
The Effect of Binaural Beat Audio on Operative Pain and Anxiety in Cataract Surgery under Topical Anaesthesia: A Randomized Controlled Trial

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
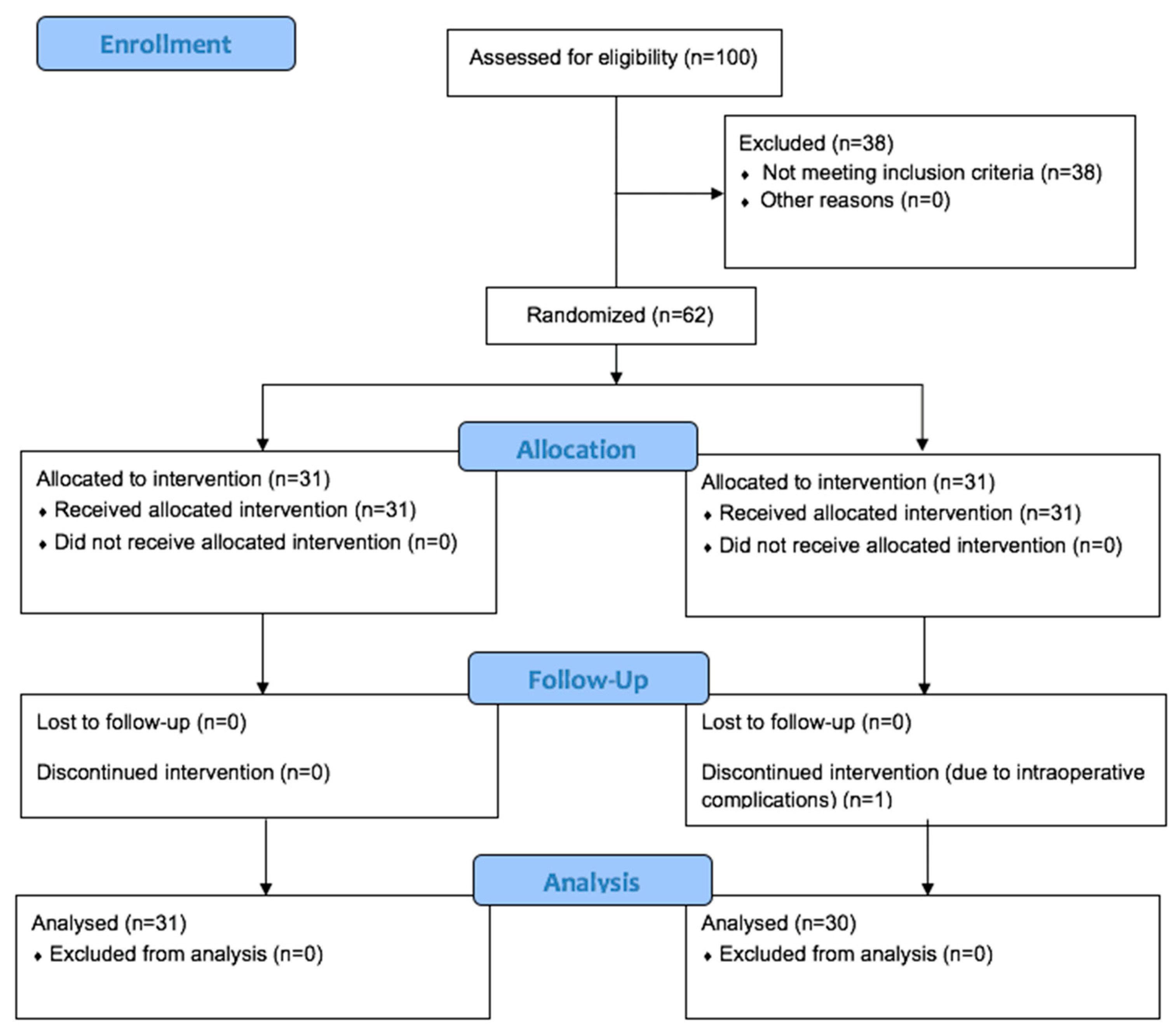
2.1. Participants
2.2. Sample Size Calculation
2.3. Subjective Assessment of Pain
2.4. Subjective Assessment of Anxiety
2.5. Objective Assessment of Pain and Anxiety
2.6. Interventions
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhao, L.Q.; Zhu, H.; Zhao, P.Q.; Wu, Q.R.; Hu, Y.Q. Topical anesthesia versus regional anesthesia for cataract surgery: A meta-analysis of randomized controlled trials. Ophthalmology 2012, 119, 659–667. [Google Scholar] [CrossRef]
- Stupp, T.; Hassouna, I.; Soppart, K.; Thanos, S.; Forster, W. Systemic adverse events: A comparison between topical and peribulbar anaesthesia in cataract surgery. Ophthalmologica 2007, 221, 320–325. [Google Scholar] [CrossRef]
- Malik, A.; Fletcher, E.C.; Chong, V.; Dasan, J. Local anesthesia for cataract surgery. J. Cataract Refract. Surg. 2010, 36, 133–152. [Google Scholar] [CrossRef] [PubMed]
- Guay, J.; Sales, K. Sub-Tenon’s anaesthesia versus topical anaesthesia for cataract surgery. Cochrane Database Syst. Rev. 2015, 8, CD006291. [Google Scholar] [CrossRef] [PubMed]
- Manners, T.D.; Burton, R.L. Randomised trial of topical versus sub-Tenon’s local anaesthesia for small-incision cataract surgery. Eye 1996, 10, 367–370. [Google Scholar] [CrossRef]
- Srinivasan, S.; Fern, A.I.; Selvaraj, S.; Hasan, S. Randomized double-blind clinical trial comparing topical and sub-Tenon’s anaesthesia in routine cataract surgery. Br. J. Anaesth. 2004, 93, 683–686. [Google Scholar] [CrossRef]
- Ruschen, H.; Celaschi, D.; Bunce, C.; Carr, C. Randomised controlled trial of sub-Tenon’s block versus topical anaesthesia for cataract surgery: A comparison of patient satisfaction. Br. J. Ophthalmol. 2005, 89, 291–293. [Google Scholar] [CrossRef][Green Version]
- Ezra, D.G.; Allan, B.D. Topical anaesthesia alone versus topical anaesthesia with intracameral lidocaine for phacoemulsification. Cochrane Database Syst. Rev. 2007, 3, CD005276. [Google Scholar]
- Ho, A.L.; Zakrzewski, P.A.; Braga-Mele, R. The effect of combined topical-intracameral anaesthesia on neuroleptic requirements during cataract surgery. Can. J. Ophthalmol. 2010, 45, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Ploghaus, A.; Narain, C.; Beckmann, C.F.; Clare, S.; Bantick, S.; Wise, R.; Matthews, P.M.; Rawlins, J.N.P.; Tracey, I. Exacerbation of pain by anxiety is associated with activity in a hippocampal network. J. Neurosci. 2001, 21, 9896–9903. [Google Scholar] [CrossRef] [PubMed]
- Habib, N.E.; Mandour, N.M.; Balmer, H.G. Effect of midazolam on anxiety level and pain perception in cataract surgery with topical anesthesia. J. Cataract Refract. Surg. 2004, 30, 437–443. [Google Scholar] [CrossRef]
- Oohashi, T.; Nishina, E.; Honda, M.; Yonekura, Y.; Fuwamoto, Y.; Kawai, N.; Maekawa, T.; Nakamura, S.; Fukuyama, H.; Shibasaki, H. Inaudible high-frequency sounds affect brain activity: Hypersonic effect. J. Neurophysiol. 2000, 83, 3548–3558. [Google Scholar] [CrossRef] [PubMed]
- Jancke, L.; Alahmadi, N. Detection of independent functional networks during music listening using electroencephalogram and sLORETA-ICA. Neuroreport 2016, 27, 455–461. [Google Scholar] [CrossRef]
- Nakamura, S.; Sadato, N.; Oohashi, T.; Nishina, E.; Fuwamoto, Y.; Yonekura, Y. Analysis of music-brain interaction with simultaneous measurement of regional cerebral blood flow and electroencephalogram beta rhythm in human subjects. Neurosci. Lett. 1999, 275, 222–226. [Google Scholar] [CrossRef]
- Bruya, M.A.; Severtsen, B. Evaluating the effects of music on electroencephalogram patterns of normal subject. J. Neurosurg. Nurs. 1984, 16, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Dabu-Bondoc, S.; Vadivelu, N.; Benson, J.; Perret, D.; Kain, Z.N. Hemispheric synchronized sounds and perioperative analgesic requirements. Anesth. Analg. 2010, 110, 208–210. [Google Scholar] [CrossRef]
- Kliempt, P.; Ruta, D.; Ogston, S.; Landeck, A.; Martay, K. Hemispheric-synchronisation during anaesthesia: A double-blind randomised trial using audiotapes for intra-operative nociception control. Anaesthesia 1999, 54, 769–773. [Google Scholar] [CrossRef]
- Zampi, D.D. Efficacy of theta binaural reats for the treatment of chronic pain. Altern. Ther. Health Med. 2016, 22, 32–38. [Google Scholar]
- Garcia-Argibay, M.; Santed, M.A.; Reales, J.M. Efficacy of binaural auditory beats in cognition, anxiety, and pain perception: A meta-analysis. Psychol. Res. 2019, 83, 357–372. [Google Scholar] [CrossRef]
- Isik, B.K.; Esen, A.; Buyukerkmen, B.; Kilinc, A.; Menziletoglu, D. Effectiveness of binaural beats in reducing preoperative dental anxiety. Br. J. Oral Maxillofac. Surg. 2017, 55, 571–574. [Google Scholar] [CrossRef]
- Padmanabhan, R.; Hildreth, A.J.; Laws, D. A prospective, randomised, controlled study examining binaural beat audio and pre-operative anxiety in patients undergoing general anaesthesia for day case surgery. Anaesthesia 2005, 60, 874–877. [Google Scholar] [CrossRef]
- Licklider, J.C.R.; Webster, J.; Hedlun, J. On the frequency limits of binaural beats. Proc. Meet Acoust. 1950, 22, 468–473. [Google Scholar] [CrossRef]
- Tobias, J.V. Application of a “relative” procedure to a problem in binaural beat perception. J. Acoust. Soc. Am. 1963, 35, 1442–1447. [Google Scholar] [CrossRef]
- Lentz, J.J.; He, Y.; Townsend, J.T. A new perspective on binaural integration using response time methodology: Super capacity revealed in conditions of binaural masking release. Front. Hum. Neurosci. 2014, 8, 641. [Google Scholar] [CrossRef] [PubMed]
- Wiwatwongwana, D.; Vichitvejpaisal, P.; Thaikruea, L.; Klaphajone, J.; Tantong, A.; Wiwatwongwana, A. The effect of music with and without binaural beat audio on operative anxiety in patients undergoing cataract surgery: A randomized controlled trial. Eye 2016, 30, 1407. [Google Scholar] [CrossRef] [PubMed]
- Oster, G. Auditory beats in the brain. Sci. Am. 1973, 229, 94–102. [Google Scholar] [CrossRef]
- Haddadi, S.; Marzban, S.; Fazeli, B.; Heidarzadeh, A.; Parvizi, A.; Naderinabi, B.; Panah, M.R.P. Comparing the effect of topical anesthesia and retrobulbar block with intravenous sedation on hemodynamic changes and satisfaction in patients undergoing cataract surgery (phaco method). Anesth. Pain Med. 2015, 5, e24780. [Google Scholar] [CrossRef]
- Aslankurt, M.; Aslan, L.; Baskan, A.M.; Aksoy, A.; Silay, E.; Yildiz, H. Pain and cooperation in patients having dominant-side or nondominant-side phacoemulsification. J. Cataract Refract. Surg. 2014, 40, 199–202. [Google Scholar] [CrossRef]
- Sharma, N.S.; Ooi, J.L.; Figueira, E.C.; Rosenberg, M.L.; Masselos, K.; Papalkar, D.P.; Paramanathan, N.; Francis, I.C.; Alexander, S.L.; Ferch, N.I. Patient perceptions of second eye clear corneal cataract surgery using assisted topical anaesthesia. Eye 2008, 22, 547–550. [Google Scholar] [CrossRef]
- Scott, J.; Huskisson, E.C. Graphic representation of pain. Pain 1976, 2, 175–184. [Google Scholar] [CrossRef]
- Revill, S.I.; Robinson, J.O.; Rosen, M.; Hogg, M.I. The reliability of a linear analogue for evaluating pain. Anaesthesia 1976, 31, 1191–1198. [Google Scholar] [CrossRef]
- Ohnhaus, E.E.; Adler, R. Methodological problems in the measurement of pain: A comparison between the verbal rating scale and the visual analogue scale. Pain 1975, 1, 379–384. [Google Scholar] [CrossRef]
- Marteau, T.M.; Bekker, H. The development of a six-item short-form of the state scale of the Spielberger State-Trait Anxiety Inventory (STAI). Br. J. Clin. Psychol. 1992, 31, 301–306. [Google Scholar] [CrossRef]
- Tluczek, A.; Henriques, J.B.; Brown, R.L. Support for the reliability and validity of a six-item state anxiety scale derived from the State-Trait Anxiety Inventory. J. Nurs. Meas. 2009, 17, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Cavdar, A.U.; Yilmaz, E.; Baydur, H. The Effect of hand massage before cataract surgery on patient anxiety and comfort: A randomized controlled study. J. Perianesth. Nurs. 2020, 35, 54–59. [Google Scholar] [CrossRef]
- Tipotsch-Maca, S.M.; Varsits, R.M.; Ginzel, C.; Vecsei-Marlovits, P.V. Effect of a multimedia-assisted informed consent procedure on the information gain, satisfaction, and anxiety of cataract surgery patients. J. Cataract Refract. Surg. 2016, 42, 110–116. [Google Scholar] [CrossRef]
- Bee Seok, C.; Abd Hamid, H.S.; Mutang, J.A.; Ismail, R. Psychometric properties of the state-trait anxiety inventory (form Y) among Malaysian university students. Sustainability 2018, 10, 3311. [Google Scholar] [CrossRef]
- Vitasari, P.; Wahab, M.N.A.; Herawan, T.; Othman, A.; Sinnadurai, S.K. Re-test of State Trait Anxiety Inventory (STAI) among engineering students in Malaysia: Reliability and validity tests. Procedia Soc. Behav. Sci. 2011, 15, 3843–3848. [Google Scholar] [CrossRef]
- Jiang, L.; Zhang, K.; He, W.; Zhu, X.; Zhou, P.; Lu, Y. Perceived pain during cataract surgery with topical anesthesia: A comparison between first-eye and second-eye surgery. J. Ophthalmol. 2015, 2015, 383456. [Google Scholar] [CrossRef] [PubMed]
- Fichman, R.A. Use of topical anesthesia alone in cataract surgery. J. Cataract Refract. Surg. 1996, 22, 612–614. [Google Scholar] [CrossRef]
- Claoue, C.; Lanigan, C. Topical anaesthesia for cataract surgery. Aust. N. Z. J. Ophthalmol. 1997, 25, 265–268. [Google Scholar] [CrossRef]
- Jacobi, P.C.; Dietlein, T.S.; Jacobi, F.K. A comparative study of topical vs. retrobulbar anesthesia in complicated cataract surgery. Arch. Ophthalmol. 2000, 118, 1037–1043. [Google Scholar] [CrossRef]
- Chittenden, H.B.; Meacock, W.R.; Govan, J.A. Topical anaesthesia with oxybuprocaine versus sub-Tenon’s infiltration with 2% lignocaine for small incision cataract surgery. Br. J. Ophthalmol. 1997, 81, 288–290. [Google Scholar] [CrossRef][Green Version]
- Lewis, A.K.; Osborn, I.P.; Roth, R. The effect of hemispheric synchronization on intraoperative analgesia. Anesth. Analg. 2004, 98, 533–536. [Google Scholar] [CrossRef]
- Socea, S.D.; Abualhasan, H.; Magen, O.; Zayit-Soudry, S.; Blumenthal, E.Z.; Duvdevan, N.; Mimouni, M. Preoperative anxiety levels and pain during cataract surgery. Curr. Eye Res. 2020, 45, 471–476. [Google Scholar] [CrossRef]
- Wahbeh, H.; Calabrese, C.; Zwickey, H. Binaural beat technology in humans: A pilot study to assess psychologic and physiologic effects. J. Altern. Complement. Med. 2007, 13, 25–32. [Google Scholar] [CrossRef]
- Le Scouarnec, R.P.; Poirier, R.M.; Owens, J.E.; Gauthier, J.; Taylor, A.G.; Foresman, P.A. Use of binaural beat tapes for treatment of anxiety: A pilot study of tape preference and outcomes. Altern. Ther. Health Med. 2001, 7, 58–63. [Google Scholar] [PubMed]
- Ko, Y.L.; Lin, P.C. The effect of using a relaxation tape on pulse, respiration, blood pressure and anxiety levels of surgical patients. J. Clin. Nurs. 2012, 21, 689–697. [Google Scholar] [CrossRef] [PubMed]
- Smolen, D.; Topp, R.; Singer, L. The effect of self-selected music during colonoscopy on anxiety, heart rate, and blood pressure. Appl. Nurs. Res. 2002, 15, 126–136. [Google Scholar] [CrossRef]
- Kim, M.S.; Cho, K.S.; Woo, H.; Kim, J.H. Effects of hand massage on anxiety in cataract surgery using local anesthesia. J. Cataract Refract. Surg. 2001, 27, 884–890. [Google Scholar] [CrossRef]
- Kavak Akelma, F.; Altinsoy, S.; Arslan, M.T.; Ergil, J. Effect of favorite music on postoperative anxiety and pain. Anaesthesist 2020, 69, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Kelton, K.; Weaver, T.L.; Willoughby, L.; Kaufman, D.; Santowski, A. The efficacy of binaural beats as a stress-buffering technique. Altern. Ther. Health Med. 2020, 27, 28–33. [Google Scholar]
- McConnell, P.A.; Froeliger, B.; Garland, E.L.; Ives, J.C.; Sforzo, G.A. Auditory driving of the autonomic nervous system: Listening to theta-frequency binaural beats post-exercise increases parasympathetic activation and sympathetic withdrawal. Front. Psychol. 2014, 5, 1248. [Google Scholar] [CrossRef]
- Gkolias, V.; Amaniti, A.; Triantafyllou, A.; Papakonstantinou, P.; Kartsidis, P.; Paraskevopoulos, E.; Bamidis, P.D.; Hadjileontiadis, L.; Kouvelas, D. Reduced pain and analgesic use after acoustic binaural beats therapy in chronic pain-A double-blind randomized control cross-over trial. Eur. J. Pain 2020, 24, 1716–1729. [Google Scholar] [CrossRef] [PubMed]
- Bednarczuk, N.F.; Casanovas Ortega, M.; Fluri, A.S.; Arshad, Q. Vestibulo-cortical hemispheric dominance: The link between anxiety and the vestibular system? Eur. J. Neurosci. 2018, 47, 1517–1524. [Google Scholar] [CrossRef]
- Solca, M.; Mottaz, A.; Guggisberg, A.G. Binaural beats increase interhemispheric alpha-band coherence between auditory cortices. Hear Res. 2016, 332, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Cao, H.; Ming, D.; Qi, H.; Wang, X.; Wang, X.; Chen, R.; Zhou, P. Analysis of EEG activity in response to binaural beats with different frequencies. Int. J. Psychophysiol. 2014, 94, 399–406. [Google Scholar] [CrossRef]
- Cupo, G.; Scarinci, F.; Ripandelli, G.; Sampalmieri, M.; Giusti, C. Changes in vital signs during cataract phacoemulsification by using peribulbar or topical anesthesia. Clin. Ther. 2012, 163, e263–e267. [Google Scholar]
- Fernandes, M.B.; Souza, R.V.; Vasconcelos, G.C.; Ribeiro, K.G.; Andrade, B.B.; Fernandes, C.R. Assessing patient satisfaction with cataract surgery under topical anesthesia supplemented by intracameral lidocaine combined with sedation. Arq. Bras. Oftalmol. 2013, 76, 345–349. [Google Scholar] [CrossRef]
- Venkatakrishnan, J.V.; Kumar, C.M.; Ratra, V.; Viswanathan, J.; Jeyaraman, V.A.; Ragavendera, T. Effect of sedation on visual sensations in patients undergoing cataract surgery under topical anaesthesia: A prospective randomized masked trial. Acta Ophthalmol. 2013, 91, 247–250. [Google Scholar] [CrossRef]
- Aslan, L.; Aslankurt, M.; Cekic, O.; Aksoy, A.; Yildiz, H. The pain experience and cooperation of patients in consecutive cataract surgery. Eur. J. Ophthalmol. 2013, 23, 339–343. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Category | Overall n (%) | Control (n = 30) | Intervention (n =31) | p-Value | ||
|---|---|---|---|---|---|---|
| n (%) | Mean (SD) | n (%) | Mean (SD) | |||
| Age | 65.8 (7.9) | 63.9 (6.2) | 67.7 (9.0) | 0.069 ** | ||
| Gender | 0.15 * | |||||
| Male | 33 (54.1) | 19 (63.3) | 14 (45.2) | |||
| Female | 28 (45.9) | 11 (36.7) | 17 (54.8) | |||
| Study Variables | Time | Mean Difference (95% CI) | p-Value |
|---|---|---|---|
| Systolic BP | Baseline/pre | −3.18 (−11.58, 5.23) | 0.453 |
| Post | 9.22 (−0.71, 19.16) | 0.068 | |
| Diastolic BP | Baseline/pre | 1.64 (−3.27, 6.55) | 0.507 |
| Post | 7.40 (2.71, 12.09) | 0.003 | |
| MAP | Baseline/pre | −0.10 (−5.31, 5.12) | 0.970 |
| Post | 8.05 (2.28, 13.82) | 0.007 | |
| Heart rate | Baseline/pre | 5.02 (−1.41, 11.44) | 0.124 |
| Post | 12.53 (7.05, 18.02) | <0.001 | |
| Anxiety | Baseline/pre | −0.65 (−1.79, 0.50) | 0.265 |
| Post | 1.63 (0.42, 2.84) | 0.009 |
| Pain Score | Post- Systolic | Post-Diastolic | Post-MAP | Post- Heart Rate | Post-Anxiety |
|---|---|---|---|---|---|
| Control | r = 0.44 | r = 0.40 | r = 0.51 | r = 0.35 | r = 0.47 |
| p = 0.015 | p = 0.029 | p = 0.004 | p = 0.055 | p = 0.008 | |
| Experimental | r = −0.15 | r = 0.02 | r = −0.08 | r = 0.11 | r = 0.25 |
| p = 0.415 | p = 0.928 | p = 0.666 | p = 0.542 | p = 0.170 |
| Variables | Group | Pretest | Posttest | Time | Group | Time*Group | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | F | p-Value | η2 | F | p-Value | η2 | F | p-Value | η2 | ||
| Systolic | Con | 158.57 (11.31) | 166.90 (13.14) | 1.71 | 0.196 | 0.03 | 0.50 | 0.485 | 0.01 | 14.41 | <0.001 | 0.19 |
| Exp | 161.74 (20.14) | 157.68 (23.92) | ||||||||||
| Diastolic | Con | 82.80 (6.41) | 88.33 (7.25) | 8.36 | 0.005 | 0.12 | 4.16 | 0.046 | 0.07 | 9.84 | 0.003 | 0.14 |
| Exp | 81.16 (11.85) | 80.94 (10.66) | ||||||||||
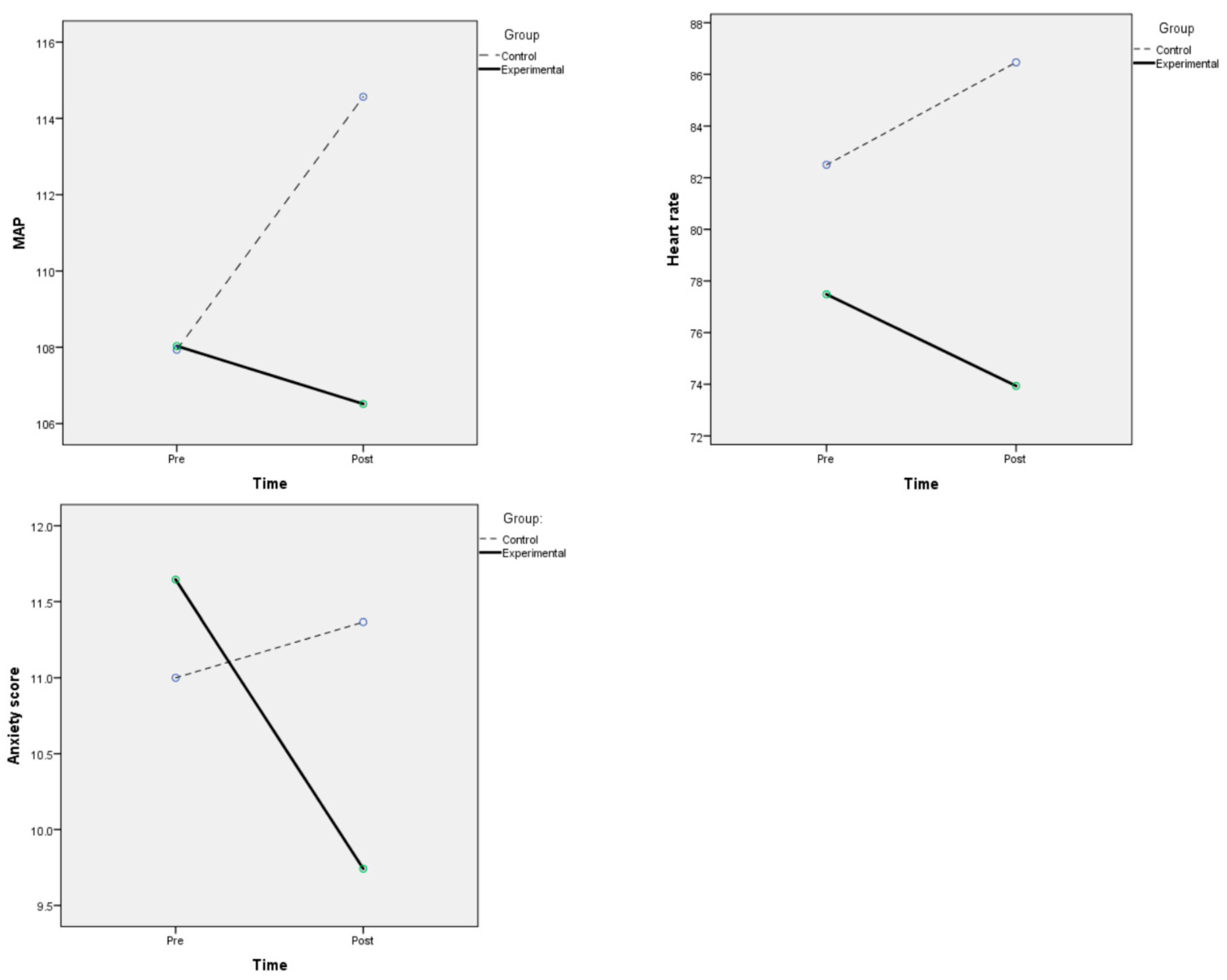
| MAP | Con | 107.93 (6.07) | 114.57 (7.54) | 5.95 | 0.018 | 0.09 | 2.44 | 0.123 | 0.04 | 15.09 | <0.001 | 0.20 |
| Exp | 108.03 (12.96) | 106.52 (13.93) | ||||||||||
| Heart rate | Con | 82.50 (11.19) | 86.47 (9.13) | 0.06 | 0.811 | 0.01 | 9.44 | 0.003 | 0.14 | 18.62 | <0.001 | 0.24 |
| Exp | 77.48 (13.71) | 73.94 (12.03) | ||||||||||
| Anxiety | Con | 11.00 (2.42) | 11.37 (2.11) | 10.23 | 0.002 | 0.15 | 0.83 | 0.366 | 0.01 | 22.32 | 0.001 | 0.27 |
| Exp | 11.65 (2.04) | 9.74 (2.58) | ||||||||||
| Variables | Group | Mean Difference Pretest-Posttest | 95% CI | p-Value |
|---|---|---|---|---|
| Systolic | Con | −8.33 | −12.23, −4.44 | <0.001 |
| Exp | 4.06 | −1.31, 9.44 | 0.133 | |
| Diastolic | Con | 5.53 | −8.20, −2.86 | <0.001 |
| Exp | 0.23 | −2.41, 2.86 | 0.862 | |
| MAP | Con | −6.63 | −9.29, −3.97 | <0.001 |
| Exp | 1.52 | −1.83, 4.86 | 0.362 | |
| Heart rate | Con | −3.97 | −6.70, −1.23 | <0.001 |
| Exp | 3.55 | 1.25, 5.84 | 0.004 | |
| Anxiety | Con | −0.37 | 0.93, −1.34 | 0.190 |
| Exp | 1.90 | 1.10, 2.70 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loong, L.J.; Ling, K.K.; Tai, E.L.M.; Kueh, Y.C.; Kuan, G.; Hussein, A. The Effect of Binaural Beat Audio on Operative Pain and Anxiety in Cataract Surgery under Topical Anaesthesia: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 10194. https://doi.org/10.3390/ijerph191610194
Loong LJ, Ling KK, Tai ELM, Kueh YC, Kuan G, Hussein A. The Effect of Binaural Beat Audio on Operative Pain and Anxiety in Cataract Surgery under Topical Anaesthesia: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(16):10194. https://doi.org/10.3390/ijerph191610194
Chicago/Turabian StyleLoong, Ling Jiunn, Koh Koon Ling, Evelyn Li Min Tai, Yee Cheng Kueh, Garry Kuan, and Adil Hussein. 2022. "The Effect of Binaural Beat Audio on Operative Pain and Anxiety in Cataract Surgery under Topical Anaesthesia: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 16: 10194. https://doi.org/10.3390/ijerph191610194
APA StyleLoong, L. J., Ling, K. K., Tai, E. L. M., Kueh, Y. C., Kuan, G., & Hussein, A. (2022). The Effect of Binaural Beat Audio on Operative Pain and Anxiety in Cataract Surgery under Topical Anaesthesia: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 19(16), 10194. https://doi.org/10.3390/ijerph191610194