
The Illness Experience of Long COVID Patients: A Qualitative Study Based on the Online Q&A Community Zhihu


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Collection
2.2. Data Source and Collection—Data Analysis
2.2.1. Open Coding
2.2.2. Axial Coding and Selective Coding
2.2.3. Coding Saturation Test
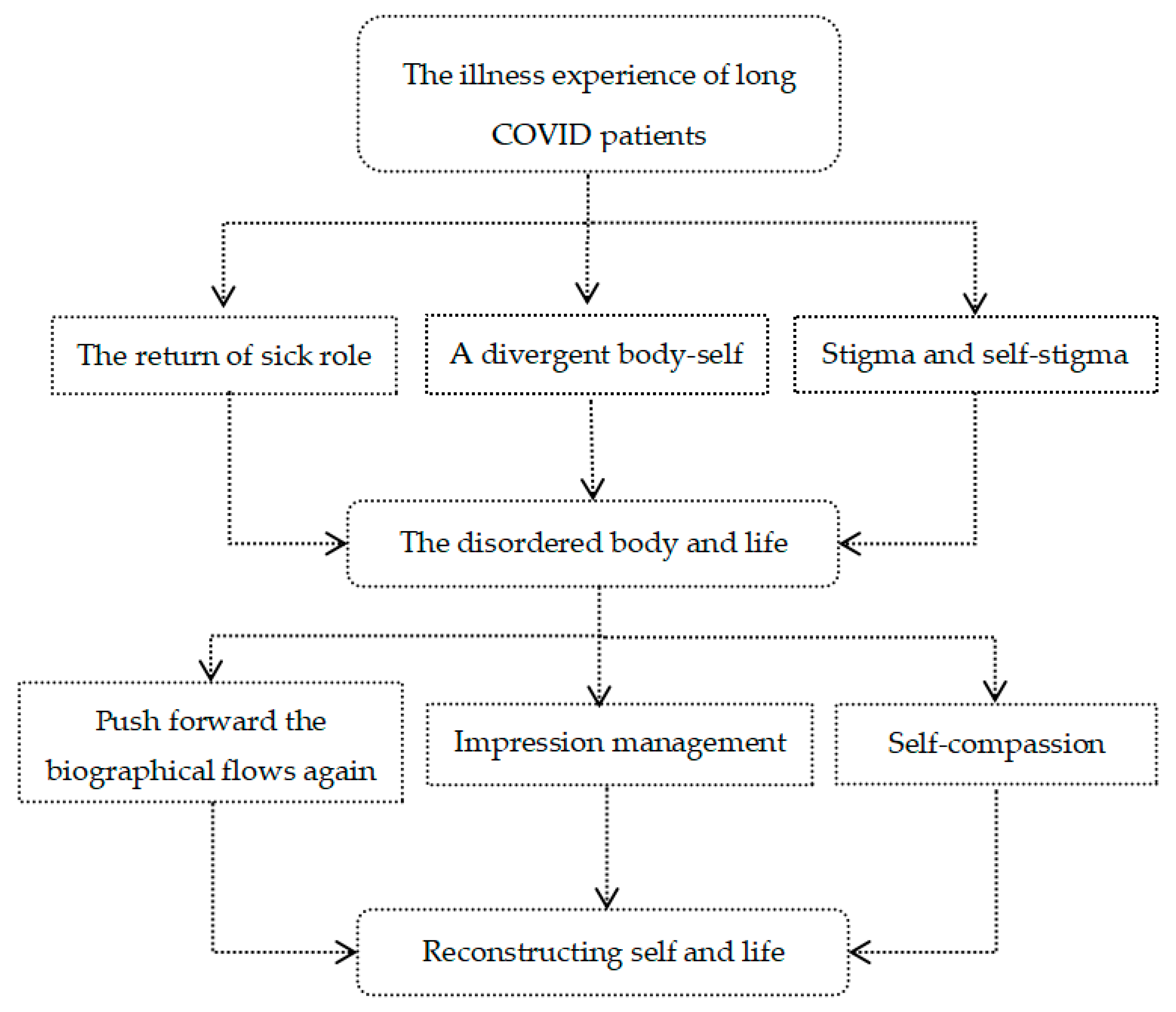
3. Results
3.1. The Disordered Body and Life
3.1.1. The Return of the Sick Role
“Thought I’d be discharged and all would be well…only to find out that I seem to have another disease, one for which there is no cure yet …”.[K,1]
“Now there are many physical sequelae, like constant headaches, dizziness, eye and orbital pain, bloodshot eyes, small dark spots appear when looking at things, easily getting fatigue, even waking up in the morning, tinnitus with pulse sounds and rumbling in the ears. I have been to the hospital many times and have had many tests done on my chest, lungs, head, nose, heart and so on, probably other tests I can’t remember. I feel helpless and pain that no one can understand and nowhere to talk about!”.[C,1]
“…the doctor unilaterally felt that my headaches were just caused by stress and also suggested me to see a psychiatrist”.[A,1]
3.1.2. A Divergent Body-Self
“…My body no longer seems to be mine… My hands sometimes shake uncontrollably as if someone is manipulating my body behind my back…”.[T,2]
“I asked myself over and over again, is this me? Is this really me? I used to run 1 km in the school sports day with ease, but now I can’t even walk up the stairs without panting”.[Z,2]
“I feel like I have become an 80-year-old granny, feeling useless and powerless ……”.[W,2]
3.1.3. Stigma and Self-Stigma
“When I meet colleagues, some just say hello at a far distance and walk away, some haven’t spoken to me again so far, some take the mask out of their pockets as soon as they see me and put it on hastily ……”.[B,3]
“The colleagues who were luckily recovered were basically discriminated against in the unit building, well, in a non-obvious way. And I was reassigned straight to the front line and stopped going to the building”.[J,3]
“I’ve been waiting for months, but still haven’t been hired, and I’ve had my nucleic acid test done so many times that I can’t remember. All the departments are afraid of taking the blame, so they are passing the buck to each other, which I know. They are afraid that I will retest positive, but I have never retested positive and now I am being labelled a ‘plague’ instead”.[U,3]
“In the six months since I was discharged from hospital, I have had little contact with relatives I used to be close to, let alone visit them”.[B,3]
“…… My best friend of more than 10 long years said when I was in hospital that she wanted to meet me for a good chat after I was discharged, but when I contacted her, she immediately changed the subject and eventually didn’t meet me ……”.[V,3]
“My personal and family information is transparent in the community and my unit, and everyone is focusing on me and on guard against me, with frequent nucleic acid tests to prevent my retest positive.”[R,3]
“…… Now I go out less and less, fearing that I will cause problems and burdens to others ……”.[I,3]
“……I always felt that I had caused trouble for the country and society, that I had disgraced my parents… When I couldn’t sleep at night, I would blame myself for going out that day, if I hadn’t gone out, I wouldn’t have been infected“.[M,3]
3.2. Reconstructing Self and Life
3.2.1. Pushing Forward the Biographical Flows Again
“I used to love bungee jumping, but now I’ve been advised by my doctor not to try it again due to health reasons … As a result I’m now hooked on embroidery and find I’m quite talented, so I’d like to try out for the city’s embroidery competition next!”[R,4]
“Even though life is hard now, I have to face the future positively! Being healthy is always the most important thing! To try all the things that I was afraid to try before!”[H,4]
“In the past, I always thought that I should work more overtime in the company to show myself in front of the leaders and get a promotion and a pay rise as soon as possible. Now I’ve come to realize that there is nothing more important than health, and it’s better to spend more time with myself and my families than to waste time on overtime”.[W,4]
3.2.2. Impression Management
“No one around me at the new school knows that I had COVID-19. I’m the same as everyone else, and my medical check-up at the beginning of the school year was fine, and I don’t say a word about it”.[M,5]
“If you want to still pretend to be normal, then the most effortless and efficient way is to hide it. Either you hide your condition or hide yourself”.[T,5]
“When people ask me if I have any after-effects of COVID-19, I choose to deny it ……”.[N,5]
“When I go to the company gym to work out, some of my colleagues will ask me intentionally or not, “Are you all right? Can you work out?”. I’m not happy inside, but I still smile and say “I’m fine” and then run 5 km to prove myself”.[B,5]
“… I often say when I talk to people that I have a high retirement salary, a filial son, and a healthy grandson who is fatter and taller than children of his age”.[O,5]
“I saw someone ask me in a private message on Zhihu app ‘How can I make people forget that I had COVID-19′ … I would like to say that although the fact that you had COVID-19 will not change, people’s attitude towards you will change. Now I volunteer in the community on weekends and many people in the community know me and have forgotten that I was once infected with COVID-19, they just say, ‘You’ve worked hard, you’re doing a good job’”.[Z,5]
3.2.3. Self-Compassion
“It may have been hard to adjust at first… but in retrospect, it was no big deal. So many of our public officials and medical staff are at work to confront the epidemic, and my hard work is nothing compared to theirs, so I’m just taking it as a training”.[G,6]
“Now what I already had the ill, instead of weeping and feeling sad every day, I would rather spend my time on more important things and be a more valuable person… I signed up to go to a remote mountainous area to teach in the summer, and when I saw that the children still love learning despite the hardship, I instantly felt that what I was doing was such a meaningful thing”.[Q,6]
“In the past six months, I’ve been through a lot of dramatic things, I got engaged, then got COVID-19, the groom broke off the engagement, lost my job, got re-employed… Life is always like this, everything doesn’t go smoothly, the most important thing is that your heart is always facing the light, shining bright like the sun!”[Y,6]
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brüssow, H.; Timmis, K. COVID-19: Long COVID and its societal consequences. Environ. Microbiol. 2021, 23, 4077–4401. [Google Scholar] [CrossRef] [PubMed]
- Rubin, R. As their numbers grow, COVID-19 “Long Haulers” stump experts. JAMA 2020, 324, 1381–1383. [Google Scholar] [CrossRef] [PubMed]
- A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus. 6 October 2021. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (accessed on 1 August 2022).
- Update on COVID-19 Outbreak as of 24:00 on 1 April. Available online: http://www.nhc.gov.cn/xcs/yqtb/202204/fbfcdb49a6784a97849d71fe8ce222a6.shtml (accessed on 1 August 2022).
- Groff, D.; Sun, A.; Ssentongo, A.E.; Ba, D.M.; Parsons, N.; Poudel, G.; Lekoubou, A.; Oh, J.S.; Ericson, J.E.; Ssentongo, P.; et al. Short-term and long-term rates of postacute sequelae of SARS-CoV-2 infection: A systematic review. JAMA Netw. Open 2021, 4, e2128568. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, H.; Patel, K.; Greenwood, D.C.; Halpin, S.; Lewthwaite, P.; Salawu, A.; Eyre, L.; Breen, A.; O’Connor, R.; Jones, A.; et al. ORCID logoLong-term clinical outcomes in survivors of severe acute respiratory syndrome and Middle East respiratory syndrome coronavirus outbreaks after hospitalisation or ICU admission: A systematic review and meta-analysis. J. Rehabil. Med. 2020, 52, jrm00063. [Google Scholar] [CrossRef] [PubMed]
- Strauss, A.; Glaser, B. Chronic Illness and the Quality of Life; Aldine: Chicago, IL, USA, 1975. [Google Scholar]
- Pierret, J. The illness experience: State of knowledge and perspectives for research. Sociol. Health Illn. 2003, 25, 4–22. [Google Scholar] [CrossRef] [Green Version]
- Gibbs, J. How metaphors shape the particularities of illness and healing experiences. Transcult. Psychiatry 2020. [Google Scholar] [CrossRef]
- Woods, M.; Macklin, R.; Dawkins, S.; Martin, A. Mental Illness, Social Suffering and Structural Antagonism in the Labour Process. Work Employ. Soc. 2019, 33, 948–965. [Google Scholar] [CrossRef]
- Bogusz, R.; Nowakowska, L.; Majchrowska, A.; Patryn, R.; Pawlikowski, J.; Zagaja, A.; Kiciński, P.; Pacyna, M.; Puacz, E. Convalescents’ Reports on COVID-19 Experience—A Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 6147. [Google Scholar] [CrossRef]
- Sahooa, S.; Mehraa, A.; Surib, V.; Malhotrab, P.; Narayana, L.; Goverdhan, Y.; Puric, D.; Grovera, S. Lived experiences of the corona survivors (patients admitted in COVID wards): A narrative real-life documented summaries of internalized guilt, shame, stigma, anger. Asian J. Psychiatr. 2020, 53, 102187. [Google Scholar] [CrossRef]
- Santiago-Rodriguez, E.I.; Maiorana, A.; Peluso, M.J.; Hoh, R.; Tai, V.; Fehrman, E.A.; Hernandez, Y.; Torres, L.; Spinelli, M.A.; Gandhi, M.; et al. Characterizing the COVID-19 Illness Experience to Inform the Study of Post-acute Sequelae and Recovery. Int. J. Behav. Med. 2021, 1–14. [Google Scholar] [CrossRef]
- Corbin, J.; Strauss, A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory, 3rd ed.; Sage: Riverside, CA, USA, 2007. [Google Scholar]
- Turner, C.; Astin, F. Grounded theory: What makes a grounded theory study? Eur. J. Cardiovasc. Nurs. 2021, 20, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Martin, V.B.; Scott, C.; Brennen, B.; Durham, M.G. What Is Grounded Theory Good For? J. Mass Commun. Q. 2018, 95, 11–22. [Google Scholar] [CrossRef]
- Hallberg, L.R.-M. The “core category“ of grounded theory: Making constant comparisons. Int. J. Qual. Stud. Health Well-Being 2006, 1, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Notification on the Issuance of the Protocol for the Treatment of COVID-19 (Trial Version 9). Available online: http://www.gov.cn/zhengce/zhengceku/2022-03/15/content_5679257.htm (accessed on 1 August 2022).
- Phelan, J.C.; Link, B.G.; Dovidio, J.F. Stigma and prejudice: One animal or two? Soc. Sci. Med. 2008, 67, 358–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, H.; Wang, Y.; Tong, Z.; Liu, X. Retest positive for SARS-CoV-2 RNA of “recovered” patients with COVID-19: Persistence, sampling issues, or re-infection? J. Med. Virol. 2020, 92, 2263–2265. [Google Scholar] [CrossRef]
- Wu, X.; Wang, Z.; He, Z.; Li, Y.; Wu, Y.; Wang, H.; Liu, Y.; Hao, F.; Tian, H. A follow-up study shows that recovered patients with re-positive PCR test in Wuhan may not be infectious. BMC Med. 2021, 19, 77. [Google Scholar] [CrossRef]
- Xian, M.; Zhao, C.; Zhou, Y. From Bureaucratic Coordination to a Data-Driven Model: Transformation and Capacity Building of Community-Based Prevention and Control of Public Health Events. Int. J. Environ. Res. Public Health 2022, 19, 8238. [Google Scholar] [CrossRef]
- Zhang, P. Analysis of the Public Health Functions of the Chinese Government in the Prevention and Control of COVID-19. Risk Manag Healthc Policy 2021, 14, 237–246. [Google Scholar] [CrossRef]
- Cluley, V.; Martin, G.; Radnor, Z.; Banerjee, J. Frailty as biographical disruption. Sociol. Health Illn. 2021, 43, 948–965. [Google Scholar] [CrossRef]
- Meijering, L.; Lettinga, A.T.; Nanninga, C.S.; Milligan, C. Interpreting therapeutic landscape experiences through rural stroke survivors’ biographies of disruption and flow. J. Rural. Stud. 2017, 51, 275–283. [Google Scholar] [CrossRef] [Green Version]
- Jetten, J.; Haslam, S.A.; Cruwys, T.; Greenaway, K.H.; Haslam, C.; Steffens, N.K. Advancing the social identity approach to health and well-being: Progressing the social cure research agenda. Eur. J. Soc. Psychol. 2017, 47, 789–802. [Google Scholar] [CrossRef]
- Barnard, L.K.; Curry, J.F. Self-Compassion: Conceptualizations, Correlates, & Interventions. Rev. Gen. Psychol. 2011, 15, 289–303. [Google Scholar] [CrossRef] [Green Version]
- Kristeva, J.; Moro, M.R.; Ødemark, J. Cultural crossings of care: An appeal to the medical humanities. Med. Humanit. 2018, 44, 55–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adom, D.; Mensah, J.A.; Osei, M. The Psychological Distress and Mental Health Disorders from COVID-19 Stigmatization in Ghana. Soc. Sci. Hum. Open 2021, 4, 100186. [Google Scholar] [CrossRef]
- Grover, S.; Sahoo, S.; Mishra, E.; Gill, K.S.; Mehra, A.; Nehra, R.; Suman, A.; Bhalla, A.; Puri, G.D. Fatigue, perceived stigma, self-reported cognitive deficitsand psychological morbidity in patients recovered from COVID-19 infection. Asian J. Psych. 2021, 64, 2815. [Google Scholar] [CrossRef]
- Kang, Y.J. South Korea’s COVID-19 infection status: From the perspective of re-positive after viral clearance by negative testing. Disaster Med. Public Health Prep. 2020, 14, 762–764. [Google Scholar] [CrossRef]
- Lan, L.; Xu, D.; Ye, G.; Xia, C.; Wang, S.; Li, Y.; Xu, H. Positive RT-PCR test results in patients recovered from COVID-19. JAMA 2020, 323, 1502–1503. [Google Scholar] [CrossRef] [Green Version]
- Urgent Notice from the Ministry of Human Resources and Social Security and the National Health and Wellness Commission on Resolutely Combating Employment Discrimination against People Recovering from COVID-19. Available online: http://www.mohrss.gov.cn/ldjcj/LDJCJzhengcewenjian/202208/t20220801_480012.html (accessed on 1 August 2022).
- Yang, T.; Wu, M.C. Discrimination against hepatitis B carriers in China. Lancet 2011, 378, 1059. [Google Scholar] [CrossRef]
- Liu, H.; Li, M.; Jin, M.; Jing, F.; Wang, H.; Chen, K. Public awareness of three major infectious diseases in rural Zhejiang province, China: A cross-sectional study. BMC Infect. Dis. 2013, 13, 192. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.; Shi, H.; Wu, X.; Jiao, L. Sentiment Analysis of Rumor Spread Amid COVID-19: Based on Weibo Text. Healthcare 2021, 9, 1275. [Google Scholar] [CrossRef]
- Lelisho, M.E.; Pandey, D.; Alemu, B.D.; Pandey, B.K.; Tareke, S.A. The Negative Impact of Social Media during COVID-19 Pandemic. Trends Inpsychol. 2022. [Google Scholar] [CrossRef]
- Shweta, S.; Saniya, B.; Huma, F. Surviving the stigma: Lessons learnt for the prevention of COVID-19 stigma and its mental health impact. J. Ment. Health Soc. Incl 2020, 24, 145–149. [Google Scholar] [CrossRef]
- Li, H.; Zheng, L.; Le, H.; Zhuo, L.; Wu, Q.; Ma, G.; Tao, H. The Mediating Role of Internalized Stigma and Shame on the Relationship between COVID-19 Related Discrimination and Mental Health Outcomes among Back-to-School Students in Wuhan. Int. J. Environ. Res. Public Health 2020, 17, 9237. [Google Scholar] [CrossRef] [PubMed]
- Van de Vyver, J.; Leite, A.C.; Alwan, N.A. Navigating the social identity of long COVID. BMJ 2021, 375, n2933. [Google Scholar] [CrossRef]
- Lie, N.-E.K.; Larsen, T.M.B.; Hauken, M.A. Coping with changes and uncertainty: A qualitative study of young adult cancer patients’ challenges and coping strategies during treatment. Eur. J. Cancer Care 2018, 27, e12743. [Google Scholar] [CrossRef]
- Singh, R.; Subedi, M. COVID-19 and stigma: Social discrimination towards frontline healthcare providers and COVID-19 recovered patients in Nepal. Asian J. Psychiatr 2020, 53, 102222. [Google Scholar] [CrossRef]
- Bouma, G.; Admiraal, J.M.; de Vries, E.G.; Schroder, C.P.; Walenkamp, A.M.; Reyners, A.K. Internet-based support programs to alleviate psychosocial and physical symptoms in cancer patients: A literature analysis. Crit. Rev. Oncol. Hematol. 2015, 95, 26–37. [Google Scholar] [CrossRef]
- Rickwood, D.; Web, M.; Kennedy, V.; Telford, N. Who Are the Young People Choosing Web-based Mental Health Support? Findings from the Implementation of Australia’s National Web-based Youth Mental Health Service, eheadspace. JMIR Ment. Health 2016, 3, e40. [Google Scholar] [CrossRef]
- Ide-Okochi, A.; Yamazaki, Y.; Tadaka, E.; Fujimura, K.; Kusunaga, T. Illness experience of adults with cervical spinal cord injury in Japan: A qualitative investigation. BMC Public Health 2013, 13, 69. [Google Scholar] [CrossRef] [Green Version]
- Lau, B.; Chan, C.; Ng, S.M. Self-compassion buffers the adverse mental health impacts of COVID-19-related threats: Results from a cross-sectional survey at the first peak of Hong Kong’s outbreak. Front. Psychol. 2020, 11, 1203. [Google Scholar] [CrossRef]
- Kavaklı, M.; Ak, M.; Uğuz, F.; Türkmen, O.O. The mediating role of self-compassion in the relationship between perceived COVID-19 threat and death anxiety. Turk. J. Clin. Psychiatry 2020, 23, 15–23. [Google Scholar] [CrossRef]
- Sontag, S. AIDS and Its Metaphors; Straus and Giroux: New York, NY, USA, 1989; p. 180. [Google Scholar]

{kind=link}
{kind=link}
| Original Texts (Excerpt) | Free Node (Excerpt) |
|---|---|
| Now there are many physical sequelae, like constant headaches, dizziness, eye and orbital pain (a1), bloodshot eyes, small dark spots appear when looking at things, easily getting fatigue (a2), even waking up in the morning, tinnitus with pulse sounds and rumbling in the ears. I have been to the hospital many times and have had many tests done on my chest, lungs, head, nose, heart and so on (a3), probably other tests I can’t remember. I feel helpless and pain that no one can understand and nowhere to talk about (a4)! Feeling like a completely different person from my old self (a5) and needing to readjust to my current body in order to continue living (a6). When I meet colleagues, some just say hello at a far distance and walk away, some haven’t spoken to me again so far, some take the mask out of their pockets as soon as they see me and put it on hastily …… (a7) | a1 Ongoing pain |
| a2 Body weakness | |
| a3 Invalid medical tests | |
| a4 Pain inside | |
| a5 Split between past and present | |
| a6 Trying to adapt to the body | |
| a7 “Social death” |
| Open Coding | Axial Coding | Selective Coding |
|---|---|---|
| Initial Category | Main Category | Core Category |
| A1 Physical abnormalities of subjective perception | B1 The return of sick role | C1 The disordered body and life |
| A2 Medical signs of objective examination | ||
| A3 Sense of lossing control of the body | B2 A divergent body-self | |
| A4 The unfamiliar body | ||
| A5 Employment discrimination | B3 Stigma and self-stigma | |
| A6 Social isolation | ||
| A7 Perceptions of being discriminated | ||
| A8 Internalised stigma | ||
| A9 Set new goals | B4 push forward the biographical flows again | C2 Reconstructing self and life |
| A10 Change the old values | ||
| A11 Conceal the illness | B5 Impression management | |
| A12 Deny the sequelae | ||
| A13 Rebuild the social image | ||
| A14 Be kind to self | B6 Self-compassion | |
| A15 Accept the imperfect self |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Bao, S.; Chen, Y. The Illness Experience of Long COVID Patients: A Qualitative Study Based on the Online Q&A Community Zhihu. Int. J. Environ. Res. Public Health 2022, 19, 9827. https://doi.org/10.3390/ijerph19169827
Wang Y, Bao S, Chen Y. The Illness Experience of Long COVID Patients: A Qualitative Study Based on the Online Q&A Community Zhihu. International Journal of Environmental Research and Public Health. 2022; 19(16):9827. https://doi.org/10.3390/ijerph19169827
Chicago/Turabian StyleWang, Yi, Sheng Bao, and Yubing Chen. 2022. "The Illness Experience of Long COVID Patients: A Qualitative Study Based on the Online Q&A Community Zhihu" International Journal of Environmental Research and Public Health 19, no. 16: 9827. https://doi.org/10.3390/ijerph19169827
APA StyleWang, Y., Bao, S., & Chen, Y. (2022). The Illness Experience of Long COVID Patients: A Qualitative Study Based on the Online Q&A Community Zhihu. International Journal of Environmental Research and Public Health, 19(16), 9827. https://doi.org/10.3390/ijerph19169827