
Focus on High School: Factors Associated with Creating Harmony between the Educational Transition and Adolescents’ Well-Being

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
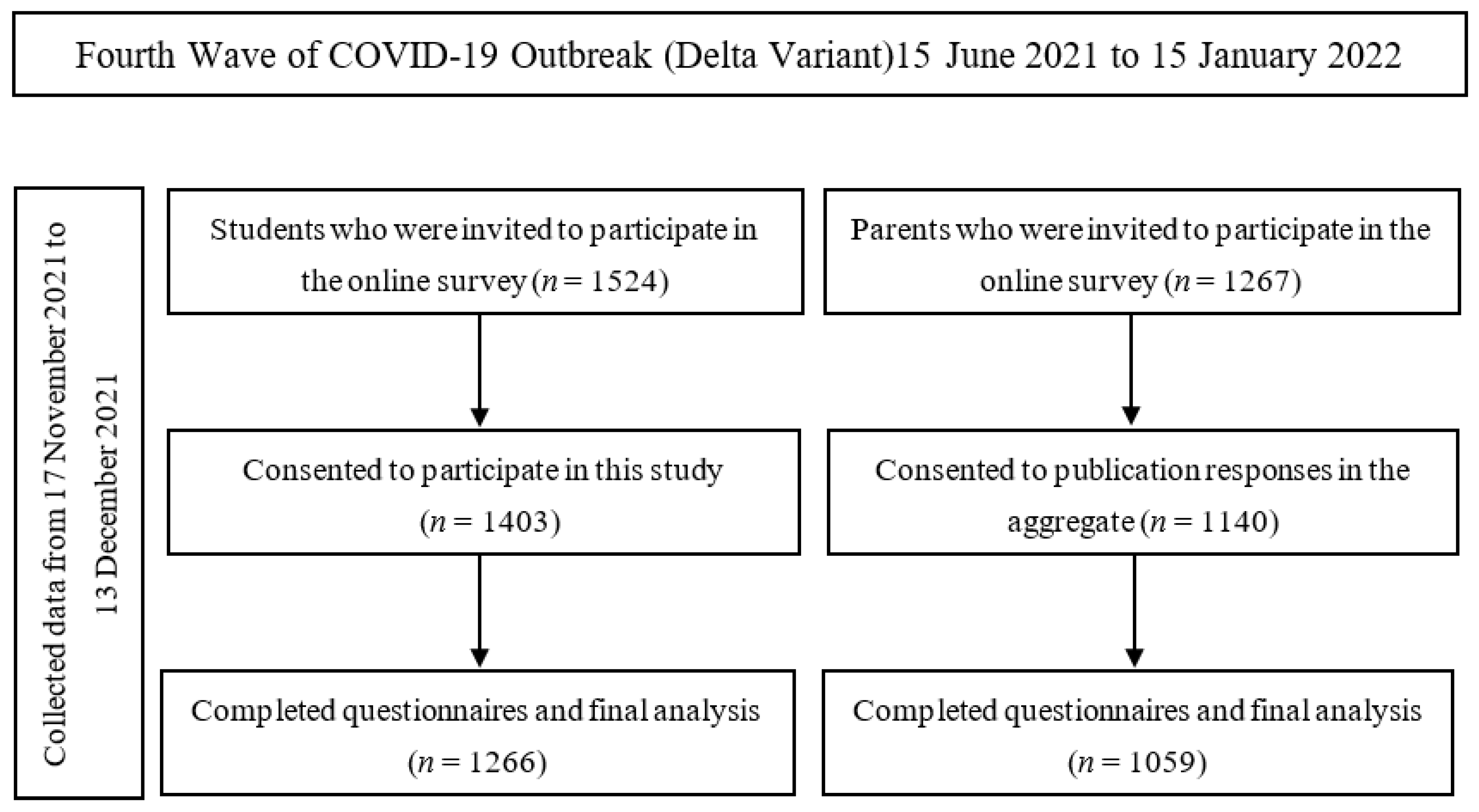
2.1. Study Design and Participants
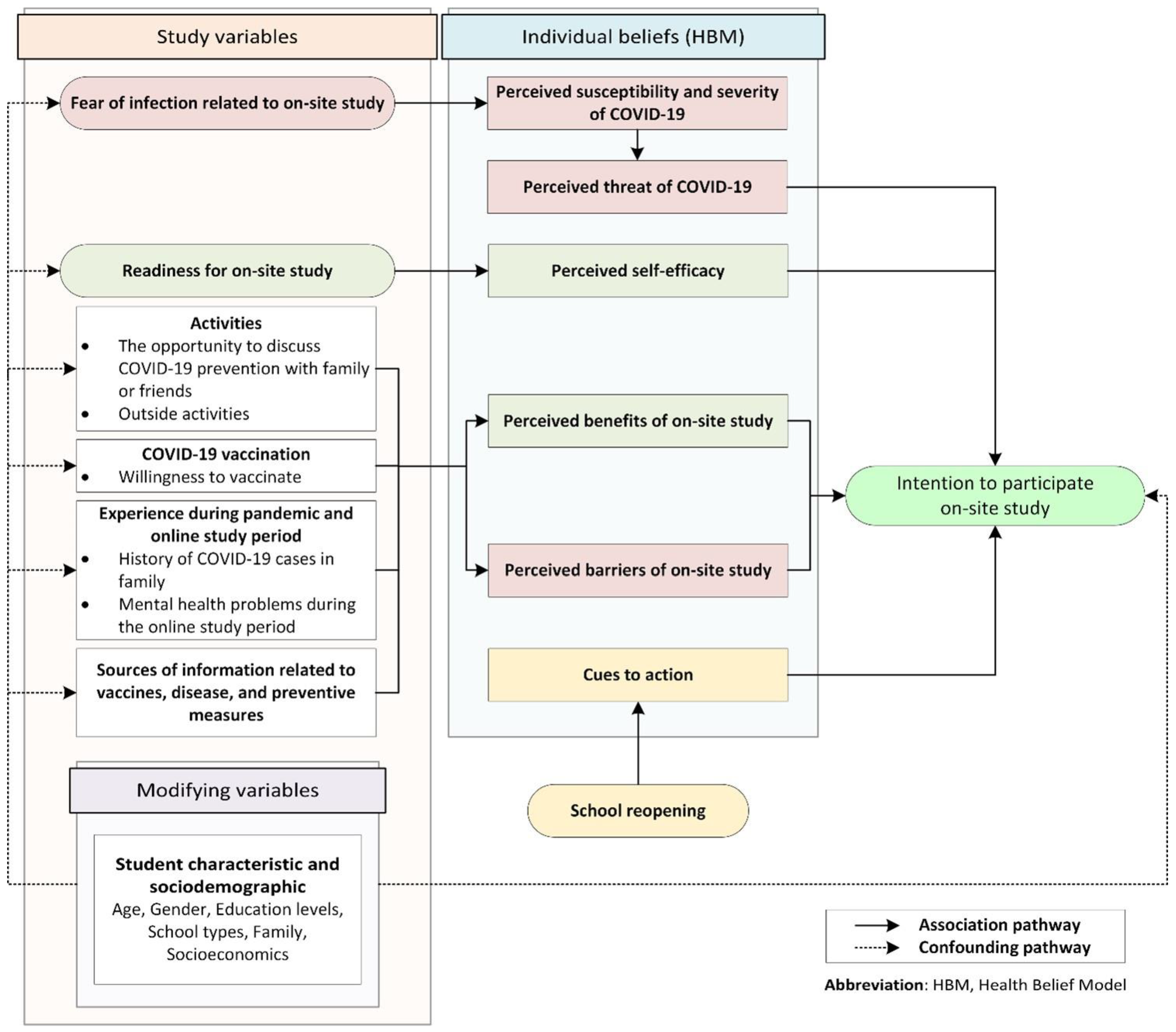
2.2. Questionnaire Design
- (1)
- Personal information including socio-demographic characteristics (age, gender, grades, school type, and transportation to school), parents’ information (occupation, educational level, and income), and family information (primary parent, family members, elderly in family, and history of previous COVID-19 infections);
- (2)
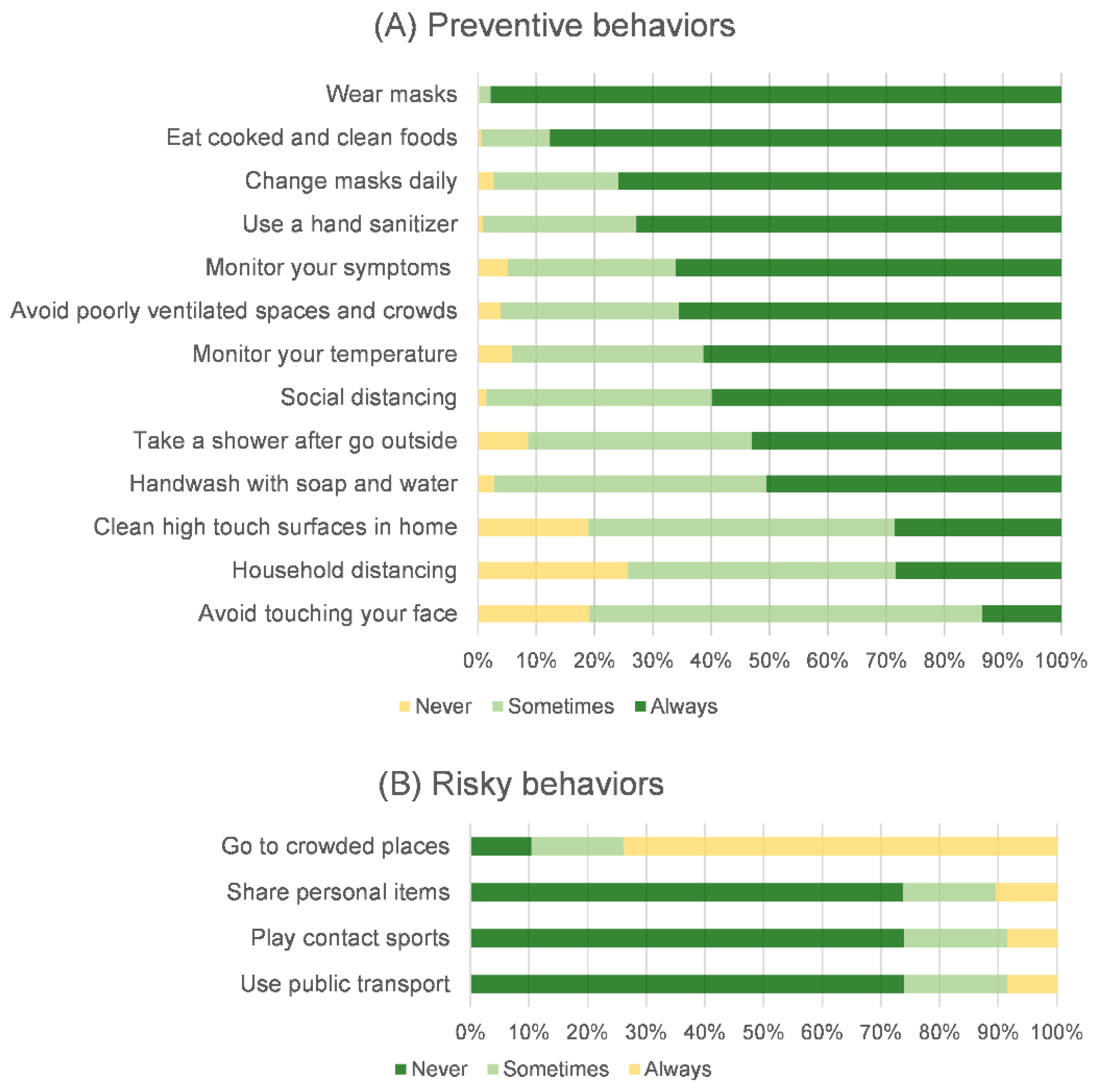
- Participants’ activities and behaviors during online classes, including the availability of alcohol-based hand sanitizer, the frequency and reason for going out for outside activities, the reasons for their opinion to be immunized, the use and disposal of masks, and their behaviors designed in accordance with the self-assessment form of preventive measures for students in preparation for on-site studying developed by the national committee, including public health experts and infectious-disease specialists from the Department of Health and educational experts from the Ministry of Education. Additionally, there was a question regarding their negative mood while taking online courses. A total of twenty questions could be answered using three categories: “never”, “sometimes”, and “always”;
- (3)
- The perceptions of students regarding their readiness for on-site studying, their desire to be on site, and their fear of being infected if returning to classrooms on site. This part could be answered using five categories: “not at all”, “slightly”, “uncertain”, “very”, and “extremely”;
- (4)
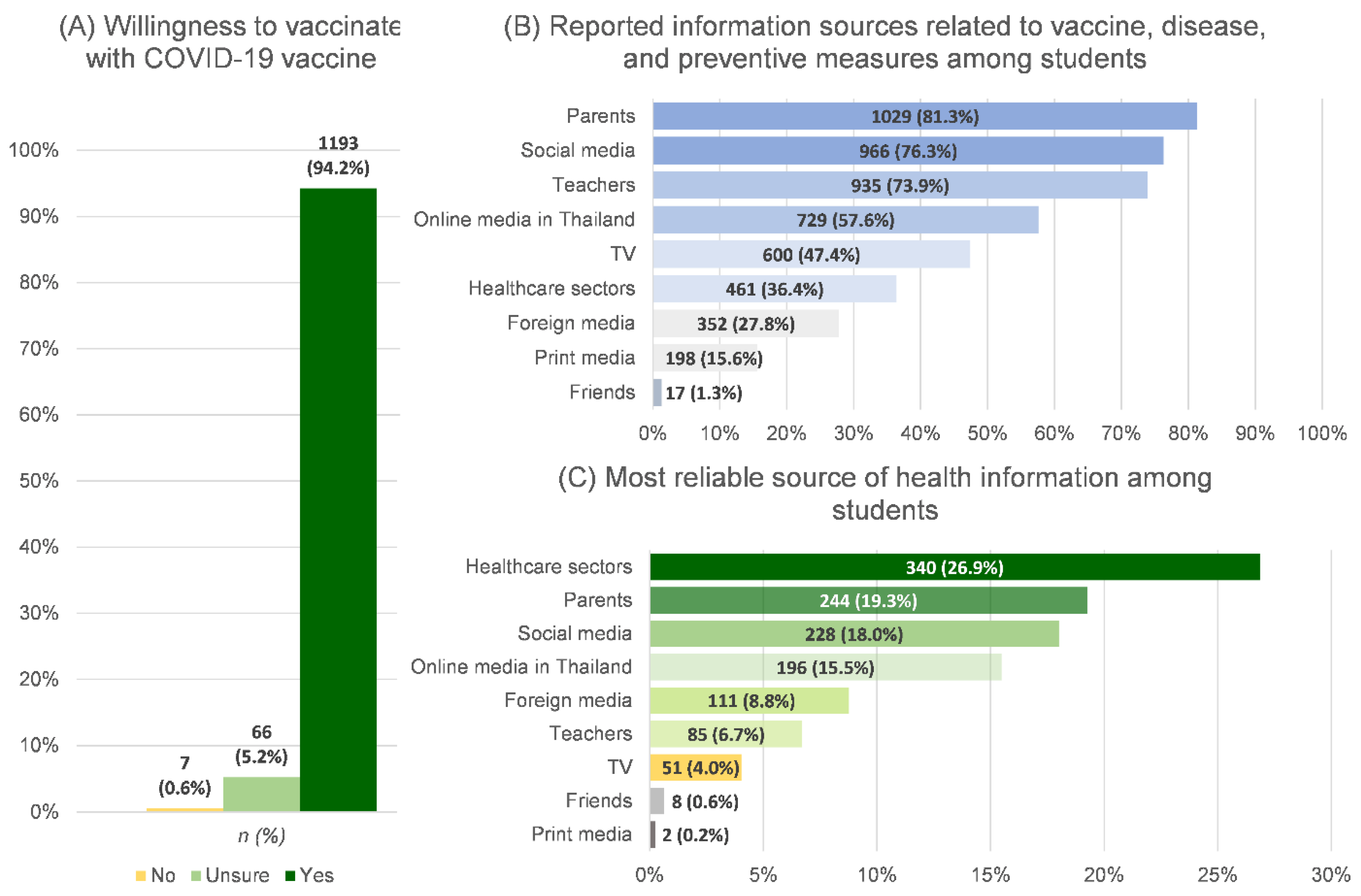
- The participants were asked about their sources of COVID-19 information, the most reliable sources, and their willingness to receive COVID-19 vaccines. The COVID-19-information sources included parents, teachers, friends, healthcare sector, television (TV), print media, foreign media, online media in Thailand, and social media. The question on willingness to receive COVID-19 vaccines could be answered using three categories: “Yes,” “Unsure,” and “No.”
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
3.1. Characteristics of Participants
3.2. Students’ Activities and Health-Related Personal Behaviors during Online-Study Period
3.3. Health-Information Receiving and Willingness to Get Vaccinated among Students
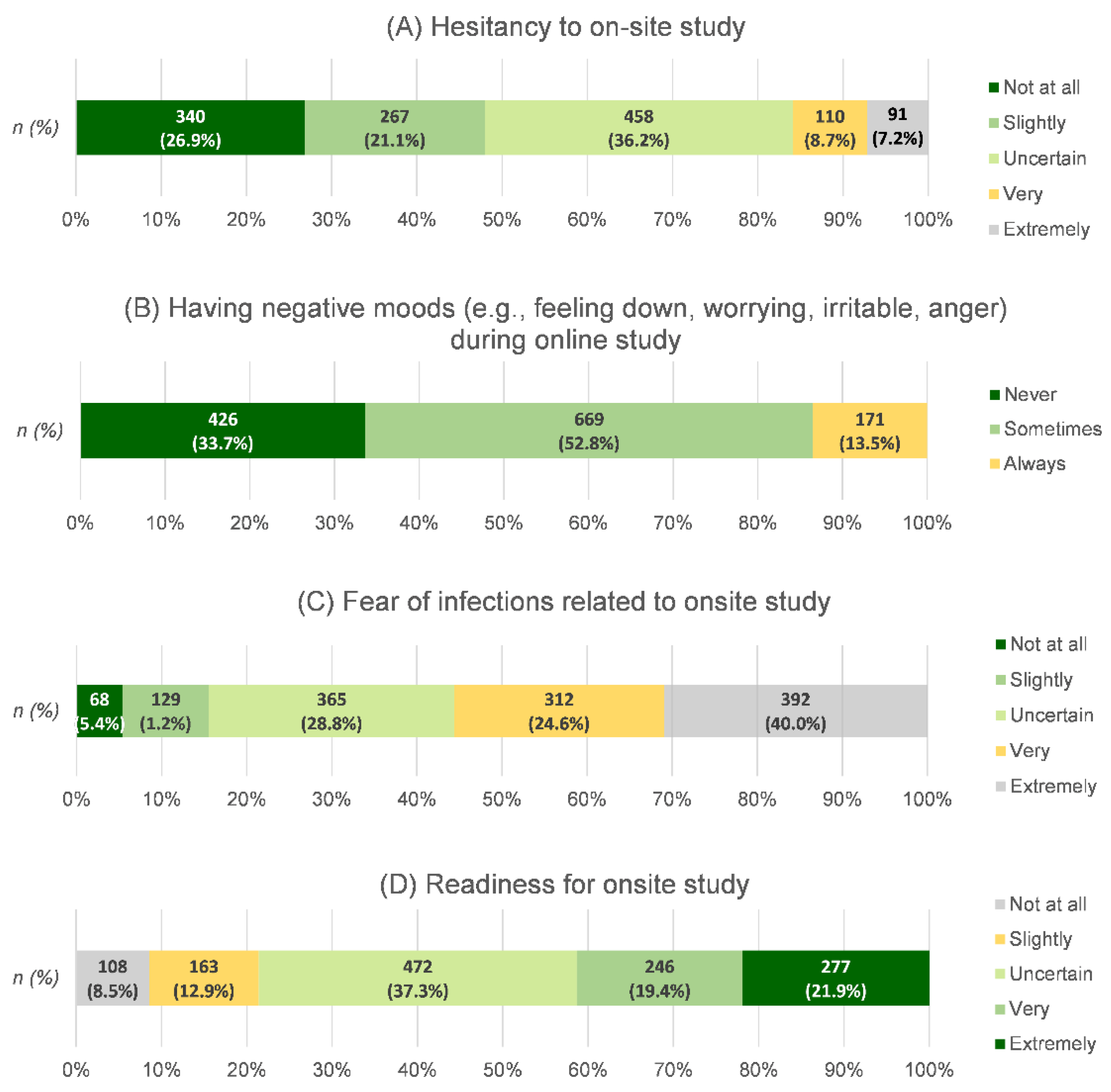
3.4. Students’ Moods during the Online-Class Period and Their Attitude toward On-Site Studying
3.5. Factors Related to Students’ Hesitancy to Study on Site
4. Discussion
4.1. Key Findings: High-School Students’ Hesitancy to Attend School for On-Site Studying and Its Associated Factors
4.2. Negative Moods during Online Study Related to Hesitancy about On-Site Studying
4.3. Fear of Infection Causing Students’ Hesitancy to Study on Site
4.4. Students’ Activities and Behaviors during Online Classes
4.5. Student Readiness to Attend School on Site
4.6. Source of Information and Willingness to Get Vaccinated
4.7. Implications
4.8. Strengths, Limitations, and Generalizability
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sheikh, A.; Sheikh, A.; Sheikh, Z.; Dhami, S. Reopening schools after the COVID-19 lockdown. J. Glob. Health 2020, 10, 010376. [Google Scholar] [CrossRef] [PubMed]
- Munro, A.P.S.; Faust, S. Children are not COVID-19 super spreaders: Time to go back to school. Arch. Dis. Child 2020, 105, 618–619. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Bloxham, C.J.; Hulme, K.D.; Sinclair, J.E.; Tong, Z.W.M.; Steele, L.E.; Noye, E.C.; Lu, J.; Xia, Y.; Chew, K.Y.; et al. A Meta-analysis on the Role of Children in Severe Acute Respiratory Syndrome Coronavirus 2 in Household Transmission Clusters. Clin. Infect. Dis. 2021, 72, e1146–e1153. [Google Scholar] [CrossRef] [PubMed]
- Hacimustafaoglu, M. COVID-19 and re-opening of schools: Opinions with scientific evidence. Turk Pediatr. Ars. 2020, 55, 337–344. [Google Scholar] [CrossRef]
- Panovska-Griffiths, J.; Kerr, C.C.; Stuart, R.M.; Mistry, D.; Klein, D.J.; Viner, R.M.; Bonell, C. Determining the optimal strategy for reopening schools, the impact of test and trace interventions, and the risk of occurrence of a second COVID-19 epidemic wave in the UK: A modelling study. Lancet Child Adolesc. Health 2020, 4, 817–827. [Google Scholar] [CrossRef]
- Goldhaber-Fiebert, J.D.; Studdert, D.M.; Mello, M.M. School Reopenings and the Community during the COVID-19 Pandemic. JAMA Health Forum 2020, 1, e201294. [Google Scholar] [CrossRef]
- Godøy, A.; Grøtting, M.W.; Hart, R.K. Reopening schools in a context of low COVID-19 contagion: Consequences for teachers, students and their parents. J. Popul. Econ. 2022, 35, 935–961. [Google Scholar] [CrossRef]
- Ciotti, S.; Moore, S.A.; Connolly, M.; Newmeyer, T. Super-Spreaders or Victims of Circumstance? Childhood in Canadian Media Reporting of the COVID-19 Pandemic: A Critical Content Analysis. Healthcare 2022, 10, 156. [Google Scholar] [CrossRef]
- Vardavas, C.; Nikitara, K.; Mathioudakis, A.G.; Boon, M.H.; Phalkey, R.; Leonardi-Bee, J.; Pharris, A.; Deogan, C.; Suk, J.E. Transmission of SARS-CoV-2 in educational settings in 2020: A review. BMJ Open 2022, 12, e058308. [Google Scholar] [CrossRef]
- Peng, X.; Liang, S.; Liu, L.; Cai, C.; Chen, J.; Huang, A.; Wang, X.; Zhao, J. Prevalence and associated factors of depression, anxiety and suicidality among Chinese high school E-learning students during the COVID-19 lockdown. Curr. Psychol. 2022, 1–12. [Google Scholar] [CrossRef]
- Elhadi, M.; Msherghi, A.; Alsoufi, A.; Buzreg, A.; Bouhuwaish, A.; Khaled, A.; Alhadi, A.; Alameen, H.; Biala, M.; Elgherwi, A.; et al. Knowledge, preventive behavior and risk perception regarding COVID-19: A self-reported study on college students. Pan Afr. Med. J. 2020, 35, 75. [Google Scholar] [CrossRef]
- López-Bueno, R.; López-Sánchez, G.F.; Casajús, J.A.; Calatayud, J.; Gil-Salmerón, A.; Grabovac, I.; Tully, M.A.; Smith, L. Health-Related Behaviors Among School-Aged Children and Adolescents During the Spanish COVID-19 Confinement. Front. Pediatr. 2020, 8, 573. [Google Scholar] [CrossRef]
- Pudjiadi, A.H.; Putri, N.D.; Sjakti, H.A.; Yanuarso, P.B.; Gunardi, H.; Roeslani, R.D.; Pasaribu, A.D.; Nurmalia, L.D.; Sambo, C.M.; Habibah, L.; et al. Parents’ Perspectives Toward School Reopening During COVID-19 Pandemic in Indonesia—A National Survey. Front. Public Health 2022, 10, 757328. [Google Scholar] [CrossRef]
- UNICEF Framework for Reopening Achools. 2020. Available online: https://www.unicef.org/documents/framework-reopening-schools (accessed on 15 July 2022).
- Rosenstock, I.M. The Health Belief Model and Preventive Health Behavior. Health Educ. Monogr. 1974, 2, 354–386. [Google Scholar] [CrossRef]
- Rosental, H.; Shmueli, L. Integrating Health Behavior Theories to Predict COVID-19 Vaccine Acceptance: Differences between Medical Students and Nursing Students. Vaccines 2021, 9, 783. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Wong, P.-F.; Lee, H.Y.; Abubakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccines Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef]
- Shmueli, L. Predicting intention to receive COVID-19 vaccine among the general population using the health belief model and the theory of planned behavior model. BMC Public Health 2021, 21, 804. [Google Scholar] [CrossRef]
- WHO Thailand. Coronavirus disease 2019 (COVID-19) WHO Thailand Situation Report 223—15 February 2022; WHO: Nonthaburi, Thailand, 2022; Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/2022_02_15_tha-sitrep-223-covid-19_eng.pdf (accessed on 15 July 2022).
- Schwartz, H.L.; Diliberti, M.K.; Grant, D. Will Students Come Back? School Hesitancy among Parents and Their Preferences for COVID-19 Safety Practices in Schools; RAND Corporation: Santa Monica, CA, USA, 2021. [Google Scholar]
- Cao, C.; Wang, L.; Fang, R.; Liu, P.; Bi, Y.; Luo, S.; Grace, E.; Olff, M. Anxiety, depression, and PTSD symptoms among high school students in China in response to the COVID-19 pandemic and lockdown. J. Affect. Disord. 2021, 296, 126–129. [Google Scholar] [CrossRef]
- Lee, H.; Noh, Y.; Seo, J.Y.; Park, S.H.; Kim, M.H.; Won, S. Impact of the COVID-19 Pandemic on the Mental Health of Adolescent Students in Daegu, Korea. J. Korean Med. Sci. 2021, 36, e321. [Google Scholar] [CrossRef]
- Wang, L.; Yeerjiang, Y.; Gao, H.F.; Pei, J.F.; Zhang, R.X.; Xu, W.H. Self-reported anxiety level and related factors in senior high school students in China during the outbreak of coronavirus disease 2019. J. Affect. Disord. 2022, 301, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Meulenbroeks, R.; van Joolingen, W.R. Students’ self-reported well-being under corona measures, lessons for the future. Heliyon 2022, 8, e08733. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.P.; Breaux, R.; Cusick, C.N.; Dvorsky, M.R.; Marsh, N.P.; Sciberras, E.; Langberg, J.M. Remote Learning during COVID-19: Examining School Practices, Service Continuation, and Difficulties for Adolescents with and Without Attention-Deficit/Hyperactivity Disorder. J. Adolesc. Health 2020, 67, 769–777. [Google Scholar] [CrossRef]
- Gao, H.; Ou, Y.; Zhang, Z.; Ni, M.; Zhou, X.; Liao, L. The Relationship between Family Support and e-Learning Engagement in College Students: The Mediating Role of e-Learning Normative Consciousness and Behaviors and Self-Efficacy. Front. Psychol. 2021, 12, 573779. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.; Xiang, M.; Cheung, T.; Xiang, Y.-T. Mental health and its correlates among children and adolescents during COVID-19 school closure: The importance of parent-child discussion. J. Affect. Disord. 2020, 279, 353–360. [Google Scholar] [CrossRef]
- Donker, M.H.; Mastrotheodoros, S.; Branje, S. Development of parent-adolescent relationships during the COVID-19 pandemic: The role of stress and coping. Dev. Psychol. 2021, 57, 1611–1622. [Google Scholar] [CrossRef]
- Lau, E.Y.H.; Li, J.-B. Hong Kong Children’s School Readiness in Times of COVID-19: The Contributions of Parent Perceived Social Support, Parent Competency, and Time Spent with Children. Front. Psychol. 2021, 12, 779449. [Google Scholar] [CrossRef]
- Spatafora, F.; Fialho, P.M.M.; Busse, H.; Helmer, S.M.; Zeeb, H.; Stock, C.; Wendt, C.; Pischke, C.R. Fear of Infection and Depressive Symptoms among German University Students during the COVID-19 Pandemic: Results of COVID-19 International Student Well-Being Study. Int. J. Environ. Res. Public Health 2022, 19, 1659. [Google Scholar] [CrossRef]
- Tang, W.; Hu, T.; Hu, B.; Jin, C.; Wang, G.; Xie, C.; Chen, S.; Xu, J. Prevalence and correlates of PTSD and depressive symptoms one month after the outbreak of the COVID-19 epidemic in a sample of home-quarantined Chinese university students. J. Affect. Disord. 2020, 274, 1–7. [Google Scholar] [CrossRef]
- Cerda, A.A.; García, L.Y.; Msc, M.A.A.C.; Mba, L.Y.G. Factors explaining the fear of being infected with COVID-19. Health Expect. 2021, 25, 506–512. [Google Scholar] [CrossRef]
- Wang, F.; Zhang, L.; Ding, L.; Wang, L.; Deng, Y. Fear of COVID-19 among College Students: A Systematic Review and Meta-Analysis. Front. Public Health 2022, 10, 846894. [Google Scholar] [CrossRef]
- Radanović, A.; Micić, I.; Pavlović, S.; Krstić, K. Don’t Think That Kids Aren’t Noticing: Indirect Pathways to Children’s Fear of COVID-19. Front. Psychol. 2021, 12, 635952. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Ye, B.; Zhang, Y.; Yang, Q. Family Cohesion and Stress Consequences among Chinese College Students during COVID-19 Pandemic: A Moderated Mediation Model. Front. Public Health 2021, 9, 703899. [Google Scholar] [CrossRef]
- Assavanopakun, P.; Promkutkao, T.; Promkutkeo, S.; Sirikul, W. Perspectives and Factors Affecting the Preventive Behavior Pertinent to COVID-19 among School Employees in Chiang Mai, Thailand: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 5662. [Google Scholar] [CrossRef] [PubMed]
- Jáuregui, A.; Argumedo, G.; Hernández-Alcaraz, C.; Contreras-Manzano, A.; Salinas-Rodríguez, A.; Salvo, D. Changes among Mexican Adults in Physical Activity and Screen Time During the COVID-19 Lockdown Period and Association with Symptoms of Depression, Anxiety, and Stress, May 29–July 31, 2020. Prev. Chronic Dis. 2022, 19, 210324. [Google Scholar] [CrossRef]
- Marckhoff, M.; Siebald, M.; Timmesfeld, N.; Janßen, M.; Romer, G.; Föcker, M. COVID-19: Effects of Pandemic Related Restrictions on Physical Activity, Screen Time, and Mental Well-being in German adolescents. Z. Für Kinder-Und Jugendpsychiatrie Und Psychother. 2022, 50, 313–326. [Google Scholar] [CrossRef]
- Amornsriwatanakul, A.; Noosorn, N.; Poonchob, K.; Wongwat, R.; Sornprasit, S.; Markmee, P.; Rosenberg, M.; Milton, K. How to Make Physical Activity Promotion Work in Thai Schools: Perspectives of Multiple Stakeholders. J. Phys. Act. Health 2022, 19, 63–70. [Google Scholar] [CrossRef]
- Sriramatr, S.; Maphong, R. Social Cognitive and Ecological Factors Influence Physical Activity among Thai Adolescents. J. Phys. Act. Health 2022, 19, 160–167. [Google Scholar] [CrossRef]
- O’Rourke, T.; Dale, R.; Humer, E.; Probst, T.; Plener, P.; Pieh, C. Health Behaviors in Austrian Apprentices and School Students during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 1049. [Google Scholar] [CrossRef]
- Hatami, H.; Abbasi-Kangevari, M.; Malekpour, M.-R.; Kolahi, A.-A. Knowledge, Attitudes, and Safety Practices about COVID-19 among High School Students in Iran during the First Wave of the Pandemic. Front. Public Health 2021, 9, 680514. [Google Scholar] [CrossRef]
- Guilamo-Ramos, V.; Benzekri, A.; Thimm-Kaiser, M.; Hidalgo, A.; Perlman, D.C. Reconsidering Assumptions of Adolescent and Young Adult Severe Acute Respiratory Syndrome Coronavirus 2 Transmission Dynamics. Clin. Infect. Dis. 2020, 73, S146–S163. [Google Scholar] [CrossRef]
- Ramaiya, A.; Villalobos, P.; Chipeta, E.; Lopez, J.V.; Maddaleno, M.; Zuo, X.; Mafuta, E.; Lulebo, A.; Green, J.; Richardson, L.; et al. How do adolescents navigate COVID-19 information, and why does it matter? J. Glob. Health 2021, 11, e001417. [Google Scholar] [CrossRef] [PubMed]
- Brandt, E.J.; Rosenberg, J.; Waselewski, M.E.; Amaro, X.; Wasag, J.; Chang, T. National Study of Youth Opinions on Vaccination for COVID-19 in the U.S. J. Adolesc. Health 2021, 68, 869–872. [Google Scholar] [CrossRef] [PubMed]
- Di Giuseppe, G.; Pelullo, C.P.; Volgare, A.S.; Napolitano, F.; Pavia, M. Parents’ Willingness to Vaccinate Their Children With COVID-19 Vaccine: Results of a Survey in Italy. J. Adolesc. Health 2022, 70, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Kitro, A.; Sirikul, W.; Dilokkhamaruk, E.; Sumitmoh, G.; Pasirayut, S.; Wongcharoen, A.; Panumasvivat, J.; Ongprasert, K.; Sapbamrer, R. COVID-19 vaccine hesitancy and influential factors among Thai parents and guardians to vaccinate their children. Vaccine X 2022, 11, 100182. [Google Scholar] [CrossRef] [PubMed]
- Ganesh, P.R.; May, R.; Dandurand, M.; Graham, J.; Rose, J.; Gullett, H.; Covell, D.; Stange, K.C. Back to the Basics: A COVID -19 Surveillance Program Within a Local School District. J. Sch. Health 2022, 92, 469–473. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | (N = 1266) | ||
|---|---|---|---|
| n | % | ||
| Age (year) | Mean ±SD | 16 | ±1 |
| Gender | Male | 456 | 36.0 |
| Female | 810 | 64.0 | |
| Education levels | 10th grade | 582 | 46.0 |
| 11th grade | 480 | 37.9 | |
| 12th grade | 204 | 16.1 | |
| School types | Private | 1050 | 83.0 |
| Government | 103 | 8.1 | |
| University demonstration | 113 | 8.9 | |
| Living with | Parents | 1203 | 95.0 |
| Relatives | 63 | 5.0 | |
| Number of family members | Less than three | 133 | 10.5 |
| From three to five | 935 | 73.9 | |
| More than five | 198 | 15.6 | |
| Elderly members | Yes | 578 | 45.7 |
| No | 688 | 54.3 | |
| History of COVID-19 cases in family | Yes | 39 | 3.1 |
| No | 1227 | 96.9 | |
| Family income (USD per month) | ≤600 | 181 | 14.3 |
| 601–1200 | 351 | 27.7 | |
| 1201–1800 | 275 | 21.7 | |
| 1801–2400 | 180 | 14.2 | |
| 2401–3000 | 121 | 9.6 | |
| >3000 | 158 | 12.5 | |
| Factors | aOR | 95%CI | p-Value | |
|---|---|---|---|---|
| Students’ Attitudes | ||||
| Being in a negative mood during the online-study period | Always (13.5%) | (ref.) | ||
| Sometime (52.8%) | 1.69 | 1.10–2.58 | 0.016 | |
| Never (33.7%) | 1.93 | 1.22–3.03 | 0.005 | |
| Readiness for on-site studying | Not at all/slightly (21.4%) | (ref.) | ||
| Uncertain (37.3%) | 0.28 | 0.14–0.58 | 0.001 | |
| Very/Extremely (41.3%) | 0.05 | 0.02–0.09 | <0.001 | |
| Fear of infection related to on-site studying | Not at all/slightly (64.6%) | (ref.) | ||
| Uncertain (24.6%) | 1.65 | 0.85–3.19 | 0.137 | |
| Very/Extremely (6.6%) | 2.95 | 1.56–5.57 | 0.001 | |
| Activities | ||||
| Having the opportunity to discuss COVID-19 prevention with family or friends. | (43.6%) | 0.71 | 0.54–0.94 | 0.016 |
| No outside activities | (18.1%) | 1.36 | 0.96–1.92 | 0.079 |
| Student’s sources of information related to vaccines, disease, and preventive measures (Received vs. Not received (ref.)) | ||||
| Parents | (81.3%) | 1.07 | 0.72–1.57 | 0.747 |
| Teachers | (76.3%) | 0.87 | 0.62–1.21 | 0.407 |
| TV | (73.9%) | 0.89 | 0.66–1.18 | 0.410 |
| Print media | (57.6%) | 1.15 | 0.77–1.73 | 0.495 |
| Online media in Thailand | (47.4%) | 0.95 | 0.72–1.26 | 0.722 |
| Healthcare sectors | (36.4%) | 1.22 | 0.91–1.65 | 0.179 |
| Social media | (27.8%) | 0.77 | 0.55–1.07 | 0.117 |
| Foreign media | (15.6%) | 0.82 | 0.59–1.13 | 0.224 |
| Friends | (1.3%) | 1.24 | 0.39–3.92 | 0.716 |
| Willingness to get vaccinated with COVID-19 vaccines | No (0.6%) | (ref.) | ||
| Unsure (5.2%) | 0.83 | 0.11–6.25 | 0.861 | |
| Yes (94.2%) | 0.74 | 0.11–5.13 | 0.759 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assavanopakun, P.; Sirikul, W.; Promkutkao, T.; Promkutkeo, S.; Panumasvivat, J. Focus on High School: Factors Associated with Creating Harmony between the Educational Transition and Adolescents’ Well-Being. Int. J. Environ. Res. Public Health 2022, 19, 9261. https://doi.org/10.3390/ijerph19159261
Assavanopakun P, Sirikul W, Promkutkao T, Promkutkeo S, Panumasvivat J. Focus on High School: Factors Associated with Creating Harmony between the Educational Transition and Adolescents’ Well-Being. International Journal of Environmental Research and Public Health. 2022; 19(15):9261. https://doi.org/10.3390/ijerph19159261
Chicago/Turabian StyleAssavanopakun, Pheerasak, Wachiranun Sirikul, Tharntip Promkutkao, Suchat Promkutkeo, and Jinjuta Panumasvivat. 2022. "Focus on High School: Factors Associated with Creating Harmony between the Educational Transition and Adolescents’ Well-Being" International Journal of Environmental Research and Public Health 19, no. 15: 9261. https://doi.org/10.3390/ijerph19159261
APA StyleAssavanopakun, P., Sirikul, W., Promkutkao, T., Promkutkeo, S., & Panumasvivat, J. (2022). Focus on High School: Factors Associated with Creating Harmony between the Educational Transition and Adolescents’ Well-Being. International Journal of Environmental Research and Public Health, 19(15), 9261. https://doi.org/10.3390/ijerph19159261