1. Introduction
During the last two years, healthcare systems needed to develop resilience to cope with the COVID-19 pandemic [
1], control resources, and align targets to their mission in order to continue to effectively deliver care [
2].
For many years, pushed by international public reforms [
3,
4,
5,
6,
7,
8,
9] or national accrediting bodies [
10], healthcare systems and organizations have developed performance measurement systems to improve the efficiency and quality of health care [
11,
12,
13,
14,
15,
16,
17,
18,
19,
20]. During the last two years, the pandemic outbreak put even more pressure on the necessity to monitor the internal processes, patient flows, etc., in order to support the efficiency and quality of delivered care services [
21,
22,
23]. The monitoring of key performance indicators was essential in meeting organizations’ objectives [
24]. Moreover, the COVID-19 pandemic made clear the necessity to gain real-time information about patients in the department, number of attendances, etc. in order to adapt the organization to the required changes [
25].
During pandemics, organizations need to mainly lead the data useful to manage people and patients [
26,
27]. In that context, such in other previously analyzed contexts (see [
28]), the strategy can be defined as an entrepreneurial strategy [
29] where the leader, in this case, the strategic task force, takes decisions autonomously. Consequently, organizations need to align their strategic objectives with the day-to-day operations by creating or adjusting their monitoring system to manage organizations and deliver care.
In this context, performance measurement systems play an essential role. Performance measurement is a “process of quantifying the efficiency and effectiveness of an action” [
30] in order to monitor it or to “align unit goals with the organization’s strategy” [
31].
One model for measuring performance and supporting strategy implementation is the Balanced Scorecard (BSC) [
31,
32]. Since the 1990s, reforms at the international levels are asking for new management models for measuring and monitoring performance [
10,
33]. BSC has become a tool supporting the alignment of organizations’ mission, vision and strategy to action by leveraging on performance measurement. The BSC “translates a company’s strategy into specific measurable objectives” and, in this way, the core of the BSC is the strategy and vision of the organization and not control [
32]. A few years later, Kaplan and Norton [
34] and Kaplan [
35] deepened the design of BSC for nonprofit and governmental settings. Traditionally, a BSC model is a “balanced” set of financial and non-financial measures that gives information from four perspectives, i.e., financial, customer, internal business and innovation and learning (or learning and growth) [
32].
Nowadays, the Balanced Scorecard is widely spread in healthcare organizations [
36,
37]. In the last years, private healthcare systems reached high costs, thus costs and value measurement are essential [
38]. Additionally, for many years, public health organizations have been pushed to apply effective management systems to measure performance [
39].
However, issues related to BSC adoption have been still underlined by literature, as described below.
In order to investigate the BSC research, the authors adopt a recognized framework developed by Bourne et al. [
40]. In their study, Bourne et al., identified from previous literature three main phases of performance measurement system implementation, i.e., design, implementation and use; besides, they underlined also the essential role of updating and reviewing processes of measures and targets. Even if they built the classification basing the study on the manufacturing sector, the framework is not context-dependent. By adopting Bourne et al. [
40]’s framework, the authors analyzed the BSC implementation process as a whole.
Moreover, in an uncertain and continuously evolving environment, the design of the adopted BSC needs to be updated to cope with the external changes and the target and performance indicators need to be reviewed to be aligned with the organization’s strategy. The traditional BSC perspectives [
32] are not always able to catch the new needs, such as the environmental dimension [
41], or integrated care and humanization [
42]. As a consequence, specific redesign of BSC perspectives aligned with the organization’s strategy and planned updating processes for measures and targets should be carried out by the organizations.
Concerning the implementation of BSC, since the beginning of the 2000s, several authors have investigated not only the drivers but also the barriers to implementing BSC [
36,
41,
43,
44]. Inamdar et al. [
45] described the challenges faced by applying the Balanced Scorecard in a healthcare organization (e.g., the need for obtaining executive time and commitment, making the scorecard simple and easy to use). Recently, other literature reviews [
46,
47] emphasized the importance of stakeholder engagement. As drivers of successful BSC implementation, some authors listed trust, leadership support, etc. However, further research is required to explore the drivers of BSC implementation such as the involvement of patients in the BSC reporting and development strategies that overcome the simply customer satisfaction questionnaires [
46]. Notwithstanding the increasing interest in patient-centered care or community building, a recent review [
46] identifies that, even though needed, “the patients are not engaged to support patient and family-centered care”.
Regarding the use of BSC among healthcare institutions, only a few research explicitly emphasizes how organizations use BSC [
42,
48] according to the adopted classification of BSC usage [
49]. Related to the public sector, an empirical study highlighted that organizations have to assess several mandatory targets, they used BSC for legitimacy seeking [
48]. Another case described how organizations have sought to use BSC for strategic decision-making and monitoring internal processes [
50]. However, the studies available are not enough to understand how healthcare organizations are using BSC (only a few papers declare explicitly how they use BSC in day-to-day activities). Consequently, further investigation is needed to shed light on this research field.
Due to the current events caused by COVID-19 pandemics, the above-mentioned gaps related to BSC design, implementation, use and review, need even more urgent answers for deepening how to support healthcare organizations in assessing performance.
To address the research gaps, the paper aims at answering the research question below: How has research on the design, implementation, use, and review of BSC in healthcare settings evolved over the years?
In light of the development plans required for healthcare systems resulting from the COVID-19 pandemic [
51,
52,
53], the study highlights the state of the art of the BSC model. By mapping the development of BSC over the years it provides two main contributions: it describes how BSC has been designed and implemented in healthcare organizations to favor an efficient and effective use of resources and it provides a comprehensive overview for future empirical research in this area.
Drawing from Bourne et al. [
40]’s classification of BSC adoption phases, the paper systematically reviews literature, without limiting the timeframe, to analyze the perspectives adopted in BSC design, the barriers and drivers to implement BSC, the several uses and the review processes of the BSC. By providing insight into the BSC evolution in healthcare, the findings could offer avenues for future research both in the academic world and also among policy-makers who could become aware of how healthcare organizations use BSC.
The paper is structured as follows.
Section 2 deepens the methodology adopted for the review.
Section 3 reveals the findings developed after the data analysis and
Section 4 discusses them to provide the avenues for future research. Finally,
Section 5 provides the main conclusion of the review and the research limitations.
2. Materials and Methods
To strengthen the transparency and rigor of the review, the research process has been driven by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) methodology [
54,
55]. PRISMA is an accepted approach developed in 2005 that provides a checklist to guide systematic literature reviews [
54,
55].
In line with the above-mentioned checklist [
54,
55] and other recent systematic reviews based on PRISMA [
47,
56], the following section deepens the review’s phases to select and analyze the selected articles.
2.1. Eligibility Criteria
According to the research objective, i.e., to investigate the evolution of the Balanced Scorecard in the healthcare context, the following criteria have been adopted:
Article characteristics: papers must be written in English and published in scientific journals. The authors’ objective is to analyze the evolution of the BSC in healthcare, thus the involved studies must be mature and approved by the scientific community to ensure a deeper comprehension of their results. Including only scientific journals, however, could introduce an academic bias.
Topic: papers must be focused on the Balanced Scorecard to improve organizational performance of the system, healthcare organization or healthcare service. Included studies have to incorporate the BSC concept as evaluated by Kaplan and Norton [
34]. Moreover, included studies must emphasize at least one of the four phases of the BSC, i.e., BSC design, implementation, use, or review [
40].
Typology of healthcare setting: papers do not must be focused on a specific setting (e.g., hospitals, health systems). To map the BSC evolution in healthcare, it is noteworthy indeed also to evaluate the evolution of research interest in the different settings related to the healthcare context.
Research methodology: according to PRISMA guidelines, selected papers can develop either empirical research or a literature review. Including both review and empirical papers allows to include record findings of previous literature reviews related to BSC in healthcare (see PRISMA flow diagram [
55]).
Consequently, the following sets of papers were excluded:
Papers not focused on healthcare settings, such as hospitals, primary services, and local health authorities. Thus, papers focused on other settings referred both to healthcare (such as healthcare supply chains) or to other settings (manufacturing, oil and gas, etc.) are not included in the analysis.
Papers not focused on BSC as a model for measuring performance or as a strategic tool.
Papers not focused on the BSC adoption phases, i.e., design, implementation, use and review according to Bourne et al. [
40]’s research.
2.2. Information Sources and Search Strategy
The records have been selected by searching on Scopus, Web of Science (WoS), and PubMed electronic databases. The identification via databases was carried out in April 2022. To map the evolution of the Balanced Scorecard in the healthcare context, the selection was not limited to a fixed time frame.
According to the database, each search string selects records by keywords (Scopus, WoS) or title (PubMed). PubMed string has been limited to the title for narrowing the bias related to the identification of records (e.g., papers focused on clinical evaluation of specific patients’ diseases) and consequently identifying only records consistent with the review aim. Moreover, each search string (see
Table 1), limits the records to papers only written in English. The limitation of the English language was carried out in all the search strings to identify only papers that can be understood by the research team.
Table 1 provides evidence related to the strings used for selecting the dataset.
As
Table 1 reveals, the terms used in the search strings highlighted the two main topics of the review: the balanced scorecard and the healthcare setting.
Regarding the balanced scorecard, the selected words are “balanced scorecard”, “balanced score card” (it is a less common way to write BSC, although incorrect), and BSC (the acronym of balanced scorecard).
Regarding the healthcare context, the selected words are health (as catches also health system, health facility, etc., but it introduces several biases such as works related to health conditions, health finance, etc.—see next section for more details), hospital, hospitals, hospitalization/hospitalisation. The last four words have the same root word; however, they have been made explicit in order not to introduce another bias related to hospitality (which refers mainly to the tourism context).
2.3. Study Selection and Data Collection Process
According to the PRISMA flow diagram [
55], the article selection process develops into identification, screening, and eligibility steps in order to identify the papers included in the review.
Each step was performed several times by the authors. The record search process has been reiterated several times as it needed to be revised and discussed among the research team. Once the objective of the review was identified, the keywords were discussed and selected only after testing the search strings. Then, the screening and eligibility steps were developed together with the research team in order to identify effective exclusion criteria.
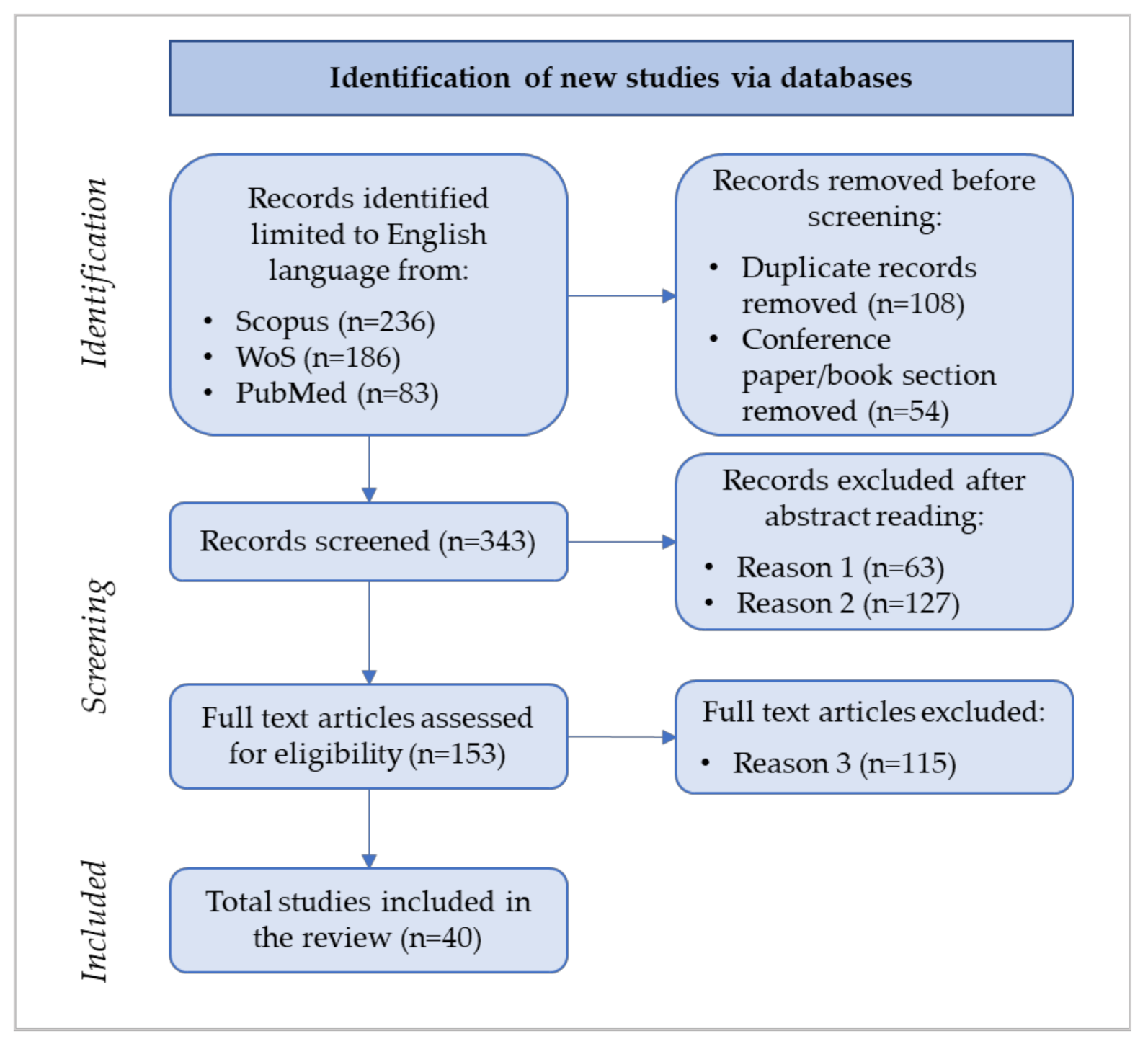
Figure 1 shows the review’s flow diagram consistent with the PRISMA guidelines (last access: May 2022).
As
Figure 1 illustrates, during the identification phase of the flow diagram 505 records were firstly sorted based on the search strings, and then, after duplicate and conference/book removal, 343 records were selected.
The abstract reading, during the screening phase, was carried out according to the exclusion criteria selected by the research team. According to the exclusion criteria described in
Section 2.1, the first exclusion criterion (i.e., Reason 1 in
Figure 1) led to the removal of 63 records; the rationale for this criterion refers to the bias introduced mainly by the keyword “health*” embedded in the search strings (as explained in
Section 2.2) because it includes non-healthcare-related articles in the 343 identified records (e.g., banking, wastewater, petroleum, manufacturing, etc.).
The second exclusion criterion, i.e., Reason 2 in
Figure 1, refers to the papers that do not focus on the balanced scorecard as a strategic tool to enhance organizational performance.
Table 2 lists the number of papers excluded according to Reason 2.
After the abstract reading, in line with the PRISMA guidelines [
57], the screening phase proceeded with the full-text reading of the 153 papers. The rationale of the third exclusion criteria is consistent with the framework, explained in the following section, adopted to analyze data.
The 40 selected papers deepen BSC design, implementation, use, or review and enable the research team to answer the research question.
2.4. Data Items and Framework Adopted
The analysis of the 40 papers was carried out by gathering information related to:
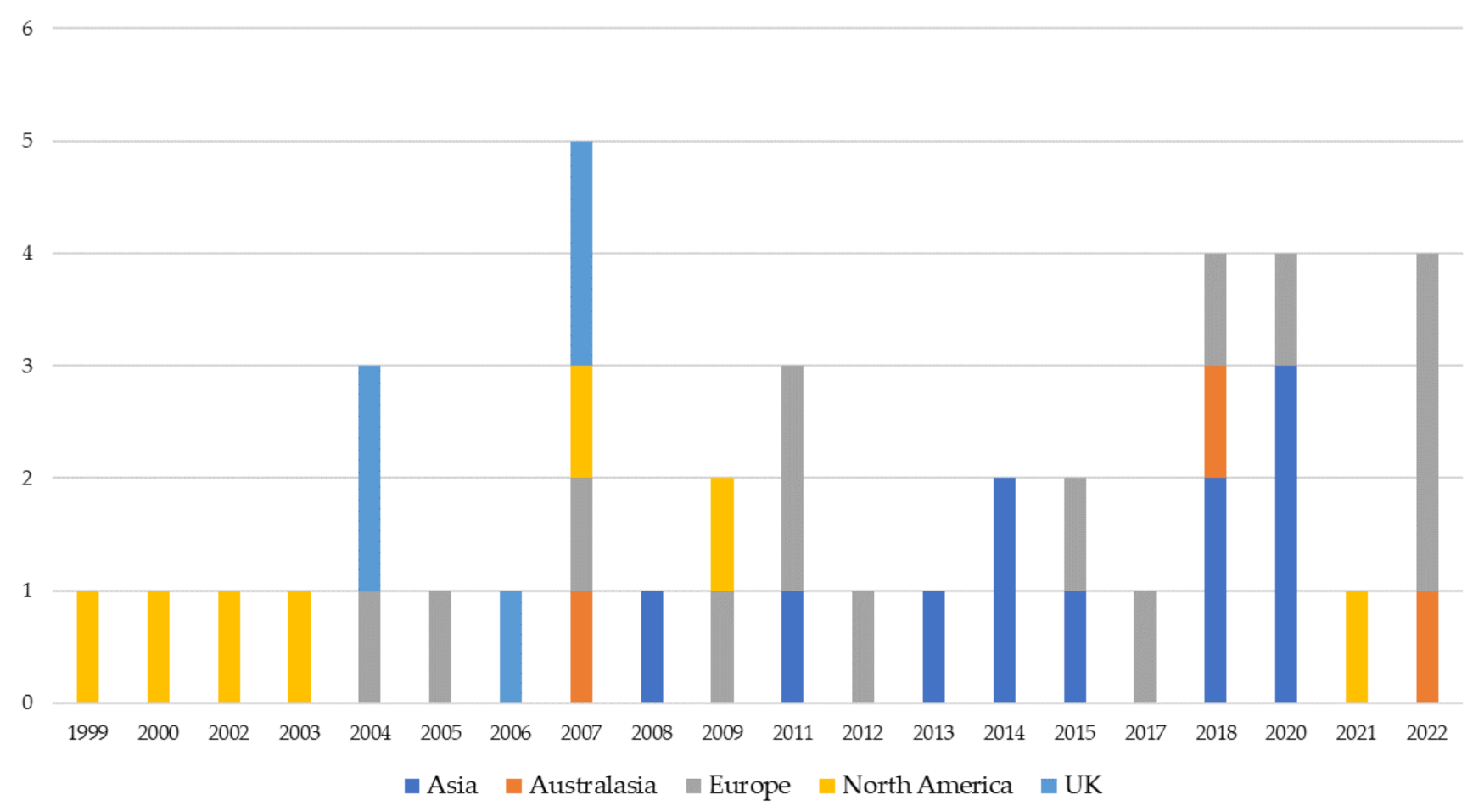
Publication year;
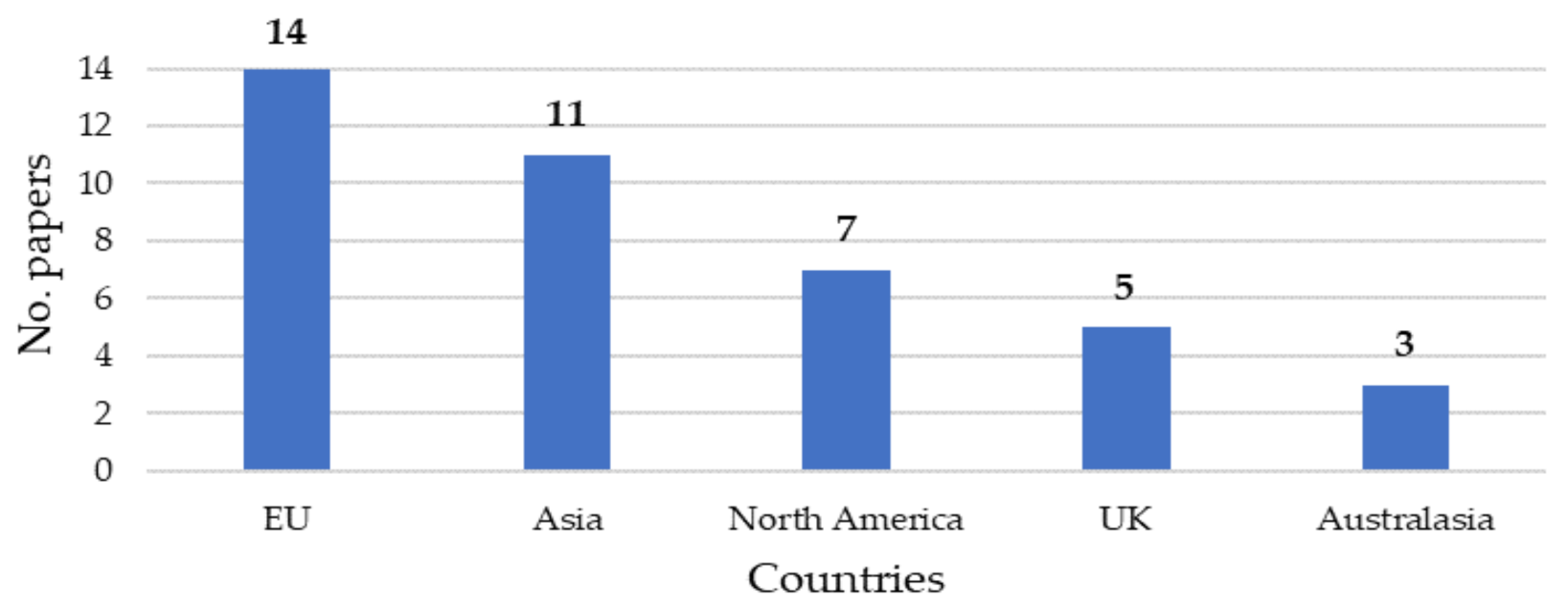
Country where the empirical research was developed, or, in the case of conceptual/review paper, the country of the corresponding author;
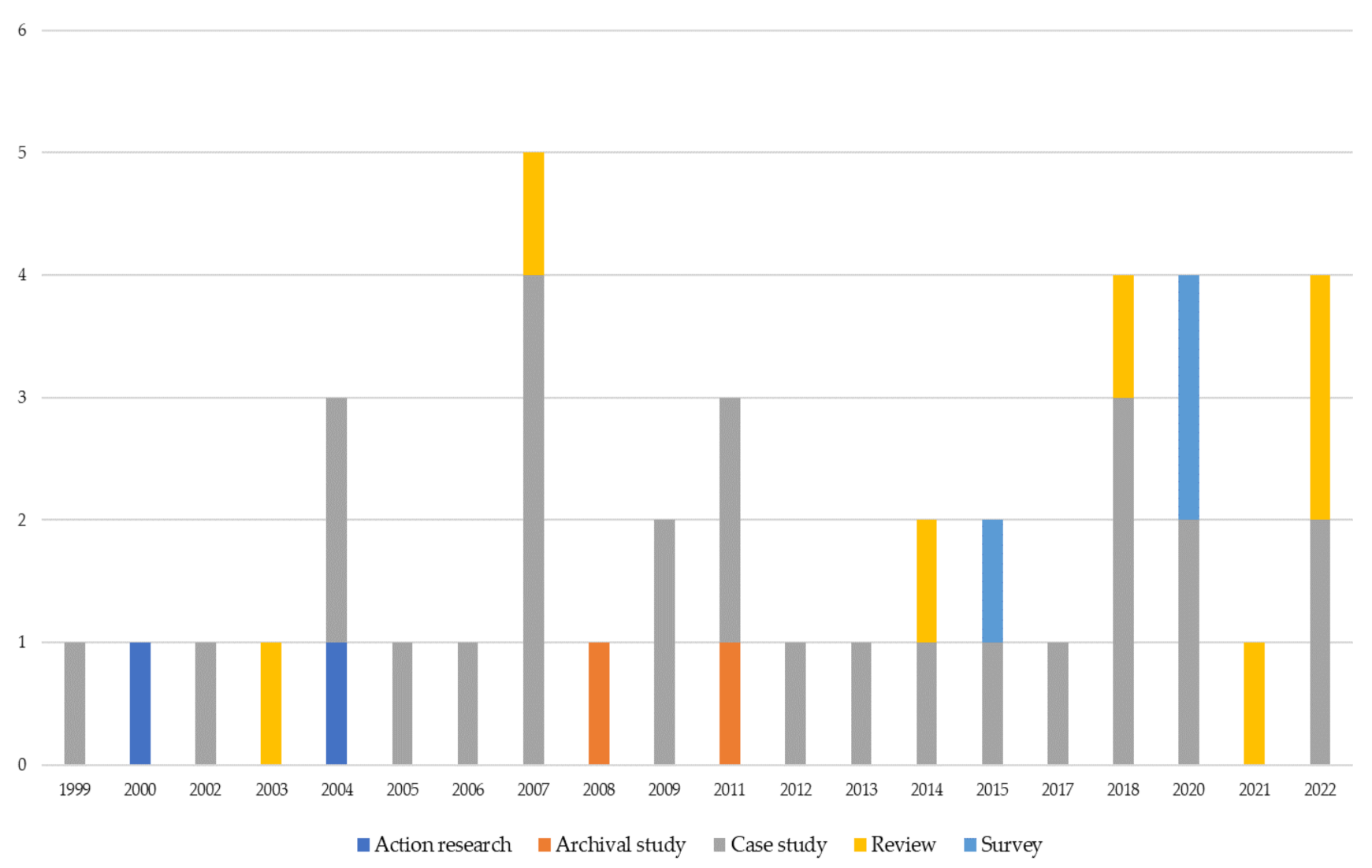
The methodology adopted: case study, survey, review, etc.;
Typology of service: private, public, no profit;
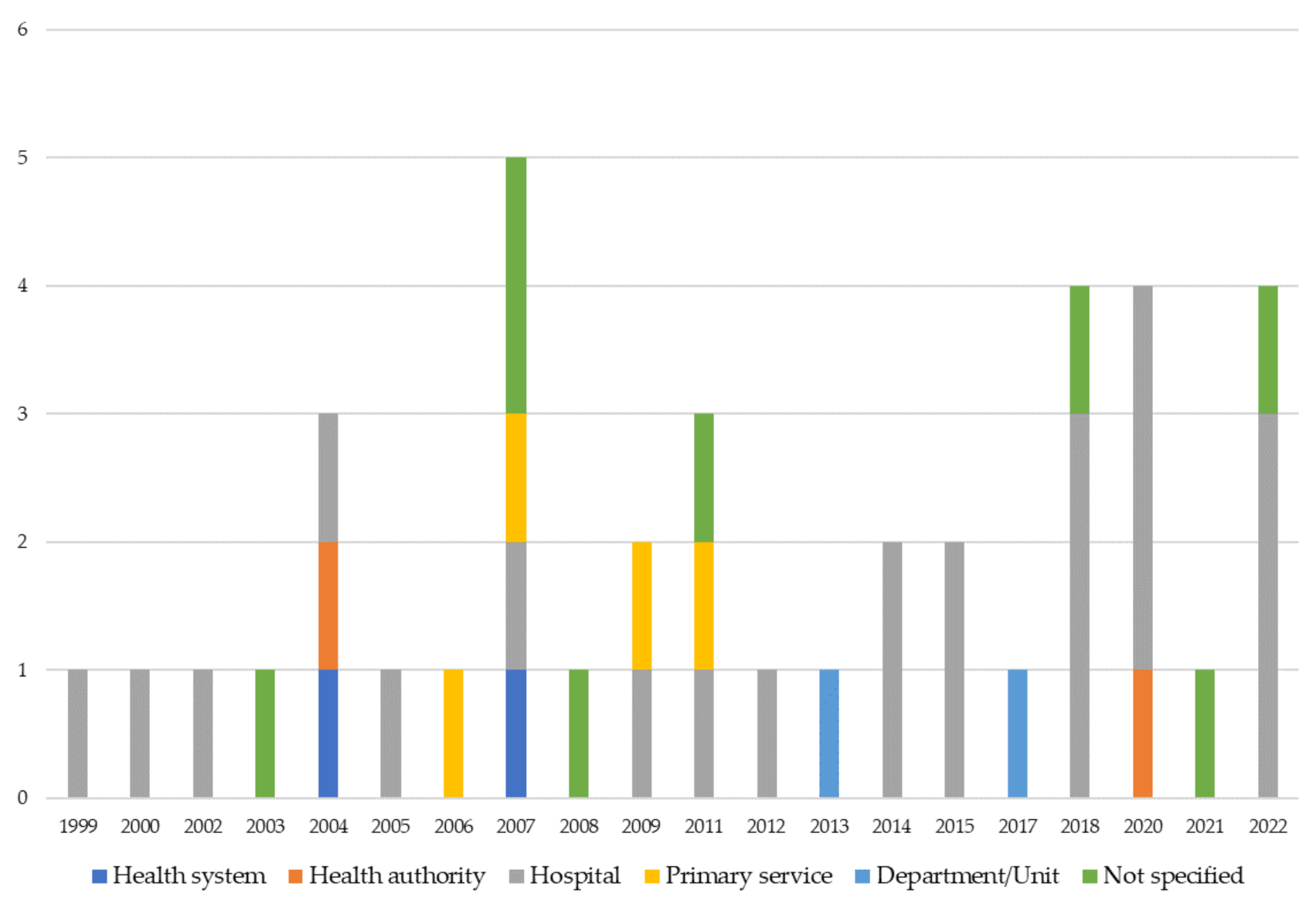
Unit of analysis: health system, health organization/hospital/health facility, department, or specific care service.
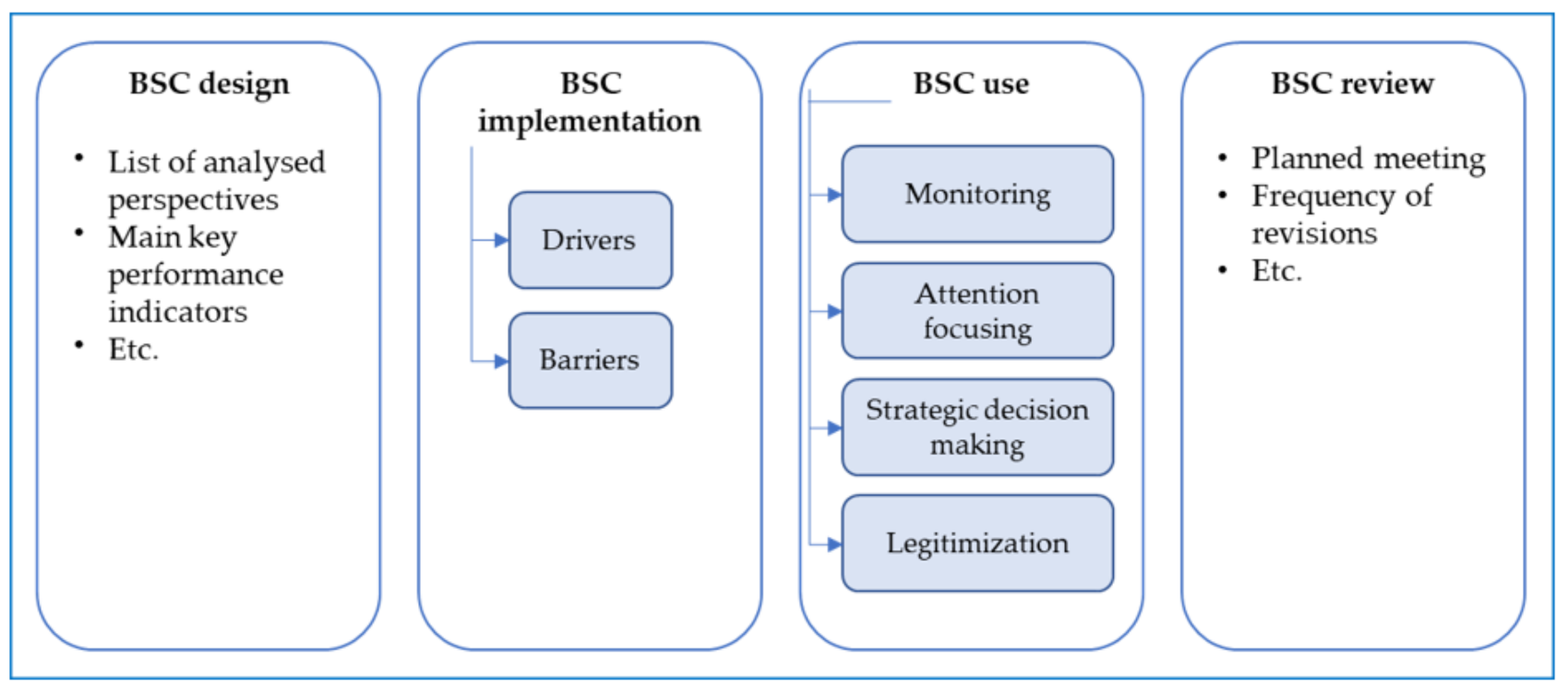
The above-listed items were used to map the evolution of BSC research in healthcare. Then, to deepen the BSC pathways in healthcare the research team adopted the framework displayed in
Figure 2.
Figure 2 reveals the framework adopted to analyze papers. As BSC literature outlines, there are four phases in the BSC adoption [
40,
58]:
Regarding the BSC design, the analysis aims at emphasizing the adopted perspectives and the main key performance indicators used;
Regarding the BSC implementation, the focus is on the drivers and barriers that push or hinder the implementation of BSC;
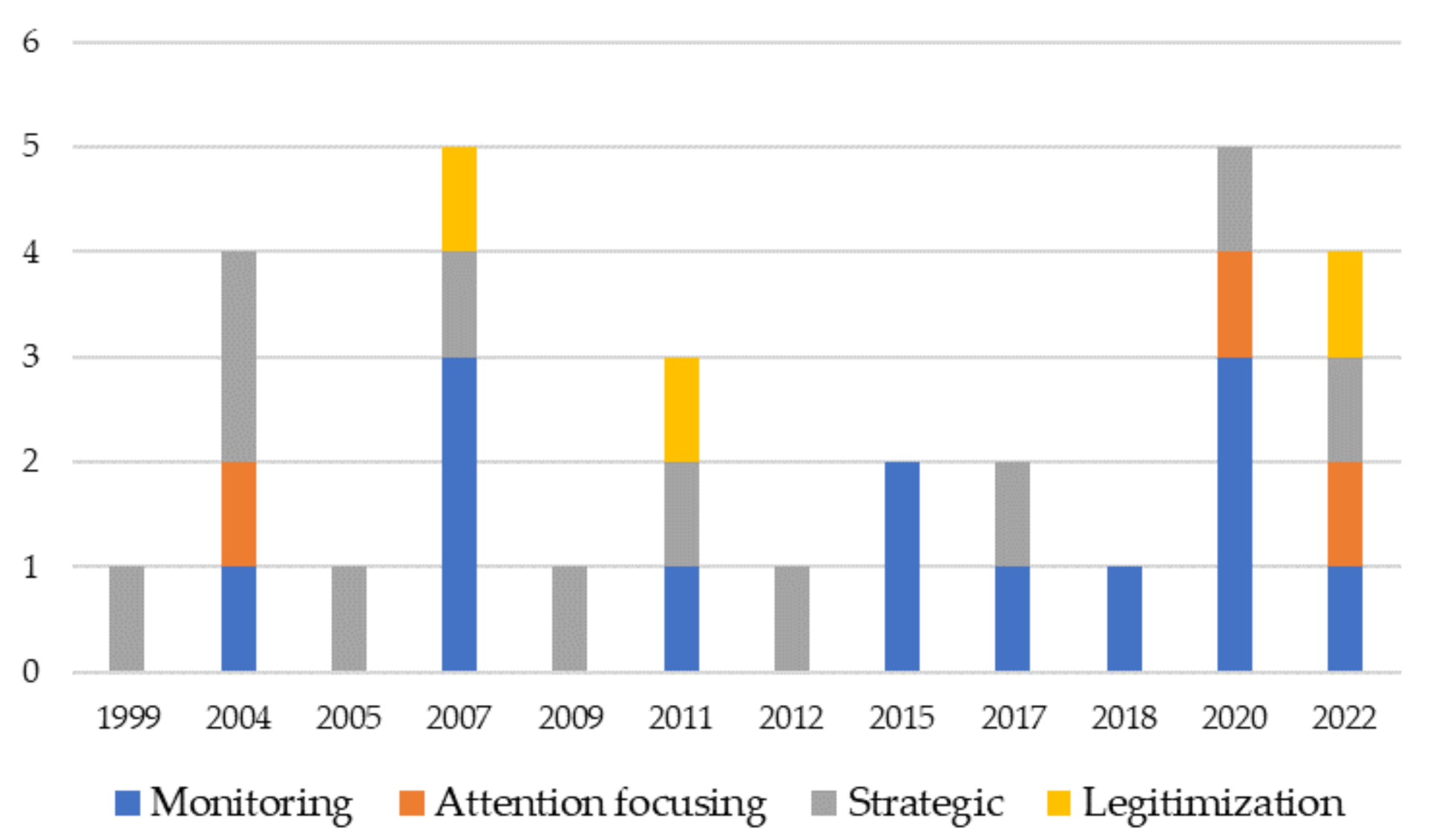
Regarding BSC use, the research team adopted a highly cited work that distinguished BSC use in monitoring, strategic decision making, attention focusing, and legitimization, also recently adopted in an empirical study focused on BSC in a hospital [
42];
Regarding the BSC review, in line with [
40], the review process includes a set of mechanisms for reviewing targets and standards and processes for a periodical review of the set of measures adopted.
Drawing from
Figure 1, the 40 selected papers were analyzed and the main findings are presented in the following section.
4. Discussion
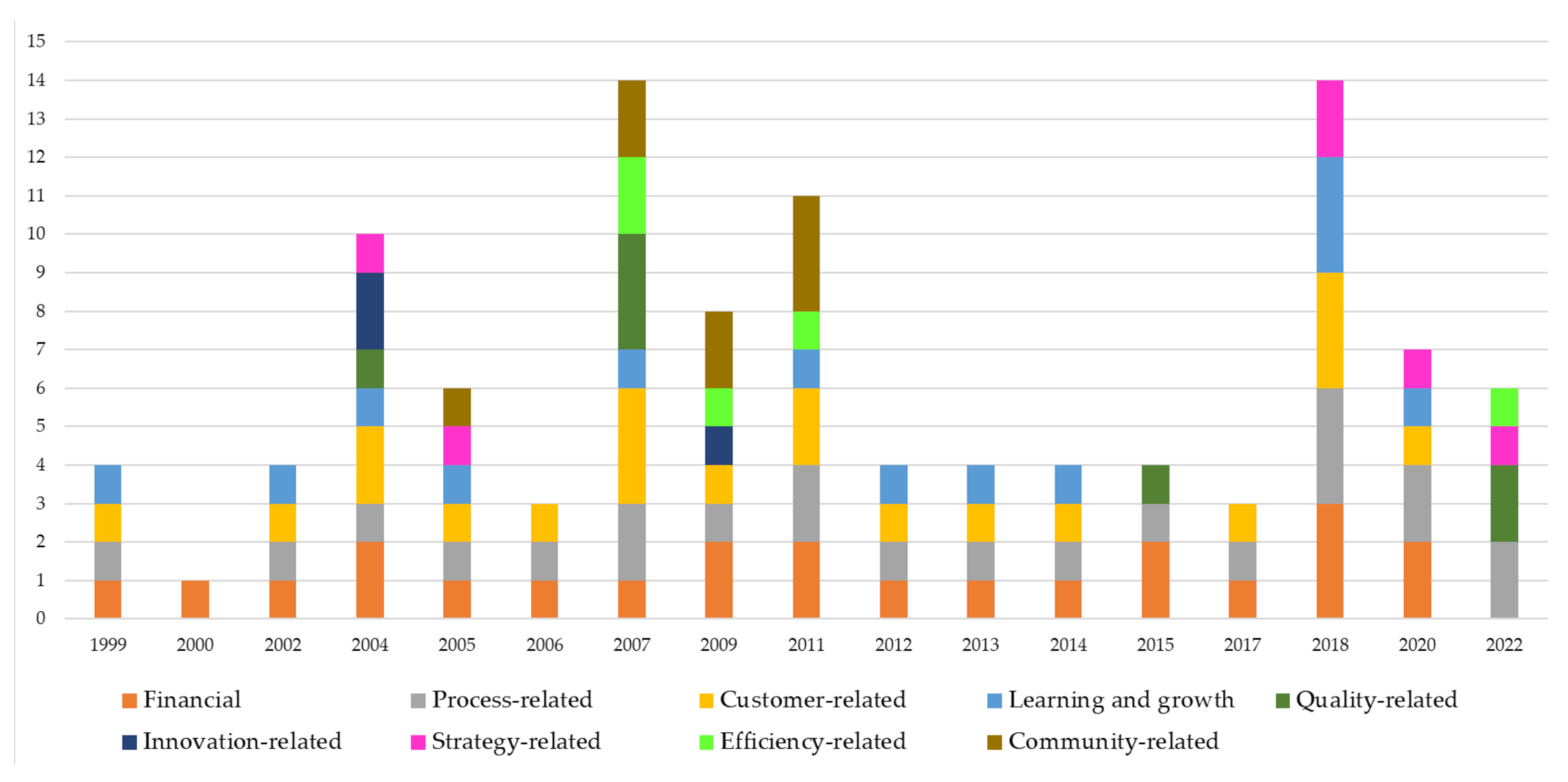
The findings reveal that research on BSC in healthcare contexts is still directed toward the BSC design process. The majority of papers (34 of the 40 papers) paid particular attention to the BSC perspectives. In line with Gonzalez-Sanchez et al. [
36], the analysis shows that papers focus mainly on the traditional four perspectives, i.e., financial, customer, processes, and learning and growth. Notwithstanding the maturity of the BSC model which emphasizes the balanced nature of the perspectives, financial is still the most analyzed (see
Table 7). As a matter of fact, even if the prevalent typology of delivered service is public, the healthcare settings at all levels (systems, organizations, primary services, etc.) need to put great attention to financial indicators such as expenditures [
39,
84], financial accessibility and viability [
63], and net profit margin [
39].
This is in line with the monitoring use of BSC, implicitly underlined by many authors [
67,
69].
However, although the financial perspective remains prevalent over the years, the process-related perspective is rapidly increasing in the number of published papers that analyze it [
39,
63,
66]. This is in line with the “attention focusing” use of BSC, where workers are motivated to achieve specific objectives (adapted from Henri’s definition [
49]). Indicators such as bed turnover, post-operative infection rate, etc., describe specific objectives to be achieved at the strategic level but also the operational level within the single service or department.
In addition to the most frequently analyzed perspectives, the review sheds light on the other five groups of perspectives. As highlighted in the Findings section, several indicators match financial, process, customer or learning and growth indicators (e.g., weight of hospital stay belongs to financial [
68,
76] and community [
66] perspectives). The paper highlights that BSC research is still mainly focused on BSC design, and, even if new perspectives emerge to emphasize some strategic objectives of organizations or systems, they are quite similar to the four traditional perspectives. They are often a subset of financial, customer, learning and growth, or process perspectives.
Thus, some future research avenues could be addressed.
Given the emphasis put on the BSC design, future research could analyze why there is no agreement between the perspectives. Even though the indicators are different between organizations and settings, the perspectives are not consistent with a specific healthcare setting. For example, the community perspective has been adopted by healthcare organizations [
86,
87] and by primary health services [
61,
80]. At the same time, the community perspective embodies some indicators belonging traditionally to the customer perspective [
61].
Concerning barriers and drivers in implementing BSC, the findings shed light on a lack of a standardized way to rank the factors that enable or restrain BSC. Some drivers match each other, for example, communication [
46,
74], absence of duplicated information and meetings are closely related. Similarly, leadership support can foster process understanding [
43], collaborative culture [
65] and participation [
80]. The same happens with barriers. The lack of organizational culture ready to accept change is closely linked to the perception of BSC as a control tool, to a narrow view of BSC, etc. In addition, papers focus on similar factors, viewing them as barriers or drivers of BSC implementation, such as leadership and organizational culture, depending on how they are perceived.
Although analyzed by several studies [
36,
41,
61,
65], there is a need for further research for identifying a standard way to explicate barriers and drivers of BSC implementation. Thus, future research could focus on management practices that enable BSC implementation at the different organizational levels (i.e., systems, organizations, primary care services, units/departments).
Concerning the use of BSC in healthcare organizations, only a few papers declare the BSC use that the organizations/systems did. Although the review identifies 13 papers concerning monitoring and 11 concerning strategic decision-making use of BSC (in line with the framework provided by Henri [
49]), the papers do not explicitly refer to how the organizations use the BSC. The remaining papers, on the other hand, did not reveal even implicitly how organizations use the BSC. Thus, future research can stress more explicitly how diverse healthcare settings use the BSC.
Regarding the last phase of BSC adoption, i.e., BSC review, only a few papers explicitly mentioned it [
41,
47,
74,
75,
80,
94]. Future research needs to focus on this fourth phase, even though during the initial phase of BSC design, the review process is essential, meetings and participation in short-term decisions [
65] can favor the implementation of BSC.
Finally, concerning the current situation, where healthcare organizations are coping in the last two years with the COVID-19 pandemic, it would be interesting empirically investigate the different outcomes achieved in the organizations that already implemented a BSC model and in those that used other measurement systems. Given the importance of gaining real-time information during a crisis [
26,
27], it would be interesting to analyze the effectiveness of BSC in this specific context. In the same way, it would be interesting to understand which BSC measures are useful during a pandemic context to endure quality and efficiency in delivering care. Notwithstanding the positive outcomes derived from BSC implementation and use, as in the review of Amer et al. [
47], no studies have been found related to the effects of BSC during pandemics.
5. Conclusions
The paper addresses the research question, i.e., how BSC evolved over the years in health settings, by mapping the development of BSC adoption phases [
40] over the years in healthcare. Through the review’s framework illustrated in
Figure 2, the BSC’s main perspectives, the barriers and drivers in implementing BSC, and the use and review of BSC have been analyzed. Although the prevalent interest in BSC research is on the design, the review analyzes several papers that focus also on the barriers and drivers, and the use of BSC (even not explicitly). However, only a few papers analyze the review process of BSC, by shedding light on the low maturity of BSC in healthcare contexts.
Moreover, the analysis of the review on BSC in healthcare settings, differently from the recent review of Amer et al., [
47] reveals that it is not possible to identify three generations of BSC. By adopting the review’s framework (
Figure 2), BSC adoption phases [
40], i.e., design, implementation, use and review are strictly related. As the findings reveal, for example, a specific focus on process perspective is followed by an increase in the “attention focusing” use of BSC. The liaison is represented by the recognized relevance of leadership support to promote a collaborative culture in implementing BSC.
Although the findings give room for several future research avenues, as discussed in the previous section, the review has some limitations. Concerning methodology, in the review have been selected search strings based on keywords in Scopus and Web of Science and on the title in PubMed. This choice, even if adopted in other reviews [
95,
96], has limited the results. Consequently, future research could run the search strings by investigating also the title and abstract (regarding Scopus and Web of Science). Moreover, the involvement of academic journals only can introduce an academic bias. Thus, future research could consider also conference papers, books, and grey literature.
Finally, the authors identified BSC as the focus of their research because it has been the most adopted model over the years. However, future research could verify through a literature review what are the other tools/models the healthcare settings use to measure performance, or if they are not adopting tools.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}








