
Contributing Factors in Whether Displaced Households Want to Receive Humanitarian Information from Humanitarian Actors: Iraq Multi-Cluster Needs Assessment

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Data Collection
2.2. Variables
2.3. Ethical Consideration
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bradley, S.; The Immediate Impact of the Pandemic on Geneva-Based Non-Governmental Organisations has been Restrained, a Survey Reveals. But NGOs Fear Tough Times Ahead Linked to Funding. Geneva: SWI. 2020. Available online: https://www.swissinfo.ch/eng/covid-19_geneva-ngos-face-uncertain-future-due-to-covid-19-funding-impact/45791450 (accessed on 8 April 2022).
- Hajjar, M.S.; Abu-Sittah, G.S. The multidimensional burden of COVID-19 on Syrian refugees in Lebanon. J. Glob. Health 2021, 1, 05003. [Google Scholar] [CrossRef]
- OCHA. Humanitarian Needs Overview Iraq 2021. Available online: https://hum-insight.info/plan/1035 (accessed on 8 April 2022).
- World Bank Group. Iraq High Frequency Phone Survey (IHFPS) to Monitor Socioeconomic Trends during COVID-19. Available online: https://www.worldbank.org/en/country/iraq/publication/iraq-high-frequency-phone-survey-ihfps-to-monitor-impacts-of-covid-19-january-2021 (accessed on 9 April 2022).
- Dodd, W.; Kipp, A.; Bustos, M.; McNeil, A.; Little, M.; Lau, L.L. Humanitarian food security interventions during the COVID-19 pandemic in low-and middle-income countries: A review of actions among non-state actors. Nutrients 2021, 13, 2333. [Google Scholar] [CrossRef] [PubMed]
- Bizri, N.A.; Alam, W.; Mobayed, T.; Tamim, H.; Makki, M.; Mushrrafieh, U. COVID-19 in conflict region: The Arab levant response. BMC Public Health 2021, 21, 1590. [Google Scholar] [CrossRef] [PubMed]
- Durrance-Bagale, A.; Salman, O.M.; Omar, M.; Alhaffar, M.; Ferdaus, M.; Newaz, S.; Krishnan, S.; Howard, N. Lessons from humanitarian clusters to strengthen health system responses to mass displacement in low and middle-income countries: A scoping review. J. Migr. Health 2020, 1, 100028. [Google Scholar] [CrossRef] [PubMed]
- Rohwerder, B. The Socioeconomic Impacts of the COVID-19 Pandemic on Forcibly Displaced Persons. In Covid Collective Helpdesk Report 6; Foreign, Commonwealth and Development Office, Institute of Development Studies: Brighton, UK, 2021. [Google Scholar]
- El Arnaout, N.; Rutherford, S.; Zreik, T.; Nabulsi, D.; Yassin, N.; Saleh, S. Assessment of the health needs of Syrian refugees in Lebanon and Syria’s neighboring countries. Confl. Health 2019, 13, 31. [Google Scholar] [CrossRef] [PubMed]
- Dhalimi, A.; Wright, A.M.; Yamin, J.; Jamil, H.; Arnetz, B.B. Perception of discrimination in employment and health in refugees and immigrants. Stigma Health 2018, 3, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Cetorelli, V.; Burnham, G.; Shabila, N. Prevalence of non-communicable diseases and access to health care and medications among Yazidis and other minority groups displaced by ISIS into the Kurdistan Region of Iraq. Confl. Health 2017, 11, 4. [Google Scholar] [CrossRef] [PubMed]
- Cantor, D.J.; Swartz, J.; Roberts, B.; Abbara, A.; Ager, A.; Bhutta, Z.A.; Blanchet, K.; Bunte, D.M.; Chukwuorji, J.C.; Daoud, N.; et al. Understanding the health needs of internally displaced persons: A scoping review. J. Migr. Health 2021, 4, 100071. [Google Scholar] [CrossRef] [PubMed]
- Ekezie, W. Resilience actions of Internally Displaced Persons (IDPs) living in camp-like settings: A Northern Nigeria case study. J. Migr. Health 2022, 6, 100115. [Google Scholar] [CrossRef] [PubMed]
- REACH Initiative. Refugee Vulnerability Profiles, Maban, Country, Upper Nile, South Sudan. 2013. Available online: https://data.unhcr.org/fr/documents/download/28967 (accessed on 5 August 2022).
- Segadlo, N.; Krause, U.; Zanker, F.; Edler, H. Effects of the COVID-19 Pandemic on Refugees and Their Protection in Kenya, Uganda, Ghana, Nigeria, South Africa and Zimbabwe; Arnold Bergstraesser Institut: Freiburg im Breisgau, Germany, 2021. [Google Scholar]
- The UN Refugee Agency (UNHCR). Internally Displaced People. UNHCR (Asia Pacific). 2021. Available online: https://www.unhcr.org/internally-displaced-people.html (accessed on 8 April 2022).
- Abdoul-Azize, H.T. Social protection for refugees in the COVID-19 pandemic era: Insights from Turkey, Colombia and Uganda. Nat. Volatiles Essent. Oils 2021, 8, 14778–14798. [Google Scholar]
- Kharroubi, S.; Naja, F.; Diab-El-Harake, M.; Jomaa, L. Food insecurity pre- and post the COVID-19 pandemic and economic crisis in Lebanon: Prevalence and projections. Nutrients 2021, 13, 2976. [Google Scholar] [CrossRef] [PubMed]
- Omidvar, N.; Ahmadi, D.; Sinclair, K.; Melgar-Quiñonez, H. Food security in selected Middle East and North Africa (MENA) countries: An inter-country comparison. Food Secur. 2019, 11, 531–540. [Google Scholar] [CrossRef]
- REACH. Iraq: Multi-Cluster Needs Assessment (MCNA)—Round VIII, December 2020. Iraq: OCHA. 2021. Available online: https://reliefweb.int/report/iraq/iraq-multi-cluster-needs-assessment-mcna-round-viii-december-2020 (accessed on 8 April 2022).
- Pham, P.N.; Fozouni, L.; Al-Saiedi, A.; Coughlin, K.; Vinck, P. Association between distress and displacement settings: A cross-sectional survey among displaced Yazidis in Northern Iraq. BMC Public Health 2021, 21, 679. [Google Scholar] [CrossRef] [PubMed]
- Lami, F.; Ali, A.A.; Fathullah, K.; Abdullatif, H. Assessment of temporary medical clinics during the Arbaeenia mass gathering at Al-Karkh, Baghdad, Iraq, in 2014: Cross-sectional study. JMIR Public Health Surveill. 2019, 5, e10903. [Google Scholar] [CrossRef] [PubMed]
- McGowan, C.R.; Baxter, L.; Deola, C.; Gayford, M.; Marston, C.; Cummings, R.; Checchi, F. Mobile clinics in humanitarian emergencies: A systematic review. Confl. Health 2020, 14, 4. [Google Scholar] [CrossRef] [PubMed]
- Robehmed, S. Designing user-centered humanitarian technologies with displaced people in Iraq: Lessons from Refunite’s mobile family tracing platform. Int. Migr. 2019, 57, 109–120. [Google Scholar] [CrossRef]
- Woods, G.; Mace, S. Connecting Humanitarian Actors and Displaced Communities: The IDP Call Centre in Iraq 2015. Available online: https://odihpn.org/publication/connecting-humanitarian-actors-and-displaced-communities-the-idp-call-centre-in-iraq/ (accessed on 8 April 2022).

{kind=link}
| Domain | Variable | Response | IDPs (n = 2161) | Returnees (n = 1513) | Total (n = 3674) | Statistic † | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Weighted% | n | Weighted% | n | Weighted% | ||||||
| Humanitarian needs | Want to receive information from humanitarian actors (top 3 priorities/multiple responses) | Safety and security | No | 1570 | 76.8 | 1001 | 64.5 | 2571 | 67.0 | 21.9 | <0.001 |
| Yes | 591 | 23.2 | 512 | 35.5 | 1103 | 33.0 | |||||
| Status of housing | No | 1650 | 84.2 | 1126 | 63.4 | 2776 | 67.6 | 72.4 | <0.001 | ||
| Yes | 511 | 15.9 | 387 | 36.6 | 898 | 32.4 | |||||
| Livelihoods | No | 809 | 35.2 | 587 | 31.8 | 1396 | 32.5 | 1.7 | 0.195 | ||
| Yes | 1352 | 64.8 | 926 | 68.2 | 2278 | 67.5 | |||||
| Water services | No | 1859 | 92.2 | 1194 | 71.0 | 3053 | 75.3 | 96.1 | <0.001 | ||
| Yes | 302 | 7.8 | 319 | 29.0 | 621 | 24.7 | |||||
| Electricity services | No | 1769 | 92.9 | 1037 | 64.6 | 2806 | 70.3 | 372.7 | <0.001 | ||
| Yes | 392 | 7.1 | 476 | 35.4 | 868 | 29.7 | |||||
| Education | No | 2063 | 96.3 | 1413 | 90.0 | 3476 | 91.2 | 17.2 | <0.001 | ||
| Yes | 98 | 3.7 | 100 | 10.1 | 198 | 8.8 | |||||
| Health care | No | 1426 | 59.6 | 1052 | 78.2 | 2478 | 74.4 | 57.5 | <0.001 | ||
| Yes | 735 | 40.4 | 461 | 21.8 | 1196 | 25.6 | |||||
| Humanitarian assistance | No | 940 | 36.3 | 944 | 68.2 | 1884 | 61.8 | 144.6 | <0.001 | ||
| Yes | 1221 | 63.7 | 569 | 31.8 | 1790 | 38.2 | |||||
| Legal services | No | 2059 | 93.2 | 1400 | 94.3 | 3459 | 94.1 | 0.8 | 0.386 | ||
| Yes | 102 | 6.8 | 113 | 5.7 | 215 | 5.9 | |||||
| House, land, and property services | No | 2119 | 98.6 | 1469 | 97.9 | 3588 | 98.1 | 0.8 | 0.369 | ||
| Yes | 42 | 1.5 | 44 | 2.1 | 86 | 2.0 | |||||
| Insufficient food (past 30 days) | No | 1874 | 80.1 | 1432 | 97.8 | 3306 | 94.2 | 274.2 | <0.001 | ||
| Yes | 287 | 19.9 | 81 | 2.2 | 368 | 5.8 | |||||
| COVID-19 impacts | Movement restrictions by government | Need to obtain security clearance/coupons | No | 2025 | 93.8 | 1376 | 94.2 | 3401 | 94.1 | 0.1 | 0.788 |
| Yes | 107 | 6.2 | 98 | 5.9 | 205 | 5.9 | |||||
| Missing | 29 | 0.0 | 39 | 0.0 | 68 | 0.0 | |||||
| Need to show ID documents | No | 2046 | 95.0 | 1363 | 89.1 | 3409 | 90.3 | 9.5 | 0.002 | ||
| Yes | 83 | 5.0 | 109 | 10.9 | 192 | 9.7 | |||||
| Missing | 32 | 0.0 | 41 | 0.0 | 73 | 0.0 | |||||
| Time restrictions on when to leave and return | No | 1993 | 89.7 | 1377 | 87.2 | 3370 | 87.7 | 1.4 | 0.242 | ||
| Yes | 146 | 10.3 | 100 | 12.8 | 246 | 12.3 | |||||
| Missing | 22 | 0.0 | 36 | 0.0 | 58 | 0.0 | |||||
| Need to provide a specific reason for movement | No | 2084 | 92.1 | 1409 | 97.5 | 3493 | 96.4 | 28.6 | <0.001 | ||
| Yes | 53 | 7.9 | 69 | 2.5 | 122 | 3.6 | |||||
| Missing | 24 | 0.0 | 35 | 0.0 | 59 | 0.0 | |||||
| Physical roadblocks | No | 2069 | 95.9 | 1390 | 96.8 | 3459 | 96.6 | 0.9 | 0.336 | ||
| Yes | 59 | 4.1 | 84 | 3.2 | 143 | 3.4 | |||||
| Missing | 33 | 0.0 | 39 | 0.0 | 72 | 0.0 | |||||
| Unemployment of household members due to COVID-19 | No | 1443 | 59.8 | 1192 | 89.6 | 2635 | 83.6 | 309.8 | <0.001 | ||
| Yes | 705 | 40.2 | 292 | 10.4 | 997 | 16.4 | |||||
| Missing | 13 | 0.0 | 29 | 0.0 | 42 | 0.0 | |||||
| Household demographic/vulnerability covariates | Number of family members * | (min = 1; max = 46) | 6.39 | (6.15, 6.62) | 5.17 | (4.98, 5.36) | 5.41 | (5.26, 5.57) | −8.0 | <0.001 | |
| Elderly-headed household (65 or older) | No | 1989 | 92.0 | 1418 | 95.0 | 3407 | 94.4 | 5.3 | 0.022 | ||
| Yes | 172 | 8.0 | 95 | 5.0 | 267 | 5.6 | |||||
| Female-headed household | No | 1901 | 87.7 | 1339 | 90.3 | 3240 | 89.8 | 2.4 | 0.120 | ||
| Yes | 260 | 12.4 | 174 | 9.7 | 434 | 10.2 | |||||
| HOH with health problems (injury, chronic/communicable disease, etc.) | No | 1392 | 65.1 | 1005 | 65.1 | 2397 | 65.1 | 0.0 | 0.986 | ||
| Yes | 769 | 34.9 | 508 | 34.9 | 1277 | 34.9 | |||||
| Employment status of HOH | No | 655 | 31.7 | 347 | 18.6 | 1002 | 21.2 | 29.6 | <0.001 | ||
| Yes | 1505 | 68.3 | 1165 | 81.4 | 2670 | 78.8 | |||||
| Missing | 1 | 0.0 | 1 | 0.0 | 2 | 0.0 | |||||
| Household’s total monthly income (per 100,000 IQD) | (min = 0; max = 70) | 4.55 | (4.15, 4.95) | 5.05 | (4.61, 5.49) | 4.95 | (4.59, 5.31) | 1.7 | 0.100 | ||
| Walking time to reach the nearest health care facility | <15 min | 1236 | 59.5 | 806 | 54.8 | 2042 | 55.7 | 7.3 | <0.001 | ||
| 15–29 min | 632 | 28.0 | 447 | 28.9 | 1079 | 28.7 | |||||
| 30–59 min | 177 | 6.7 | 116 | 12.2 | 293 | 11.1 | |||||
| 1–3 h | 63 | 3.5 | 108 | 3.8 | 171 | 3.7 | |||||
| 3 h < | 53 | 2.3 | 36 | 0.4 | 89 | 0.8 | |||||
| Walking time to reach the nearest marketplace | <15 min | 1800 | 83.4 | 1191 | 75.9 | 2991 | 77.4 | 4.1 | 0.003 | ||
| 15–29 min | 246 | 11.7 | 210 | 17.6 | 456 | 16.4 | |||||
| 30–59 min | 88 | 3.8 | 36 | 4.1 | 124 | 4.0 | |||||
| 1–2 h | 20 | 0.8 | 25 | 1.3 | 45 | 1.2 | |||||
| 2 h< | 7 | 0.3 | 51 | 1.2 | 58 | 1.0 | |||||
| Variable | Total | IDPs | Returnees | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | Robust SE | p-Value | LL | UL | OR | Robust SE | p-Value | LL | UL | OR | Robust SE | p-Value | LL | UL | |
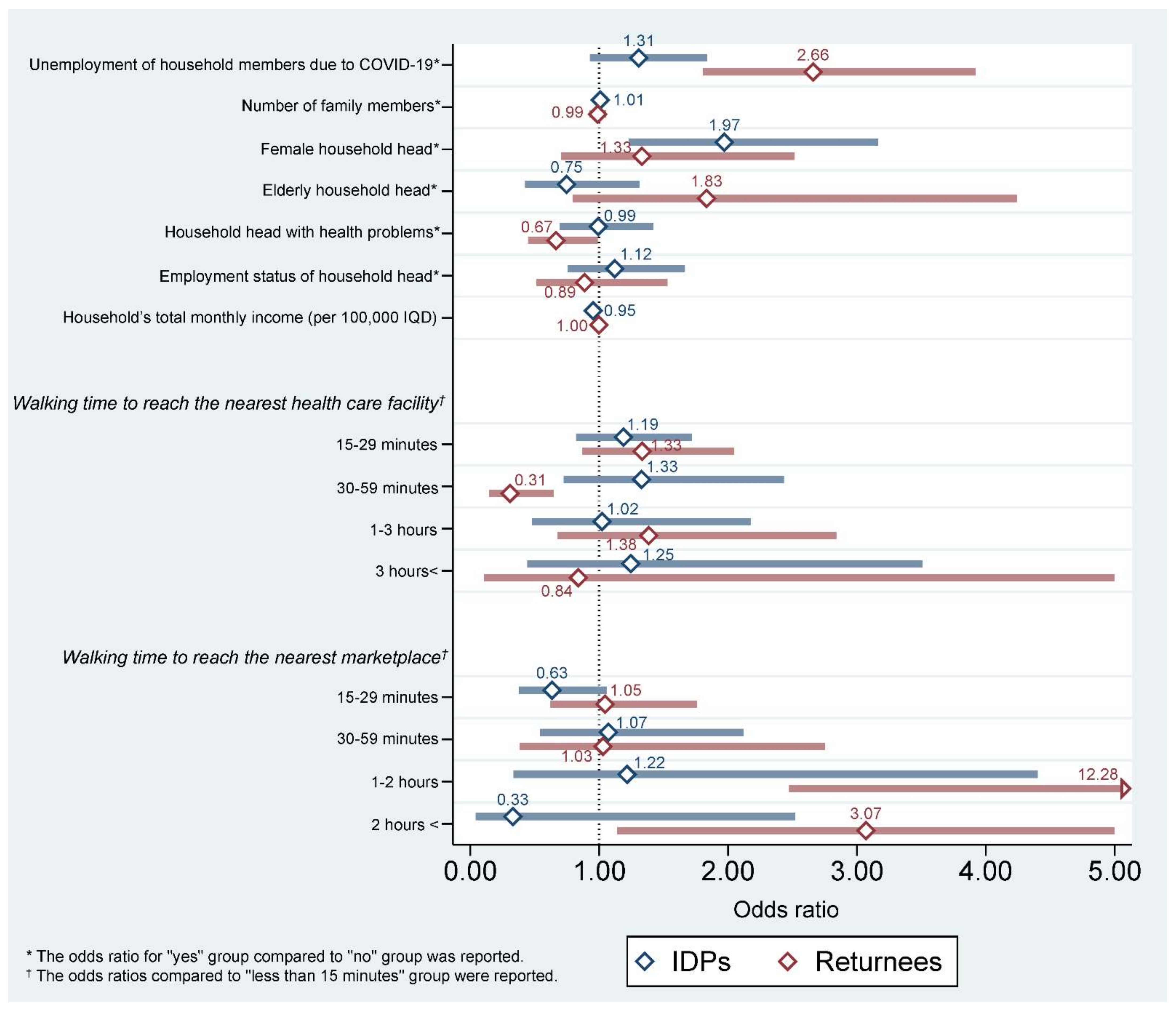
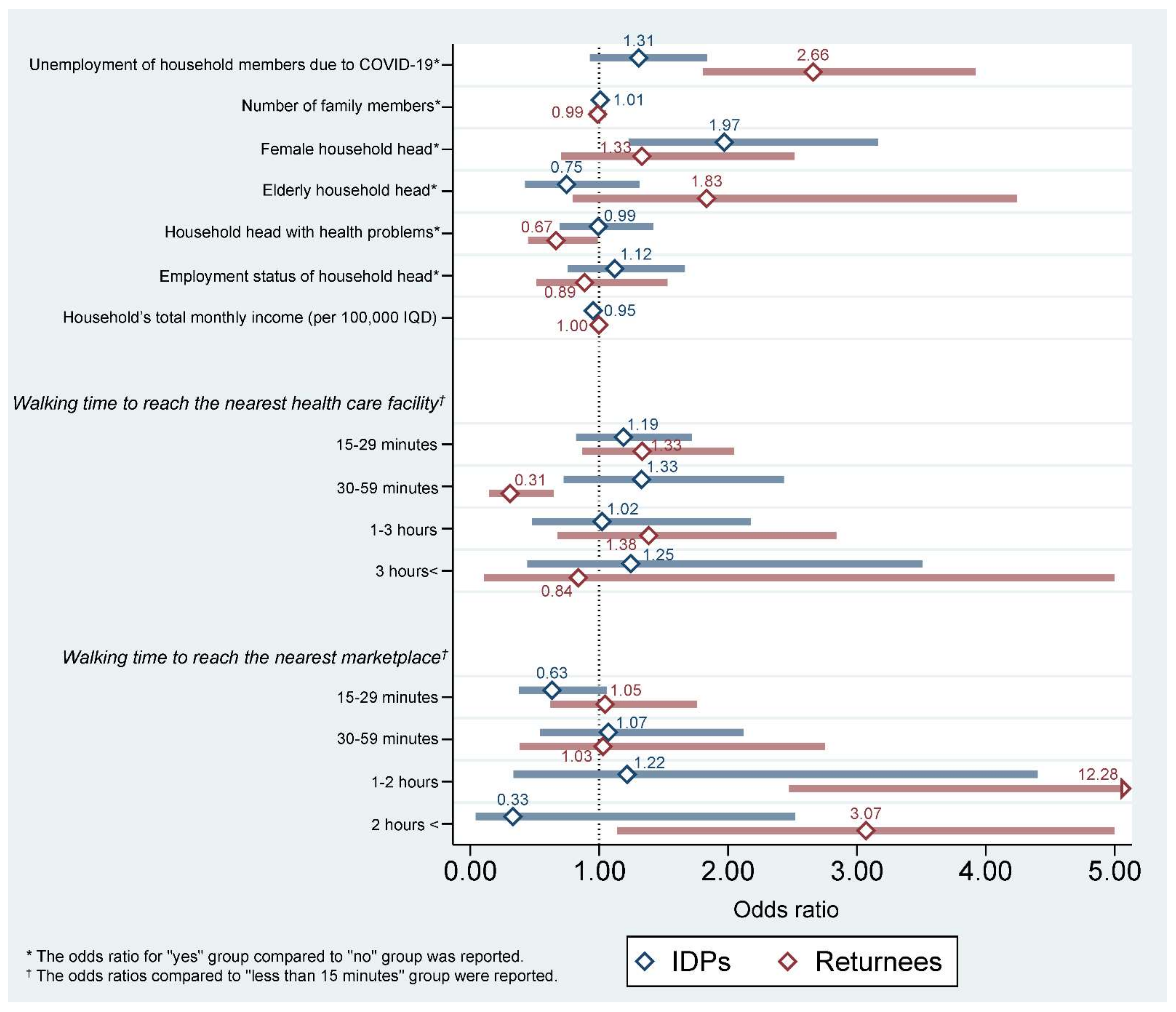
| Unemployment of household members due to COVID-19 | |||||||||||||||
| No | 1.000 | ref | 1.000 | ref | 1.000 | ref | |||||||||
| Yes | 2.061 | 0.287 | <0.001 | 1.569 | 2.708 | 1.307 | 0.227 | 0.124 | 0.929 | 1.839 | 2.661 | 0.526 | < 0.001 | 1.805 | 3.922 |
| Displacement status | |||||||||||||||
| IDPs | 1.000 | ref | N/A | ||||||||||||
| Returnees | 0.325 | 0.040 | <0.001 | 0.255 | 0.414 | ||||||||||
| Number of family members | |||||||||||||||
| 0.996 | 0.024 | 0.865 | 0.949 | 1.045 | 1.009 | 0.027 | 0.749 | 0.956 | 1.064 | 0.988 | 0.033 | 0.726 | 0.926 | 1.055 | |
| Female HOH | |||||||||||||||
| No | 1.000 | ref | 1.000 | ref | 1.000 | ref | |||||||||
| Yes | 1.434 | 0.336 | 0.124 | 0.906 | 2.271 | 1.971 | 0.476 | 0.005 | 1.228 | 3.164 | 1.333 | 0.432 | 0.376 | 0.706 | 2.516 |
| Elderly HOH | |||||||||||||||
| No | 1.000 | ref | 1.000 | ref | 1.000 | ref | |||||||||
| Yes | 1.411 | 0.445 | 0.275 | 0.760 | 2.620 | 0.747 | 0.214 | 0.310 | 0.426 | 1.311 | 1.833 | 0.783 | 0.156 | 0.793 | 4.239 |
| HOH with health problems | |||||||||||||||
| No | 1.000 | ref | 1.000 | ref | 1.000 | ref | |||||||||
| Yes | 0.759 | 0.119 | 0.077 | 0.558 | 1.031 | 0.993 | 0.180 | 0.968 | 0.695 | 1.418 | 0.666 | 0.134 | 0.044 | 0.449 | 0.988 |
| Employment status of HOH | |||||||||||||||
| No | 1.000 | ref | 1.000 | ref | 1.000 | ref | |||||||||
| Yes | 0.931 | 0.181 | 0.712 | 0.635 | 1.364 | 1.121 | 0.226 | 0.571 | 0.755 | 1.666 | 0.887 | 0.247 | 0.666 | 0.514 | 1.530 |
| Household’s total monthly income (per 100,000 IQD) | |||||||||||||||
| 0.983 | 0.013 | 0.198 | 0.959 | 1.009 | 0.953 | 0.017 | 0.008 | 0.920 | 0.987 | 0.999 | 0.017 | 0.932 | 0.966 | 1.033 | |
| Walking time to reach the nearest health care facility | |||||||||||||||
| <15 min | 1.000 | ref | 1.000 | ref | 1.000 | ref | |||||||||
| 15–29 min | 1.315 | 0.231 | 0.120 | 0.931 | 1.857 | 1.189 | 0.224 | 0.359 | 0.822 | 1.720 | 1.334 | 0.291 | 0.187 | 0.869 | 2.046 |
| 30–59 min | 0.454 | 0.119 | 0.003 | 0.272 | 0.759 | 1.329 | 0.410 | 0.356 | 0.726 | 2.433 | 0.308 | 0.117 | 0.002 | 0.146 | 0.649 |
| 1–3 h | 1.370 | 0.404 | 0.286 | 0.768 | 2.444 | 1.022 | 0.394 | 0.954 | 0.480 | 2.176 | 1.385 | 0.507 | 0.374 | 0.675 | 2.841 |
| 3 h< | 0.910 | 0.461 | 0.852 | 0.337 | 2.455 | 1.246 | 0.658 | 0.678 | 0.442 | 3.510 | 0.839 | 0.879 | 0.867 | 0.107 | 6.554 |
| Walking time to reach the nearest marketplace | |||||||||||||||
| <15 min | 1.000 | ref | 1.000 | ref | 1.000 | ref | |||||||||
| 15–29 min | 0.939 | 0.209 | 0.776 | 0.607 | 1.451 | 0.634 | 0.166 | 0.082 | 0.380 | 1.059 | 1.046 | 0.277 | 0.864 | 0.623 | 1.758 |
| 30–59 min | 0.988 | 0.389 | 0.975 | 0.456 | 2.140 | 1.072 | 0.373 | 0.842 | 0.542 | 2.120 | 1.030 | 0.516 | 0.953 | 0.386 | 2.752 |
| 1–2 h | 11.569 | 9.386 | 0.003 | 2.358 | 56.769 | 1.217 | 0.798 | 0.765 | 0.336 | 4.402 | 17.275 | 17.106 | 0.004 | 2.476 | 120.500 |
| 2 h < | 2.789 | 1.257 | 0.023 | 1.153 | 6.747 | 0.331 | 0.342 | 0.285 | 0.043 | 2.519 | 3.070 | 1.553 | 0.027 | 1.138 | 8.281 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noh, J.-W.; Cheon, J.; Kim, K.-B.; Song, S.E.; Cha, J.; Kwon, Y.D. Contributing Factors in Whether Displaced Households Want to Receive Humanitarian Information from Humanitarian Actors: Iraq Multi-Cluster Needs Assessment. Int. J. Environ. Res. Public Health 2022, 19, 10114. https://doi.org/10.3390/ijerph191610114
Noh J-W, Cheon J, Kim K-B, Song SE, Cha J, Kwon YD. Contributing Factors in Whether Displaced Households Want to Receive Humanitarian Information from Humanitarian Actors: Iraq Multi-Cluster Needs Assessment. International Journal of Environmental Research and Public Health. 2022; 19(16):10114. https://doi.org/10.3390/ijerph191610114
Chicago/Turabian StyleNoh, Jin-Won, Jooyoung Cheon, Kyoung-Beom Kim, Si Eun Song, Jiho Cha, and Young Dae Kwon. 2022. "Contributing Factors in Whether Displaced Households Want to Receive Humanitarian Information from Humanitarian Actors: Iraq Multi-Cluster Needs Assessment" International Journal of Environmental Research and Public Health 19, no. 16: 10114. https://doi.org/10.3390/ijerph191610114
APA StyleNoh, J.-W., Cheon, J., Kim, K.-B., Song, S. E., Cha, J., & Kwon, Y. D. (2022). Contributing Factors in Whether Displaced Households Want to Receive Humanitarian Information from Humanitarian Actors: Iraq Multi-Cluster Needs Assessment. International Journal of Environmental Research and Public Health, 19(16), 10114. https://doi.org/10.3390/ijerph191610114