
Relationship between Preventive Health Behavior, Optimistic Bias, Hypochondria, and Mass Psychology in Relation to the Coronavirus Pandemic among Young Adults in Korea


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Enrollment
2.3. Measurement
2.3.1. Optimistic Bias
2.3.2. Hypochondriasis
2.3.3. Mass Psychology
2.3.4. Preventive Health Behavior
2.4. Data Collection and Ethical Consideration
2.5. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Difference between Optimistic Bias, Hypochondriasis, and Mass Psychology Associated with Participants’ Characteristics
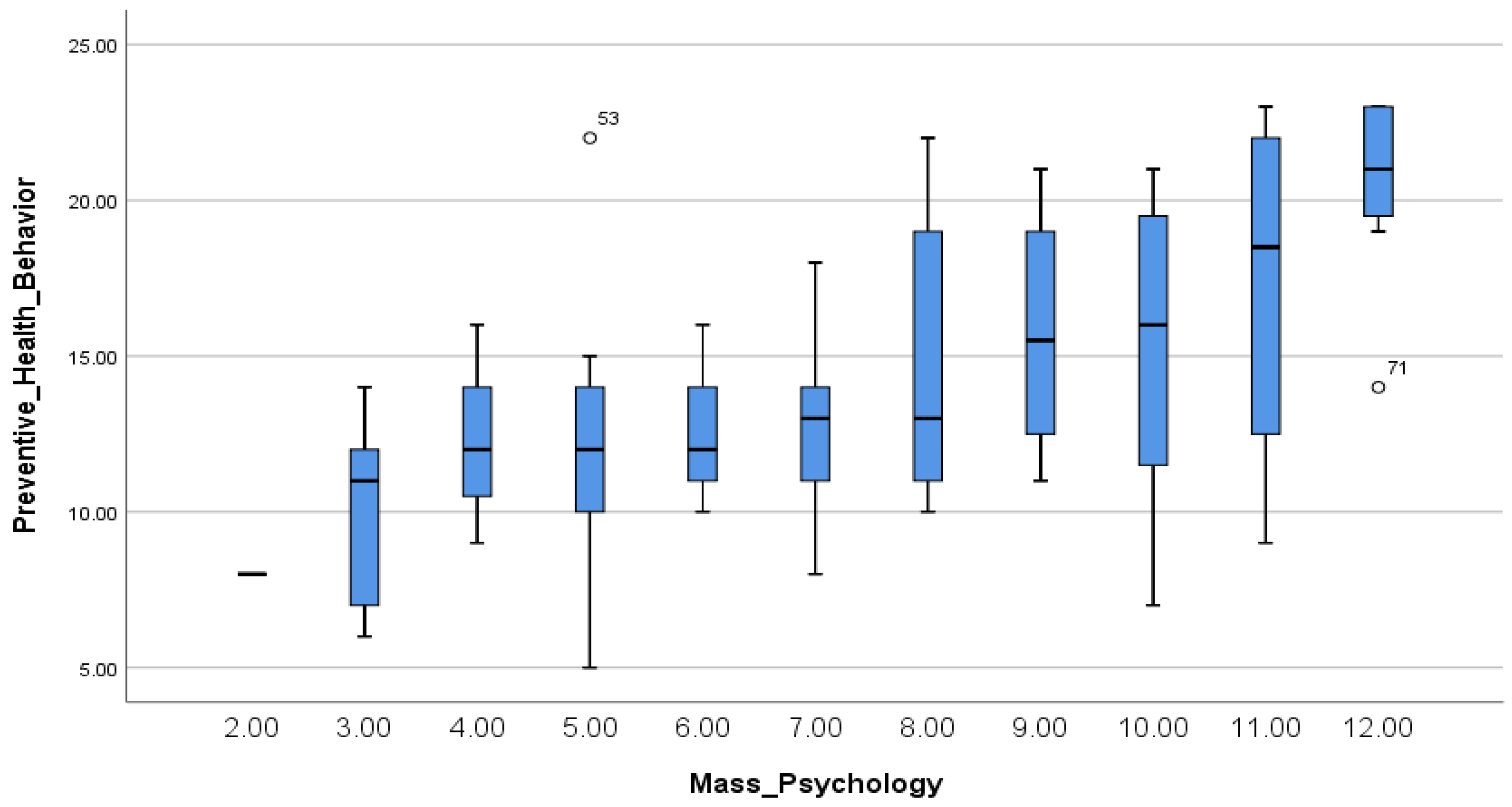
3.3. Relationship between Preventive Health Behavior, Optimistic Bias, Hypochondria, and Mass Psychology
3.4. Preventive Health Behavior by Optimistic Bias, Hypochondria, and Mass Psychology
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/?mapFilter=cases (accessed on 1 August 2022).
- KDCA. Coronavirus (COVID-19), Republic of Korea. Available online: http://ncov.mohw.go.kr/en/ (accessed on 1 August 2022).
- Bish, A.; Michie, S. Demographic and Attitudinal Determinants of Protective Behaviors during Pandemic: A review. Br. J. Health Psychol. 2010, 15, 797–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.; Kim, S. Analysis of the Impact of Health Beliefs and Resource Factors on Preventive Behaviors against the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 8666. [Google Scholar] [CrossRef]
- Kim, J.H.; Yoon, Y.M. An Experimental Study on the Factors Affecting Persuasiveness of Health Messages in AIDS Campaign. Public Relat. 2010, 14, 83–123. [Google Scholar] [CrossRef]
- Weinstein, N.D. Why It Won’t Happen to Me: Perceptions of Risk Factors and Susceptibility. Health Psychol. 1984, 2, 11–20. [Google Scholar] [CrossRef]
- Fragkaki, I.; Maciejewski, D.F.; Weijman, E.L.; Feltes, J.; Cima, M. Human Responses to Covid-19: The Role of Optimism Bias, Perceived Severity, and Anxiety. Personal. Individ. Differ. 2021, 176, 110781. [Google Scholar] [CrossRef]
- Sharot, T. The Optimism bias. Curr. Biol. 2011, 21, R941–R945. [Google Scholar] [CrossRef] [Green Version]
- Park, T.; Ju, I.; Ohs, J.E.; Hinsley, A. Optimistic Bias and Preventive Behavioral Engagement in the Context of COVID-19. Res. Soc. Adm. Pharm. 2021, 17, 1859–1866. [Google Scholar] [CrossRef]
- McColl, K.; Debin, M.; Souty, C.; Guerrisi, C.; Turbelin, C.; Falchi, A.; Bonmarin, I.; Paolotti, D.; Obi, C.; Duggan, J.; et al. Are People Optimistically Biased About the Risk of COVID-19 Infection? Lessons from the First Wave of the Pandemic in Europe. Int. J. Environ. Res. Public Health 2021, 19, 436. [Google Scholar] [CrossRef]
- Warwick, H.M.; Salkovskis, P.M. Hypochondriasis. Behav. Res. Ther. 1990, 28, 105–117. [Google Scholar] [CrossRef]
- Olatunji, B.O.; Deacon, B.J.; Abramowitz, J.S. Is Hypochondriasis an Anxiety Disorder? Br. J. Psychiatry 2009, 194, 481–482. [Google Scholar] [CrossRef]
- Lee, I.H. A Relationship of Personality and Hypochondriacal Illness Attitudes. Korean J. Health Psychol. 2009, 14, 293–311. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Kim, J.H.; Cho, Y.R. Roles of Cognitive Vulnerability and Emotion Dysregulation in Hypochondriacal and Social Anxiety Symptoms Among Undergraduates. Cogn. Behav. Ther. 2015, 15, 113–136. [Google Scholar]
- Lee, I.H. Factor Structure of the Illness Attitudes Scale (IAS) in a Korean College Sample. Korean J. Health Psychol. 2004, 9, 203–218. [Google Scholar]
- Yamaguchi, S. Biased Risk Perceptions Among Japanese: Illusion of Interdependence among Risk Companions. Asian J. Soc. Psychol. 1998, 1, 117–131. [Google Scholar] [CrossRef]
- Ho, A.S.Y.; Leung, K. Group Size Effects on Risk Perception: A Test of Several Hypotheses. Asian J. Soc. Psychol. 1998, 1, 133–145. [Google Scholar] [CrossRef]
- Lee, D.S. A Structural Model Development of Health Insensitivity in Korean Adult. Korean J. Adult Nurs. 2004, 16, 355–365. [Google Scholar]
- Rubin, G.J.; Amlot, R.; Page, L.; Wessely, S. Public Perception, Anxiety, and Behavior Change in Relation to the Swine Flu Outbreak: Cross Sectional Telephone Survey. BMJ 2009, 339, b2651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.; Kim, B.; Kim, K.A. Preventive Behavioral Insights for Emerging Adults: A Survey during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 2569. [Google Scholar] [CrossRef]
- Clarke, V.A.; Lovegrove, H.; Williams, A.; Machperson, M. Unrealistic Optimism and Health Belief Model. J. Behav. Med. 2000, 23, 367–376. [Google Scholar] [CrossRef]
- Kellner, R. Hypochondriasis and Somatization. JAMA 1987, 258, 2718–2722. [Google Scholar] [CrossRef]
- Lee, J.S. The Catastrophizing Tendency of Individuals with High Health Anxiety. Master’s Thesis, Seoul National University, Seoul, Korea, 2004. [Google Scholar]
- Cho, S.Y. A Study on the Relationship Between Cervical Cancer Preventive Behavioral Intentions and Optimistic Bias among Korean Female College Students. Korean J. Commun. Stud. 2018, 26, 101–124. [Google Scholar] [CrossRef]
- Trobst, K.K.; Wiggins, J.S.; Costa, P.T.; Herbst, J.H.; McCrae, R.R.; Masters, H.L. Personality Psychology and Problem Behaviors: HIV Risk and the Five-Factor Model. J. Pers. 2000, 68, 1233–1252. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Kim, S. A Meta-Analytic Review of Koreans’ Cultural Self-Orientation: Focusing on Collectivism and Individualism. Locality Glob. 2018, 42, 5–37. [Google Scholar] [CrossRef]
- Kim, C.D. The Coping Process of Koreans as Compared to White Americans: The Influence of Culture. Korea J. Youth Couns. 1994, 2, 96–113. [Google Scholar]
- Baek, S.Y. A Study on Factors Affecting National Cancer Prevention Practices Health Behavior of Nursing Students. J. Digit. Converg. 2020, 18, 29–37. [Google Scholar] [CrossRef]
- Adachi, M.; Murakami, M.; Yoneoka, D.; Kawashima, T.; Hashizume, M.; Sakamoto, H.; Eguchi, A.; Ghaznavi, C.; Gilmour, S.; Kaneko, S.; et al. Factors Associated with the Risk Perception of COVID-19 Infection and Severe Illness: A Cross-Sectional Study in Japan. SSM Popul. Health 2021, 18, 101–105. [Google Scholar] [CrossRef]
- Son, H.J.; Lee, K.E. The Influence of Health Concern, Health Anxiety, and Communication with Healthcare Providers on Health Information Seeking Behavior on the Internet. J. Health Info. Stat. 2019, 44, 73–82. [Google Scholar] [CrossRef]
- Kim, D.J. Factors Affecting Preventive Behavior for COVID-19 in the Prolonged Pandemic: Focusing on HBM, RISP, Optimistic Bias, and Emotion. Locality Commun. 2022, 26, 5–35. [Google Scholar] [CrossRef]
- Kwon, M.S.; Choi, Y. Factors Affecting Preventive Behavior related to Tuberculosis among University Students in Korea: Focused on Knowledge, Attitude and Optimistic Bias related to Tuberculosis. J. Korean Acad. Fundam. Nurs. 2020, 27, 236–245. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | Mean ± SD | Category | n (%) | Normality Test † | |
|---|---|---|---|---|---|
| Kolmogorov–Smirnov (p) | Shapiro–Wilk (p) | ||||
| Age (year) | 25.40 ± 2.79 | ≤25 | 27 (30.0) | ||
| ≥26 | 63 (70.0) | ||||
| Gender | Male | 38 (41.8) | |||
| Female | 53 (58.2) | ||||
| Experience of COVID-19 | Yes | 50 (54.9) | |||
| No | 41 (45.1) | ||||
| Experience of illness (including COVID-19) | Yes | 67 (73.6) | |||
| No | 24 (26.4) | ||||
| Present illness | Yes | 10 (11.0) | |||
| No | 81 (89.0) | ||||
| History of hospital administration | Yes | 52 (57.1) | |||
| No | 39 (42.9) | ||||
| Preventive health behavior † | 14.15 ± 4.42 | Lower than 25% (≤11) | 28 (30.8) | 0.130 (0.001) | 0.962 (0.010) |
| 25–75% (12–16) | 36 (39.6) | ||||
| Higher than 75% (≥17) | 27 (29.7) | ||||
| Optimistic bias † | 0.34 ± 1.12 | Negative (−) | 9 (9.9) | 0.290 (0.000) | 0.830 (0.000) |
| Neutral (0) | 52 (57.1) | ||||
| Positive (+) | 30 (33.0) | ||||
| Hypochondria † | 30.73 ± 13.54 | Lower than 25% (≤21) | 23 (25.3) | 0.108 (0.011) | 0.948 (0.001) |
| 25–75% (22–37) | 45 (79.5) | ||||
| Higher than 75% (≥38) | 23 (25.3) | ||||
| Mass psychology † | 7.58 ± 2.49 | Lower than 25% (≤6) | 33 (36.3) | 0.100 (0.026) | 0.968 (0.023) |
| 25–75% (7–9) | 35 (38.5) | ||||
| Higher than 75% (≥10) | 23 (25.3) | ||||
| PHB | Mean | SD | Median | Mode |
|---|---|---|---|---|
| PHB1 (hand washing) | 1.93 | 1.02 | 2 | 3 |
| PHB2 (wearing mask) | 3.10 | 0.97 | 3 | 4 |
| PHB3 (social distancing) | 2.16 | 1.13 | 2 | 2 |
| PHB4 (hydration) | 1.79 | 1.25 | 2 | 1 |
| PHB5 (influenza vaccination) | 1.65 | 1.44 | 1 | 0 |
| PHB6 (COVID-19 vaccination) | 2.53 | 0.77 | 3 | 3 |
| Variables | Category | Preventive Health Behavior | Optimistic Bias | Hypochondria | Mass Psychology | ||||
|---|---|---|---|---|---|---|---|---|---|
| M ± SD | Z (p) † | M ± SD | Z (p) † | M ± SD | Z (p) † | M ± SD | Z (p) † | ||
| Age (year) | ≤25 | 14.04 ± 4.51 | −0.049 (0.961) | 0.40 ± 1.18 | −0.504 (0.614) | 33.25 ± 14.87 | −0.877 (0.381) | 6.63 ± 2.59 | −2.514 (0.012) |
| ≥26 | 14.11 ± 4.38 | 0.31 ± 1.10 | 29.43 ± 12.89 | 7.97 ± 2.38 | |||||
| Gender | Male | 14.26 ± 4.98 | −0.065 (0.948) | 0.45 ± 1.20 | −0.036 (0.971) | 30.21 ± 12.77 | −0.125 (0.901) | 7.79 ± 2.51 | −0.596 (0.551) |
| Female | 14.08 ± 4.01 | 0.26 ± 1.06 | 31.09 ± 14.18 | 7.43 ± 2.50 | |||||
| Experience of COVID-19 | Yes | 13.62 ± 4.09 | −1.161 (0.246) | 0.22 ± 0.91 | −1.597 (0.110) | 33.50 ± 13.88 | −2.567 (0.010) | 7.18 ± 2.41 | −1.326 (0.185) |
| No | 14.80 ± 4.77 | 0.49 ± 1.33 | 27.34 ± 12.46 | 8.07 ± 2.53 | |||||
| Experience of Illness (including COVID-19) | Yes | 13.84 ± 4.19 | −1.075 (0.282) | 0.16 ± 1.07 | −2.592 (0.010) | 33.31 ± 13.97 | −3.259 (0.001) | 7.28 ± 2.42 | −1.737 (0.082) |
| No | 15.04 ± 4.98 | 0.83 ± 1.13 | 23.50 ± 9.17 | 8.42 ± 2.57 | |||||
| Present illness | Yes | 14.40 ± 5.30 | −0.006 (0.995) | −0.60 ± 1.71 | −2.109 (0.035) | 36.20 ± 19.40 | −0.086 (0.388) | 7.70 ± 2.67 | −0.064 (0.949) |
| No | 14.12 ± 4.34 | 0.46 ± 0.98 | 30.05 ± 12.64 | 7.57 ± 2.49 | |||||
| History of hospital administration | Yes | 14.09 ± 3.70 | −0.402 (0.687) | 0.23 ± 1.26 | −1.015 (0.310) | 30.33 ± 13.38 | −0.490 (0.624) | 7.73 ± 2.02 | −0.590 (0.555) |
| No | 14.23 ± 5.28 | 0.49 ± 0.88 | 31.26 ± 13.91 | 7.38 ± 3.03 | |||||
| Preventive Health Behavior | Optimistic Bias | Hypochondria | Mass Psychology | |
|---|---|---|---|---|
| Preventive health behavior | 1 | −0.072 (0.495) | 0.188 (0.075) | 0.509 (0.000) † |
| Optimistic bias | 1 | −0.111 (0.293) | 0.02 (0.868) | |
| Hypochondria | 1 | −0.017 (0.875) | ||
| Mass psychology | 1 |
| Preventive Health Behavior | ||||||
|---|---|---|---|---|---|---|
| Group | n (%) | Mean Rank ± SE | χ2 † | p | Post Hoc | |
| Optimistic bias | Negative (−) | 9 (9.9) | 14.89 ± 1.41 | 0.663 | 0.718 | |
| Neutral (0) | 52 (57.1) | 14.27 ± 0.59 | ||||
| Positive (+) | 30 (33.0) | 13.73 ± 0.87 | ||||
| Hypochondria | Lower than 25% | 23 (25.3) | 12.87 ± 0.94 | 4.439 | 0.109 | |
| 25–75% | 45 (79.5) | 14.22 ± 0.62 | ||||
| Higher than 75% | 23 (25.3) | 15.30 ± 0.98 | ||||
| Mass psychology | Lower than 25% a | 33 (36.3) | 11.82 ± 0.58 | 18.348 | 0.000 | a < b, a < c, b = c |
| 25–75% b | 35 (38.5) | 14.34 ± 0.64 | ||||
| Higher than 75% c | 23 (25.3) | 17.22 ± 1.00 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, D.-S.; Koo, H.-J.; Choi, S.-O.; Kim, J.-I.; Kim, Y.S. Relationship between Preventive Health Behavior, Optimistic Bias, Hypochondria, and Mass Psychology in Relation to the Coronavirus Pandemic among Young Adults in Korea. Int. J. Environ. Res. Public Health 2022, 19, 9620. https://doi.org/10.3390/ijerph19159620
Lee D-S, Koo H-J, Choi S-O, Kim J-I, Kim YS. Relationship between Preventive Health Behavior, Optimistic Bias, Hypochondria, and Mass Psychology in Relation to the Coronavirus Pandemic among Young Adults in Korea. International Journal of Environmental Research and Public Health. 2022; 19(15):9620. https://doi.org/10.3390/ijerph19159620
Chicago/Turabian StyleLee, Dong-Suk, Hyun-Ju Koo, Seung-Ok Choi, Ji-In Kim, and Yeon Sook Kim. 2022. "Relationship between Preventive Health Behavior, Optimistic Bias, Hypochondria, and Mass Psychology in Relation to the Coronavirus Pandemic among Young Adults in Korea" International Journal of Environmental Research and Public Health 19, no. 15: 9620. https://doi.org/10.3390/ijerph19159620
APA StyleLee, D.-S., Koo, H.-J., Choi, S.-O., Kim, J.-I., & Kim, Y. S. (2022). Relationship between Preventive Health Behavior, Optimistic Bias, Hypochondria, and Mass Psychology in Relation to the Coronavirus Pandemic among Young Adults in Korea. International Journal of Environmental Research and Public Health, 19(15), 9620. https://doi.org/10.3390/ijerph19159620