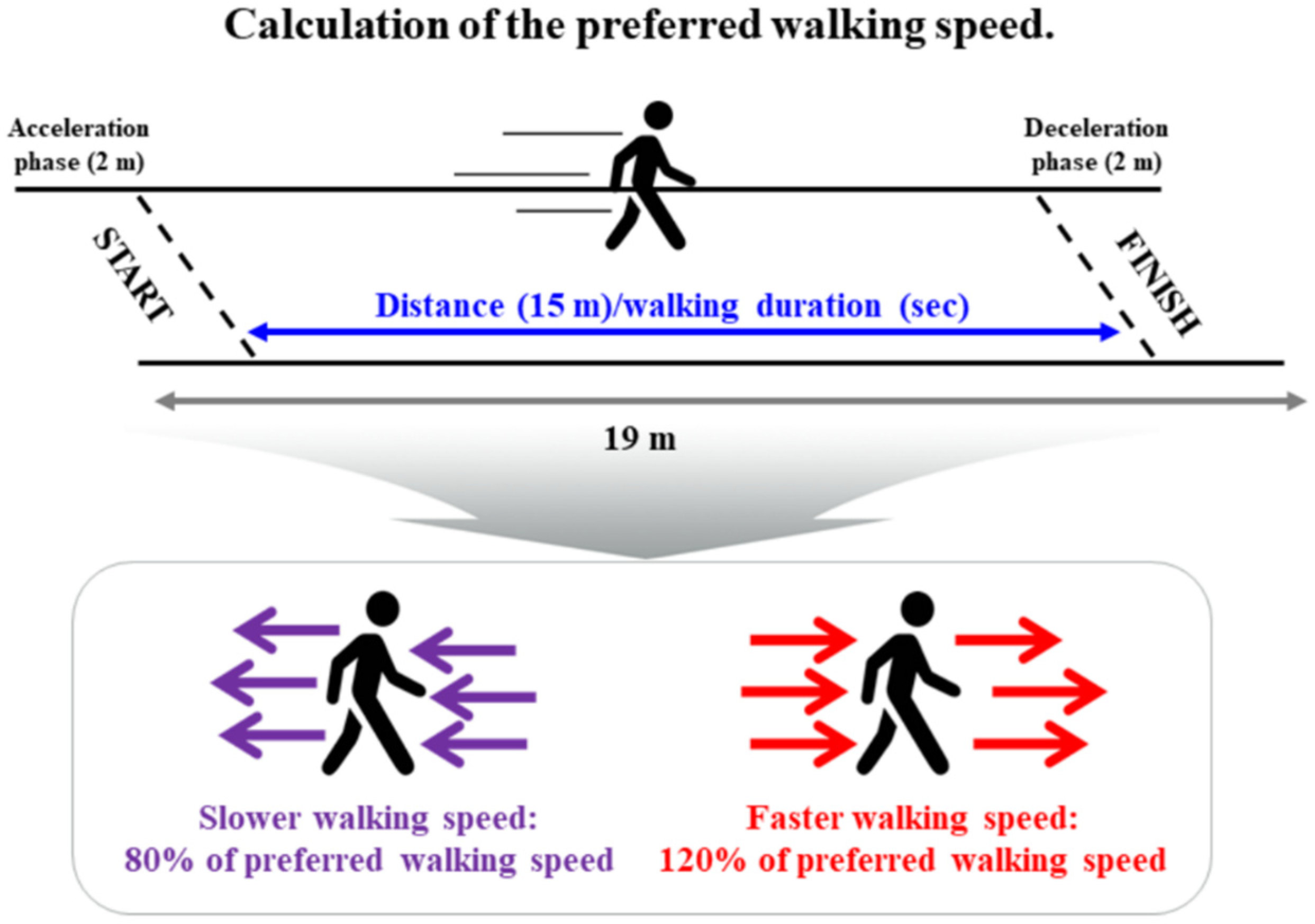
2.3. Assessment of Gait Performance
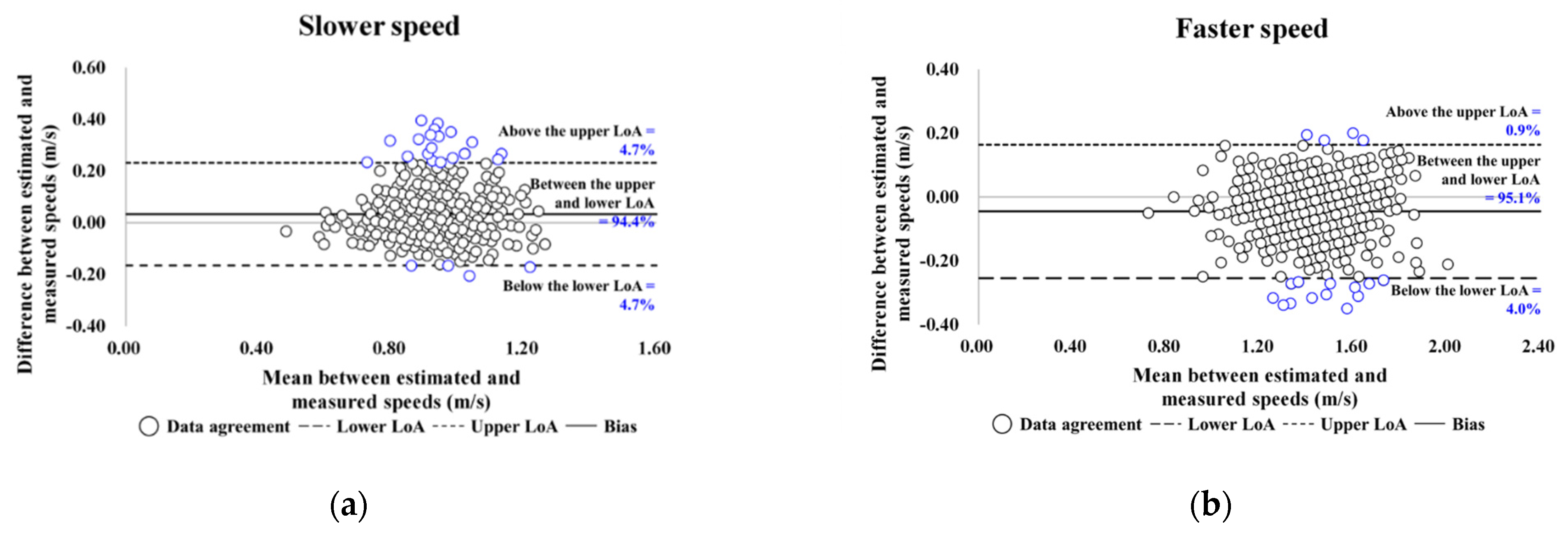
2.4. Instrumentation
2.5. Data Analysis and Statistical Analysis
3. Results
3.1. Participant Demographic, MM-, MS-, and MF-Related, and Gait Variables
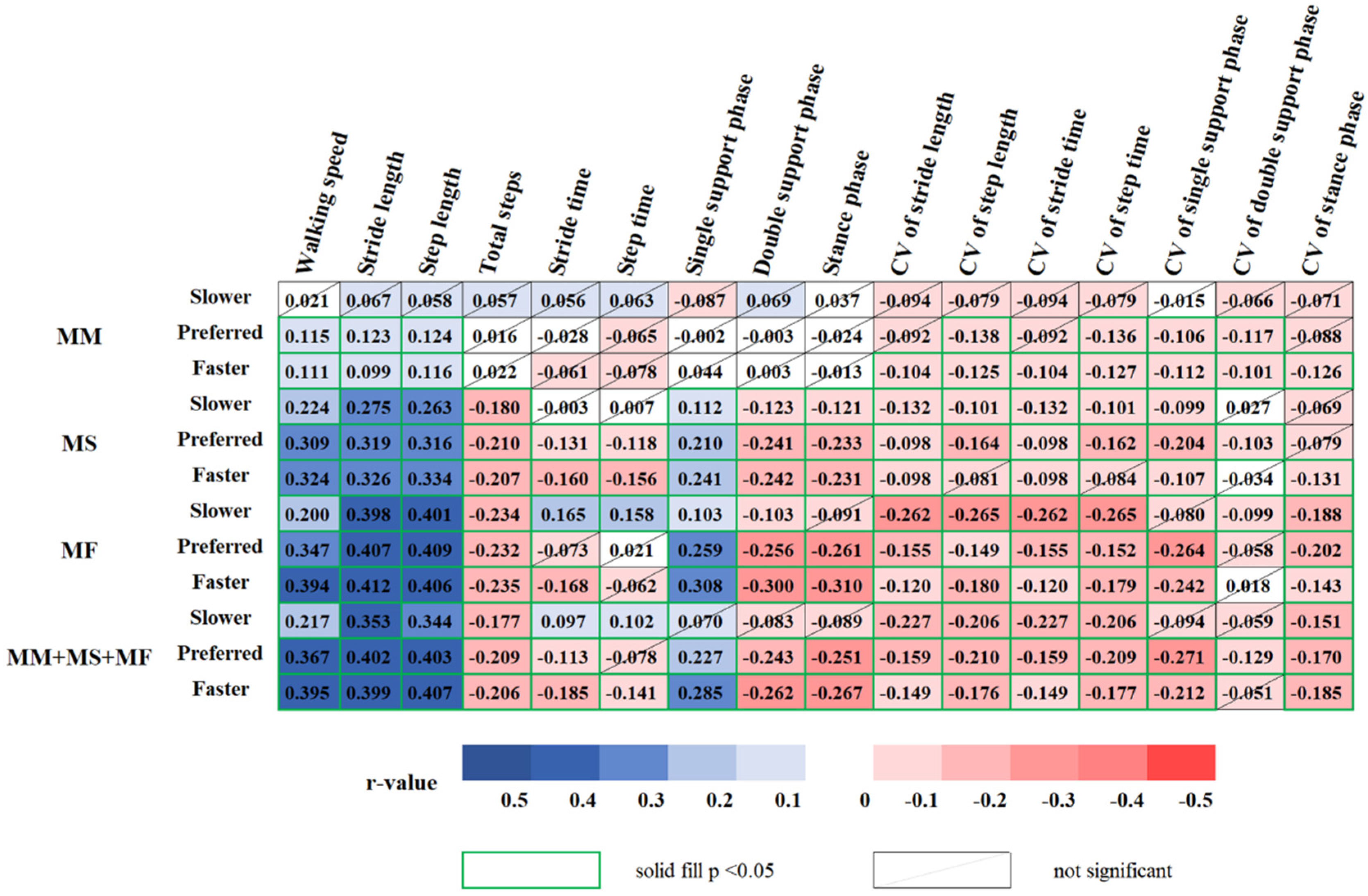
3.2. Relationship between Gait with MM-, MS-, and MF-Related Variables
3.3. Association of Gait with MM-, MS-, and MF-Related Variables
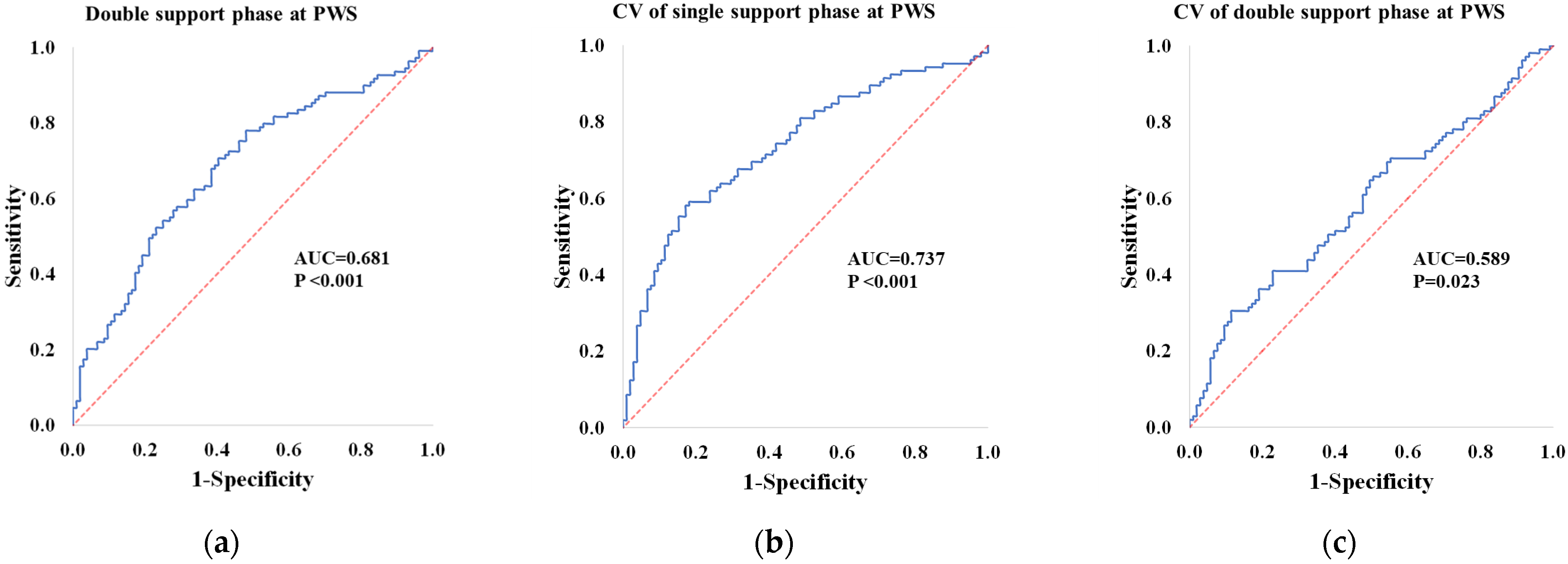
3.4. Classifier Variables for the Low and High Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Larsson, L.; Degens, H.; Li, M.; Salviati, L.; Lee, Y.I.; Thompson, W.; Kirkland, J.L.; Sandri, M. Sarcopenia: Aging-related loss of muscle mass and function. Physiol. Rev. 2019, 99, 427–511. [Google Scholar] [CrossRef] [PubMed]
- Martinikorena, I.; Martínez-Ramírez, A.; Gómez, M.; Lecumberri, P.; Casas-Herrero, A.; Cadore, E.L.; Millor, N.; Zambom-Ferraresi, F.; Idoate, F.; Izquierdo, M. Gait variability related to muscle quality and muscle power output in frail nonagenarian older adults. J. Am. Med. Dir. Assoc. 2016, 17, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Yeung, S.S.Y.; Reijnierse, E.M.; Pham, V.K.; Trappenburg, M.C.; Lim, W.K.; Meskers, C.G.M.; Maier, A.B. Sarcopenia and its association with falls and fractures in older adults: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2019, 10, 485–500. [Google Scholar] [CrossRef] [PubMed]
- Schwenk, M.; Howe, C.; Saleh, A.; Mohler, J.; Grewal, G.; Armstrong, D.; Najafi, B. Frailty and technology: A systematic review of gait analysis in those with frailty. Gerontology 2014, 60, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Perez-Sousa, M.A.; Venegas-Sanabria, L.C.; Chavarro-Carvajal, D.A.; Cano-Gutierrez, C.A.; Izquierdo, M.; Correa-Bautista, J.E.; Ramírez-Vélez, R. Gait speed as a mediator of the effect of sarcopenia on dependency in activities of daily living. J. Cachexia Sarcopenia Muscle 2019, 10, 1009–1015. [Google Scholar] [CrossRef]
- Kim, J.K.; Bae, M.N.; Lee, K.B.; Hong, S.G. Identification of patients with sarcopenia using gait parameters based on inertial sensors. Sensors 2021, 21, 1786. [Google Scholar] [CrossRef] [PubMed]
- Lord, S.; Galna, B.; Rochester, L. Moving forward on gait measurement: Toward a more refined approach. Mov. Disord. 2013, 28, 1534–1543. [Google Scholar] [CrossRef]
- Noh, B.; Youm, C.; Goh, E.; Lee, M.; Park, H.; Jeon, H.; Kim, O.Y. XGBoost based machine learning approach to predict the risk of fall in older adults using gait outcomes. Sci. Rep. 2021, 11, 12183. [Google Scholar] [CrossRef]
- Jabbar, K.A.; Seah, W.T.; Lau, L.K.; Pang, B.W.; Ng, D.H.; Tan, Q.L.; Chen, K.K.; Ullal, J.M.; Ng, T.-P.; Wee, S.-L. Fast gait spatiotemporal parameters in adults and association with muscle strength—The Yishun study. Gait Posture 2021, 85, 217–223. [Google Scholar] [CrossRef]
- Shin, S.; Valentine, R.J.; Evans, E.M.; Sosnoff, J.J. Lower extremity muscle quality and gait variability in older adults. Age Ageing 2012, 41, 595–599. [Google Scholar] [CrossRef]
- Galna, B.; Lord, S.; Rochester, L. Is gait variability reliable in older adults and Parkinson’s disease? Towards an optimal testing protocol. Gait Posture 2013, 37, 580–585. [Google Scholar] [CrossRef]
- Rennie, L.; Löfgren, N.; Moe-Nilssen, R.; Opheim, A.; Dietrichs, E.; Franzén, E. The reliability of gait variability measures for individuals with Parkinson’s disease and healthy older adults—The effect of gait speed. Gait Posture 2018, 62, 505–509. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Youm, C.; Jeon, J.; Cheon, S.M.; Park, H. Validity of shoe-type inertial measurement units for Parkinson’s disease patients during treadmill walking. J. NeuroEngineering Rehabil. 2018, 15, 38. [Google Scholar] [CrossRef] [PubMed]
- Bravi, M.; Gallotta, E.; Morrone, M.; Maselli, M.; Santacaterina, F.; Toglia, R.; Foti, C.; Sterzi, S.; Bressi, F.; Miccinilli, S. Concurrent validity and inter trial reliability of a single inertial measurement unit for spatial-temporal gait parameter analysis in patients with recent total hip or total knee arthroplasty. Gait Posture 2020, 76, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Almarwani, M.; VanSwearingen, J.M.; Perera, S.; Sparto, P.J.; Brach, J.S. Challenging the motor control of walking: Gait variability during slower and faster pace walking conditions in younger and older adults. Arch. Gerontol. Geriatr. 2016, 66, 54–61. [Google Scholar] [CrossRef]
- Ko, S.U.; Hausdorff, J.M.; Ferrucci, L. Age-associated differences in the gait pattern changes of older adults during fast-speed and fatigue conditions: Results from the Baltimore longitudinal study of ageing. Age Ageing 2010, 39, 688–694. [Google Scholar] [CrossRef]
- Yoshiko, A.; Ogawa, M.; Shimizu, K.; Radaelli, R.; Neske, R.; Maeda, H.; Maeda, K.; Teodoro, J.; Tanaka, N.; Pinto, R.S.; et al. Chair sit-to-stand performance is associated with diagnostic features of sarcopenia in older men and women. Arch. Gerontol. Geriatr. 2021, 96, 104463. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Noh, B.; Youm, C.; Lee, M.; Park, H. Associating gait phase and physical fitness with global cognitive function in the aged. Int. J. Environ. Res. Public Health 2020, 17, 4786. [Google Scholar] [CrossRef]
- Lord, S.; Galna, B.; Verghese, J.; Coleman, S.; Burn, D.; Rochester, L. Independent domains of gait in older adults and associated motor and nonmotor attributes: Validation of a factor analysis approach. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 820–827. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef]
- Maltais, M.L.; Desroches, J.; Dionne, I.J. Changes in muscle mass and strength after menopause. J. Musculoskelet Neuronal Interact. 2009, 9, 186–197. [Google Scholar]
- Visser, M.; Goodpaster, B.H.; Kritchevsky, S.B.; Newman, A.B.; Nevitt, M.; Rubin, S.M.; Simonsick, E.M.; Harris, T.B. Muscle mass, muscle strength, and muscle fat infiltration as predictors of incident mobility limitations in well-functioning older persons. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 324–333. [Google Scholar] [CrossRef]
- Aboutorabi, A.; Arazpour, M.; Bahramizadeh, M.; Hutchins, S.W.; Fadayevatan, R. The effect of aging on gait parameters in able-bodied older subjects: A literature review. Aging Clin. Exp. Res. 2016, 28, 393–405. [Google Scholar] [CrossRef]
- Knaggs, J.D.; Larkin, K.A.; Manini, T.M. Metabolic cost of daily activities and effect of mobility impairment in older adults. J. Am. Geriatr. Soc. 2011, 59, 2118–2123. [Google Scholar] [CrossRef][Green Version]
- McGibbon, C.A.; Puniello, M.S.; Krebs, D.E. Mechanical energy transfer during gait in relation to strength impairment and pathology in elderly women. Clin. Biomech. 2001, 16, 324–333. [Google Scholar] [CrossRef]
- Schultz, A.B. Muscle function and mobility biomechanics in the elderly: An overview of some recent research. J. Gerontol. A Biol. Sci. Med. Sci. 1995, 50, 60–63. [Google Scholar]
- Winter, D.A. Biomechanics and Motor Control of Human Gait: Normal, Elderly and Pathological, 2nd ed.; University of Waterloo Press: Waterloo, ON, Canada, 1991. [Google Scholar]
- Den Otter, A.R.; Geurts, A.C.; Mulder, T.; Duysens, J. Speed related changes in muscle activity from normal to very slow walking speeds. Gait Posture 2004, 19, 270–278. [Google Scholar] [CrossRef]
- Neptune, R.R.; Sasaki, K.; Kautz, S.A. The effect of walking speed on muscle function and mechanical energetics. Gait Posture 2008, 28, 135–143. [Google Scholar] [CrossRef]
- Callisaya, M.L.; Blizzard, L.; McGinley, J.L.; Schmidt, M.D.; Srikanth, V.K. Sensorimotor factors affecting gait variability in older people—a population-based study. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 386–392. [Google Scholar] [CrossRef]
- Ju, S. Correlation between lower limb muscle asymmetry during the sit-to-stand task and spatiotemporal gait asymmetry in subjects with stroke. J. Exerc. Rehabil. 2020, 16, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Orendurff, M.S.; Segal, A.D.; Klute, G.K.; Berge, J.S.; Rohr, E.S.; Kadel, N.J. The effect of walking speed on center of mass displacement. J. Rehabil. Res. Dev. 2004, 41, 829–834. [Google Scholar] [CrossRef] [PubMed]
- Nascimbeni, A.; Minchillo, M.; Salatino, A.; Morabito, U.; Ricci, R. Gait attentional load at different walking speeds. Gait Posture 2015, 41, 304–306. [Google Scholar] [CrossRef] [PubMed]
- Hausdorff, J.M. Gait variability: Methods, modeling and meaning. J. NeuroEngineering Rehabil. 2005, 2, 19. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Rios, D.A.; Edelberg, H.K. Gait variability and fall risk in community-living older adults: A 1-year prospective study. Arch. Phys. Med. Rehabil. 2001, 82, 1050–1056. [Google Scholar] [CrossRef]
- Brach, J.S.; Studenski, S.; Perera, S.; VanSwearingen, J.M.; Newman, A.B. Stance time and step width variability have unique contributing impairments in older persons. Gait Posture 2008, 27, 431–439. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Cudkowicz, M.E.; Firtion, R.; Wei, J.Y.; Goldberger, A.L. Gait variability and basal ganglia disorders: Stride-to-stride variations of gait cycle timing in Parkinson’s disease and Huntington’s disease. Mov. Disord. 1998, 13, 428–437. [Google Scholar] [CrossRef]
- Hausdorff, J.M. Gait dynamics, fractals and falls: Finding meaning in the stride-to-stride fluctuations of human walking. Hum. Mov. Sci. 2007, 26, 555–589. [Google Scholar] [CrossRef]
- Montero-Odasso, M.; Muir, S.W.; Hall, M.; Doherty, T.J.; Kloseck, M.; Beauchet, O.; Speechley, M. Gait variability is associated with frailty in community-dwelling older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2011, 66, 568–576. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All Participants |
|---|---|
| Age (years) | 72.39 ± 4.94 |
| Height (cm) | 153.06 ± 5.30 |
| Body mass (kg) | 58.21 ± 8.34 |
| BMI (kg/m2) | 24.95 ± 3.12 |
| BFP (%) | 34.47 ± 5.69 |
| Skeletal muscle mass (kg) | 20.41 ± 2.55 |
| MM (kg/m2) | 8.69 ± 0.80 |
| MS (kg) | 22.02 ± 4.14 |
| MF (s) | 9.81 ± 3.47 |
| SWS | |
| Estimated/measured (m/s) | 0.94/0.90 |
| ICC (2,1) | 0.825 |
| p-value | <0.001 |
| FWS | |
| Estimated/measured (m/s) | 1.41/1.45 |
| ICC (2,1) | 1.000 |
| p-value | <0.001 |
| Variables | β (SE) | T | p-Value |
|---|---|---|---|
| MM | R2 = 0.345 | ||
| Stride length (preferred) | 0.098 (0.036) | 2.732 | 0.007 |
| MS | R2 = 0.265 | ||
| Walking speed (faster) | 0.112 (0.057) | 1.984 | 0.048 |
| CV of double support phase (preferred) | −0.120 (0.042) | –2.879 | 0.004 |
| Double support phase (preferred) | −0.136 (0.056) | −2.445 | 0.015 |
| MF | R2 = 0.300 | ||
| CV of step time (slower) | −0.183 (0.038) | −4.805 | <0.001 |
| Stride time (slower) | 0.258 (0.040) | 6.476 | <0.001 |
| Walking speed (faster) | 0.311 (0.044) | 7.118 | <0.001 |
| CV of single support phase (preferred) | −0.084 (0.040) | −2.122 | 0.034 |
| MM + MS + MF | R2 = 0.330 | ||
| Stride length (preferred) | 0.182 (0.061) | 2.973 | 0.003 |
| Double support phase (faster) | −0.203 (0.059) | −3.475 | 0.001 |
| CV of double support phase (preferred) | −0.122 (0.046) | −2.636 | 0.009 |
| Stride time (slower) | 0.117 (0.050) | 2.354 | 0.019 |
| CV of single support phase (preferred) | −0.105 (0.050) | −2.081 | 0.038 |
| Variables | β (SE) | OR (95% CI) | p-Value | RN2 | |
|---|---|---|---|---|---|
| MM | Stride length (preferred) | 0.639 (0.284) | 1.895 (1.086–3.306) | 0.024 | 0.705 |
| MS | Double support phase (preferred) | −0.563 (0.192) | 0.569 (0.391–0.830) | 0.003 | 0.426 |
| MF | Walking speed (faster) | 1.145 (0.222) | 3.144 (2.036–4.856) | <0.001 | 0.402 |
| Stride time (slower) | 0.783 (0.204) | 2.187 (1.466–3.263) | <0.001 | ||
| MM + MS + MF | Stride length (preferred) | 1.063 (0.283) | 2.896 (1.664–5.040) | <0.001 | 0.591 |
| CV of single support phase (preferred) | −0.514 (0.234) | 0.598 (0.378–0.947) | 0.028 | ||
| CV of double support phase (preferred) | −0.428 (0.202) | 0.652 (0.438–0.968) | 0.034 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, B.; Youm, C.; Park, H.; Lee, M.; Choi, H. Association of Muscle Mass, Muscle Strength, and Muscle Function with Gait Ability Assessed Using Inertial Measurement Unit Sensors in Older Women. Int. J. Environ. Res. Public Health 2022, 19, 9901. https://doi.org/10.3390/ijerph19169901
Kim B, Youm C, Park H, Lee M, Choi H. Association of Muscle Mass, Muscle Strength, and Muscle Function with Gait Ability Assessed Using Inertial Measurement Unit Sensors in Older Women. International Journal of Environmental Research and Public Health. 2022; 19(16):9901. https://doi.org/10.3390/ijerph19169901
Chicago/Turabian StyleKim, Bohyun, Changhong Youm, Hwayoung Park, Myeounggon Lee, and Hyejin Choi. 2022. "Association of Muscle Mass, Muscle Strength, and Muscle Function with Gait Ability Assessed Using Inertial Measurement Unit Sensors in Older Women" International Journal of Environmental Research and Public Health 19, no. 16: 9901. https://doi.org/10.3390/ijerph19169901
APA StyleKim, B., Youm, C., Park, H., Lee, M., & Choi, H. (2022). Association of Muscle Mass, Muscle Strength, and Muscle Function with Gait Ability Assessed Using Inertial Measurement Unit Sensors in Older Women. International Journal of Environmental Research and Public Health, 19(16), 9901. https://doi.org/10.3390/ijerph19169901