
Effect of a Short Course on Improving the Cadres’ Knowledge in the Context of Reducing Stunting through Home Visits in Yogyakarta, Indonesia

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Procedures
2.3. Participants
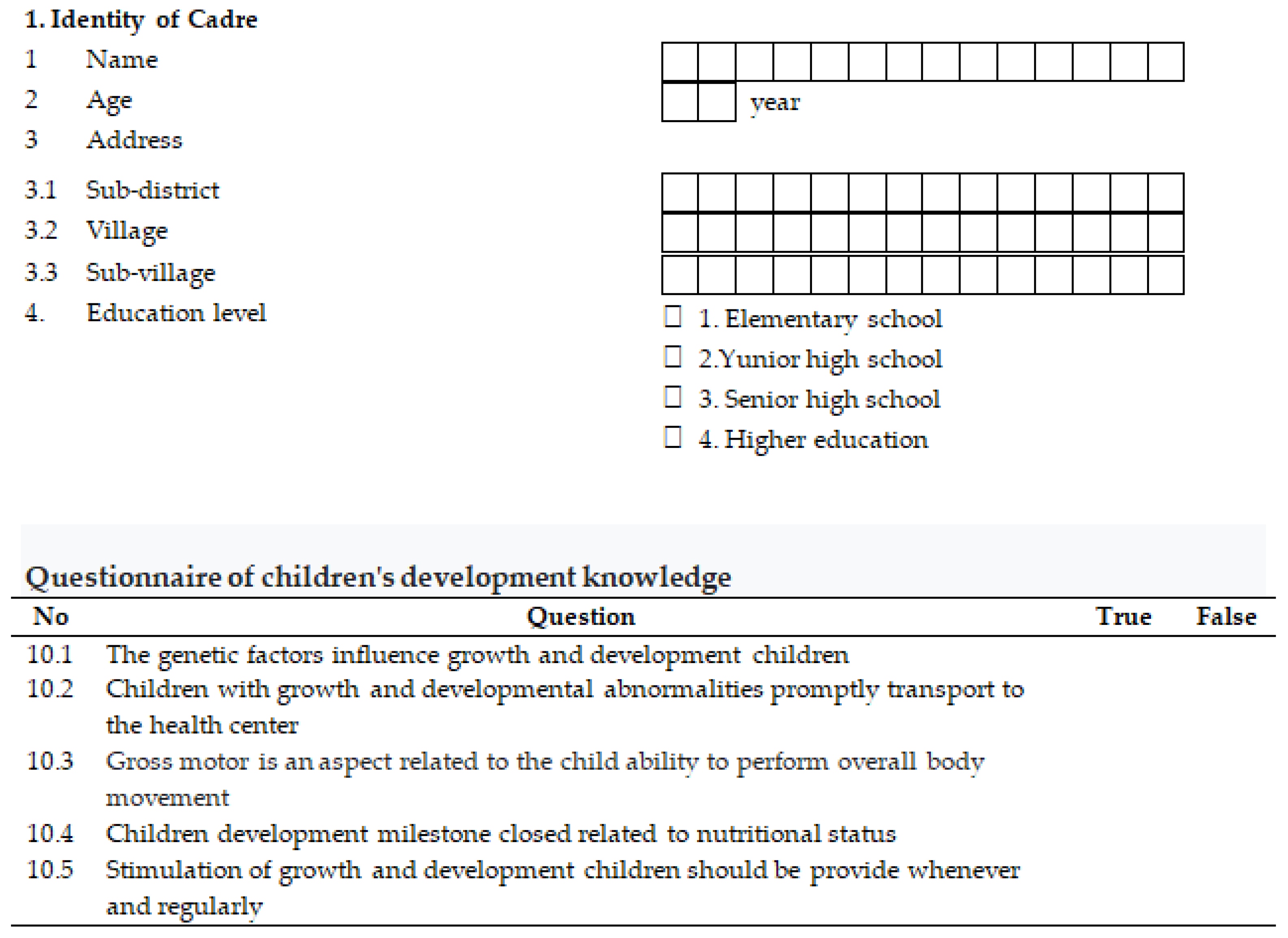
2.4. Data Collection
2.5. Data Management and Analysis
3. Results
3.1. Baseline Characteristics
3.2. Short Course
“We are pleased with this short course because the duration is sufficient, not too long, and allows us to schedule a home visit.”(SR, 31 years old)
“At first, we had to fix an appointment with the mother, but now it is more accessible through a cellphone. However, we are happy because home visits make us understand the condition of children and their families, hence, it won’t be intensive when we meet at the Integrated Health Service Post.”(TS, 45 years old)
“I’m becoming more courageous in assisting children. During the home visit, I recalled how we taught monitoring of children’s growth and development, IYCF, and the information was transferred to the mothers until she was understood.”(D, 42 years old)
4. Discussion
5. Limitation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Malnutrition. 2021. Available online: https://www.who.int/publications/i/item/WHO-NMH-NHD-14.3 (accessed on 7 April 2022).
- President Republic Indonesia. Presidential Regulation Nomor 18 Tahun 2020 Issue National Mid-Term Development Plan Year 2020–2024. 2020. Available online: https://peraturan.bpk.go.id/Home/Details/131386/perpres-no-18-tahun-2020 (accessed on 8 March 2022).
- WHO. Global Nutrition Targets 2025: Stunting Policy Brief. 2014. Available online: https://www.who.int/publications-detail-redirect/WHO-NMH-NHD-14.2 (accessed on 23 March 2022).
- Ministry of Health Republic Indonesia. Book of SSGI Study Results at the National, Provincial and Regency/City Levels in 2021; Ministry of Health Republic Indonesia: Jakarta, Indonesia, 2021.
- De Onis, M.; Borghi, E.; Arimond, M.; Webb, P.; Croft, T.; Saha, K.; De-Regil, L.M.; Thuita, F.; Heidkamp, R.; Krasevec, J.; et al. Prevalence thresholds for wasting, overweight and stunting in children under 5 years. Public Health Nutr. 2018, 22, 175–179. [Google Scholar] [CrossRef]
- Shiroya-Wandabwa, M.; Kabue, M.; Kasungami, D.; Wambua, J.; Otieno, D.; Waka, C.; Ngindu, A.; Ayuyo, C.; Kigondu, S.; Oliech, J.; et al. Coaching Community Health Volunteers in Integrated Community Case Management Improves the Care of Sick Children Under-5: Experience from Bondo, Kenya. Int. J. Integr. Care 2018, 18, 5. [Google Scholar] [CrossRef] [PubMed]
- Mediani, H.S.; Hendrawati, S.; Pahria, T.; Mediawati, A.S.; Suryani, M. Factors Affecting the Knowledge and Motivation of Health Cadres in Stunting Prevention Among Children in Indonesia. J. Multidiscip. Healthc. 2022, 15, 1069–1082. [Google Scholar] [CrossRef] [PubMed]
- Saprii, L.; Richards, E.; Kokho, P.; Theobald, S. Community health workers in rural India: Analysing the opportunities and challenges Accredited Social Health Activists (ASHAs) face in realising their multiple roles. Hum. Resour. Health 2015, 13, 95. [Google Scholar] [CrossRef] [PubMed]
- Wibowo, Y.; Setiadi, A.P.; Halim, S.V.; Saputra, R.D.; Oktavia, R.; Irianti, R.; Lestari, P.I.; Puspitasari, C.R.; Sunderland, B. A pilot study of cadre training to promote responsible self-medication in Indonesia: Which is better specific or general modules? Health Soc. Care Community 2020, 29, 554–563. [Google Scholar] [CrossRef]
- Rawal, L.B.; Mahmud, K.; Islam, S.M.S.; Mahumud, R.A.; Nuruzaman; Ahmed, S.M. Training mid-level health cadres to improve health service delivery in rural Bangladesh. Prim. Health Care Res. Dev. 2016, 17, 503–513. [Google Scholar] [CrossRef]
- Fitryasari, E.D.; Tristiana, R.; Windy, D.R.; Kurniasari, A. Keswacarri As An Effort To Increase Cadre Capability For Treating Mental Disorders Patients In The Modern Industrial Community 4.0. J. Pengabdi. Masy. Dalam Kesehat. 2022, 4, 25–30. [Google Scholar] [CrossRef]
- Effendy, D.S.; Prangthip, P.; Soonthornworasiri, N.; Winichagoon, P.; Kwanbunjan, K. Nutrition education in Southeast Sulawesi Province, Indonesia: A cluster randomized controlled study. Matern. Child Nutr. 2020, 16, e13030. [Google Scholar] [CrossRef]
- Elisaria, E.; Mrema, J.; Bogale, T.; Segafredo, G.; Festo, C. Effectiveness of integrated nutrition interventions on childhood stunting: A quasi-experimental evaluation design. BMC Nutr. 2021, 7, 17. [Google Scholar] [CrossRef]
- Titaley, C.R.; Dibley, M.J.; Ariawan, I.; Mu’Asyaroh, A.; Paramashanti, B.A.; Alam, A.; Damayanti, R.; Do, T.T.; Ferguson, E.; Htet, M.K.; et al. The impact of a package of behaviour change interventions on breastfeeding practices in East Java Province, Indonesia. Matern. Child Nutr. 2022, 18, e13362. [Google Scholar] [CrossRef]
- Dufour, R.; Beaudet, N.; Lecavalier, M. Accompaniment to improve public health professional practic. Sante Publique 2014, 26, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Paramashanti, B.A.; Sulistyawati, S. Pengaruh integrasi intervensi gizi dan stimulasi tumbuh kembang terhadap peningkatan berat badan dan perkembangan balita kurus. J. Gizi Klin. Indones. 2018, 15, 16–21. [Google Scholar] [CrossRef]
- President Republic Indonesia. Presidential Regulation No 72 Year 2021 Issue Stunting Reduction Acceleration. 2021. Available online: https://peraturan.bpk.go.id/Home/Details/174964/perpres-no-72-tahun-2021 (accessed on 1 February 2022).
- Prosnitz, D.; Herrera, S.; Coelho, H.; Davis, L.M.; Zalisk, K.; Yourkavitch, J. Evidence of Impact: ICCM as a strategy to save lives of children under five. J. Glob. Health 2019, 9, 010801. [Google Scholar] [CrossRef] [PubMed]
- WHO. Integrated Community Case Management. 2014. Available online: https://www.afro.who.int/news/integrated-community-case-management (accessed on 4 February 2022).
- Jones, G.; Steketee, R.W.; Black, R.E.; Bhutta, Z.A.; Morris, S.S.; Bellagio Child Survival Study Group. How many child deaths can we prevent this year? Lancet 2013, 362, 65–71. [Google Scholar] [CrossRef]
- Onono, M.; Abdi, M.; Opondo, I.; Okung’U, J.; Asadhi, E.; Nyamai, R.; Karimurio, L.; Okoth, P.; Qazi, S.A. Using the RE-AIM framework to evaluate the implementation of integrated community case management in Kenya. Acta Paediatr. 2018, 107, 53–62. [Google Scholar] [CrossRef]
- Ministry of Health Republic Indonesia. Guidance for Cadre of Integrated Health Service Post (Posyandu); Ministry of Health Republic Indonesia: Jakarta, Indonesia, 2019.
- Ministry of Village Development Republic Indonesia. Regulation No 7 Year 2021 Issue Prioritization of Village Fund Utilization in Indonesia. 2020. Available online: https://peraturan.bpk.go.id/Home/Details/199693/permendesa-pdtt-no-7-tahun-2021 (accessed on 2 February 2022).
- Ministry of State Secretariat Republic Indonesia. Program Pillars. 2021. Available online: https://stunting.go.id/en/program-pillars/pillar-3/ (accessed on 25 February 2022).
- Afifa, I. Kinerja Kader dalam Pencegahan Stunting: Peran Lama Kerja sebagai Kader, Pengetahuan dan Motivasi. J. Kedokt. Brawijaya 2019, 30, 336–341. [Google Scholar] [CrossRef]
- Rinawan, F.R.; Kusumastuti, P.; Mandiri, A.; Dewi, R.K. Association of Cadre’s Knowledge with Age, Duration of Work, Education, and Employment on the Use of iPosyandu Application in Pasawahan, Purwakarta. J. Ilmu Kesehat. Masy. 2020, 11, 150–159. [Google Scholar] [CrossRef]
- Bantul District Health Office. Posyandu Cadre Competency Examination. 2022. Available online: https://dinkes.bantulkab.go.id/news/uji-kompetensi-kader-posyandu#! (accessed on 30 June 2022).
- Tampake, R.; Arianty, R.; Mangundap, S.A.; Emy, B.; Sasmita, H. The Effectiveness of Training on Improving the Ability of Health Cadres in Early Detection of Stunting in Toddlers. Open Access Maced. J. Med Sci. 2021, 9, 373–377. [Google Scholar] [CrossRef]
- Ameh, C.A.; White, S.; Dickinson, F.; Mdegela, M.; Madaj, B.; Broek, N.V.D. Retention of knowledge and skills after Emergency Obstetric Care training: A multi-country longitudinal study. PLoS ONE 2018, 13, e0203606. [Google Scholar] [CrossRef]
- Cochrane, L.J.; Olson, C.A.; Murray, S.; Dupuis, M.; Tooman, T.; Hayes, S. Gaps between knowing and doing: Understanding and assessing the barriers to optimal health care. J. Contin. Educ. Health Prof. 2007, 27, 94–102. [Google Scholar] [CrossRef]
- Davis, B.; Summers, M. Applying Dale’s Cone of Experience to increase learning and retention: A study of student learning in a foundational leadership course. QScience Proc. 2015, 2015, 6. [Google Scholar] [CrossRef]
- Cho, M.-K.; Kim, M.Y. Factors Affecting Learning Satisfaction in Face-to-Face and Non-Face-to-Face Flipped Learning among Nursing Students. Int. J. Environ. Res. Public Health 2021, 18, 8641. [Google Scholar] [CrossRef] [PubMed]
- Ransom, A.; LaGrant, B.; Spiteri, A.; Kushnir, T.; Anderson, A.K.; De Rosa, E. Face-to-face learning enhances the social transmission of information. PLoS ONE 2022, 17, e0264250. [Google Scholar] [CrossRef] [PubMed]
- Bessadok, A. Analyzing student aspirations factors affecting e-learning system success using a structural equation model. Educ. Inf. Technol. 2022. [Google Scholar] [CrossRef]
- Baeten, M.; Dochy, F.; Struyven, K. The effects of different learning environments on students’ motivation for learning and their achievement. Br. J. Educ. Psychol. 2012, 83, 484–501. [Google Scholar] [CrossRef]
- Indra, J.; Khoirunurrofik, K. Understanding the role of village fund and administrative capacity in stunting reduction: Empirical evidence from Indonesia. PLoS ONE 2022, 17, e0262743. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variables | n | % |
|---|---|---|
| Age (years old) | ||
| <30 | 6 | 7.0 |
| 30–40 | 12 | 40.0 |
| >40 | 18 | 53.0 |
| Marital Status | ||
| Married | 30 | 100.0 |
| Formal Education | ||
| Junior High School | 9 | 30.0 |
| Senior High School | 19 | 63.3 |
| University | 2 | 6.7 |
| Occupation | ||
| Farmer | 8 | 26.7 |
| Self-employed | 4 | 13.3 |
| Housewife | 18 | 60.0 |
| Years of role as cadres (years) | ||
| <5 | 7 | 23.3 |
| 6–10 | 5 | 16.7 |
| >10 | 18 | 60.0 |
| History of training | ||
| IYCF | 30 | 100.0 |
| Growth monitoring | 30 | 100.0 |
| Cadre competency certification | 30 | 100.0 |
| Take a short course completely | 30 | 100.0 |
| Variables | CGM | CDM | IYCF | Average |
|---|---|---|---|---|
| Pretest | 71.50 ± 1.41 | 70.87 ± 1.96 | 71.33 ± 1.32 | 71.23 ± 0.75 |
| Post-test 1 | 77.57 ± 2.34 | 77.57 ± 1.96 | 77.17 ± 2.81 | 77.43 ± 1.29 |
| Post-test 2 | 80.07 ± 2.02 | 80.13 ± 2.16 | 83.03 ± 3.51 | 81.08 ± 1.72 |
| Post-test 1—Pretest Effect size 95%CI | 6.07 * (5.09–7.04) | 6.70 * (5.67–7.73) | 5.83 * (4.44–7.22) | 6.20 * (5.68–6.72) |
| Post-test 2—Pretest Effect size 95% CI | 8.57 * (7.58–9.56) | 9.27 * (8.28–10.25) | 11.7 * (10.55–12.85) | 9.84 * (9.16–10.53) |
| Variable 2 | CGM 1 | CDM 1 | IYCF 1 | Average 1 |
|---|---|---|---|---|
| Post-test 2 | 8.57 * (7.60–9.53) | 9.27 * (8.31–10.22) | 11.7 * (10.31–13.09) | 9.84 * (9.17–10.52) |
| Post-test 1 | 6.07 * (5.10–7.03) | 6.70 * (5.75–7.65) | 5.83 * (4.44–7.23) | 6.20 * (5.52–6.88) |
| Pretest | Ref | Ref | Ref | Ref |
| Cons | 71.71 | 73.47 | 69.41 | 71.53 |
| QIC | 373.938 | 428.937 | 601.954 | 179.888 |
| Aspect | Opinion |
|---|---|
| Affective attitude | Cadres felt excited and were more intensive in assisting stunted children. They can educate mothers more comprehensively. |
| Burden | Mothers denied their children were stunted, even asking for measurements on the spot. However, after explaining the program’s benefits, they wanted to be educated. Another burden issue is time mismatch and time-consumption, because it takes 30–60 min for each child’s home visit. |
| Ethics | Short courses and home visits do not conflict with existing norms, programs, culture, and beliefs, even if mothers and cadres give each other a strengthening of returns to reduce the problem of stunted children. |
| Perception of effectiveness | This program is beneficial because home visits educate mothers regarding growth monitoring, how to stimulate development, measuring developmental achievements, and appropriate feeding of children. Furthermore, the program support further decreases the prevalence of stunting. |
| Intervention coherence | Cadres understand the program flow. |
| Opportunity cost | The home visit program has implications for time, travelling cost, and other resources, along with food ingredients and BKB kits (Indonesian: acronym for Bina Keluarga Balita, or Toddler Family Development) as educational media. |
| Self-efficacy | Training makes cadres confident; hence, they can solve stunting problems through home visits. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siswati, T.; Iskandar, S.; Pramestuti, N.; Raharjo, J.; Rialihanto, M.P.; Rubaya, A.K.; Wiratama, B.S. Effect of a Short Course on Improving the Cadres’ Knowledge in the Context of Reducing Stunting through Home Visits in Yogyakarta, Indonesia. Int. J. Environ. Res. Public Health 2022, 19, 9843. https://doi.org/10.3390/ijerph19169843
Siswati T, Iskandar S, Pramestuti N, Raharjo J, Rialihanto MP, Rubaya AK, Wiratama BS. Effect of a Short Course on Improving the Cadres’ Knowledge in the Context of Reducing Stunting through Home Visits in Yogyakarta, Indonesia. International Journal of Environmental Research and Public Health. 2022; 19(16):9843. https://doi.org/10.3390/ijerph19169843
Chicago/Turabian StyleSiswati, Tri, Slamet Iskandar, Nova Pramestuti, Jarohman Raharjo, Muhammad Primiaji Rialihanto, Agus Kharmayana Rubaya, and Bayu Satria Wiratama. 2022. "Effect of a Short Course on Improving the Cadres’ Knowledge in the Context of Reducing Stunting through Home Visits in Yogyakarta, Indonesia" International Journal of Environmental Research and Public Health 19, no. 16: 9843. https://doi.org/10.3390/ijerph19169843
APA StyleSiswati, T., Iskandar, S., Pramestuti, N., Raharjo, J., Rialihanto, M. P., Rubaya, A. K., & Wiratama, B. S. (2022). Effect of a Short Course on Improving the Cadres’ Knowledge in the Context of Reducing Stunting through Home Visits in Yogyakarta, Indonesia. International Journal of Environmental Research and Public Health, 19(16), 9843. https://doi.org/10.3390/ijerph19169843