
Classification of Deprivation Indices That Applied to Detect Health Inequality: A Scoping Review



Abstract
:1. Introduction
Practical Aspects of the Development of Deprivation Indexes
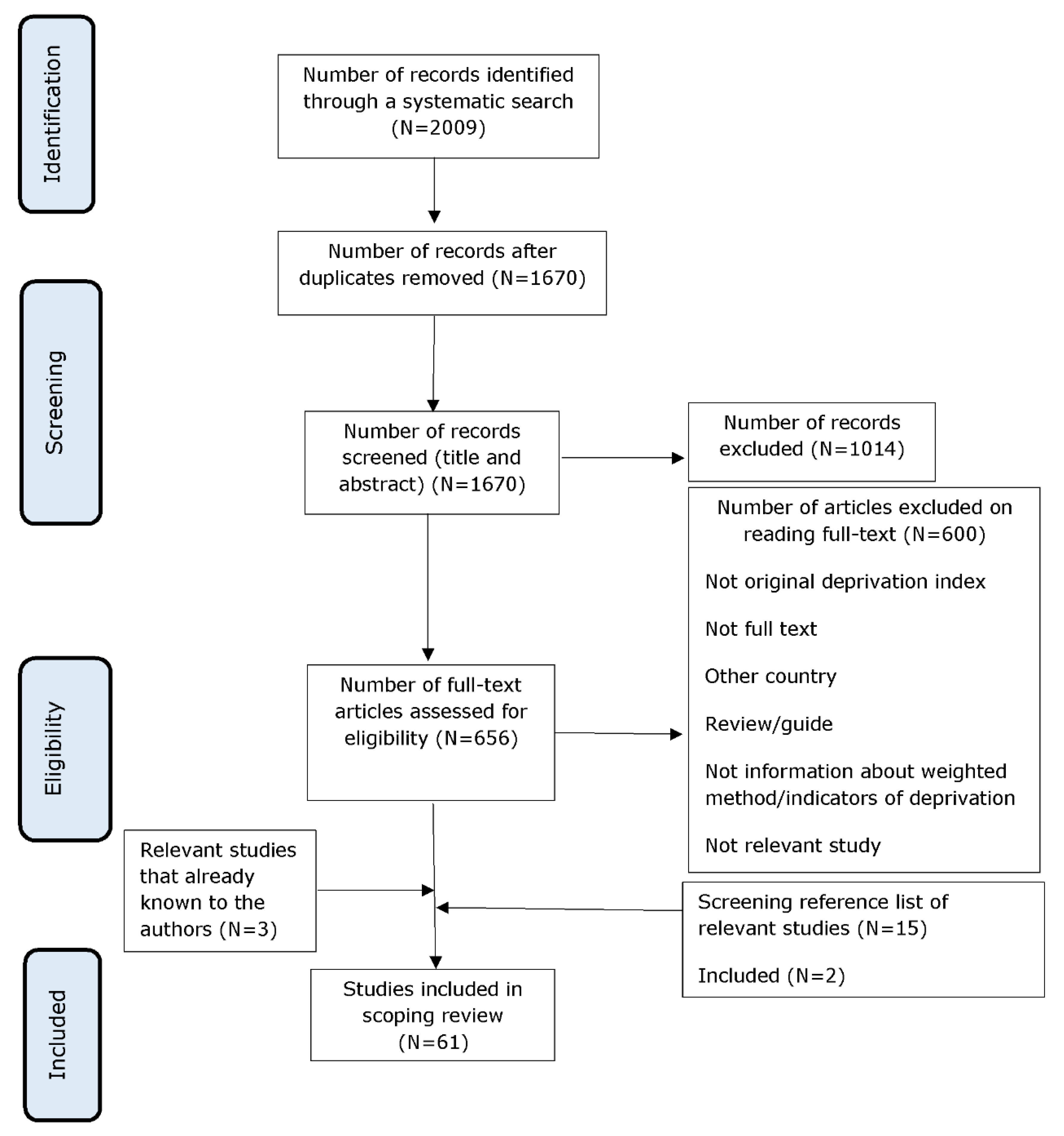
2. Methods
Data Extraction and Analysis
3. Results
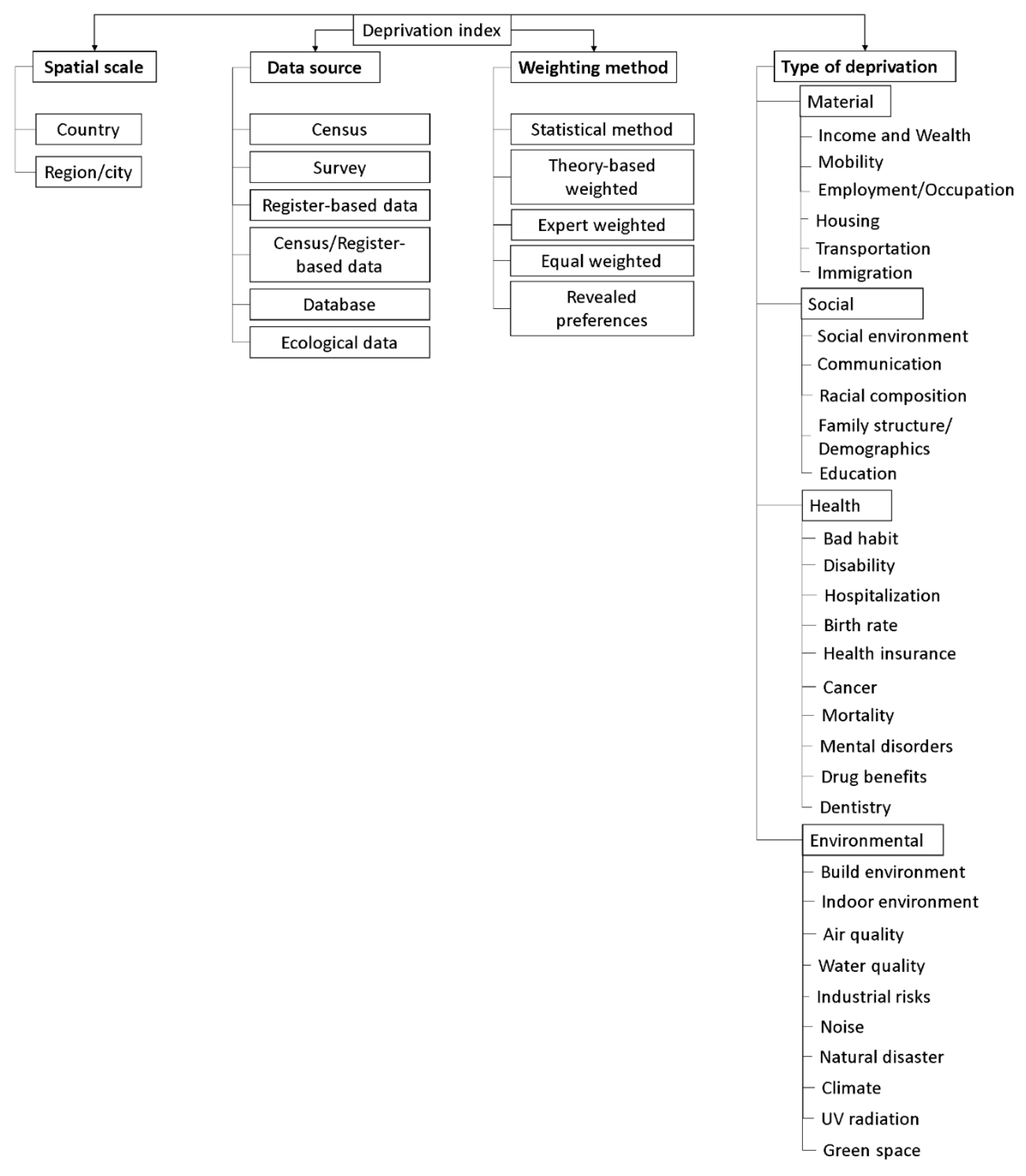
3.1. Taxonomy of Deprivation Indices
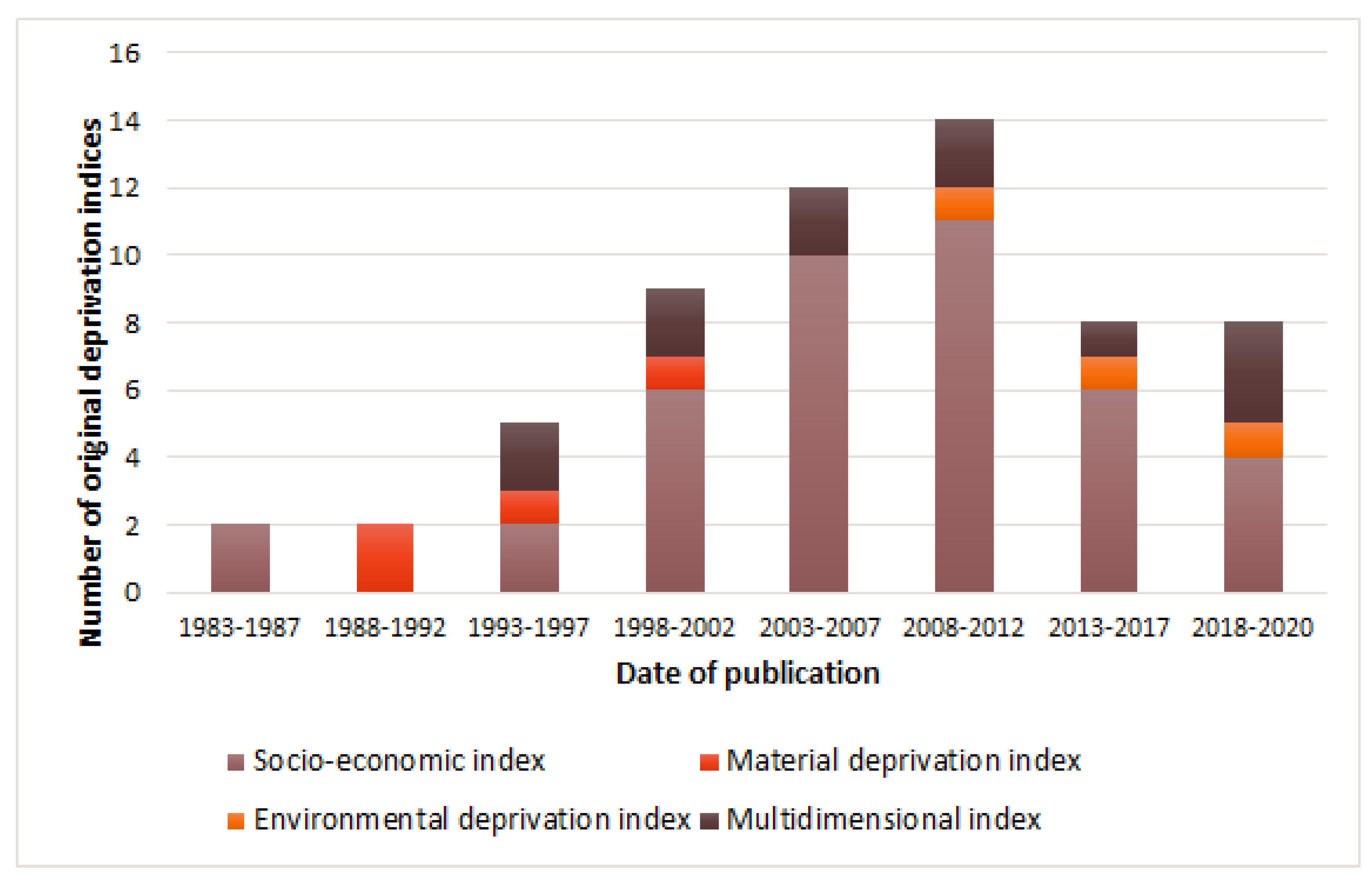
3.2. Type of Deprivation
- Multidimensional indices, which were also divided into indices containing indicators of domains from sub-classes “social”, “material” and “health” [105,106]; “social”, “material” and “environmental” [107,108,109,110]; and indicators of domains from all sub-classes [32,34,111,112,113,114] (see Table S2).
3.3. Spatial Scale
3.4. Data Source
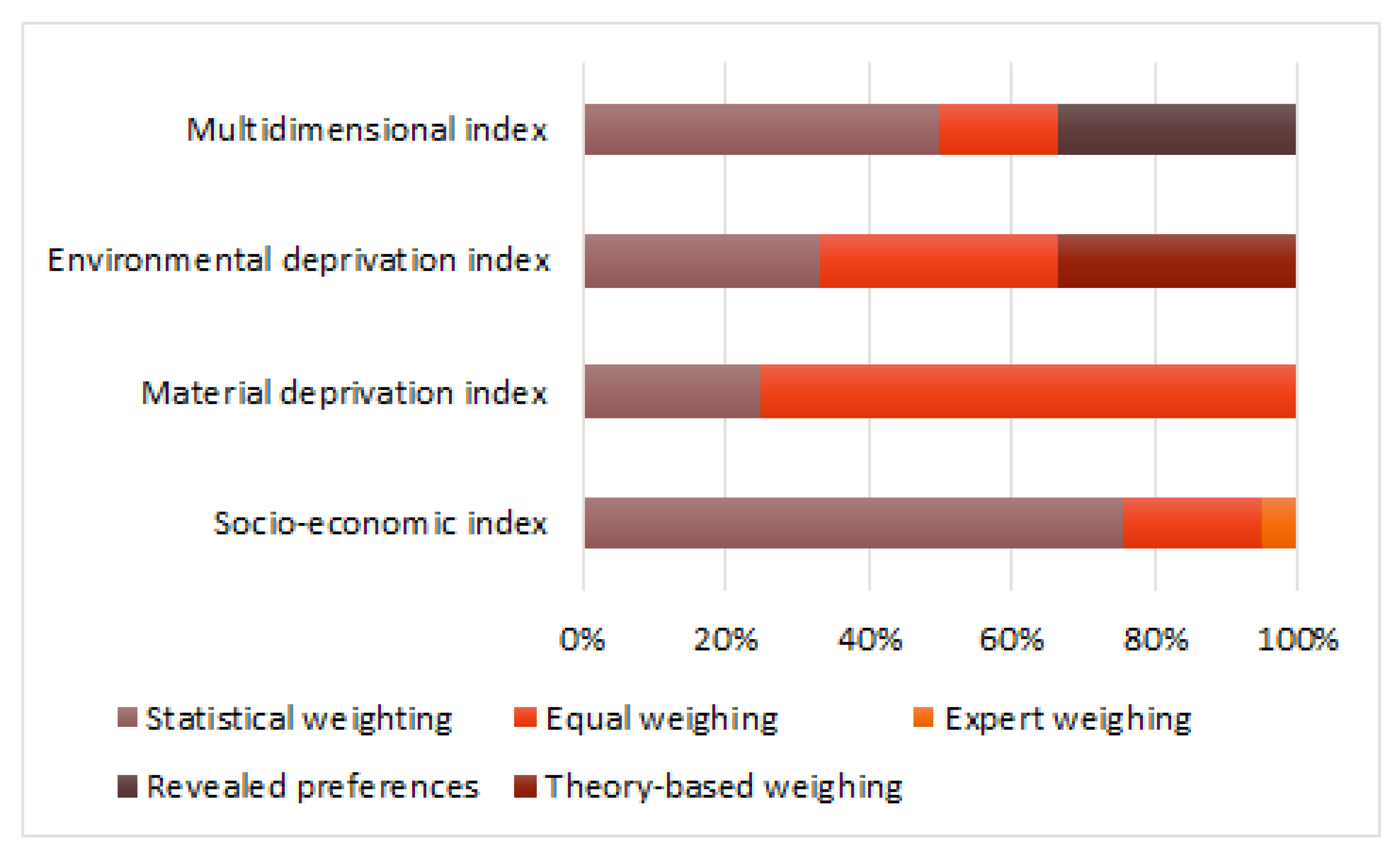
3.5. Weighting Methods
3.6. Using Indices outside of Research
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sub-Class | Definition |
|---|---|
| Census | A survey conducted on the full set of observation objects belonging to a given population or universe [142]. Typically, a Census is conducted every 5 or 10 years rather than annually [143]. |
| Survey | An investigation about the characteristics of a given population by means of collecting data from a sample of that population and estimating their characteristics through the systematic use of statistical methodology [142]. A sample survey can be repeated much more often than a Census because it costs less [143]. |
| Register-based data | The data that are in or originate from a register. Register is a database which is updated continuously (often for administrative purposes, such as population registers or building registers) and from which statistics can be extracted/aggregated/computed [143]. |
| Census/Register-based data | The data from a Census and register. |
| Database |
|
| Ecological data | Representation of information about the natural world presented in a structured format suitable for interpretation or processing, that could be reinterpreted for use in a different field of study or context [145]. |
| Sub-Class | Total |
|---|---|
| Census | 73% (44/60) |
| Survey | 10% (6/60) |
| Register-based data | 3% (2/60) |
| Census/Register-based data | 7% (4/60) |
| Database | 3% (2/60) |
| Ecological data | 3% (2/60) |
References
- Pettigrew, T.F. Samuel Stouffer and relative deprivation. Soc. Psychol. Q. 2015, 78, 7–24. [Google Scholar] [CrossRef]
- Ladin, K. Absolute deprivation. In The Wiley Blackwell Encyclopedia of Health, Illness, Behavior, and Society; Cockerham, W.C., Dingwall, R., Quah, S., Eds.; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2014. [Google Scholar] [CrossRef]
- Schervish, P.G. Peter Townsend. Poverty in the United Kingdom: A Survey of Household Resources and Standards of Living. Pp. 1216. Berkeley, CA: University of California Press, 1979. $37.50. Paperbound, $15.95. Ann. Am. Acad. Political Soc. Sci. 1981, 456, 182–183. [Google Scholar] [CrossRef]
- Fretz, A.; Schneider, A.L.; McEvoy, J.W.; Hoogeveen, R.; Ballantyne, C.M.; Coresh, J.; Selvin, E. The association of socioeconomic status with subclinical myocardial damage, incident cardiovascular events, and mortality in the ARIC study. Am. J. Epidemiol. 2016, 183, 452–461. [Google Scholar] [CrossRef]
- Marshall, I.J.; Wang, Y.; Crichton, S.; McKevitt, C.; Rudd, A.G.; Wolfe, C.D. The effects of socioeconomic status on stroke risk and outcomes. Lancet Neurol. 2015, 14, 1206–1218. [Google Scholar] [CrossRef]
- Chung, G.K.K.; Lai, F.T.T.; Yeoh, E.K.; Chung, R.Y. Educational inequality in physician-diagnosed hypertension widened and persisted among women from 1999 to 2014 in Hong Kong. Sci. Rep. 2019, 9, 14361. [Google Scholar] [CrossRef]
- Alicandro, G.; Frova, L.; Sebastiani, G.; El Sayed, I.; Boffetta, P.; La Vecchia, C. Educational inequality in cancer mortality: A record linkage study of over 35 million Italians. Cancer Causes Control. 2017, 28, 997–1006. [Google Scholar] [CrossRef]
- Großschädl, F.; Stolz, E.; Mayerl, H.; Rásky, É.; Freidl, W.; Stronegger, W. Educational inequality as a predictor of rising back pain prevalence in Austria-sex differences. Eur. J. Public Health 2016, 26, 248–253. [Google Scholar] [CrossRef]
- Ravesteijn, B.; van Kippersluis, H.; van Doorslaer, E. The contribution of occupation to health inequality. Res. Econ. Inequal. 2013, 21, 311–332. [Google Scholar] [CrossRef]
- Madsen, J.; Kanstrup, A.M.; Josephsson, S. The assumed relation between occupation and inequality in health. Scand. J. Occup. Ther. 2016, 23, 1–12. [Google Scholar] [CrossRef]
- Huisman, M.; Van Lenthe, F.; Avendano, M.; Mackenbach, J. The contribution of job characteristics to socioeconomic inequalities in incidence of myocardial infarction. Soc. Sci. Med. 2008, 66, 2240–2252. [Google Scholar] [CrossRef]
- Costa, G. Health inequalities among occupations: Epidemiologic hints for labour and social protection policies. Med. Lav. 2005, 96, 7–27. (In Italian) [Google Scholar]
- Timmermans, E.J.; Veldhuizen, E.M.; Snijder, M.B.; Huisman, M.; Kunst, A.E. Neighbourhood safety and smoking in population subgroups: The HELIUS study. Prev. Med. 2018, 112, 111–118. [Google Scholar] [CrossRef]
- Lee, H.Y.; Oh, J.; Kawachi, I.; Heo, J.; Kim, S.; Lee, J.K.; Kang, D. Positive and negative social support and depressive symptoms according to economic status among adults in Korea: Cross-sectional results from the Health Examinees-Gem Study. BMJ Open 2019, 9, e023036. [Google Scholar] [CrossRef] [PubMed]
- Zajacova, A.; Lawrence, E.M. The relationship between education and health: Reducing disparities through a contextual approach. Annu. Rev. Public Health 2018, 39, 273–289. [Google Scholar] [CrossRef] [PubMed]
- Labbe, E.; Blanquet, M.; Gerbaud, L.; Poirier, G.; Sass, C.; Vendittelli, F.; Moulin, J.J. A new reliable index to measure individual deprivation: The EPICES score. Eur. J. Public Health 2015, 25, 604–609. [Google Scholar] [CrossRef]
- Vaucher, P.; Bischoff, T.; Diserens, E.A.; Herzig, L.; Meystre-Agustoni, G.; Panese, F.; Favrat, B.; Sass, C.; Bodenmann, P. Detecting and measuring deprivation in primary care: Development, reliability and validity of a self-reported questionnaire: The DiPCare-Q. BMJ Open 2012, 2, e000692. [Google Scholar] [CrossRef]
- Salmond, C.; Crampton, P.; King, P.; Waldegrave, C. NZiDep: A New Zealand index of socioeconomic deprivation for individuals. Soc. Sci. Med. 2006, 62, 1474–1485. [Google Scholar] [CrossRef]
- Winkleby, M.A.; Jatulis, D.E.; Frank, E.; Fortmann, S.P. Socioeconomic status and health: How education, income, and occupation contribute to risk factors for cardiovascular disease. Am. J. Public Health 1992, 82, 816–820. [Google Scholar] [CrossRef]
- Metcalf, P.A.; Scragg, R.R.; Schaaf, D.; Dyall, L.; Black, P.N.; Jackson, R.T. Comparison of different markers of socioeconomic status with cardiovascular disease and diabetes risk factors in the Diabetes, Heart and Health Survey. N. Z. Med. J. 2008, 121, 45–56. [Google Scholar]
- Metcalf, P.; Scragg, R.; Davis, P. Relationship of different measures of socioeconomic status with cardiovascular disease risk factors and lifestyle in a New Zealand workforce survey. N. Z. Med. J. 2007, 120, U2392. [Google Scholar]
- Kivimäki, M.; Batty, G.D.; Pentti, J.; Shipley, M.J.; Sipilä, P.N.; Nyberg, S.T.; Suominen, S.B.; Oksanen, T.; Stenholm, S.; Virtanen, M.; et al. Association between socioeconomic status and the development of mental and physical health conditions in adulthood: A multi-cohort study. Lancet Public Health 2020, 5, e140–e149. [Google Scholar] [CrossRef]
- Quezada, A.D.; Lozada-Tequeanes, A.L. Time trends and sex differences in associations between socioeconomic status indicators and overweight-obesity in Mexico (2006–2012). BMC Public Health 2015, 15, 1244. [Google Scholar] [CrossRef] [PubMed]
- Townsend, P. Deprivation. J. Soc. Pol. 1987, 16, 125–146. [Google Scholar] [CrossRef]
- Carstairs, V.; Morris, R. Deprivation: Explaining differences in mortality between Scotland and England and Wales. Br. Med. J. 1989, 299, 886–889. [Google Scholar] [CrossRef] [PubMed]
- Jarman, B. Identification of underprivileged areas. Br. Med. J. (Clin. Res. Ed.) 1983, 286, 1705–1709. [Google Scholar] [CrossRef]
- Malmström, M.; Sundquist, J.; Bajekal, M.; Johansson, S.E. Indices of need and social deprivation for primary health care. Scand. J. Soc. Med. 1998, 26, 124–130. [Google Scholar] [CrossRef]
- Gray, A.M. Inequalities in health. The Black Report: A summary and comment. Int. J. Health Serv. 1982, 12, 349–380. [Google Scholar] [CrossRef]
- Marmot, M.G. Social inequalities in mortality: The social environment. In Class and Health: Research and Longitudinal Data; Wilkinson, R.G., Ed.; Tavistock: London, UK, 1986; pp. 21–33. [Google Scholar]
- Acheson, D. Independent Inquiry into Inequalities in Health; Stationary Office: London, UK, 1998. [Google Scholar]
- Northern Ireland Statistics & Research Agency. NI Multiple Deprivation Measure 2001. Available online: http://www.nisra.gov.uk/deprivation/nimdm_2001.htm (accessed on 27 April 2020).
- Jordan, H.; Roderick, P.; Martin, D. The index of multiple deprivation 2000 and accessibility effects on health. J. Epidemiol. Community Health 2004, 58, 250–257. [Google Scholar] [CrossRef]
- The Scottish Government. Using the Scottish Index of Multiple Deprivation 2004: Guidance. Available online: https://www.webarchive.org.uk/wayback/archive/20150218202114/http://www.gov.scot/Publications/2005/01/20458/49127 (accessed on 10 February 2021).
- University of Oxford—Department of Social Policy and Social Work. Index of Multiple Deprivation for Wales. Available online: http://gov.wales/docs/statistics/2011/110831wimd2000en.pdf (accessed on 10 February 2021).
- Robinson, W.S. Ecological correlations and the behavior of individuals. Am. Sociol. Rev. 1950, 15, 351–357. [Google Scholar] [CrossRef]
- Noble, M.; Wright, G.; Smith, G.; Dibben, C. Measuring multiple deprivation at the small-area level. Environ. Plan. A Econ. Space 2006, 38, 169–185. [Google Scholar] [CrossRef]
- Maroko, A.R.; Doan, T.M.; Arno, P.S.; Hubel, M.; Yi, S.; Viola, D. Integrating social determinants of health with treatment and prevention: A new tool to assess local area deprivation. Prev. Chronic. Dis. 2016, 13, E128. [Google Scholar] [CrossRef] [PubMed]
- Mehra, R.; Shebl, F.M.; Cunningham, S.D.; Magriples, U.; Barrette, E.; Herrera, C.; Kozhimannil, K.B.; Ickovics, J.R. Area-level deprivation and preterm birth: Results from a national, commercially-insured population. BMC Public Health 2019, 19, 236. [Google Scholar] [CrossRef] [PubMed]
- Zelenina, A.; Shalnova, S.; Maksimov, S.; Drapkina, O. Characteristics of Composite Deprivation Indices Used in Public Health: A Scoping Review Protocol. 14 September 2021. Available online: https://www.researchsquare.com/article/rs-903435/v1 (accessed on 14 August 2022).
- Salvador-Carulla, L.; Salinas-Pérez, J.A.; Martín, M.; Grané, M.S.; Gibert, K.; Roca, M.; Bulbena, A. GClin-SEP group. A preliminary taxonomy and a standard knowledge base for mental-health system indicators in Spain. Int. J. Ment. Health Syst. 2010, 4, 29. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.J.; Coronado, F.; Boulton, M.L.; Merrill, J.A. Public Health Enumeration Working Group. The public health workforce taxonomy: Revisions and recommendations for implementation. J. Public Health Manag. Pract. 2018, 24, E1–E11. [Google Scholar] [CrossRef]
- Alexander, D.; Bourek, A.; Kilroe, J.; Rigby, M.; Staines, A. The RICHE taxonomy—An innovative means of classification of child health research. Child. Care Health Dev. 2014, 40, 632–639. [Google Scholar] [CrossRef]
- Allik, M.; Leyland, A.; Travassos Ichihara, M.Y.; Dundas, R. Creating small-area deprivation indices: A guide for stages and options. J. Epidemiol. Community Health 2020, 74, 20–25. [Google Scholar] [CrossRef]
- Ferragina, E.; Tomlinson, M.; Walker, R. Poverty and participation in twenty-first century multicultural Britain. Soc. Policy Soc. 2017, 16, 535–559. [Google Scholar] [CrossRef]
- Arcaya, M.C.; Arcaya, A.L.; Subramanian, S.V. Inequalities in health: Definitions, concepts, and theories. Glob. Health Action 2015, 8, 27106. [Google Scholar] [CrossRef]
- Charlton, J.; Rudisill, C.; Bhattarai, N.; Gulliford, M. Impact of deprivation on occurrence, outcomes and health care costs of people with multiple morbidity. J. Health Serv. Res. Policy 2013, 18, 215–223. [Google Scholar] [CrossRef]
- Brulle, R.J.; Pellow, D.N. Environmental justice: Human health and environmental inequalities. Annu. Rev. Public Health 2006, 27, 103–124. [Google Scholar] [CrossRef]
- Morello-Frosch, R.; Pastor, M., Jr.; Porras, C.; Sadd, J. Environmental justice and regional inequality in southern California: Implications for future research. Environ. Health Perspect. 2002, 110, 149–154. [Google Scholar] [CrossRef]
- Yue, C.; Liu, Y. Impact of education on the income of different social groups. Front. Educ. China 2007, 2, 191–200. [Google Scholar] [CrossRef]
- Blaug, M. The correlation between education and earnings: What does it signify? High. Educ. Q. 1947, 1, 53–76. [Google Scholar] [CrossRef]
- Chung, W.; Lim, S.J.; Lee, S.; Kim, R.; Kim, J. Gender-specific interactions between education and income in relation to obesity: A cross-sectional analysis of the Fifth Korea National Health and Nutrition Examination Survey (KNHANES V). BMJ Open 2017, 7, e014276. [Google Scholar] [CrossRef] [PubMed]
- Lalloué, B.; Monnez, J.M.; Padilla, C.; Kihal, W.; Le Meur, N.; Zmirou-Navier, D.; Deguen, S. A statistical procedure to create a neighborhood socioeconomic index for health inequalities analysis. Int. J. Equity Health 2013, 12, 21. [Google Scholar] [CrossRef]
- Breysse, P.N. Lead Elimination for the 21st Century. J. Public Health Manag Pract. 2019, 25, S3–S4. [Google Scholar] [CrossRef] [PubMed]
- Mankikar, D.; Campbell, C.; Greenberg, R. Evaluation of a home-based environmental and educational intervention to improve health in vulnerable households: Southeastern Pennsylvania lead and healthy homes program. Int. J. Environ. Res. Public Health 2016, 13, 900. [Google Scholar] [CrossRef]
- Office of the Surgeon General (US). The Surgeon General’s Call to Action to Promote Healthy Homes; Office of the Surgeon General (US): Rockville, MD, USA, 2009. Available online: https://www.ncbi.nlm.nih.gov/books/NBK44192/ (accessed on 26 October 2021).
- Krieger, J.; Higgins, D.L. Housing and health: Time again for public health action. Am. J. Public Health 2002, 92, 758–768. [Google Scholar] [CrossRef]
- Bashir, S.A. Home is where the harm is: Inadequate housing as a public health crisis. Am. J. Public Health 2002, 92, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Schederecker, F.; Kurz, C.; Fairburn, J.; Maier, W. Do alternative weighting approaches for an Index of Multiple Deprivation change the association with mortality? A sensitivity analysis from Germany. BMJ Open 2019, 9, e028553. [Google Scholar] [CrossRef]
- Zadnik, V.; Reich, B.J. Analysis of the relationship between socioeconomic factors and stomach cancer incidence in Slovenia. Neoplasma 2006, 53, 103–110. [Google Scholar] [PubMed]
- Meijer, M.; Engholm, G.; Grittner, U.; Bloomfield, K. A socioeconomic deprivation index for small areas in Denmark. Scand. J. Public Health 2013, 41, 560–569. [Google Scholar] [CrossRef] [PubMed]
- Havard, S.; Deguen, S.; Bodin, J.; Louis, K.; Laurent, O.; Bard, D. A small-area index of socioeconomic deprivation to capture health inequalities in France. Soc. Sci. Med. 2008, 67, 2007–2016. [Google Scholar] [CrossRef] [PubMed]
- Rey, G.; Jougla, E.; Fouillet, A.; Hémon, D. Ecological association between a deprivation index and mortality in France over the period 1997 - 2001: Variations with spatial scale, degree of urbanicity, age, gender and cause of death. BMC Public Health 2009, 9, 33. [Google Scholar] [CrossRef] [PubMed]
- Lasbeur, L.; Kaminski, M.; Ancel, P.; Du Mazaubrun, C.; Zeitlin, J. Analyser les inégalités socio-économiques de santé à partir des données du recensement: L’exemple de la grande prématurité à Paris-Petite couronne. Population 2006, 61, 567–584. [Google Scholar] [CrossRef]
- Hagedoorn, P.; Vandenheede, H.; Vanthomme, K.; Willaert, D.; Gadeyne, S. A cohort study into head and neck cancer mortality in Belgium (2001–2011): Are individual socioeconomic differences conditional on area deprivation? Oral Oncol. 2016, 61, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Splichalova, A.; Slachtova, H.; Tomaskova, H.; Polaufova, P. Analysis of Mortality in the Czech Republic Using the Newly Constructed Socioeconomic Deprivation Index. Epidemiology 2007, 18, S19. [Google Scholar] [CrossRef]
- Winkleby, M.; Sundquist, K.; Cubbin, C. Inequities in CHD incidence and case fatality by neighborhood deprivation. Am. J. Prev. Med. 2007, 32, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Ramos, M.; Sánchez, J.; Garrucho, G.; Viciana, F. Inequalities in mortality in Seville. Gac. Sanit. 2004, 18, 16–23. (In Spanish) [Google Scholar] [CrossRef]
- Domínguez-Berjón, M.F.; Borrell, C.; Cano-Serral, G.; Esnaola, S.; Nolasco, A.; Pasarín, M.I.; Ramis, R.; Saurina, C.; Escolar-Pujolar, A. Constructing a deprivation index based on census data in large Spanish cities (the MEDEA project). Gac. Sanit. 2008, 22, 179–187. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Compés Dea, M.L.; Olivan Bellido, E.; Feja Solana, C.; Aguilar Palacio, I.; García-Carpintero Romero Del Hombrebueno, G.; Adiego Sancho, B. Construction of a deprivation index by Basic Healthcare Area in Aragon using Population and Housing Census 2011. Rev. Esp. Salud. Publica. 2018, 92, e201812087. (In Spanish) [Google Scholar]
- Duque, I.; Domínguez-Berjón, M.F.; Cebrecos, A.; Prieto-Salceda, M.D.; Esnaola, S.; Calvo Sánchez, M.; Marí-Dell’Olmo, M. Deprivation index by enumeration district in Spain, 2011. Gac. Sanit. 2021, 35, 113–122. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Álvarez-del Arco, D.; Vicente Sánchez, M.; Alejos, B.; Pascual, C.; Regidor, E. Process and results of constructing a deprivation index for the districts of Madrid and Barcelona, Spain. Rev. Esp. Salud. Publica 2013, 87, 317–329. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Ocaña-Riola, R.; Saurina, C.; Fernández-Ajuria, A.; Lertxundi, A.; Sánchez-Cantalejo, C.; Saez, M.; Ruiz-Ramos, M.; Barceló, M.A.; March, J.C.; Martínez, J.M.; et al. Area deprivation and mortality in the provincial capital cities of Andalusia and Catalonia (Spain). J. Epidemiol. Community Health 2008, 62, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Benach, J.; Yasui, Y. Geographical patterns of excess mortality in Spain explained by two indices of deprivation. J. Epidemiol. Community Health 1999, 53, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Cantalejo, C.; Ocana-Riola, R.; Fernández-Ajuria, A. Deprivation index for small areas in Spain. Soc. Indic. Res. 2008, 89, 259–273. [Google Scholar] [CrossRef]
- García-Gil, C.; Cruz-Rojo, C.; Alvarez-Girón, M.; Solano-Parés, A. Health inequalities in Seville, Spain: Use of indicators of social deprivation and mortality in small areas. Public Health 2004, 118, 11–20. [Google Scholar] [CrossRef]
- Esnaola, S.; Aldasoro, E.; Ruiz, R.; Audicana, C.; Pérez, Y.; Calvo, M. Socioeconomic inequalities in mortality in the Basque Country. Gac. Sanit. 2006, 20, 16–24. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Panczak, R.; Galobardes, B.; Voorpostel, M.; Spoerri, A.; Zwahlen, M.; Egger, M.; Swiss National Cohort and Swiss Household Panel. A Swiss neighbourhood index of socioeconomic position: Development and association with mortality. J. Epidemiol. Community Health 2012, 66, 1129–1136. [Google Scholar] [CrossRef]
- Juhász, A.; Nagy, C.; Páldy, A.; Beale, L. Development of a Deprivation Index and its relation to premature mortality due to diseases of the circulatory system in Hungary, 1998-2004. Soc. Sci. Med. 2010, 70, 1342–1349. [Google Scholar] [CrossRef] [PubMed]
- Caranci, N.; Biggeri, A.; Grisotto, L.; Pacelli, B.; Spadea, T.; Costa, G. The Italian deprivation index at census block level: Definition, description and association with general mortality. Epidemiol. Prev. 2010, 34, 167–176. (In Italian) [Google Scholar] [PubMed]
- Ivaldi, E.; Testi, A. Genoa index of deprivation (GDI): An index of material deprivation for geographical areas. In Social Indicators: Statistics, Trends and Policy Development; Baird, C.M., Ed.; Nova Science Publishers: Hauppauge, NY, USA, 2011. [Google Scholar]
- Cadum, E.; Costa, G.; Biggeri, A.; Martuzzi, M. Deprivation and mortality: A deprivation index suitable for geographical analysis of inequalities. Epidemiol. Prev. 1999, 23, 175–187. (In Italian) [Google Scholar]
- Michelozzi, P.; Perucci, C.A.; Forastiere, F.; Fusco, D.; Ancona, C.; Dell’Orco, V. Inequality in health: Socioeconomic differentials in mortality in Rome, 1990–1995. J. Epidemiol. Community Health 1999, 53, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, A.; Gnavi, R.; Marinacci, C.; Costa, G. Socioeconomic inequalities in coronary heart disease in Italy: A multilevel population-based study. Soc. Sci. Med. 2006, 63, 446–456. [Google Scholar] [CrossRef]
- Haase, T.; Pratschke, J.; Gleeson, J. All-Island Deprivation Index: Towards the development of consistent deprivation measures for the Island of Ireland. Borderl. J. Spat. Plan. Irel. 2012, 2, 21–37. [Google Scholar]
- Salmond, C.E.; Crampton, P. Development of New Zealand’s deprivation index (NZDep) and its uptake as a national policy tool. Can. J. Public Health 2012, 103, S7–S11. [Google Scholar] [PubMed]
- Trewin, D. Socio-Economic Indexes for Areas Australia; Australian Bureau of Statistics: Belconnen, Australian, 2003. [Google Scholar]
- Bell, N.; Schuurman, N.; Oliver, L.; Hayes, V.M. Towards the construction of place specific measures of deprivation: A case study from the Vancouver Metropolitan area. Can. Geogr. 2007, 51, 444–461. [Google Scholar] [CrossRef]
- Pampalon, R.; Raymond, G. A deprivation index for health and welfare planning in Quebec. Chronic. Dis. Can. 2000, 21, 104–113. [Google Scholar]
- Mustard, C.A.; Frohlich, N. Socioeconomic status and the health of the population. Med. Care 1995, 33, DS43–DS54. [Google Scholar] [CrossRef]
- Butler, D.C.; Petterson, S.; Phillips, R.L.; Bazemore, A.W. Measures of social deprivation that predict health care access and need within a rational area of primary care service delivery. Health Serv. Res. 2013, 48, 539–559. [Google Scholar] [CrossRef]
- Andrews, M.R.; Tamura, K.; Claudel, S.E.; Xu, S.; Ceasar, J.N.; Collins, B.S.; Langerman, S.; Mitchell, V.M.; Baumer, Y.; Powell-Wiley, T.M. Geospatial Analysis of Neighborhood Deprivation Index (NDI) for the United States by County. J. Maps 2020, 16, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Miller, B.A.; Hankey, B.F.; Feuer, E.J.; Pickle, L.W. Changing area socioeconomic patterns in U.S. cancer mortality, 1950–1998: Part I—All cancers among men. J. Natl. Cancer Inst. 2002, 94, 904–915. [Google Scholar] [CrossRef] [PubMed]
- Sampson, R.J. Neighborhoods and Violent Crime: A Multilevel Study of Collective Efficacy. Science 1997, 277, 918–924. [Google Scholar] [CrossRef] [PubMed]
- Messer, L.C.; Laraia, B.A.; Kaufman, J.S.; Eyster, J.; Holzman, C.; Culhane, J.; Elo, I.; Burke, J.G.; O’Campo, P. The development of a standardized neighborhood deprivation index. J. Urban Health 2006, 83, 1041–1062. [Google Scholar] [CrossRef] [PubMed]
- Lòpez-De Fede, A.; Stewart, J.E.; Hardin, J.W.; Mayfield-Smith, K. Comparison of small-area deprivation measures as predictors of chronic disease burden in a low-income population. Int. J. Equity Health 2016, 15, 89. [Google Scholar] [CrossRef]
- Brokamp, C.; LeMasters, G.K.; Ryan, P.H. Residential mobility impacts exposure assessment and community socioeconomic characteristics in longitudinal epidemiology studies. J. Expo. Sci. Environ. Epidemiol. 2016, 26, 428–434. [Google Scholar] [CrossRef]
- Wheeler, D.C.; Raman, S.; Jones, R.M.; Schootman, M.; Nelson, E.J. Bayesian deprivation index models for explaining variation in elevated blood lead levels among children in Maryland. Spat. Spatiotemporal Epidemiol. 2019, 30, 100286. [Google Scholar] [CrossRef]
- Dubowitz, T.; Heron, M.; Bird, C.E.; Lurie, N.; Finch, B.K.; Basurto-Dávila, R.; Hale, L.; Escarce, J.J. Neighborhood socioeconomic status and fruit and vegetable intake among whites, blacks, and Mexican Americans in the United States. Am. J. Clin. Nutr. 2008, 87, 1883–1891. [Google Scholar] [CrossRef]
- Townsend, P.; Phillimore, P.; Beattie, A. Health and Deprivation: Inequality and The North; Croom Helm: London, UK, 1988. [Google Scholar]
- Kelly, A.; Sinclair, H. Deprivation and health: Identifying the black spots. J. Health Gain 1997, 1, 13–14. [Google Scholar]
- Diez-Roux, A.V.; Kiefe, C.I.; Jacobs, D.R., Jr.; Haan, M.; Jackson, S.A.; Nieto, F.J.; Paton, C.C.; Schulz, R. Area characteristics and individual-level socioeconomic position indicators in three population-based epidemiologic studies. Ann. Epidemiol. 2001, 11, 395–405. [Google Scholar] [CrossRef]
- Richardson, E.A.; Mitchell, R.; Shortt, N.K.; Pearce, J.; Dawson, T.P. Developing Summary Measures of Health-Related Multiple Physical Environmental Deprivation for Epidemiological Research. Environ. Plan. A Econ. Space 2010, 42, 1650–1668. [Google Scholar] [CrossRef]
- Peyvandi, S.; Baer, R.J.; Chambers, C.D.; Norton, M.E.; Rajagopal, S.; Ryckman, K.K.; Moon-Grady, A.; Jelliffe-Pawlowski, L.L.; Steurer, M.A. Environmental and Socioeconomic Factors Influence the Live-Born Incidence of Congenital Heart Disease: A Population-Based Study in California. J. Am. Heart. Assoc. 2020, 9, e015255. [Google Scholar] [CrossRef] [PubMed]
- Benmarhnia, T.; Laurian, L.; Deguen, S. Measuring spatial environmental deprivation: A new index and its application in France. Environ. Justice 2013, 6, 48–55. [Google Scholar] [CrossRef]
- Colls, C.; Mias, M.; García-Altés, A. A deprivation index to reform the financing model of primary care in Catalonia. Gac. Sanit. 2020, 34, 44–50. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Kolak, M.; Bhatt, J.; Park, Y.H.; Padrón, N.A.; Molefe, A. Quantification of Neighborhood-Level Social Determinants of Health in the Continental United States. JAMA Netw. Open 2020, 3, e1919928. [Google Scholar] [CrossRef]
- Salcedo, N.; Saez, M.; Bragulat, B.; Saurina, C. Does the effect of gender modify the relationship between deprivation and mortality? BMC Public Health 2012, 12, 574. [Google Scholar] [CrossRef]
- Langlois, A.; Kitchen, P. Identifying and Measuring Dimensions of Urban Deprivation in Montreal: An Analysis of the 1996 Census Data. Urban Studies 2001, 38, 119–139. [Google Scholar] [CrossRef]
- Perkins, P.; Royster, M.; Studer, K.; Wibberly, K.; Reed, K.; Henry, K.; Anson-Dwamena, T. Developing Healthy Communities: The Health Opportunity Index. In Proceedings of the American Public Health Association (APHA) 140th Annual Meeting, San Francisco, CA, USA, 27–31 October 2012. [Google Scholar]
- Acevedo-Garcia, D.; McArdle, N.; Hardy, E.F.; Crisan, U.I.; Romano, B.; Norris, D.; Baek, M.; Reece, J. The child opportunity index: Improving collaboration between community development and public health. Health Aff. (Millwood) 2014, 33, 1948–1957. [Google Scholar] [CrossRef]
- Simpson, L. The Department of Environment’s index of local conditions: Don’t touch it. Radic. Stat. 1995, 61, 13–25. [Google Scholar]
- Noble, M.; Lloyd, M.; Wright, G.; Dibben, C.; Smith, G. Developing deprivation measures for Northern Ireland. J. Stat. Soc. Inq. Soc. Irel. 2002, XXXI, 5–25. [Google Scholar]
- Scottish Index of Multiple Deprivation 2004: Summary Technical Report. Available online: https://www.webarchive.org.uk/wayback/archive/20200207120514/https://www2.gov.scot/Topics/Statistics/SIMD/Publications (accessed on 26 October 2021).
- Maizlish, N.; Delaney, T.; Dowling, H.; Chapman, D.A.; Sabo, R.; Woolf, S.; Orndahl, C.; Hill, L.; Snellings, L. California Healthy Places Index: Frames Matter. Public Health Rep. 2019, 134, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Department of the Environment, Transport and the Regions. 1998 Index of Local Deprivation: A Summary of Results; DETR: London, UK, 1998. Available online: https://www.legco.gov.hk/yr99-00/english/bc/bc09/papers/1471e01.pdf (accessed on 26 October 2021).
- McLennan, D.; Noble, S.; Noble, M.; Plunkett, E.; Wright, G.; Gutacker, N. English Indices of Deprivation 2019: Technical Report; Ministry of Housing, Communities & Local Government: London, UK, 2019. [Google Scholar]
- IJpelaar, J.; Power, T.; Green, B. Northern Ireland Multiple Deprivation Measures 2017. J. Stat. Soc. Inq. Soc. Irel. 2018, 48, 163–174. [Google Scholar]
- Welsh Index of Multiple Deprivation (Full Index Update with Ranks): 2019|GOV.WALES. Available online: https://gov.wales/welsh-index-multiple-deprivation-full-index-update-ranks-2019 (accessed on 26 October 2021).
- Scottish index of Multiple Deprivation (Full Index Update with Ranks): 2020|GOV.SCOT. Available online: https://www.gov.scot/collections/scottish-index-of-multiple-deprivation-2020/ (accessed on 26 October 2021).
- Teljeur, C.; Darker, C.D.; Barry, J.; O’Dowd, T. The Trinity National Deprivation Index for Health and Health Services Research 2016. Department of Public Health & Primary Care. Trinity College Dublin. 2019. Available online: https://www.tcd.ie/medicine/public_health_primary_care/assets/pdf/Trinity-deprivation-report-11-2019.pdf (accessed on 26 October 2021).
- Rosano, A.; Pacelli, B.; Zengarini, N.; Costa, G.; Cislaghi, C.; Caranci, N. Update and review of the 2011 Italian deprivation index calculated at the census section level. Epidemiol. Prev. 2020, 44, 162–170. (In Italian) [Google Scholar] [CrossRef] [PubMed]
- Lecoffre, C.; Decool, E.; Olié, V. Mortalité cardio-neuro-vasculaire et désavantage social en France en 2011. Bull. Epidémiol. Hebd. 2016, 20, 352–358. (In French) [Google Scholar]
- Socioeconomic Deprivation Indexes: NZDep and NZiDep, Department of Public Health (Full Index Update). Available online: https://www.otago.ac.nz/wellington/departments/publichealth/research/hirp/otago020194.html (accessed on 26 October 2021).
- Socio-Economic Indexes for Areas (Full Index Update). Available online: https://www.abs.gov.au/websitedbs/censushome.nsf/home/seifa (accessed on 26 October 2021).
- Pampalon, R.; Hamel, D.; Gamache, P.; Simpson, A.; Philibert, M.D. Validation of a deprivation index for public health: A complex exercise illustrated by the Quebec index. Chronic Dis. Inj. Can. 2014, 34, 12–22. [Google Scholar] [CrossRef]
- Metge, C.; Chateau, D.; Prior, H.; Soodeen, R.; De Coster, C.; Barre, L. Composite Measures/Indices of Health and Health System Performance; Manitoba Centre for Health Policy: Winnipeg, MB, Canada, 2009. [Google Scholar]
- Bell, N.; Schuurman, N.; Hayes, M.V. Using GIS-based methods of multicriteria analysis to construct socio-economic deprivation indices. Int. J. Health Geogr. 2007, 6, 17. [Google Scholar] [CrossRef]
- Kind, A.J.H.; Buckingham, W. Making Neighborhood Disadvantage Metrics Accessible: The Neighborhood Atlas. N. Engl. J. Med. 2018, 378, 2456–2458. [Google Scholar] [CrossRef]
- Brokamp, C.; Beck, A.F.; Goyal, N.K.; Ryan, P.; Greenberg, J.M.; Hall, E.S. Material community deprivation and hospital utilization during the first year of life: An urban population-based cohort study. Ann. Epidemiol. 2019, 30, 37–43. [Google Scholar] [CrossRef]
- Sheiham, A. Closing the gap in a generation: Health equity through action on the social determinants of health. A report of the WHO Commission on Social Determinants of Health (CSDH) 2008. Community Dent. Health. 2009, 26, 2–3. [Google Scholar]
- Ribeiro, A.I.; Launay, L.; Guillaume, E.; Launoy, G.; Barros, H. The Portuguese version of the European Deprivation Index: Development and association with all-cause mortality. PLoS ONE 2018, 13, e0208320. [Google Scholar] [CrossRef]
- Poeran, J.; Maas, A.F.; Birnie, E.; Denktas, S.; Steegers, E.A.; Bonsel, G.J. Social deprivation and adverse perinatal outcomes among Western and non-Western pregnant women in a Dutch urban population. Soc. Sci. Med. 2013, 83, 42–49. [Google Scholar] [CrossRef]
- California EnviroScreen: A Tool for Evaluating California Communities; California Department of Pesticide Regulation: Sacramento, CA, USA, 2015. Available online: http://www.cdpr.ca.gov/docs/dept/prec/2015/032015_calenviroscreen.pdf (accessed on 26 October 2021).
- Brook, J.R.; Setton, E.M.; Seed, E.; Shooshtari, M.; Doiron, D. CANUE—The Canadian Urban Environmental Health Research Consortium. The Canadian Urban Environmental Health Research Consortium—A protocol for building a national environmental exposure data platform for integrated analyses of urban form and health. BMC Public Health 2018, 18, 114. [Google Scholar] [CrossRef] [PubMed]
- Hoffimann, E.; Barros, H.; Ribeiro, A.I. Socioeconomic inequalities in green space quality and accessibility—Evidence from a southern European city. Int. J. Environ. Res. Public Health 2017, 14, 916. [Google Scholar] [CrossRef] [PubMed]
- Ouidir, M.; Lepeule, J.; Siroux, V.; Malherbe, L.; Meleux, F.; Rivière, E.; Launay, L.; Zaros, C.; Cheminat, M.; Charles, M.A.; et al. Is atmospheric pollution exposure during pregnancy associated with individual and contextual characteristics? A nationwide study in France. J. Epidemiol. Community Health 2017, 71, 1026–1036. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, A.I.; Krainski, E.T.; Carvalho, M.S.; De Fátima de Pina, M. The influence of socioeconomic deprivation, access to healthcare and physical environment on old-age survival in Portugal. Geospat. Health 2017, 12, 581. [Google Scholar] [CrossRef]
- Gomes, B.; Pinheiro, M.J.; Lopes, S.; de Brito, M.; Sarmento, V.P.; Lopes Ferreira, P.; Barros, H. Risk factors for hospital death in conditions needing palliative care: Nationwide population-based death certificate study. Palliat. Med. 2018, 32, 891–901. [Google Scholar] [CrossRef]
- Bryere, J.; Menvielle, G.; Dejardin, O.; Launay, L.; Molinie, F.; Stucker, I.; Luce, D.; Launoy, G. ICARE group. Neighborhood deprivation and risk of head and neck cancer: A multilevel analysis from France. Oral Oncol. 2017, 71, 144–149. [Google Scholar] [CrossRef]
- Apolinário, D.; Ribeiro, A.I.; Krainski, E.; Sousa, P.; Abranches, M.; Duarte, R. Tuberculosis inequalities and socio-economic deprivation in Portugal. Int. J. Tuberc. Lung Dis. 2017, 21, 784–789. [Google Scholar] [CrossRef]
- Petit, M.; Bryère, J.; Maravic, M.; Pallaro, F.; Marcelli, C. Hip fracture incidence and social deprivation: Results from a French ecological study. Osteoporos. Int. 2017, 28, 2045–2051. [Google Scholar] [CrossRef]
- Economic Commission for Europe of the United Nations (UNECE). Terminology on Statistical Metadata; Statistical Standards and Studies, No. 53; Economic Commission for Europe of the United Nations: Geneva, Switzerland, 2000. [Google Scholar]
- Eurostat. Urban Audit, Methodological Handbook; 2004 edition; Office for Official Publications of the European Communities: Luxembourg, 2004. [Google Scholar]
- OEHHA. December 2010. Cumulative Impacts: Building a Scientific Foundation; p. 3. Available online: https://oehha.ca.gov/media/downloads/calenviroscreen/report/cireport123110.pdf (accessed on 26 October 2021).
- Aubin, I.; Cardou, F.; Boisvert-Marsh, L.; Garnier, E.; Strukelj, M.; Munson, A.D. Managing data locally to answer questions globally: The role of collaborative science in ecology. J. Veg. Sci. 2020, 31, 509–517. [Google Scholar] [CrossRef]

| Sub-Class/Domain | Socio-Economic Index | Material Deprivation Index | Environmental Deprivation Index | Multidimensional Index | Total |
|---|---|---|---|---|---|
| Income and wealth | 18 (44%) | 1 (25%) | - | 11 (91%) | 30 |
| Mobility | 3 (7%) | - | - | - | 3 |
| Employment/occupation | 40 (98%) | 4 (100%) | - | 11 (92%) | 55 |
| Housing | 27 (66%) | 4 (100%) | - | 11 (92%) | 42 |
| Transportation | 12 (28%) | 3 (75%) | - | 4 (36%) | 19 |
| Immigration | 7 (17%) | - | - | 3 (25%) | 10 |
| Social environment | 1 (2%) | - | - | 4 (33%) | 5 |
| Racial composition | 4 (10%) | - | - | 3 (25%) | 7 |
| Communication | 5 (12%) | - | - | 1 (8%) | 6 |
| Family structure/demographics | 26 (63%) | - | - | 6 (50%) | 32 |
| Education | 38 (93%) | - | - | 12 (100%) | 50 |
| Health (sub-class) | - | - | - | 8 (66%) | 8 |
| - | - | - | 1 (8%) | 1 |
| - | - | - | 5 (42%) | 5 |
| - | - | - | 2 (13%) | 2 |
| - | - | - | 3 (25%) | 3 |
| - | - | - | 2 (13%) | 2 |
| - | - | - | 2 (13%) | 2 |
| - | - | - | 6 (50%) | 6 |
| - | - | - | 2 (13%) | 2 |
| - | - | - | 1 (8%) | 1 |
| - | - | - | 1 (8%) | 1 |
| Environmental (sub-class) | - | - | 3 (100%) | 10 (83%) | 13 |
| - | - | - | 7 (58%) | 7 |
| - | - | - | 2 (13%) | 2 |
| - | - | 3 (100%) | 4 (33%) | 7 |
| - | - | 2 (66%) | 1 (8%) | 3 |
| - | - | 3 (100%) | 2 (13%) | 5 |
| - | - | 1 (33%) | 1 (8%) | 2 |
| - | - | 1 (8%) | 1 | |
| - | - | 1 (33%) | 1 | |
| - | - | 1 (33%) | 1 | |
| - | - | 1 (33%) | 2 (13%) | 3 |
| Total | 41 (100%) | 4 (100%) | 3 (100%) | 12 (100%) | 60 (100%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zelenina, A.; Shalnova, S.; Maksimov, S.; Drapkina, O. Classification of Deprivation Indices That Applied to Detect Health Inequality: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 10063. https://doi.org/10.3390/ijerph191610063
Zelenina A, Shalnova S, Maksimov S, Drapkina O. Classification of Deprivation Indices That Applied to Detect Health Inequality: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(16):10063. https://doi.org/10.3390/ijerph191610063
Chicago/Turabian StyleZelenina, Anastasia, Svetlana Shalnova, Sergey Maksimov, and Oksana Drapkina. 2022. "Classification of Deprivation Indices That Applied to Detect Health Inequality: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 16: 10063. https://doi.org/10.3390/ijerph191610063
APA StyleZelenina, A., Shalnova, S., Maksimov, S., & Drapkina, O. (2022). Classification of Deprivation Indices That Applied to Detect Health Inequality: A Scoping Review. International Journal of Environmental Research and Public Health, 19(16), 10063. https://doi.org/10.3390/ijerph191610063