
Association between Family Dysfunction and Post-Traumatic Stress Disorder in School Students during the Second COVID-19 Epidemic Wave in Peru



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
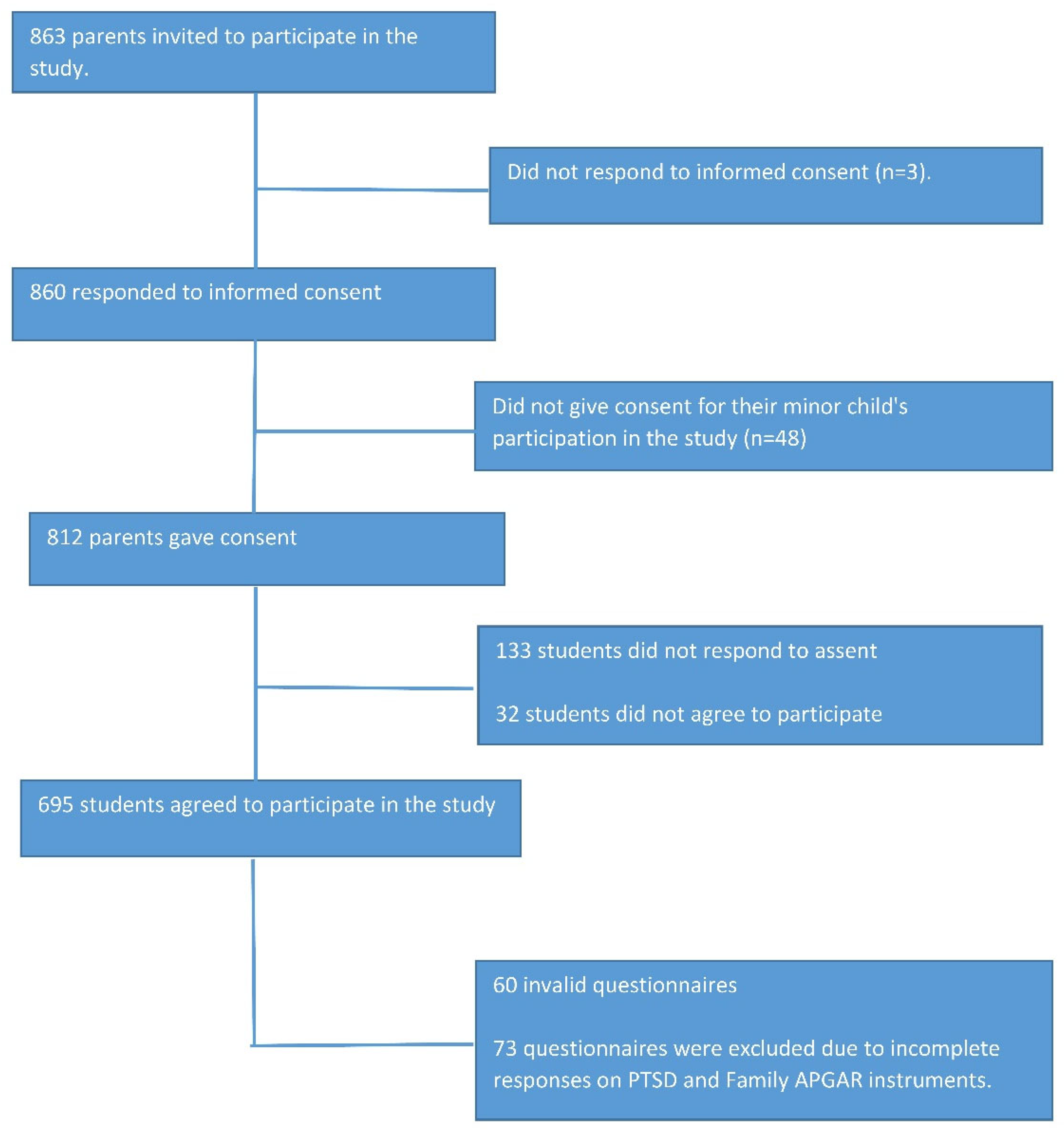
2.2. Population and Sample
2.3. Data Collection Procedures
2.4. Instruments
2.5. Variables
2.6. Data Analysis
2.7. Ethical Aspects
3. Results
4. Discussion
4.1. Prevalence of Post-Traumatic Stress
4.2. Family Dysfunction and Post-Traumatic Stress
4.3. Other Factors Associated with Post-Traumatic Stress
4.4. Implications of Findings in Mental Health Policy
4.5. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cid Rodríguez, M.d.C.; Montes de Oca Ramos, R.; Hernandez Díaz, O. La Familia En El Cuidado de La Salud. Rev. Méd. Electr. 2014, 36, 462–472. [Google Scholar]
- La Influencia de La Funcionalidad Familiar En El Riesgo Suicida y Trastorno Depresivo En Adolescentes Del Cantón Puerto Quito. Available online: http://repositorio.puce.edu.ec/handle/22000/12860 (accessed on 3 March 2022).
- Trastorno de Estrés Postraumático en Niños y Adolescentes. Revisión del Concepto y Actualizaciones. Available online: https://psiquiatria.com/bibliopsiquis/trastorno-de-estres-postraumatico-en-ninos-y-adolescentes-revision-del-concepto-y-actualizaciones (accessed on 3 March 2022).
- Bhushan, B.; Basu, S.; Ganai, U.J. Post-Traumatic Stress and Growth Among the Children and Adolescents in the Aftermath of COVID-19. Front. Psychol. 2022, 12. [Google Scholar] [CrossRef]
- Selçuk, E.B.; Demir, A.Ç.; Erbay, L.G.; Özcan, Ö.Ö.; Gürer, H.; Dönmez, Y.E. Anxiety, Depression and Post-Traumatic Stress Disorder Symptoms in Adolescents during the COVID-19 Outbreak and Associated Factors. Int. J. Clin. Pract. 2021, 75, e14880. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Related Posttraumatic Stress Disorder in Children and Adolescents in Saudi Arabia. Available online: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0255440 (accessed on 4 November 2021).
- Palacio-Ortiz, J.D.; Londoño-Herrera, J.P.; Nanclares-Márquez, A.; Robledo-Rengifo, P.; Quintero-Cadavid, C.P. Trastornos psiquiátricos en los niños y adolescentes en tiempo de la pandemia por COVID-19. Rev. Colomb. Psiquiatr. 2020, 49, 279–288. [Google Scholar] [CrossRef]
- Garibay-Ramirez, J.; Jiménez-Garcés, C.; Vieyra-Reyes, P.; Hernández-González, M.M.; Villalón-López, J. Disfunción familiar y depresión en niños de 8-12 años de edad. Rev. Med. E Investig. 2014, 2, 107–111. [Google Scholar] [CrossRef]
- Escobar Sáez, M.J. Disfunción Familiar En Adolescentes de Quinto de Secundaría de Un Colegio Público y Un Colegio Privado En El Distrito de La Molina; Universidad de Lima, Lima, Peru: 2015. Available online: https://repositorio.ulima.edu.pe/handle/20.500.12724/1721 (accessed on 15 June 2022).
- Vásquez Coba, C.X. El Estrés Postraumático y las Condiciones Familiares, en los Niños y Adolescentes. 2011. Available online: http://www.dspace.uce.edu.ec/handle/25000/1202 (accessed on 15 June 2022).
- Alderfer, M.A.; Navsaria, N.; Kazak, A.E. Family Functioning and Posttraumatic Stress Disorder in Adolescent Survivors of Childhood Cancer. J. Fam. Psychol. JFP J. Div. Fam. Psychol. Am. Psychol. Assoc. Div. 2009, 23, 717–725. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research Electronic Data Capture (REDCap)—A Metadata-Driven Methodology and Workflow Process for Providing Translational Research Informatics Support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap Consortium: Building an International Community of Software Platform Partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Suarez Cuba, M.A.; Alcalá Espinoza, M. Apgar familiar: Una herramienta para detectar disfunción familiar. Rev. Méd. Paz 2014, 20, 53–57. [Google Scholar]
- Smilkstein, G.; Ashworth, C.; Montano, D. Validity and Reliability of the Family APGAR as a Test of Family Function. J. Fam. Pract. 1982, 15, 303–311. [Google Scholar]
- Bellón Saameño, J.A.; Delgado Sánchez, A.; Luna del Castillo, J.d.D.; Lardelli Claret, P. Validez y fiabilidad del cuestionario de función familiar Apgar-familiar. Aten. Primaria 1996, 18, 289–296. [Google Scholar] [PubMed]
- Cabello, H.C.; Rodríguez, T.C.; León, J.L.V.; Barboza, M.P.; De la Cruz Valles, M. Análisis factorial confirmatorio de la escala de percepción del funcionamiento familiar de Smilkstein en adolescentes peruanos. Salud Soc. 2015, 6, 140–153. [Google Scholar] [CrossRef]
- Rincón, P.; Gysling, M.; Jiménez, C.; Lloyd, S.; Navarro, M.F.; Retamal, L.; Cova, F.; Valdivia, M.; Pérez-Salas, C.P.; Melipillán, R.; et al. Propiedades Psicométricas de La Escala de Síntomas de TEPT Para Niños (CPSS) En Población Chilena Afectada Por El Terremoto y Tsunami Del 27-F de 2010. Ter. Psicol. 2014, 32, 57–64. [Google Scholar] [CrossRef]
- Bustos, P.; Rincón, P.; Aedo, J. Validación Preliminar de La Escala Infantil de Síntomas Del Trastorno de Estrés Postraumático (Child PTSD Symptom Scale, CPSS) En Niños/as y Adolescentes Víctimas de Violencia Sexual. Psykhe Santiago 2009, 18, 113–126. [Google Scholar] [CrossRef]
- Campbell-Sills, L.; Stein, M.B. Psychometric Analysis and Refinement of the Connor-Davidson Resilience Scale (CD-RISC): Validation of a 10-Item Measure of Resilience. J. Trauma. Stress 2007, 20, 1019–1028. [Google Scholar] [CrossRef] [PubMed]
- Escala de Resiliencia de Connor-Davidson (CD-RISC). Available online: https://www.researchgate.net/publication/277139516_Escala_de_Resiliencia_de_Connor-Davidson_CD-RISC (accessed on 14 June 2019).
- Blanco, V.; Guisande, M.A.; Sánchez, M.T.; Otero, P.; Vázquez, F.L. Spanish Validation of the 10-Item Connor-Davidson Resilience Scale (CD-RISC 10) with Non-Professional Caregivers. Aging Ment. Health 2019, 23, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Dolores Serrano-Parra, M.; Garrido-Abejar, M.; Notario-Pacheco, B.; Bartolomé-Gutiérrez, R.; Solera-Martínez, M.; Martínez-Vizcaíno, V. Validity of the Connor-Davidson resilience scale (10 items) in a population of elderly. Enferm. Clin. 2013, 23, 14–21. [Google Scholar] [CrossRef]
- Notario-Pacheco, B.; Martínez-Vizcaíno, V.; Trillo-Calvo, E.; Pérez-Yus, M.C.; Serrano-Parra, D.; García-Campayo, J. Validity and Reliability of the Spanish Version of the 10-Item CD-RISC in Patients with Fibromyalgia. Health Qual. Life Outcomes 2014, 12, 14. [Google Scholar] [CrossRef] [PubMed]
- Notario-Pacheco, B.; Solera-Martínez, M.; Serrano-Parra, M.D.; Bartolomé-Gutiérrez, R.; García-Campayo, J.; Martínez-Vizcaíno, V. Reliability and Validity of the Spanish Version of the 10-Item Connor-Davidson Resilience Scale (10-Item CD-RISC) in Young Adults. Health Qual. Life Outcomes 2011, 9, 63. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Ventura Bances, M.P. Eficacia de un programa de intervención grupal cognitivo-conductual para disminuir el trastorno de ansiedad generalizada en pacientes del Puesto de Salud Las Dunas-Surco. Univ. Nac. Mayor San Marcos 2009. Available online: https://cybertesis.unmsm.edu.pe/handle/20.500.12672/618 (accessed on 15 June 2022).
- Mills, S.D.; Fox, R.S.; Malcarne, V.L.; Roesch, S.C.; Champagne, B.R.; Sadler, G.R. The Psychometric Properties of the Generalized Anxiety Disorder-7 Scale in Hispanic Americans with English or Spanish Language Preference. Cultur. Divers. Ethnic Minor. Psychol. 2014, 20, 463–468. [Google Scholar] [CrossRef]
- Villarreal-Zegarra, D.; Copez-Lonzoy, A.; Bernabé-Ortiz, A.; Melendez-Torres, G.J.; Bazo-Alvarez, J.C. Valid Group Comparisons Can Be Made with the Patient Health Questionnaire (PHQ-9): A Measurement Invariance Study across Groups by Demographic Characteristics. PLoS ONE 2019, 14, e0221717. [Google Scholar] [CrossRef]
- Yoon, S.; Lee, Y.; Han, C.; Pae, C.-U.; Yoon, H.-K.; Patkar, A.A.; Steffens, D.C.; Kim, Y.-K. Usefulness of the Patient Health Questionnaire-9 for Korean Medical Students. Acad. Psychiatry J. Am. Assoc. Dir. Psychiatr. Resid. Train. Assoc. Acad. Psychiatry 2014, 38, 661–667. [Google Scholar] [CrossRef]
- Marshall, R.D.; Schneier, F.R.; Lin, S.H.; Simpson, H.B.; Vermes, D.; Liebowitz, M. Childhood Trauma and Dissociative Symptoms in Panic Disorder. Am. J. Psychiatry 2000, 157, 451–453. [Google Scholar] [CrossRef] [PubMed]
- Cuneo, C.; González, I.; Jara, M.; Palomares, L.; Rammasy, C.; Cruz, C.; Florenzano, R. Validación Externa de La Escala de Trauma de Marshall. In Trauma Infanto-Juvenil y Psicopatología Adulta; Florenzano, R., Weil, K., Carvajal, C., Cruz, C., Eds.; Universidad de los Andes: Cundinamarca, Colombia, 2005; Chapter 9. [Google Scholar] [CrossRef]
- Cáceres-Taco, E.; Vásquez-Gómez, F. Intento suicida y antecedente de experiencias traumáticas durante la infancia en adultos con diagnóstico de depresión, trastorno de personalidad limítrofe o esquizofrenia. Rev. Neuropsiquiatr. 2013, 76, 255. [Google Scholar] [CrossRef]
- Ballesteros, T.S.; Vitriol, G.V.; Florenzano, U.R.; Vacarezza, L.A.; Calderón, K.A. Mujeres Con Depresión Severa: Relación Entre Trauma Infantil y Gravedad de Síntomas Clínicos. Rev. Chil. Neuro-Psiquiatr. 2007, 45, 288–295. [Google Scholar] [CrossRef][Green Version]
- Saunders, J.B.; Aasland, O.G.; Amundsen, A.; Grant, M. Alcohol Consumption and Related Problems among Primary Health Care Patients: WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption—I. Addict. Abingdon Engl. 1993, 88, 349–362. [Google Scholar] [CrossRef]
- Saunders, J.B.; Aasland, O.G.; Babor, T.F.; de la Fuente, J.R.; Grant, M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption—II. Addict. Abingdon Engl. 1993, 88, 791–804. [Google Scholar] [CrossRef]
- Rubio Valladolid, G.; Bermejo Vicedo, J.; Caballero Sánchez-Serrano, M.C.; Santo-Domingo Carrasco, J. Validación de La Prueba Para La Identificación de Trastornos Por Uso de Alcohol (AUDIT) En Atención Primaria. Rev. Clín. Esp. 1998, 198, 11–14. [Google Scholar]
- Cuestionario AUDIT Para La Detección Del Consumo de Alcohol. Available online: https://www.msdmanuals.com/medical-calculators/AlcoholScreen-es.htm (accessed on 11 January 2022).
- Wathelet, M.; Fovet, T.; Jousset, A.; Duhem, S.; Habran, E.; Horn, M.; Debien, C.; Notredame, C.-E.; Baubet, T.; Vaiva, G.; et al. Prevalence of and Factors Associated with Post-Traumatic Stress Disorder among French University Students 1 Month after the COVID-19 Lockdown. Transl. Psychiatry 2021, 11, 327. [Google Scholar] [CrossRef] [PubMed]
- Shek, D.T.L.; Zhao, L.; Dou, D.; Zhu, X.; Xiao, C. The Impact of Positive Youth Development Attributes on Posttraumatic Stress Disorder Symptoms Among Chinese Adolescents Under COVID-19. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2021, 68, 676–682. [Google Scholar] [CrossRef]
- Yang, L.; Wu, M.; Wang, Y.; Peng, B. The Influence of Family Function on State Anxiety of Chinese College Students During the Epidemic of COVID-19. Front. Psychol. 2021, 12, 701945. [Google Scholar] [CrossRef]
- Hinojos-Gallardo, L.C.; Ruiz-Escalona, L.; Cisneros-Castolo, M.; Mireles-Vega, E.; Pando-Tarín, G.A.; Bejarano-Marín, J.M. Estrés postraumático en la población pediátrica atendida en el Hospital Infantil del estado de Chihuahua, México. Bol. Méd. Hosp. Infant. México 2011, 68, 290–295. [Google Scholar]
- Guo, L.; Tian, L.; Scott Huebner, E. Family Dysfunction and Anxiety in Adolescents: A Moderated Mediation Model of Self-Esteem and Perceived School Stress. J. Sch. Psychol. 2018, 69, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Browne, D.T.; Wade, M.; May, S.S.; Jenkins, J.M.; Prime, H. COVID-19 Disruption Gets inside the Family: A Two-Month Multilevel Study of Family Stress during the Pandemic. Dev. Psychol. 2021, 57, 1681–1692. [Google Scholar] [CrossRef]
- Cohodes, E.M.; McCauley, S.; Gee, D.G. Parental Buffering of Stress in the Time of COVID-19: Family-Level Factors May Moderate the Association Between Pandemic-Related Stress and Youth Symptomatology. Res. Child Adolesc. Psychopathol. 2021, 49, 935–948. [Google Scholar] [CrossRef]
- Zeng, Y.; Ye, B.; Zhang, Y.; Yang, Q. Family Cohesion and Stress Consequences Among Chinese College Students During COVID-19 Pandemic: A Moderated Mediation Model. Front. Public Health 2021, 9, 703899. [Google Scholar] [CrossRef] [PubMed]
- Migliorini, C.; Lam, D.S.-M.; Harvey, C. Supporting Family and Friends of Young People with Mental Health Issues Using Online Technology: A Rapid Scoping Literature Review. Early Interv. Psychiatry 2021, 2021, 1–23. [Google Scholar] [CrossRef]
- Asociaciones Entre Exposición a Traumas, Trastorno de Estrés Postraumático y Síntomas de Depresión en Adolescentes Sobrevivientes del Terremoto de Lushan 2013. Available online: https://psiquiatria.com/depresion/asociaciones-entre-exposicion-a-traumas-trastorno-de-estres-postraumatico-y-sintomas-de-depresion-en-adolescentes-sobrevivientes-del-terremoto-de-lushan-2013/ (accessed on 11 January 2022).
- Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.J.; Chatterjee, S.; Lahiri, D.; Lavie, C.J. Psychosocial Impact of COVID-19. Diabetes Metab. Syndr. 2020, 14, 779–788. [Google Scholar] [CrossRef]
- Marthoenis, M.; Ilyas, A.; Sofyan, H.; Schouler-Ocak, M. Prevalence, Comorbidity and Predictors of Post-Traumatic Stress Disorder, Depression, and Anxiety in Adolescents Following an Earthquake. Asian J. Psychiatry 2019, 43, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Swekwi, U.; Tu, C.-C.; Dai, X. Psychological Effects of the COVID-19 Pandemic on Wuhan’s High School Students. Child. Youth Serv. Rev. 2020, 119, 105634. [Google Scholar] [CrossRef] [PubMed]
- Avanci, J.Q.; Serpeloni, F.; de Oliveira, T.P.; de Assis, S.G. Posttraumatic Stress Disorder among Adolescents in Brazil: A Cross-Sectional Study. BMC Psychiatry 2021, 21, 75. [Google Scholar] [CrossRef] [PubMed]
- Resultados Preliminares Del Impacto de La COVID-19 En Niños/as y Adolescentes Expuestos a Maltrato Intrafamiliar|Terapia Psicológica. Available online: https://teps.cl/index.php/teps/article/view/301 (accessed on 11 January 2022).
- Wethington, H.R.; Hahn, R.A.; Fuqua-Whitley, D.S.; Sipe, T.A.; Crosby, A.E.; Johnson, R.L.; Liberman, A.M.; Mościcki, E.; Price, L.N.; Tuma, F.K.; et al. The effectiveness of interventions to reduce psychological harm from traumatic events among children and adolescents: A systematic review. Am. J. Prev. Med. 2008, 35, 287–313. [Google Scholar] [CrossRef] [PubMed]
- Claudet, I.; Marchand-Tonel, C.; Kelly-Irving, M.; Gaudron, C.Z.; Raynaud, J.-P.; Delpierre, C.; Bréhin, C. The Psychological Effects of COVID-19-Related Containment in Children: The E-COCCON French Study. Arch. Pediatr. Organe Off. Soc. Francaise Pediatr. 2022, 29, 188–193. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | n (%) |
|---|---|
| Age (years) * | 14.41 ± 1.41 |
| Gender | |
| Male | 66 (11.7) |
| Female | 496 (88.3) |
| School year | |
| First | 83 (14.8) |
| Second | 63 (11.2) |
| Third | 71 (12.6) |
| Fourth | 146 (26.0) |
| Fifth | 199 (35.4) |
| Compliance with isolation measures | |
| No | 24 (4.3) |
| Yes | 538 (95.7) |
| COVID-19 pandemic severity degree | |
| Very serious | 403 (71.7) |
| Serious | 109 (19.4) |
| Neutral | 27 (4.8) |
| Overrated | 10 (1.8) |
| Very overrated | 13 (2.3) |
| Trust in the government to manage the COVID-19 pandemic | |
| Much trust | 18 (3.2) |
| Little trust | 155 (27.6) |
| Not trust, nor distrust | 178 (31.7) |
| Little distrust | 119 (21.2) |
| Much distrust | 92 (16.4) |
| Family member with recent COVID-19 | |
| No | 136 (24.2) |
| Yes | 426 (75.8) |
| Family member deceased due to COVID-19 | |
| No | 289 (51.4) |
| Yes | 273 (48.6) |
| Previous history of mental health disorders | |
| No | 493 (87.7) |
| Yes | 69 (12.3) |
| Seeking mental health support † | |
| No | 461 (82.0) |
| Yes | 101 (18.0) |
| Mental health support source | |
| Family | 37 (36.6) |
| School | 2 (2.0) |
| MINSA mental health facility | 13 (12.9) |
| Others | 49 (48.5) |
| Depression † | |
| Minimal | 112 (23.6) |
| Mild | 142 (30.0) |
| Moderate | 93 (19.6) |
| Moderate serious | 65 (13.7) |
| Serious | 63 (13.3) |
| Anxiety † | |
| No | 175 (37.8) |
| Mild | 129 (27.9) |
| Moderate | 91 (19.7) |
| Severe | 68 (14.7) |
| Resilience | 24.32 ± 8.09 |
| Alcohol consumption | |
| Low risk | 458 (92.9) |
| Medium risk | 29 (5.9) |
| High risk | 4 (0.8) |
| Probable addiction | 2 (0.4) |
| Childhood trauma † | |
| No | 263 (57.6) |
| Yes | 194 (42.5) |
| Family dysfunction | |
| No | 205 (36.5) |
| Mild | 136 (24.2) |
| Moderate | 101 (18.0) |
| Severe | 120 (21.4) |
| Post-traumatic stress | |
| No | 223 (39.7) |
| Yes | 339 (60.3) |
| Variables | Post-Traumatic Stress | p * | |
|---|---|---|---|
| No (n = 223) | Yes (n = 339) | ||
| n (%) | n (%) | ||
| Age (years) ** | 14.16 ± 1.52 | 14.59 ± 1.31 | 0.001 |
| Gender | <0.001 | ||
| Male | 42 (63.6) | 24 (36.4) | |
| Female | 181 (36.5) | 315 (63.5) | |
| School grade | 0.001 | ||
| First | 47 (56.6) | 36 (43.4) | |
| Second | 31 (49.2) | 32 (50.8) | |
| Third | 28 (39.4) | 43 (60.6) | |
| Fourth | 46 (31.5) | 100 (68.5) | |
| Fifth | 71 (35.7) | 128 (64.3) | |
| Compliance with isolation measures | 0.823 | ||
| No | 9 (37.5) | 15 (62.5) | |
| Yes | 214 (39.8) | 324 (60.2) | |
| COVID-19 pandemic severity degree | 0.562 | ||
| Very serious | 159 (39.5) | 244 (60.6) | |
| Serious | 43 (39.5) | 66 (60.6) | |
| Neutral | 12 (44.4) | 15 (55.6) | |
| Overrated | 2 (20.0) | 8 (80.0) | |
| Really overrated | 7 (53.9) | 6 (46.2) | |
| Trust in the government to manage the COVID-19 pandemic | <0.001 | ||
| Much trust | 12 (66.7) | 6 (33.3) | |
| Little trust | 79 (51.0) | 76 (49.0) | |
| Not trust, nor distrust | 55 (30.9) | 123 (69.1) | |
| Little distrust | 43 (36.1) | 76 (63.9) | |
| Much distrust | 34 (37.0) | 58 (63.0) | |
| Family member who have suffered from COVID-19 | 0.224 | ||
| No | 60 (44.1) | 76 (55.9) | |
| Yes | 163 (38.3) | 263 (61.7) | |
| Family member deceased due to COVID-19 | 0.907 | ||
| No | 114 (39.5) | 175 (60.6) | |
| Yes | 109 (39.9) | 164 (60.1) | |
| Previous history of mental health disorder | <0.001 | ||
| No | 219 (44.4) | 274 (55.6) | |
| Yes | 4 (5.8) | 65 (94.2) | |
| Mental health support search | <0.001 | ||
| No | 205 (44.5) | 256 (55.5) | |
| Yes | 18 (17.9) | 83 (82.2) | |
| Depression | <0.001 | ||
| Minimal | 91 (81.3) | 21 (18.8) | |
| Mild | 59 (41.6) | 83 (58.5) | |
| Moderate | 21 (22.6) | 72 (77.4) | |
| Moderate to serious | 5 (7.7) | 60 (92.3) | |
| Serious | 0 (0.0) | 63 (100) | |
| Anxiety | <0.001 | ||
| No | 124 (70.9) | 51 (29.1) | |
| Mild | 34 (26.4) | 95 (73.6) | |
| Moderate | 11 (12.1) | 80 (87.9) | |
| Severe | 1 (1.5) | 67 (98.5) | |
| Resilience ** | 26.99 ± 8.26 | 22.78 ±7.58 | <0.001 |
| Alcohol | 0.179 | ||
| Low risk | 175 (38.2) | 283 (61.8) | |
| Medium risk | 8 (27.6) | 21 (72.4) | |
| High risk | 0 (0.0) | 4 (100.0) | |
| Probable addiction | 0 (0.0) | 2 (100.0) | |
| Childhood trauma | <0.001 | ||
| No | 124 (47.2) | 139 (52.9) | |
| Yes | 42 (21.7) | 152 (78.4) | |
| Family APGAR | <0.001 | ||
| Normal | 129 (62.9) | 76 (37.1) | |
| Mild | 42 (30.9) | 94 (62.1) | |
| Moderate | 23 (22.8) | 78 (77.2) | |
| Severe | 29 (24.2) | 91 (75.8) | |
| Characteristics | Post-Traumatic Stress | |||||
|---|---|---|---|---|---|---|
| Simple Regression | Multiple Regression * | |||||
| PR | 95% CI | p ** | PR | 95% CI | p ** | |
| Age (years) | 1.09 | 1.04–1.15 | 0.001 | 1.00 | 0.87–1.14 | 0.948 |
| Gender | ||||||
| Male | Ref. | Ref. | ||||
| Female | 1.75 | 1.26–2.42 | 0.001 | 1.33 | 0.98–1.80 | 0.065 |
| School grade | ||||||
| First | Ref. | Ref. | ||||
| Second | 1.17 | 0.83–1.66 | 0.371 | 0.89 | 0.65–1.21 | 0.454 |
| Third | 1.40 | 1.02–1.90 | 0.035 | 0.78 | 0.54–1.13 | 0.196 |
| Fourth | 1.58 | 1.21–2.07 | 0.001 | 0.88 | 0.57- 1.36 | 0.567 |
| Fifth | 1.48 | 1.14–1.94 | 0.004 | 0.91 | 0.53–1.57 | 0.738 |
| Compliance with isolation measures | ||||||
| No | Ref. | Ref. | ||||
| Yes | 0.96 | 0.70–1.32 | 0.819 | 1.01 | 0.80–1.27 | 0.949 |
| COVID-19 pandemic severity degree | ||||||
| Very serious | Ref. | Ref. | ||||
| Serious | 1.00 | 0.84–1.19 | 0.999 | 1.00 | 0.88–1.14 | 0.998 |
| Neutral | 0.92 | 0.65–1.30 | 0.627 | 1.12 | 0.76–1.64 | 0.570 |
| Overrated | 1.32 | 0.96–1.82 | 0.088 | 1.10 | 0.77–1.56 | 0.614 |
| Really overrated | 0.76 | 0.42–1.38 | 0.370 | 0.66 | 0.35–1.24 | 0.197 |
| Trust in the government management | ||||||
| Much trust | Ref. | Ref. | ||||
| Little trust | 1.47 | 0.75–2.88 | 0.261 | 1.36 | 0.74–2.48 | 0.321 |
| Not trust, nor distrust | 2.07 | 1.07–4.02 | 0.031 | 1.59 | 0.88–2.89 | 0.126 |
| Little trust | 1.92 | 0.98–3.74 | 0.056 | 1.65 | 0.90–3.02 | 0.102 |
| Much distrust | 1.89 | 0.97–3.70 | 0.063 | 1.55 | 0.84–2.87 | 0.159 |
| Family member with recent COVID-19 | ||||||
| No | Ref. | Ref. | ||||
| Yes | 1.10 | 0.93–1.31 | 0.243 | 0.98 | 0.85–1.22 | 0.731 |
| Close relative deceased due to COVID-19 | ||||||
| No | Ref. | Ref. | ||||
| Yes | 0.99 | 0.87–1.13 | 0.907 | 1.01 | 0.90–1.13 | 0.892 |
| Previous history of mental health disorders | ||||||
| No | Ref. | Ref. | ||||
| Yes | 1.69 | 1.53–1.87 | <0.001 | 0.98 | 0.87–1.10 | 0.711 |
| Seeking mental health support | ||||||
| No | Ref. | Ref. | ||||
| Yes | 1.48 | 1.31 – 1.67 | <0.001 | 1.20 | 1.06 – 1.35 | 0.003 |
| Depression | ||||||
| Minimal | Ref. | Ref. | ||||
| Mild | 3.12 | 2.07–4.70 | <0.001 | 2.11 | 1.37–3.24 | 0.001 |
| Moderate | 4.13 | 2.76–6.17 | <0.001 | 2.44 | 1.57–3.79 | <0.001 |
| Moderate to serious | 4.92 | 3.33–7.29 | <0.001 | 2.57 | 1.66–4.00 | <0.001 |
| Serious | 5.33 | 3.63–7.85 | <0.001 | 2.62 | 1.67–4.09 | <0.001 |
| Anxiety | ||||||
| No | Ref. | Ref. | ||||
| Mild | 2.53 | 1.96–3.26 | <0.001 | 1.68 | 1.29–2.18 | <0.001 |
| Moderate | 3.02 | 2.36–3.85 | <0.001 | 1.62 | 1.23–2.12 | 0.001 |
| Severe | 3.38 | 2.68–4.27 | <0.001 | 1.71 | 1.31–2.24 | <0.001 |
| Resilience | 0.98 | 0.97–0.99 | <0.001 | 0.99 | 0.98–1.00 | 0.006 |
| Alcohol | ||||||
| Low risk | Ref. | Ref. | ||||
| Medium risk | 1.71 | 0.93–1.48 | 0.188 | 0.97 | 0.78–1.21 | 0.809 |
| High risk | 1.62 | 1.51–1.74 | <0.001 | 1.11 | 0.75–1.66 | 0.603 |
| Probable addiction | 1.62 | 1.51–1.74 | <0.001 | 1.51 | 0.91–2.53 | 0.114 |
| Childhood trauma | ||||||
| No | Ref. | Ref. | ||||
| Yes | 1.48 | 1.29–1.70 | <0.001 | 1.04 | 0.93–1.17 | 0.479 |
| Family APGAR | ||||||
| Normal | Ref. | Ref. | ||||
| Mild | 1.86 | 1.51–2.30 | <0.001 | 1.37 | 1.14–1.65 | 0.001 |
| Moderate | 2.08 | 1.69–2.56 | <0.001 | 1.26 | 1.04–1.54 | 0.021 |
| Severe | 2.05 | 1.67–2.51 | <0.001 | 1.08 | 0.89–1.31 | 0.461 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernandez-Canani, M.A.; Burga-Cachay, S.C.; Valladares-Garrido, M.J. Association between Family Dysfunction and Post-Traumatic Stress Disorder in School Students during the Second COVID-19 Epidemic Wave in Peru. Int. J. Environ. Res. Public Health 2022, 19, 9343. https://doi.org/10.3390/ijerph19159343
Fernandez-Canani MA, Burga-Cachay SC, Valladares-Garrido MJ. Association between Family Dysfunction and Post-Traumatic Stress Disorder in School Students during the Second COVID-19 Epidemic Wave in Peru. International Journal of Environmental Research and Public Health. 2022; 19(15):9343. https://doi.org/10.3390/ijerph19159343
Chicago/Turabian StyleFernandez-Canani, Maria A., Stefany C. Burga-Cachay, and Mario J. Valladares-Garrido. 2022. "Association between Family Dysfunction and Post-Traumatic Stress Disorder in School Students during the Second COVID-19 Epidemic Wave in Peru" International Journal of Environmental Research and Public Health 19, no. 15: 9343. https://doi.org/10.3390/ijerph19159343
APA StyleFernandez-Canani, M. A., Burga-Cachay, S. C., & Valladares-Garrido, M. J. (2022). Association between Family Dysfunction and Post-Traumatic Stress Disorder in School Students during the Second COVID-19 Epidemic Wave in Peru. International Journal of Environmental Research and Public Health, 19(15), 9343. https://doi.org/10.3390/ijerph19159343