
Environmental Factors Associated with Severe Motorcycle Crash Injury in University Neighborhoods: A Multicenter Study in Taiwan

 ,
, 
 ,
, 


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Design and Participants
2.3. Measurements
2.4. Statistical Analysis
3. Results
Subgroup Analysis of 18–24-Year-Old Patients
4. Discussion
4.1. Limitations
4.2. Practical Implications
5. Conclusions
- Although motorcycle crash injury is serious, especially among young adults, data on environmental factors affecting injury severity among motorcyclists in university neighborhoods are limited.
- Our study is the first to investigate the association between environmental factors and motorcycle crash injury severity in university neighborhoods in Taiwan.
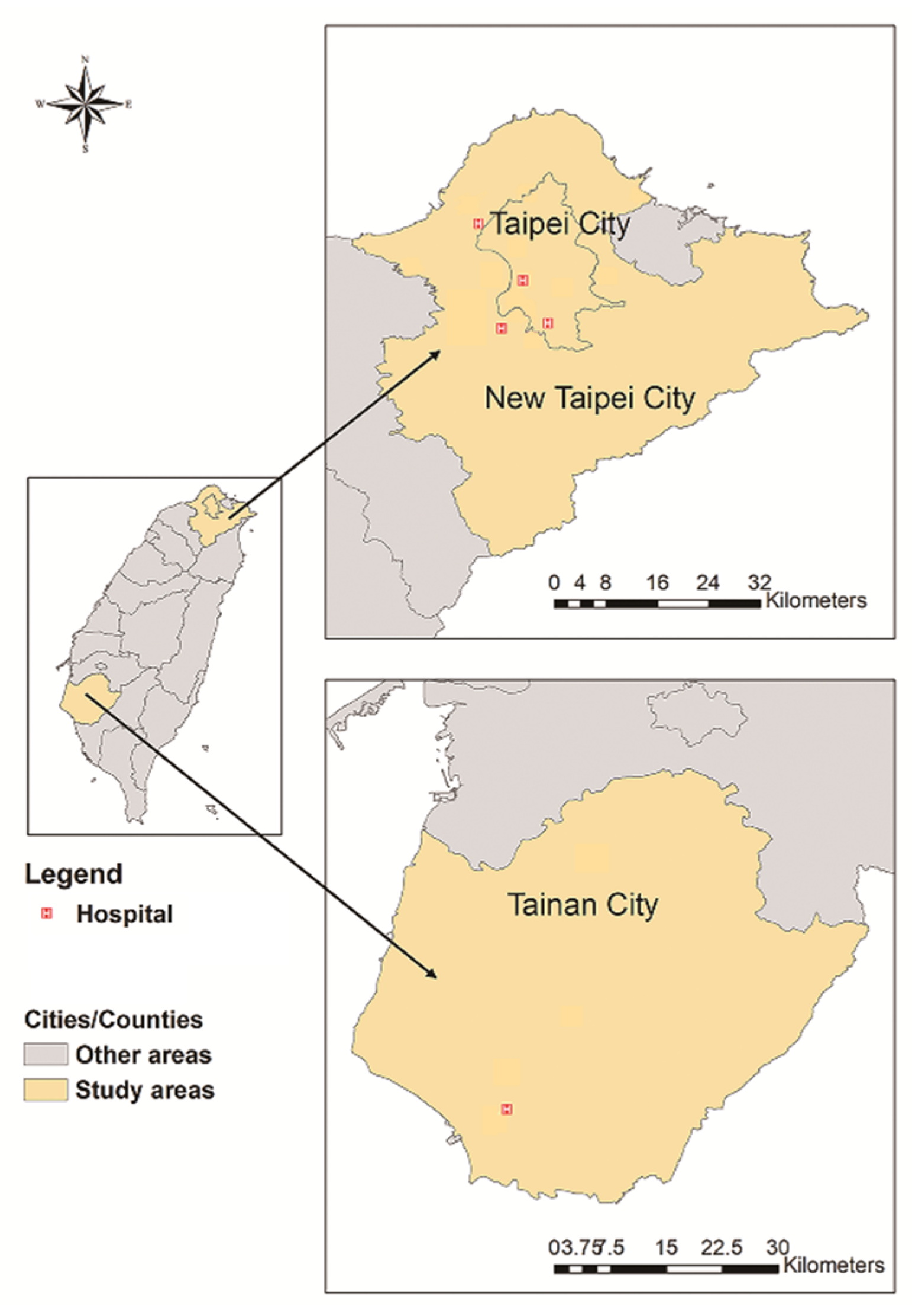
- A university neighborhood is defined as an area with the most movement of university students.
- The subgroup analysis sample, namely, the 18–24-year-old adults injured in a motorcycle accident in a university neighborhood, can considerably represent university students.
- The significant risk of severe injury while driving in the early morning may reflect the high motorcyclist volume and chaotic traffic conditions during this period in university neighborhoods.
- Our data reveal actionable targets for mitigating RTIs in university neighborhoods, namely, flashing signals at intersections and roadside obstacles.
- Single-motorcycle crashes and drunk driving are significant risk factors for severe motorcycle crash injury in university neighborhoods.
- Adverse weather does not increase the risk of severe motorcycle crash injuries in university neighborhoods.
- The protective effect of longer time to hospital indicates the effectiveness of urban emergency medical services in Taiwan.
- In our study results, female motorcyclists are significantly associated with severe motorcycle crash injury in university neighborhoods, which may be due to the high proportion of female motorcyclists in Taiwan. Further in-depth research is necessary.
- The results of the subgroup analysis may reflect lifestyle habits of young adults in university neighborhoods, such as not engaging in drunk driving and frequently driving in the afternoon and late at night.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Status Report on Road Safety 2018. Available online: https://www.who.int/publications-detail-redirect/9789241565684 (accessed on 19 May 2022).
- Fagnant, D.J.; Kockelman, K.M. Motorcycle use in the United States: Crash experiences, safety perspectives, and countermeasures. J. Transp. Saf. Secur. 2015, 7, 20–39. [Google Scholar] [CrossRef]
- Wick, M.; Müller, E.J.; Ekkernkamp, A.; Muhr, G. The motorcyclist: Easy rider or easy victim? An analysis of motorcycle accidents in Germany. Am. J. Emerg. Med. 1998, 16, 320–323. [Google Scholar] [CrossRef]
- Cracchiolo, A.; Blazina, M.E.; MacKinnon, D.S. Motorcycle injuries to university students: The high price of the economical motorbike. JAMA 1968, 204, 77–78. [Google Scholar] [CrossRef] [PubMed]
- Lam, C.; Pai, C.W.; Chuang, C.C.; Yen, Y.C.; Wu, C.C.; Yu, S.H.; Hung, K.S.; Chiu, W.T. Rider factors associated with severe injury after a light motorcycle crash: A multicentre study in an emerging economy setting. PLoS ONE 2019, 14, e0219132. [Google Scholar] [CrossRef] [PubMed]
- Department of Statistics, Ministry of Transportation and Communications, Taiwan (ROC). 2016 National Travel Survey. Available online: https://www.motc.gov.tw/ch/home.jsp?id=56&parentpath=0%2C6&mcustomize=statistics101.jsp (accessed on 19 May 2022). (In Chinese)
- Available online: https://www.gvm.com.tw/article/68169 (accessed on 19 May 2022).
- Campus Security Report Center, Ministry of Education, Taiwan (ROC). Available online: https://csrc.edu.tw/FileManage/CheckData?sno=504&MergedId=83a8f152f88c4bf19f42317bd7f3eb2a (accessed on 19 May 2022). (In Chinese).
- The Control Yuan, Taiwan (ROC). Available online: https://www.cy.gov.tw/News_Content.aspx?n=213&s=7584 (accessed on 16 May 2022). (In Chinese)
- Lin, M.R.; Chang, S.H.; Pai, L.; Keyl, P.M. A longitudinal study of risk factors for motorcycle crashes among junior college students in Taiwan. Accid. Anal. Prev. 2003, 35, 243–252. [Google Scholar] [CrossRef]
- Chumpawadee, U.; Homchampa, P.; Thongkrajai, P.; Suwanimitr, A.; Chadbunchachai, W. Factors related to motorcycle accident risk behavior among university students in northeastern Thailand. Southeast Asian J. Trop. Med. Public Health 2015, 46, 805–821. [Google Scholar]
- Lin, M.R.; Chang, S.H.; Huang, W.; Hwang, H.F.; Pai, L. Factors associated with severity of motorcycle injuries among young adult riders. Ann. Emerg. Med. 2003, 41, 783–791. [Google Scholar] [CrossRef]
- Rhee, K.A.; Kim, J.K.; Lee, Y.I.; Ulfarsson, G.F. Spatial regression analysis of traffic crashes in Seoul. Accid. Anal. Prev. 2016, 91, 190–199. [Google Scholar] [CrossRef]
- Warsh, J.; Rothman, L.; Slater, M.; Steverango, C.; Howard, A. Are school zones effective? An examination of motor vehicle versus child pedestrian crashes near schools. Inj. Prev. 2009, 15, 226–229. [Google Scholar] [CrossRef]
- Wang, Y.Y.; Haque, M.M.; Chin, H.C.; Yun, J.G. Injury severity of pedestrian crashes in Singapore. In Proceedings of the Australasian Transport Research Forum 2013, Brisbane, Australia, 2–4 October 2013. [Google Scholar]
- Lin, C.L. A Study of the Integration of the Interface between Cheng-Kung University Campus and Urban Space. Master’s Thesis, National Cheng Kung University, Tainan, Taiwan, 2006. (In Chinese). [Google Scholar]
- Verzosa, N.; Miles, R. Severity of road crashes involving pedestrians in Metro Manila, Philippines. Accid. Anal. Prev. 2016, 94, 216–226. [Google Scholar] [CrossRef]
- Establishment and Application of Traffic Accident Injury Data Collection System (2/2). Available online: https://www.iot.gov.tw/cp-78-12430-1759c-1.html (accessed on 19 May 2022). (In Chinese)
- Ministry of Education, Taiwan (ROC). Available online: https://stats.moe.gov.tw/files/investigate/high_graduate/106/106_graduate.pdf (accessed on 19 May 2022). (In Chinese)
- Hot Spots around the School. Available online: https://roadsafety.tw/SchoolHotSpots (accessed on 19 May 2022).
- Lin, M.R.; Kraus, J.F. A review of risk factors and patterns of motorcycle injuries. Accid. Anal. Prev. 2009, 41, 710–722. [Google Scholar] [CrossRef] [PubMed]
- Fan, H.P.; Chiu, W.T.; Lin, M.R. Effects of helmet nonuse and seating position on patterns and severity of injuries in child motorcycle passengers. BMC Public Health 2019, 19, 1070. [Google Scholar] [CrossRef]
- Google Maps Platform. Available online: https://cloud.google.com/maps-platform/ (accessed on 19 May 2022).
- Taiwan Geospatial One-Stop Portal. Available online: https://www.tgos.tw/TGOS/Web/TGOS_Home.aspx (accessed on 19 May 2022). (In Chinese).
- Jeng, I.L. A Study of Interaction between Campus and District Environment—Analysis of Students Daily Activities in the National Taiwan Normal University. Master’s Thesis, National Taiwan University of Science and Technology, Taipei, Taiwan, 1999. (In Chinese). [Google Scholar]
- Li, C.K. The Industrial Spatial Cluster around the University. Master’s Thesis, National Cheng Kung University, Tainan, Taiwan, 2012. (In Chinese). [Google Scholar]
- Wei, C.H. A Study of the Relation among College Students’ Lifestyles and Cultural Consumption—Case Study of NTNU Commercial Area. Master’s Thesis, National Taiwan Normal University, Taipei, Taiwan, 2006. (In Chinese). [Google Scholar]
- Yang, C.Y.; Chiu, J.F.; Lin, M.C.; Cheng, M.F. Geographic variations in mortality from motor vehicle crashes in Taiwan. J. Trauma 1997, 43, 74–77. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.Y.; Hung, Y.T.; Chuang, Y.L.; Chen, Y.J.; Weng, W.S.; Liu, J.S.; Liang, K.Y. Incorporating development stratification of Taiwan townships into sampling design of large scale health interview survey. J. Health Manag. 2006, 4, 1–22. (In Chinese) [Google Scholar] [CrossRef]
- Lin, Y.H.; Chen, Y.C.; Tseng, Y.H.; Lin, M.H.; Hwang, S.J.; Chen, T.J.; Chou, L.F. Trend of urban-rural disparities in hospice utilization in Taiwan. PLoS ONE 2013, 8, e62492. [Google Scholar] [CrossRef]
- Baker, S.P.; O’Neill, B.; Haddon, W., Jr.; Long, W.B. The injury severity score: A method for describing patients with multiple injuries and evaluating emergency care. J. Trauma 1974, 14, 187–196. [Google Scholar] [CrossRef]
- Gennarelli, T.A.; Wodzin, E.; Barrington, I.L.; Association for the Advancement of Automotive Medicine. Abbreviated Injury Scale 2005: Update 2008; Association for the Advancement of Automotive Medicine: Barrington, IL, USA, 2008. [Google Scholar]
- Clark, D.E.; Black, A.W.; Skavdahl, D.H.; Hallagan, L.D. Open-access programs for injury categorization using ICD-9 or ICD-10. Inj. Epidemiol. 2018, 5, 11. [Google Scholar] [CrossRef]
- Weichenthal, S.; Farrell, W.; Goldberg, M.; Joseph, L.; Hatzopoulou, M. Characterizing the impact of traffic and the built environment on near-road ultrafine particle and black carbon concentrations. Environ. Res. 2014, 132, 305–310. [Google Scholar] [CrossRef]
- Palmer, C. Major trauma and the injury severity score-where should we set the bar? Annu. Proc. Assoc. Adv. Automot. Med. 2007, 51, 13–29. [Google Scholar]
- Stevenson, M.; Segui-Gomez, M.; Lescohier, I.; Di Scala, C.; McDonald-Smith, G. An overview of the injury severity score and the new injury severity score. Inj. Prev. 2001, 7, 10–13. [Google Scholar] [CrossRef]
- DiMaggio, C.; Ayoung-Chee, P.; Shinseki, M.; Wilson, C.; Marshall, G.; Lee, D.C.; Wall, S.; Maulana, S.; Pachter, H.L.; Frangos, S. Traumatic injury in the United States: In-patient epidemiology 2000–2011. Injury 2016, 47, 1393–1403. [Google Scholar] [CrossRef] [PubMed]
- Lam, C.; Wiratama, B.S.; Chang, W.H.; Chen, P.L.; Chiu, W.T.; Saleh, W.; Pai, C.W. Effect of motorcycle helmet types on head injuries: Evidence from eight level-I trauma centres in Taiwan. BMC Public Health 2020, 20, 78. [Google Scholar] [CrossRef] [PubMed]
- Mickey, R.M.; Greenland, S. The impact of confounder selection criteria on effect estimation. Am. J. Epidemiol. 1989, 129, 125–137. [Google Scholar] [CrossRef]
- Maldonado, G.; Greenland, S. Simulation study of confounder-selection strategies. Am. J. Epidemiol. 1993, 138, 923–936. [Google Scholar] [CrossRef]
- Pai, C.W.; Chen, P.L. Evaluation of injuries sustained by motorcyclists in approach-turn crashes in Taiwan. Accid. Anal. Prev. 2019, 124, 33–39. [Google Scholar] [CrossRef]
- Chan, T.C.; Pai, C.W.; Wu, C.C.; Hsu, J.C.; Chen, R.J.; Chiu, W.T.; Lam, C. Association of air pollution and weather factors with traffic injury severity: A study in Taiwan. Int. J. Environ. Res. Public Health 2022, 19, 7442. [Google Scholar] [CrossRef]
- Puratmaja, Y.; Handayani, L.; Sunardi, K.S. Factors associated with motorcycle risk behavior in Thai university students, Khon Kaen. Int. J. Eval. Res. Educ. 2017, 6, 270–276. [Google Scholar] [CrossRef][Green Version]
- Cheng, W.; Gill, G.S.; Sakrani, T.; Dasu, M.; Zhou, J. Predicting motorcycle crash injury severity using weather data and alternative Bayesian multivariate crash frequency models. Accid. Anal. Prev. 2017, 108, 172–180. [Google Scholar] [CrossRef]
- Li, X.; Liu, J.; Zhang, Z.; Parrish, A.; Jones, S. A spatiotemporal analysis of motorcyclist injury severity: Findings from 20 years of crash data from Pennsylvania. Accid. Anal. Prev. 2021, 151, 105952. [Google Scholar] [CrossRef]
- Quddus, M.A.; Noland, R.B.; Chin, H.C. An analysis of motorcycle injury and vehicle damage severity using ordered probit models. J. Saf. Res. 2002, 33, 445–462. [Google Scholar] [CrossRef]
- Abdul Manan, M.M.; Várhelyi, A.; Çelik, A.K.; Hashim, H.H. Road characteristics and environment factors associated with motorcycle fatal crashes in Malaysia. IATSS Res. 2018, 42, 207–220. [Google Scholar] [CrossRef]
- Pervez, A.; Lee, J.; Huang, H. Identifying factors contributing to the motorcycle crash severity in Pakistan. J. Adv. Transp. 2021, 2021, 6636130. [Google Scholar] [CrossRef]
- Jing Chuan Child Safety Foundation. Available online: https://www.safe.org.tw/key_report/research_detail/90?key_id=648 (accessed on 18 May 2022). (In Chinese).
- Thompson, J.; Baldock, M.; Lindsay, T. Motorcycle crashes resulting in hospital admissions in South Australia: Crash characteristics and injury patterns. J. Road Saf. 2020, 31, 10–19. [Google Scholar] [CrossRef]
- Beak, T.H.; Park, B.H. Safety evaluation of flashing yellow operation at night. J. Korean Soc. Transp. 2013, 31, 16–25. [Google Scholar] [CrossRef][Green Version]
- Office of Safety, Federal Highway Administration, United States. Removal of Signal Flashing Mode during Late-Night/Early-Morning Operation. Available online: https://rosap.ntl.bts.gov/view/dot/42543 (accessed on 19 May 2022).
- Polanis, S.F. Right-angle crashes and late-night/early-morning flashing operation: 19 case studies. ITE J. 2002, 72, 26–28. [Google Scholar]
- Pai, C.W.; Saleh, W. Modelling motorcyclist injury severity by various crash types at T-junctions in the UK. Saf. Sci. 2008, 46, 1234–1247. [Google Scholar] [CrossRef]
- Petit, L.; Zaki, T.; Hsiang, W.; Leslie, M.P.; Wiznia, D.H. A review of common motorcycle collision mechanisms of injury. EFORT Open Rev. 2020, 5, 544–548. [Google Scholar] [CrossRef]
- Chang, Y.H.; Li, C.Y.; Lu, T.H.; Artanti, K.D.; Hou, W.H. Risk of injury and mortality among driver victims involved in single-vehicle crashes in Taiwan: Comparisons between vehicle types. Int. J. Environ. Res. Public Health 2020, 17, 4687. [Google Scholar] [CrossRef]
- Ooi, S.; Wong, S.; Yeap, J.; Umar, R. Relationship between cervical spine injury and helmet use in motorcycle road crashes. Asia Pac. J. Public Health 2011, 23, 608–619. [Google Scholar] [CrossRef]
- Savolainen, P.; Mannering, F. Probabilistic models of motorcyclists’ injury severities in single- and multi-vehicle crashes. Accid. Anal. Prev. 2007, 39, 955–963. [Google Scholar] [CrossRef]
- Nunn, S. Death by motorcycle: Background, behavioral, and situational correlates of fatal motorcycle collisions. J. Forensic Sci. 2011, 56, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Waseem, M.; Ahmed, A.; Saeed, T.U. Factors affecting motorcyclists’ injury severities: An empirical assessment using random parameters logit model with heterogeneity in means and variances. Accid. Anal. Prev. 2019, 123, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Shajith, S.L.A.; Pasindu, H.R.; Ranawaka, R.K.T.K. Evaluating the risk factors in fatal accidents involving motorcycle—Case study on motorcycle accidents in Sri Lanka. Engineer 2019, 52, 33–42. [Google Scholar] [CrossRef]
- Shaheed, M.S.; Gkritza, K. An exploratory multinomial logit analysis of single-vehicle motorcycle accident severity. Anal. Methods Accid. Res. 2014, 2, 30–38. [Google Scholar] [CrossRef]
- Haworth, N.; Rowden, P. Fatigue in motorcycle crashes: Is there an issue? In 2006 Australasian Road Safety Research, Policing and Education Conference Proceedings; Able Video & Multimedia Pty Ltd.: Gold Coast, Australia, 2006. [Google Scholar]
- Shin, D.S.; Byun, J.H.; Jeong, B.Y. Crashes and traffic signal violations caused by commercial motorcycle couriers. Saf. Health Work 2019, 10, 213–218. [Google Scholar] [CrossRef]
- Aidoo, E.N.; Amoh-Gyimah, R. Modelling the risk factors for injury severity in motorcycle users in Ghana. J. Public Health (Berl.) 2020, 28, 199–209. [Google Scholar] [CrossRef]
- Abrari Vajari, M.; Aghabayk, K.; Sadeghian, M.; Shiwakoti, N. A multinomial logit model of motorcycle crash severity at Australian intersections. J. Saf. Res. 2020, 73, 17–24. [Google Scholar] [CrossRef]
- Pai, C.W.; Saleh, W. An analysis of motorcyclist injury severity under various traffic control measures at three-legged junctions in the UK. Saf. Sci. 2007, 45, 832–847. [Google Scholar] [CrossRef]
- Lam, C.; Chen, C.I.; Chuang, C.C.; Wu, C.C.; Yu, S.H.; Chang, K.K.; Chiu, W.T. Improving the timeliness and accuracy of injury severity data in road traffic accidents in an emerging economy setting. Int. J. Qual. Health Care 2019, 31, 140–146. [Google Scholar] [CrossRef]
- Gómez-García, L.; Hidalgo-Solórzano, E.; Pérez-Núñez, R.; Jacobo-Zepeda, V.F.; Ascencio-Tene, R.G.; Lunnen, J.C.; Mehmood, A. Factors associated with the severity of road traffic injuries from emergency department based surveillance system in two Mexican cities. BMC Emerg. Med. 2022, 22, 20. [Google Scholar] [CrossRef]
- Alanazy, A.R.M.; Wark, S.; Fraser, J.; Nagle, A. Factors impacting patient outcomes associated with use of emergency medical services operating in urban versus rural areas: A systematic review. Int. J. Environ. Res. Public Health 2019, 16, 1728. [Google Scholar] [CrossRef] [PubMed]
- Rusli, R.; Oviedo-Trespalacios, O.; Abd Salam, S.A. Risky riding behaviours among motorcyclists in Malaysia: A roadside survey. Transp. Res. Part F Traffic Psychol. Behav. 2020, 74, 446–457. [Google Scholar] [CrossRef]
- Hsu, T.P.; Sadullah, A.; Nguyen, X.D. A comparative study on motorcycle traffic development of Taiwan, Malaysia and Vietnam. J. Eastern Asia Soc. Trans. Stud. 2003, 5, 179–193. [Google Scholar]
- Department of Statistics, Ministry of Transportation and Communications, Taiwan (ROC). Available online: https://www.motc.gov.tw/ch/home.jsp?id=56&parentpath=0,6 (accessed on 19 May 2022). (In Chinese)
- Saadat, S.; Soori, H. Epidemiology of traffic injuries and motor vehicles utilization in the Capital of Iran: A population based study. BMC Public Health 2011, 11, 488. [Google Scholar] [CrossRef]
- Xuequn, Y.; Ke, L.; Ivers, R.; Du, W.; Senserrick, T. Prevalence rates of helmet use among motorcycle riders in a developed region in China. Accid. Anal. Prev. 2011, 43, 214–219. [Google Scholar] [CrossRef]
- De Oliveira, N.L.; de Sousa, R.M. Risk for injuries among motorcyclists involved in traffic incidents. Rev. Esc. Enferm. USP 2012, 46, 1133–1140. [Google Scholar] [CrossRef]
- Chang, H.L.; Shih, C.K. Using a multidimensional Rasch model approach to measure the police’s perceived ability to detect, detain and intercept DWI vehicles when conducting sobriety checkpoints. Accid. Anal. Prev. 2012, 48, 505–517. [Google Scholar] [CrossRef]
- Huang, C.Y.; Chou, S.E.; Su, W.T.; Liu, H.T.; Hsieh, T.M.; Hsu, S.Y.; Hsieh, H.Y.; Hsieh, C.H. Effect of lowering the blood alcohol concentration limit to 0.03 among hospitalized trauma patients in southern Taiwan: A cross-sectional analysis. Risk Manag. Healthc. Policy 2020, 13, 571–581. [Google Scholar] [CrossRef]
- Nguyen, D.V.M.; Vu, A.T.; Polders, E.; Ross, V.; Brijs, T.; Wets, G.; Brijs, K. Modeling the injury severity of small-displacement motorcycle crashes in Hanoi City, Vietnam. Saf. Sci. 2021, 142, 105371. [Google Scholar] [CrossRef]
- Se, C.; Champahom, T.; Jomnonkwao, S.; Chaimuang, P.; Ratanavaraha, V. Empirical comparison of the effects of urban and rural crashes on motorcyclist injury severities: A correlated random parameters ordered probit approach with heterogeneity in means. Accid. Anal. Prev. 2021, 161, 106352. [Google Scholar] [CrossRef]
- Isa, M.H.; Jawa, Z.M.; Sarani, R.; Wong, S.V. Injury severity analysis of accidents involving young motorcycle riders in Malaysia. J. Eastern Asia Soc. Trans. Stud. 2011, 9, 1997–2010. [Google Scholar] [CrossRef]
- Chiu, W.T.; Kuo, C.Y.; Hung, C.C.; Chen, M. The effect of the Taiwan motorcycle helmet use law on head injuries. Am. J. Public Health 2000, 90, 793–796. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | ISS < 8 (n = 4 238) | ISS ≥ 8 (n = 513) | Simple Logistic Regression | |||
|---|---|---|---|---|---|---|
| n | % | n | % | OR (95% CI) | p Value | |
| Sex | ||||||
| Men | 2634 | 90.30 | 283 | 9.70 | 0.749 (0.623–0.901) | 0.002 |
| Women | 1604 | 87.46 | 230 | 12.54 | 1.335 (1.110–1.605) | 0.002 |
| Age group (year) | ||||||
| <24 | 1714 | 90.78 | 174 | 9.22 | 0.756 (0.623–0.917) | 0.004 |
| 25–44 | 1476 | 91.17 | 143 | 8.83 | 0.723 (0.590–0.886) | 0.002 |
| 45–64 | 842 | 85.22 | 146 | 14.78 | 1.605 (1.306–1.972) | <0.0001 |
| ≥65 | 206 | 80.47 | 50 | 19.53 | 2.114 (1.529–2.921) | <0.0001 |
| Drunk driving | ||||||
| No | 4213 | 89.33 | 503 | 10.67 | 0.298 (0.142–0.625) | 0.001 |
| Yes | 25 | 71.43 | 10 | 28.57 | 3.352 (1.601–7.019) | 0.001 |
| Cylinder capacity (cc) | ||||||
| <250 | 4200 | 89.21 | 508 | 10.79 | 0.919 (0.360–2.346) | 0.860 |
| ≥250 | 38 | 88.37 | 5 | 11.63 | 1.088 (0.426–2.776) | 0.860 |
| License status | ||||||
| Licensed | 4024 | 89.48 | 473 | 10.52 | 0.629 (0.443–0.893) | 0.010 |
| Unlicensed | 214 | 84.25 | 40 | 15.75 | 1.590 (1.120–2.258) | 0.010 |
| Weather | ||||||
| Fine | 3001 | 88.53 | 389 | 11.47 | 1.293 (1.045–1.599) | 0.018 |
| Adverse | 1 237 | 90.89 | 124 | 9.11 | 0.773 (0.625–0.957) | 0.018 |
| Day of the week | ||||||
| Weekday | 2955 | 89.03 | 364 | 10.97 | 1.061 (0.867–1.298) | 0.567 |
| Weekend | 1 283 | 89.59 | 149 | 10.41 | 0.943 (0.771–1.153) | 0.567 |
| Time of crash | ||||||
| 12:00 a.m.–3:59 a.m. | 181 | 87.44 | 26 | 12.56 | 1.197 (0.785–1.824) | 0.404 |
| 4:00 a.m.–7:59 a.m. | 378 | 86.10 | 61 | 13.90 | 1.379 (1.034–1.838) | 0.029 |
| 8:00 a.m.–11:59 a.m. | 1147 | 89.82 | 130 | 10.18 | 0.915 (0.741–1.129) | 0.406 |
| 12:00 p.m.–3:59 p.m. | 831 | 88.31 | 110 | 11.69 | 1.119 (0.894–1.400) | 0.325 |
| 4:00 p.m.–7:59 p.m. | 966 | 89.94 | 108 | 10.06 | 0.903 (0.722–1.130) | 0.373 |
| 8:00 p.m.–11:59 p.m. | 735 | 90.41 | 78 | 9.59 | 0.855 (0.663–1.101) | 0.225 |
| Rush hour | ||||||
| Yes (7:00 a.m.–9:59 a.m.; 6:00 p.m.–8:59 p.m.) | 1564 | 90.20 | 170 | 9.80 | 0.847 (0.698–1.029) | 0.095 |
| No (10:00 a.m.–5:59 p.m.; 9:00 p.m.–6:59 a.m.) | 2674 | 88.63 | 343 | 11.37 | 1.180 (0.972–1.433) | 0.095 |
| Speed limit (km/h) | ||||||
| ≤50 | 4175 | 89.23 | 504 | 10.77 | 0.845 (0.418–1.709) | 0.639 |
| >50 | 63 | 87.50 | 9 | 12.50 | 1.183 (0.585–2.394) | 0.639 |
| Road alignment | ||||||
| Straight road | 1712 | 89.82 | 194 | 10.18 | 0.897 (0.743–1.084) | 0.260 |
| Curved road | 86 | 86.00 | 14 | 14.00 | 1.355 (0.765–2.402) | 0.298 |
| Crossroad/Roundabout | 2440 | 88.89 | 305 | 11.11 | 1.081 (0.897–1.302) | 0.416 |
| Road surface | ||||||
| Dry | 3480 | 88.89 | 435 | 11.11 | 1.215 (0.943–1.565) | 0.133 |
| Wet/Slippery | 758 | 90.67 | 78 | 9.33 | 0.823 (0.639–1.061) | 0.133 |
| Sight | ||||||
| Good | 4176 | 89.21 | 505 | 10.79 | 0.937 (0.446–1.968) | 0.864 |
| Bad | 62 | 88.57 | 8 | 11.43 | 1.067 (0.508–2.241) | 0.864 |
| Signal status | ||||||
| Normal | 1707 | 89.00 | 211 | 11.00 | 1.036 (0.860–1.248) | 0.710 |
| Flashing | 147 | 79.89 | 37 | 20.11 | 2.163 (1.490–3.141) | <0.0001 |
| No | 2384 | 90.00 | 265 | 10.00 | 0.831 (0.692–0.998) | 0.048 |
| Collision partner | ||||||
| Pedestrian | 137 | 91.33 | 13 | 8.67 | 0.778 (0.437–1.385) | 0.394 |
| Vehicle | 3855 | 89.48 | 453 | 10.52 | 0.750 (0.562–1.001) | 0.051 |
| None | 246 | 83.96 | 47 | 16.04 | 1.637 (1.181–2.268) | 0.003 |
| Road width (m) median (IQR) | 10 | (11) | 11 | (11) | 0.994 (0.984–1.005) | 0.281 |
| Time to hospital (min) median (IQR) | 33 | (38) | 28 | (14) | 0.984 (0.972–0.995) | 0.005 |
| Variables | β | SE | OR | 95% CI | p Value |
|---|---|---|---|---|---|
| Sex | |||||
| Men | Reference | ||||
| Women | 0.274 | 0.097 | 1.315 | 1.087–1.592 | 0.005 |
| Age group (year) | |||||
| <24 | 0.083 | 0.121 | 1.086 | 0.857–1.376 | 0.493 |
| 25–44 | Reference | ||||
| 45–64 | 0.560 | 0.127 | 1.751 | 1.365–2.247 | <0.001 |
| ≥65 | 0.935 | 0.184 | 2.547 | 1.776–3.653 | <0.001 |
| Drunk driving | |||||
| No | Reference | ||||
| Yes | 1.071 | 0.391 | 2.918 | 1.355–6.281 | 0.006 |
| Weather | |||||
| Fine | Reference | ||||
| Adverse | −0.250 | 0.111 | 0.779 | 0.626–0.969 | 0.025 |
| Time of crash | |||||
| 12:00 a.m.–3:59 a.m. | 0.359 | 0.238 | 1.432 | 0.899–2.282 | 0.131 |
| 4:00 a.m.–7:59 a.m. | 0.342 | 0.170 | 1.408 | 1.010–1.963 | 0.043 |
| 8:00 a.m.–11:59 a.m. | Reference | ||||
| 12:00 p.m.–3:59 p.m. | 0.182 | 0.139 | 1.200 | 0.913–1.577 | 0.191 |
| 4:00 p.m.–7:59 p.m. | 0.028 | 0.140 | 1.028 | 0.782–1.353 | 0.841 |
| 8:00 p.m.–11:59 p.m. | 0.047 | 0.156 | 1.048 | 0.772–1.421 | 0.765 |
| Signal status | |||||
| Normal | Reference | ||||
| Flashing | 0.677 | 0.203 | 1.968 | 1.324–2.927 | 0.001 |
| None | −0.166 | 0.100 | 0.847 | 0.697–1.030 | 0.096 |
| Collision partner | |||||
| Pedestrian | Reference | ||||
| Vehicle | 0.217 | 0.299 | 1.242 | 0.691–2.232 | 0.469 |
| None | 0.765 | 0.336 | 2.150 | 1.112–4.155 | 0.023 |
| Time to hospital (per 10 min) | −0.001 | 0.001 | 0.987 | 0.976–0.998 | 0.018 |
| Variables | β | SE | OR | 95% CI | p Value |
|---|---|---|---|---|---|
| Sex | |||||
| Men | Reference | ||||
| Women | 0.441 | 0.167 | 1.555 | 1.121–2.157 | 0.008 |
| Time of crash | |||||
| 12:00 a.m.–3:59 a.m. | 0.749 | 0.335 | 2.116 | 1.096–4.083 | 0.026 |
| 4:00 a.m.–7:59 a.m. | 0.586 | 0.364 | 1.797 | 0.881–3.667 | 0.107 |
| 8:00 a.m.–11:59 a.m. | Reference | ||||
| 12:00 p.m.–3:59 p.m. | 0.559 | 0.244 | 1.749 | 1.085–2.819 | 0.022 |
| 4:00 p.m.–7:59 p.m. | 0.180 | 0.266 | 1.198 | 0.711–2.016 | 0.497 |
| 8:00 p.m.–11:59 p.m. | 0.210 | 0.264 | 1.233 | 0.735–2.071 | 0.427 |
| Signal status | |||||
| Normal | Reference | ||||
| Flashing | 1.069 | 0.297 | 2.913 | 1.628–5.213 | <0.001 |
| None | −0.047 | 0.174 | 0.954 | 0.679–1.342 | 0.788 |
| Time to hospital (per 10 min) | −0.002 | 0.001 | 0.976 | 0.954–0.999 | 0.038 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, H.-Y.; Li, J.-S.; Pai, C.-W.; Chien, W.-C.; Huang, W.-C.; Hsu, C.-W.; Wu, C.-C.; Yu, S.-H.; Chiu, W.-T.; Lam, C. Environmental Factors Associated with Severe Motorcycle Crash Injury in University Neighborhoods: A Multicenter Study in Taiwan. Int. J. Environ. Res. Public Health 2022, 19, 10274. https://doi.org/10.3390/ijerph191610274
Lin H-Y, Li J-S, Pai C-W, Chien W-C, Huang W-C, Hsu C-W, Wu C-C, Yu S-H, Chiu W-T, Lam C. Environmental Factors Associated with Severe Motorcycle Crash Injury in University Neighborhoods: A Multicenter Study in Taiwan. International Journal of Environmental Research and Public Health. 2022; 19(16):10274. https://doi.org/10.3390/ijerph191610274
Chicago/Turabian StyleLin, Heng-Yu, Jian-Sing Li, Chih-Wei Pai, Wu-Chien Chien, Wen-Cheng Huang, Chin-Wang Hsu, Chia-Chieh Wu, Shih-Hsiang Yu, Wen-Ta Chiu, and Carlos Lam. 2022. "Environmental Factors Associated with Severe Motorcycle Crash Injury in University Neighborhoods: A Multicenter Study in Taiwan" International Journal of Environmental Research and Public Health 19, no. 16: 10274. https://doi.org/10.3390/ijerph191610274
APA StyleLin, H.-Y., Li, J.-S., Pai, C.-W., Chien, W.-C., Huang, W.-C., Hsu, C.-W., Wu, C.-C., Yu, S.-H., Chiu, W.-T., & Lam, C. (2022). Environmental Factors Associated with Severe Motorcycle Crash Injury in University Neighborhoods: A Multicenter Study in Taiwan. International Journal of Environmental Research and Public Health, 19(16), 10274. https://doi.org/10.3390/ijerph191610274