
Cone-Beam Computed Tomography (CBTC) Applied to the Study of Root Morphological Characteristics of Deciduous Teeth: An In Vitro Study


Abstract
:
1. Introduction
2. Materials and Methods
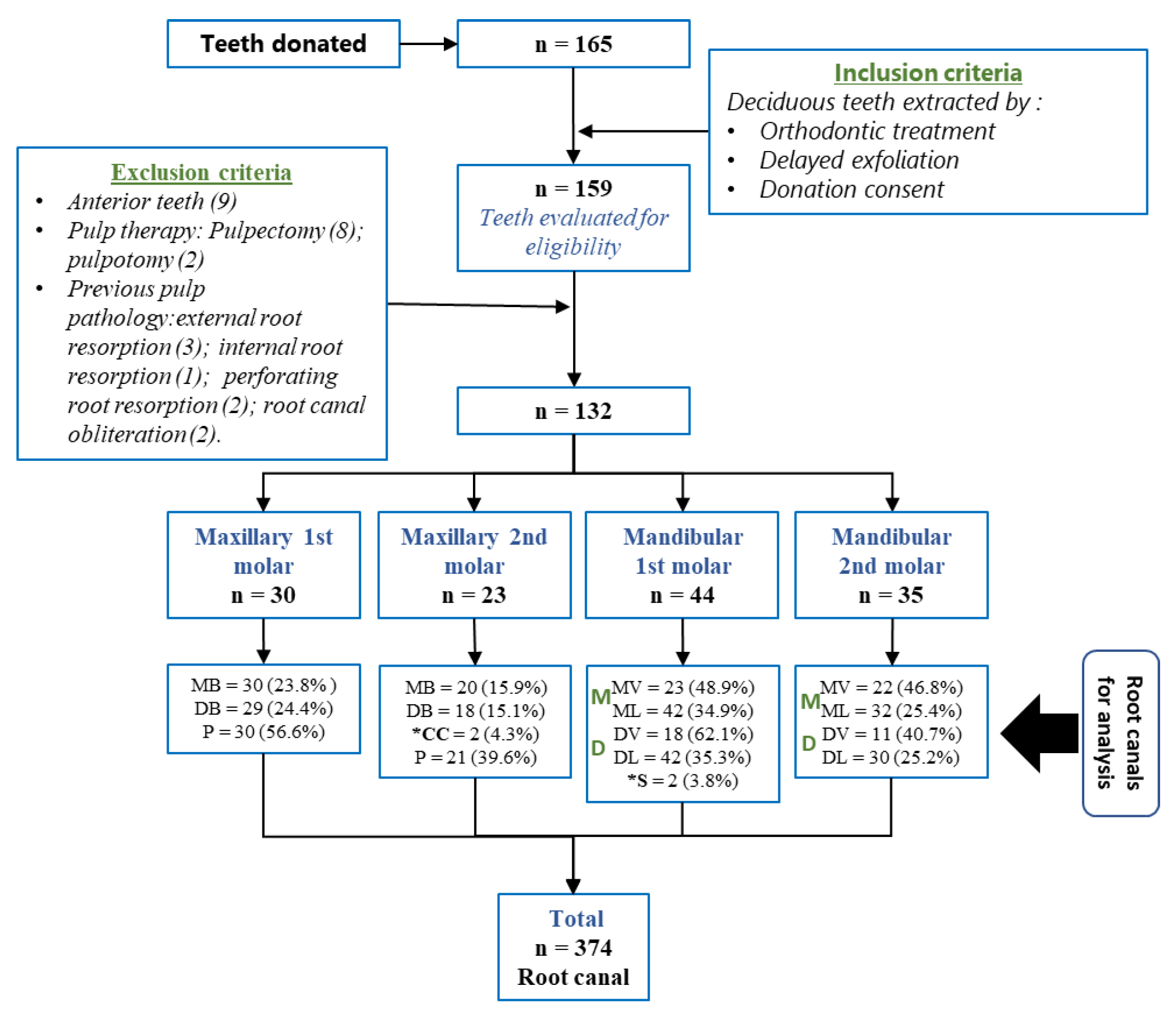
2.1. Sample Selection
2.2. Collection, Storage of Teeth and Formation of Groups
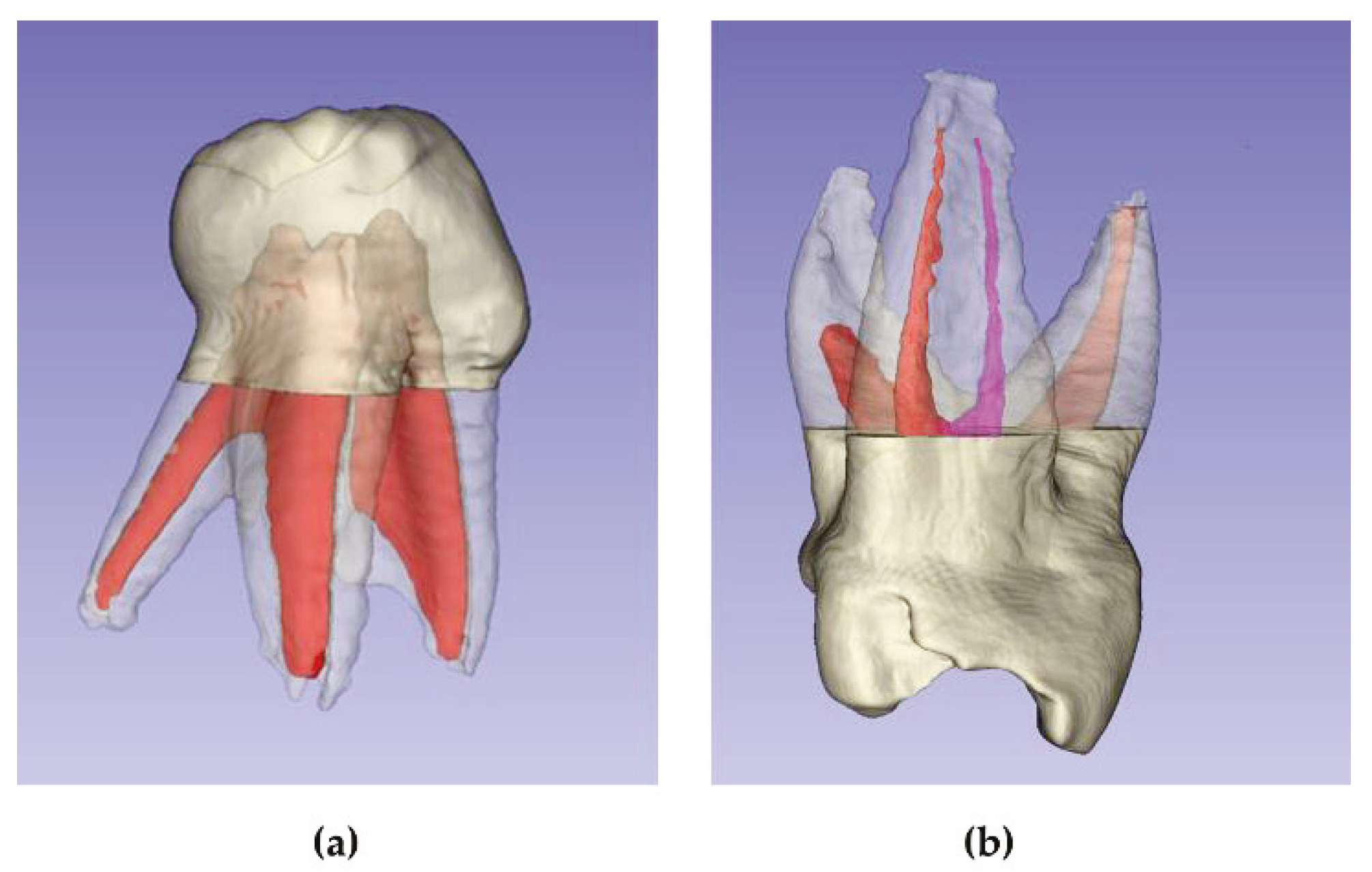
2.3. Image Acquisition and 3D Reconstruction
2.4. Evaluation of Canal Morphology
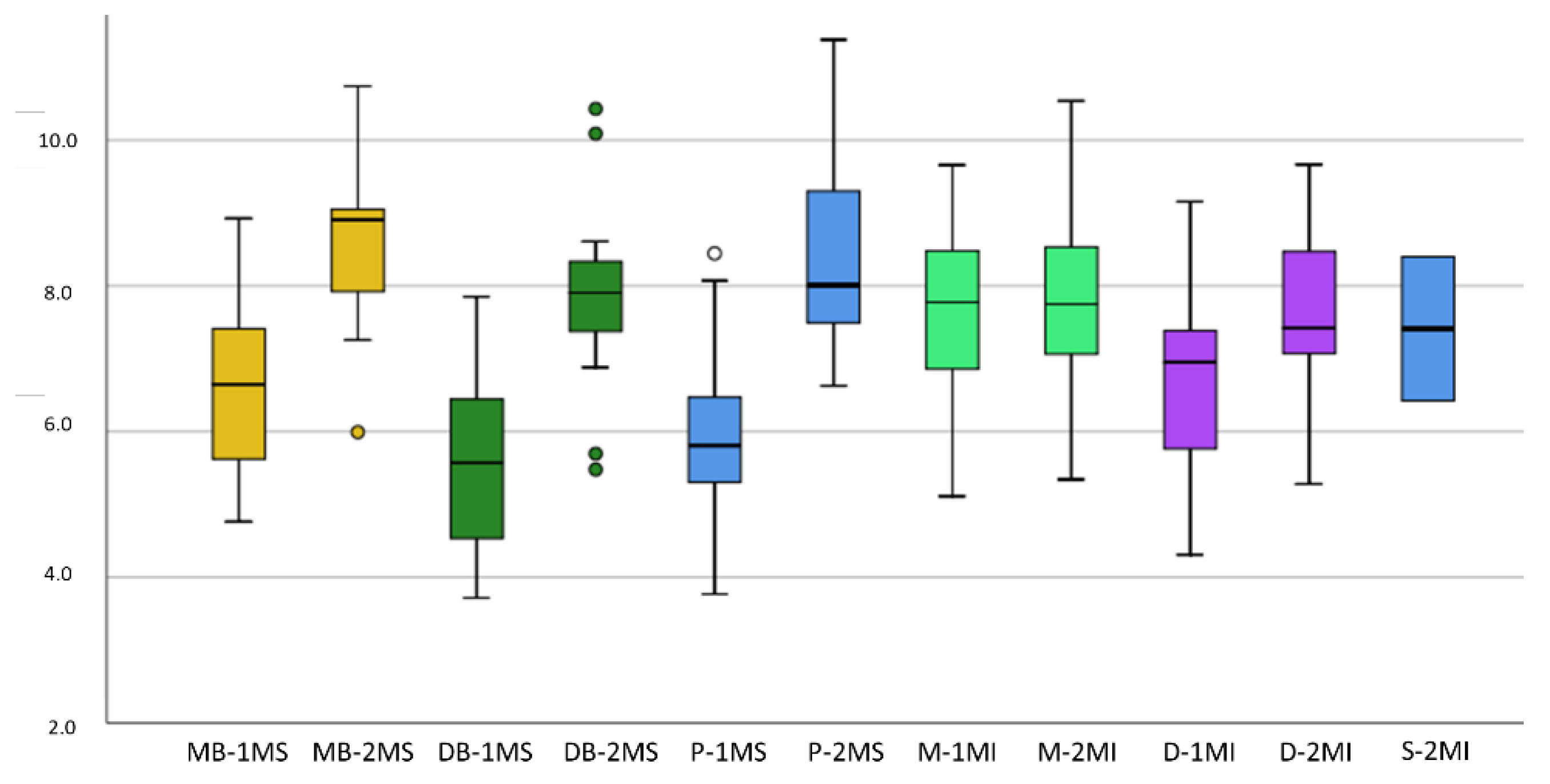
2.5. Root and Canal Length Measurement
2.6. Root Canal Angulation
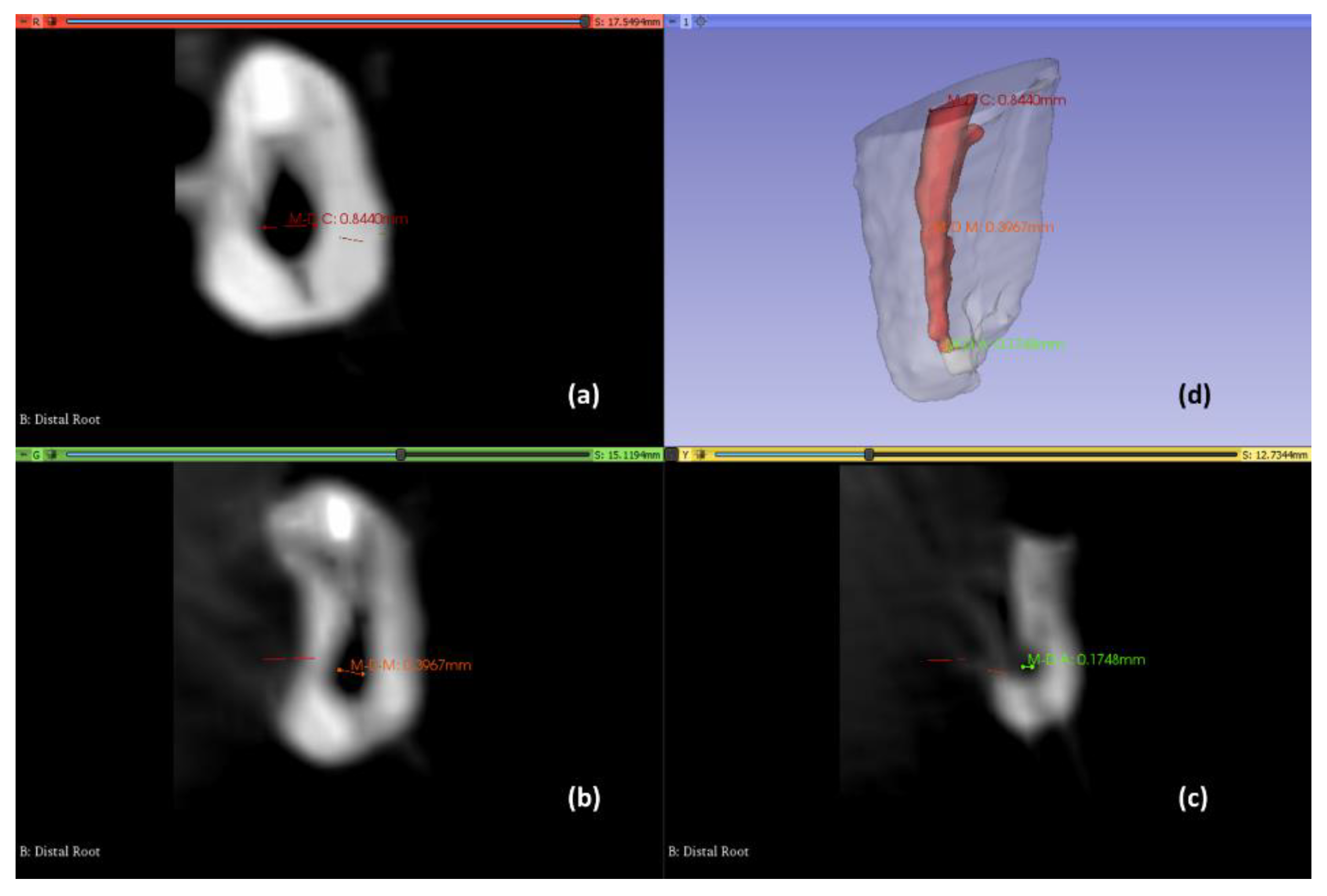
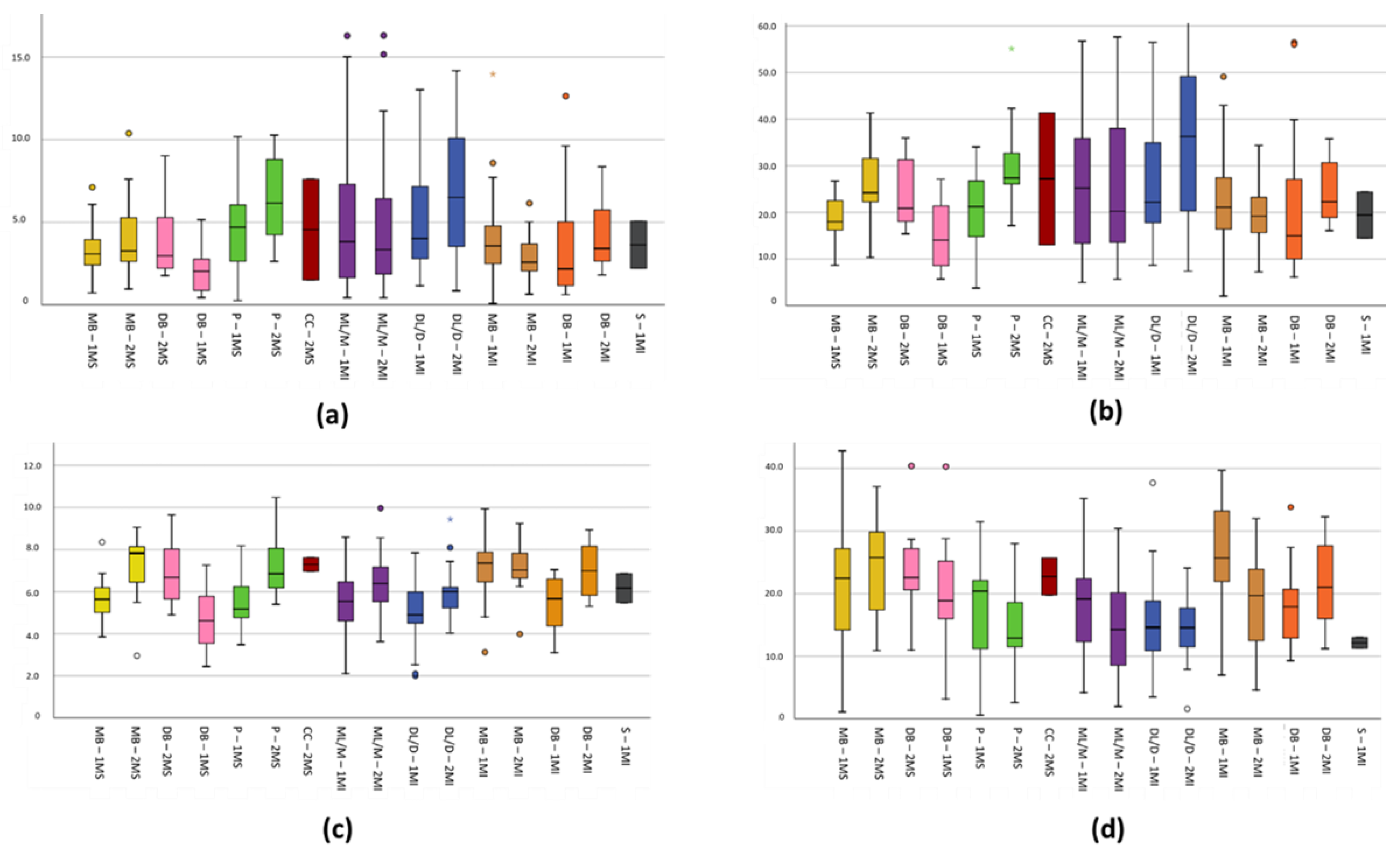
2.7. Root Canal Diameter Measurements
2.8. Volumes and Surfaces Measurement
2.9. Calibration, Pilot Test, Internal Validity
2.10. Statistical Analysis
3. Results
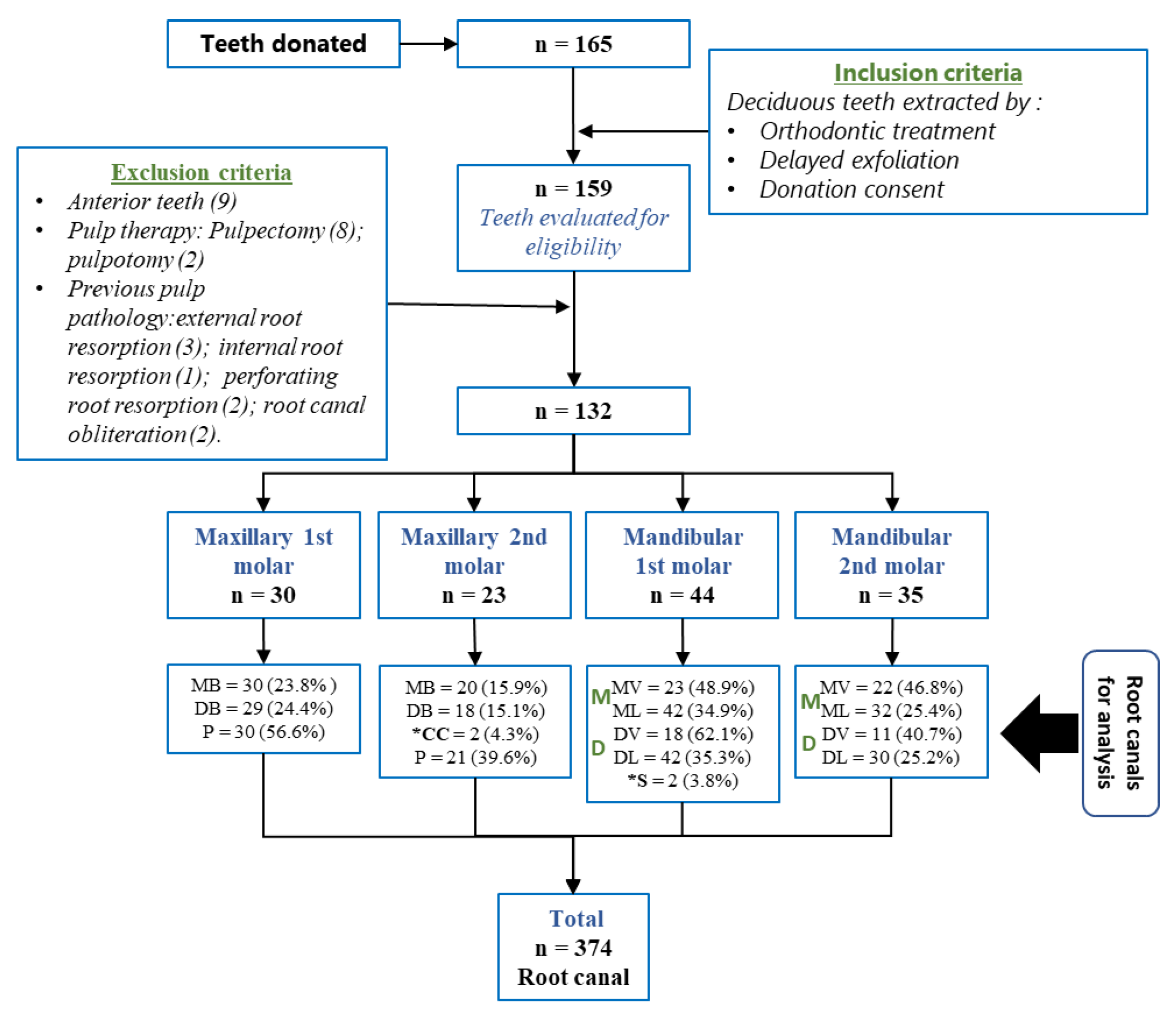
3.1. Sample Distribution
3.2. General Characteristics
3.3. Specific Characteristics
4. Discussion
4.1. General External Characteristics of the Root Morphology of the Maxillary Molars
4.2. General Internal Characteristics of the Root Morphology of the Maxillary Molars
4.3. General External Characteristics of the Root Morphology of the Mandibular Molars
4.4. General Internal Characteristics of the Root Morphology of the Mandibular Molars
4.5. Root Canal Characteristics of the Maxillary and Mandibular Molars
4.5.1. Typology of Root Canals
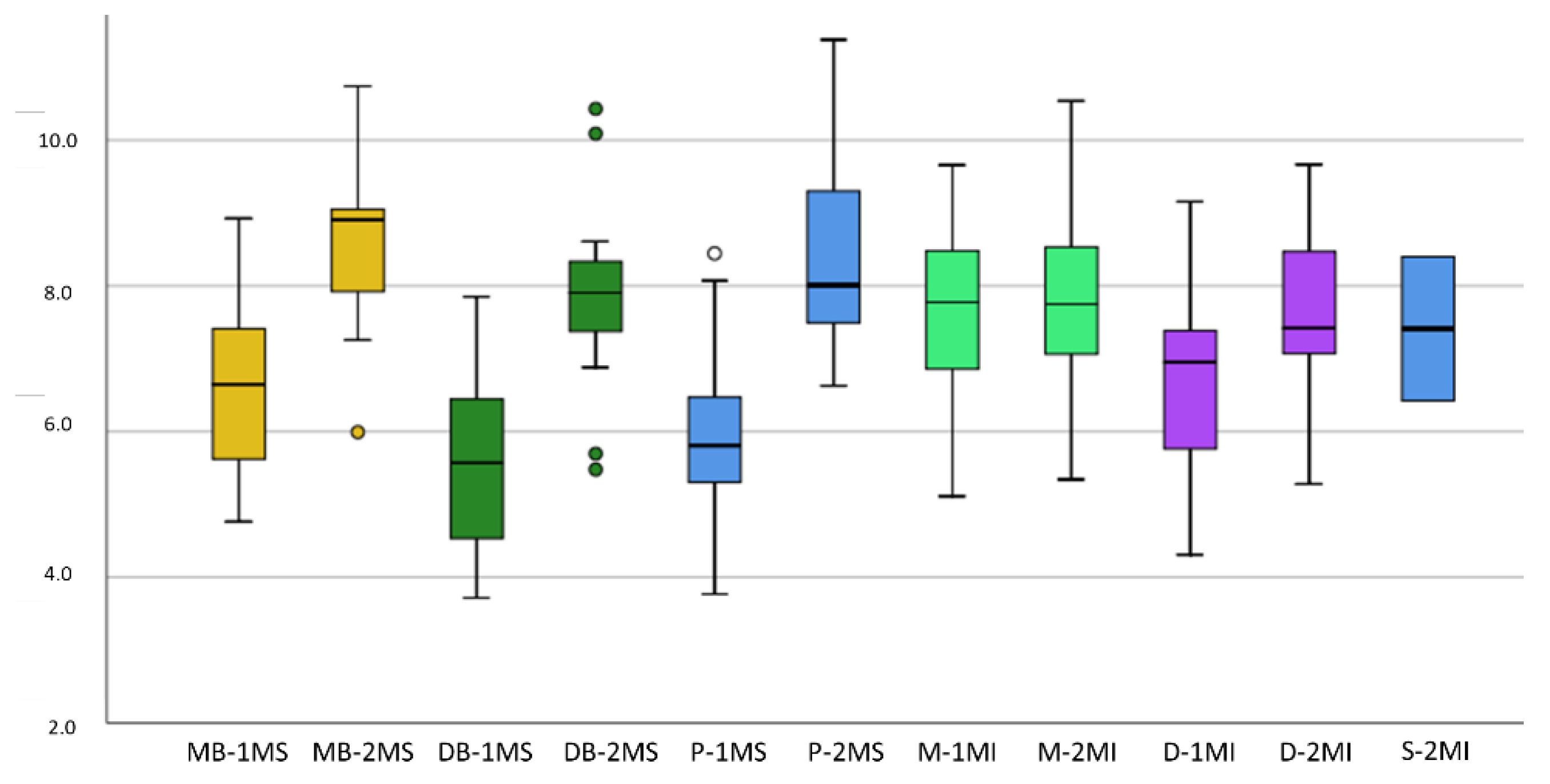
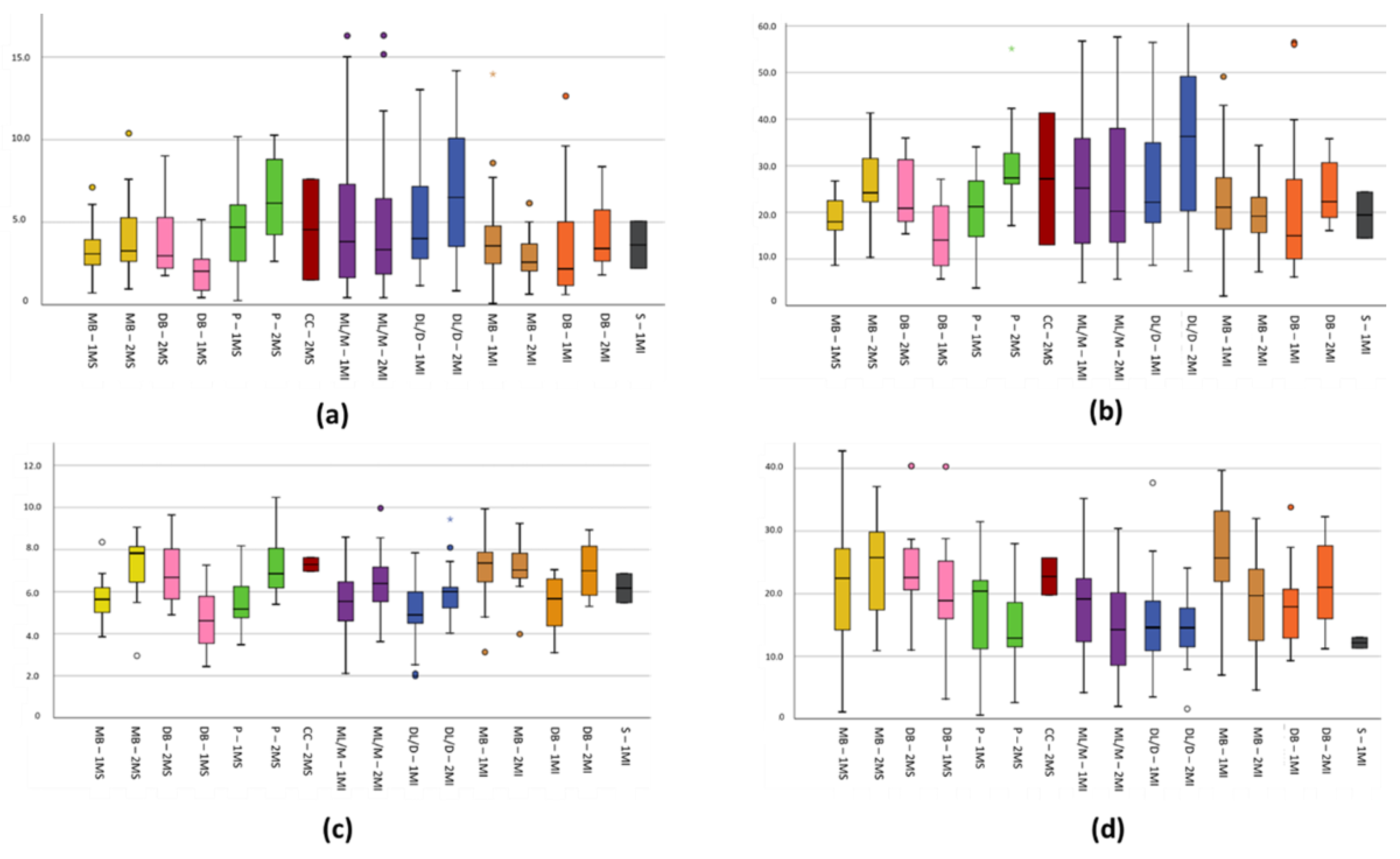
4.5.2. The Axial Length of the Root Canal
4.5.3. Two-Dimensional Surface in mm2 of the Root Canals
4.5.4. Three-Dimensional Volume in mm3 of the Root Canals
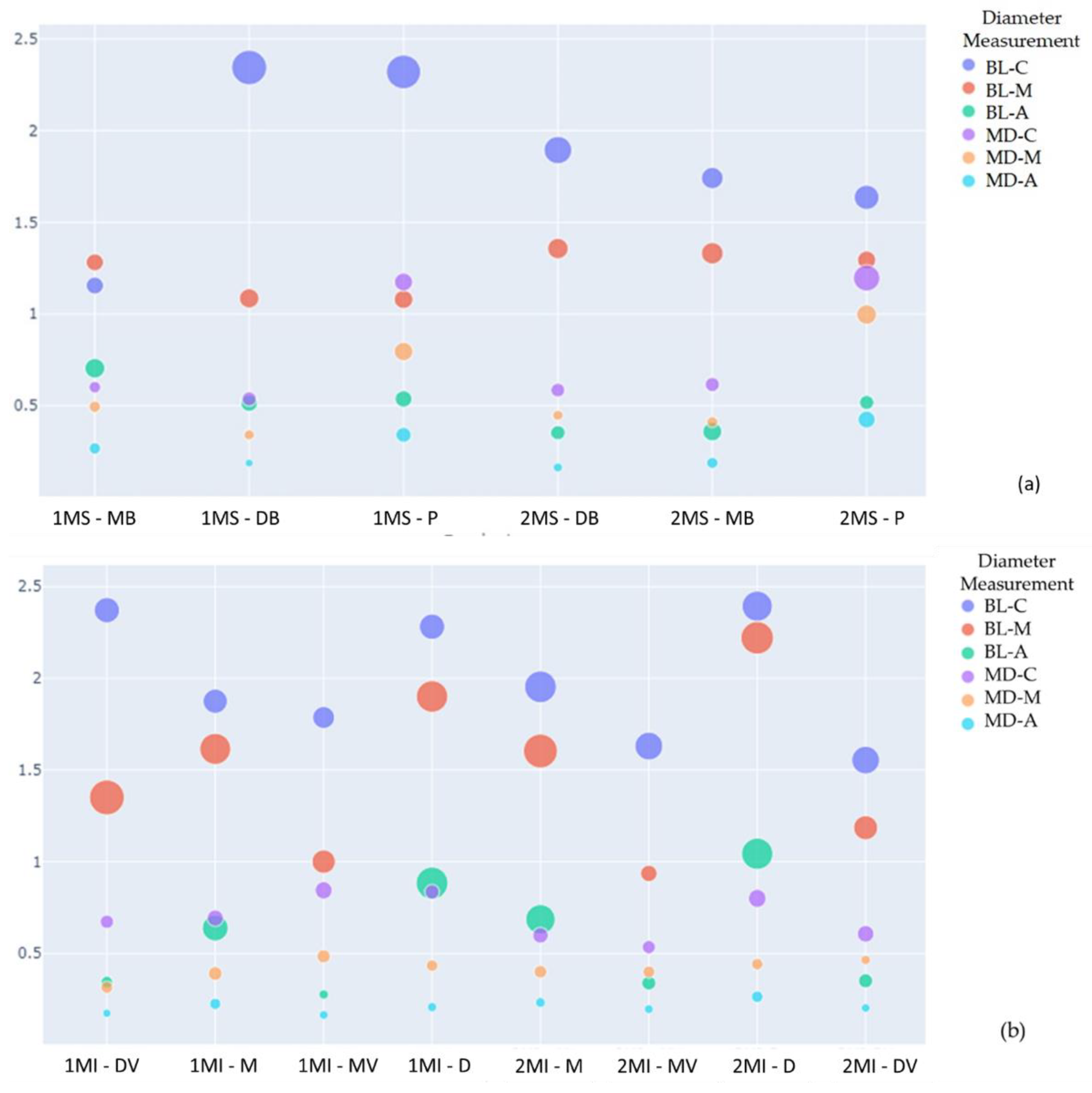
4.5.5. Mesiodistal and Buccolingual Diameters of the Root Canals
4.5.6. Curvatures of the Root Canals
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bagherian, A.; Kalhori, K.A.M.; Sadeghi, M.; Mirhosseini, F.; Parisay, I. An in Vitro Study of Root and Canal Morphology of Human Deciduous Molars in an Iranian Population. J. Oral Sci. 2010, 52, 397–403. [Google Scholar] [CrossRef] [Green Version]
- Ziya, M.; Yüksel, B.N.; Sarı, Ş. Root Canal Morphology of Mandibular Primary Molars: A Micro-Ct Study. Cumhur. Dent. J. 2019, 22, 382–389. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, H.M.A. Anatomical Challenges, Electronic Working Length Determination and Current Developments in Root Canal Preparation of Primary Molar Teeth. Int. Endod. J. 2013, 46, 1011–1022. [Google Scholar] [CrossRef]
- Ahmed, H.M.A.; Musale, P.K.; El Shahawy, O.I.; Dummer, P.M.H. Application of a New System for Classifying Tooth, Root and Canal Morphology in the Primary Dentition. Int. Endod. J. 2020, 53, 27–35. [Google Scholar] [CrossRef] [Green Version]
- Katge, F.; Wakpanjar, M. Root Canal Morphology of Primary Molars by Clearing Technique: An in Vitro Study. J. Indian Soc. Pedod. Prev. Dent. 2018, 36, 151–157. [Google Scholar] [CrossRef]
- Acar, B.; Kamburoğlu, K.; Tatar, İ.; Arıkan, V.; Çelik, H.H.; Yüksel, S.; Özen, T. Comparison of Micro-Computerized Tomography and Cone-Beam Computerized Tomography in the Detection of Accessory Canals in Primary Molars. Imaging Sci. Dent. 2015, 45, 205–211. [Google Scholar] [CrossRef] [Green Version]
- Fumes, A.C.; Sousa-Neto, M.D.; Leoni, G.B.; Versiani, M.A.; da Silva, L.A.B.B.; da Silva, R.A.B.B.; Consolaro, A. Root Canal Morphology of Primary Molars: A Micro-Computed Tomography Study. Eur. Arch. Paediatr. Dent. 2014, 15, 317–326. [Google Scholar] [CrossRef]
- Ozcan, G.; Sekerci, A.E.; Cantekin, K.; Aydinbelge, M.; Dogan, S. Evaluation of Root Canal Morphology of Human Primary Molars by Using CBCT and Comprehensive Review of the Literature. Acta Odontol. Scand. 2016, 74, 250–258. [Google Scholar] [CrossRef]
- Datta, P.; Zahir, S.; Kundu, G.; Dutta, K.; Dentistry, P. An in Vitro Study of Root Canal System of Human Primary Molars by Using Multidetector Computed Tomography. Pedod. Pre. Dent. 2019, 37, 120–126. [Google Scholar] [CrossRef]
- Nazeer, M.R.; Khan, F.R. Evaluation of the Root and Canal Morphology of Mandibular First Permanent Molars in a Sample of Pakistani Population by Cone-Beam Computed Tomography. J. Pak. Med. Assoc. 2019, 69, 1084–1089. [Google Scholar]
- Gupta, D.; Grewal, N. Root Canal Configuration of Deciduous Mandibular First Molars—An in Vitro Study. J. Indian Soc. Pedod. Prev. Dent. 2005, 23, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Sharma, U.; Gulati, A.; Gill, N. An Investigation of Accessory Canals in Primary Molars—An Analytical Study. Int. J. Paediatr. Dent. 2016, 26, 149–156. [Google Scholar] [CrossRef]
- Gaurav, V.; Srivastava, N.; Rana, V.; Adlakha, V. A Study of Root Canal Morphology of Human Primary Incisors and Molars Using Cone Beam Computerized Tomography: An in Vitro Study. J. Indian Soc. Pedod. Prev. Dent. 2013, 31, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-L.; Chang, H.-H.H.; Kuo, C.-I.I.; Chen, S.-K.K.; Guo, M.-K.K.; Huang, G.-F.F.; Lin, C.-P.P. A Study on the Root Canal Morphology of Primary Molars by High-Resolution Computed Tomography. J. Dent. Sci. 2013, 8, 321–327. [Google Scholar] [CrossRef] [Green Version]
- Zoremchhingi; Joseph, T.; Varma, B.; Mungara, J. A Study of Root Canal Morphology of Human Primary Molars Using Computerised Tomography: An in Vitro Study. J. Indian Soc. Pedod. Prev. Dent. 2005, 23, 7–12. [Google Scholar] [CrossRef]
- Yang, R.; Yang, C.; Liu, Y.; Hu, Y.; Zou, J. Evaluate Root and Canal Morphology of Primary Mandibular Second Molars in Chinese Individuals by Using Cone-Beam Computed Tomography. J. Formos. Med. Assoc. 2013, 112, 390–395. [Google Scholar] [CrossRef] [Green Version]
- Moyaho-Bernal, M.; Carrasco-Gutiérrez, R.; Jiménez-Flores, R.; Juárez-Luna, G.; López-Del Pino, G.; Mendoza-García, L.; Teutle-Coyotecatl, B. Prevalence of Three-Rooted Primary Mandibular First and Second Molars: Clinical and Radiographic Findings in a Mexican Population. Acta Odontol. Latinoam. 2021, 34, 149–155. [Google Scholar] [CrossRef]
- Ozcan, G.; Sekerci, A.E.; Kocoglu, F. C-Shaped Mandibular Primary First Molar Diagnosed with Cone Beam Computed Tomography: A Novel Case Report and Literature Review of Primary Molars′ Root Canal Systems. J. Indian Soc. Pedod. Prev. Dent. 2016, 34, 397–404. [Google Scholar] [CrossRef]
- Neboda, C.; Anthonappa, R.P.; King, N.M. Preliminary Investigation of the Variations in Root Canal Morphology of Hypomineralised Second Primary Molars. Int. J. Paediatr. Dent. 2018, 28, 310–318. [Google Scholar] [CrossRef]
- Weine, F.S.; Healey, H.J.; Gerstein, H.; Evanson, L. Canal Configuration in the Mesiobuccal Root of the Maxillary First Molar and Its Endodontic Significance. Oral Surg. Oral Med. Oral Pathol. 1969, 28, 419–425. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, S.W. A Comparison of Canal Preparations in Straight and Curved Root Canals. Oral Surg. Oral Med. Oral Pathol. 1971, 32, 271–275. [Google Scholar] [CrossRef]
- Muhammad, S.; Shahid, R.; Siddiqui, M.I. Root and canal Morphology of Humain Primary Molars in a local Population of Southern Punjab: An in vitro Syudy. PJMHS 2015, 9, 1043–1047. [Google Scholar]
- Fernandes, S.; Patel, D.G.; Ranadheer, E.; Kalgudi, J.; Santoki, J.; Chaudhary, S. Occlusal Traits of Primary Dentition among Pre-School Children of Mehsana District, North Gujarat, India. J. Clin. Diagnostic Res. 2017, 11, 92–96. [Google Scholar] [CrossRef]
- Taneja, S.; Jain, A. Primary Mandibular Molars with Supernumerary Roots: A Report of 2 Cases. Gen. Dent. 2020, 68, 43–46. [Google Scholar]
- Garcovich, D.; Zhou Wu, A.; Sanchez Sucar, A.M.; Adobes Martin, M. The online attention to orthodontic research: An Altmetric analysis of the orthodontic journals indexed in the journal citation reports from 2014 to 2018. Prog. Orthod. 2020, 21, 31. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Maxillary | Mandibular | |||||
|---|---|---|---|---|---|---|
| Weine’s Classification | 1M | 2M | 1M | 2M | ||
| Root | Frequency (%) | Frequency (%) | Root | Frequency (%) | Frequency (%) | |
| I | MB | 28 (93.3%) * | 16 (69.6%) * | M | 14 (31.1%) | 7 (20.6%) |
| II | 2 (8.7%) | 3 (6.7%) | 1 (2.9%) | |||
| III | 1 (4.3%) | 20 (44.4%) * | 24 (70.6%) * | |||
| IV | 2 (6.7%) | 4 (17.4%) | 8 (17.8%) | 2 (5.9%) | ||
| I | DB | 13 (46.4%) | 9 (39.1%) | D | 18 (40%) | 13 (38.2%) |
| II | 2 (8.7%) | 1 (2.2%) | 1 (2.9%) | |||
| III | 13 (46.4%) | 10 (43.5%) | 16 (36.6%) | 14 (41.2%) | ||
| IV | 2 (7.1%) | 2 (8.7%) | 10 (22.2%) | 6 (17,6%) | ||
| Fusion PR + DBR | 14 (46.6%) | 9 (39.1%) | ||||
| I | P | 13 (81.3%) | 12 (85.7%) | S | 2 (100%) | |
| II | 2 (14.3%) | |||||
| III | 1 (6.3%) | |||||
| IV | 2 (12.5%) | |||||
| Root | Maxillary | |||
| 1M | 2M | |||
| Mean | SD | Mean | SD | |
| MB | 6.58 | 1.14 | 8.61 * | 1.15 |
| DB | 5.57 | 1.23 | 7.90 * | 1.41 |
| P | 5.98 | 1.07 | 8.43 * | 1.38 |
| Mandibular | ||||
| 1M | 2M | |||
| Mean | SD | Mean | SD | |
| M | 7.58 | 1.27 | 7.89 | 1.35 |
| D | 6.57 | 1.20 | 7.62 * | 1.21 |
| S | 7.41 | 1.39 | ||
| Tooth | Root Canal | Length (mm) | Angulation (Degree) | Surface (mm2) | Volume (mm3) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |||
| Maxillary | ||||||||||
| 1M | MB | 5.68 | 0.88 | 21.2 | 11.68 | 18.66 | 4.79 | 3.42 | 1.53 | |
| DB | 4.66 | 1.30 | 20.32 | 8.46 | 15.54 | 7.46 | 2.26 | 1.50 | ||
| P | 5.58 | 1.26 | 17.58 | 8.30 | 21.06 | 8.03 | 4.71 | 2.66 | ||
| 2M | MB | 7.25 * | 1.42 | 23.83 | 7.41 | 26.28 * | 7.40 | 4.21 | 2.38 | |
| CC | 7.29 | 0.45 | 22.75 | 4.17 | 27.19 | 19.99 | 4.55 | 4.30 | ||
| DB | 6.75 * | 1.39 | 24.03 | 7.28 | 24.20 * | 7.56 | 3.68 * | 1.89 | ||
| P | 7.20 * | 1.39 | 15.25 | 6.04 | 29.70 * | 9.22 | 6.89 * | 3.92 | ||
| Mandibular | ||||||||||
| 1M | M | B | 7.06 | 1.41 | 25.98 * | 8.21 | 23.98 | 11.42 | 4.34 | 2.96 |
| L | 5.49 | 1.39 | 18.72 * | 7.46 | 26.09 | 14.39 | 5.06 | 4.14 | ||
| D | B | 5.45 | 1.27 | 18.00 | 6.43 | 21.81 | 15.71 | 3.48 | 3.35 | |
| L | 4.98 | 1.31 | 14.87 | 6.77 | 26.79 | 12.63 | 5.02 | 3.19 | ||
| S | 6.16 | 0.97 | 12.15 | 1.20 | 19.42 | 6.97 | 3.63 | 2.01 | ||
| 2M | M | B | 7.18 | 1.13 | 18.74 | 7.61 | 19.67 | 6.10 | 2.91 | 1.36 |
| L | 6.31 | 1.38 | 14.67 | 7.81 | 25.71 | 16.84 | 5.10 | 5.11 | ||
| D | B | 7.05 * | 1.34 | 21.95 * | 7.33 | 24.85 | 7.01 | 4.22 | 2.07 | |
| L | 5.94 * | 1.16 | 14.45 | 4.97 | 35.28 * | 15.79 | 7.65 * | 5.71 | ||
| Maxillary | Mandibular | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1M | 2M | 1M | 2M | |||||||||||
| Root canal | measure | Mean | SD | Mean | SD | Root | Canal | measure | Mean | SD | Mean | SD | ||
| MB | BL | C | 1.15 | 0.34 | 1.68 * | 0.5 | M | B | BL | C | 1.78 | 0.5 | 1.63 | 0.81 |
| M | 1.28 | 0.34 | 1.31 | 0.48 | M | 1 | 0.57 | 0.93 | 0.28 | |||||
| A | 0.70 * | 0.46 | 0.37 | 0.43 | A | 0.27 | 0.09 | 0.33 | 0.21 | |||||
| MD | C | 0.6 | 0.16 | 0.61 | 0.25 | MD | C | 0.84 | 0.3 | 0.53 | 0.19 | |||
| M | 0.49 | 0.16 | 0.41 | 0.14 | M | 0.48 | 0.19 | 0.4 | 0.15 | |||||
| A | 0.26 | 0.16 | 0.18 | 0.16 | A | 0.16 | 0.08 | 0.19 | 0.08 | |||||
| DB | BL | C | 2.34 | 1.42 | 1.89 | 0.89 | L | BL | C | 1.83 | 0.56 | 1.95 | 1.06 | |
| M | 1.08 | 0.44 | 1.35 | 0.49 | M | 1.64 | 1.02 | 1.6 | 1.2 | |||||
| A | 0.51 | 0.32 | 0.35 | 0.25 | A | 0.65 | 0.71 | 0.68 | 0.91 | |||||
| MD | C | 0.53 | 0.24 | 0.58 | 0.23 | M-D | C | 0.69 * | 0.28 | 0.59 | 0.26 | |||
| M | 0.34 | 0.13 | 0.44 * | 0.12 | M | 0.39 | 0.21 | 0.4 | 0.17 | |||||
| A | 0.18 | 0.07 | 0.16 | 0.1 | A | 0.22 | 0.14 | 0.23 | 0.1 | |||||
| P | BL | C | 2.32 | 1.37 | 1.63 | 0.71 | D | B | L | C | 2.37 * | 0.67 | 1.55 | 0.8 |
| M | 1.08 | 0.4 | 1.29 | 0.39 | M | 1.35 | 1.27 | 1.18 | 0.61 | |||||
| A | 0.53 | 0.32 | 0.51 | 0.24 | A | 0.34 | 0.15 | 0.35 | 0.21 | |||||
| MD | C | 1.17 | 0.38 | 1.19 | 0.81 | MD | C | 0.67 | 0.19 | 0.6 | 0.29 | |||
| M | 0.79 | 0.4 | 0.99 | 0.45 | M | 0.31 | 0.15 | 0.46 | 0.09 | |||||
| A | 0.34 | 0.27 | 0.42 | 0.34 | A | 0.17 | 0.07 | 0.2 | 0.08 | |||||
| L | BL | C | 2.28 | 0.67 | 2.39 | 0.96 | ||||||||
| M | 1.9 | 1.04 | 2.22 | 1.11 | ||||||||||
| A | 0.88 | 1.07 | 1.04 | 1.02 | ||||||||||
| MD | C | 0.83 | 0.21 | 0.8 | 0.32 | |||||||||
| M | 0.43 | 0.14 | 0.44 | 0.14 | ||||||||||
| A | 0.2 | 0.09 | 0.26 * | 0.14 | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ticona-Flores, J.; Diéguez-Pérez, M. Cone-Beam Computed Tomography (CBTC) Applied to the Study of Root Morphological Characteristics of Deciduous Teeth: An In Vitro Study. Int. J. Environ. Res. Public Health 2022, 19, 9162. https://doi.org/10.3390/ijerph19159162
Ticona-Flores J, Diéguez-Pérez M. Cone-Beam Computed Tomography (CBTC) Applied to the Study of Root Morphological Characteristics of Deciduous Teeth: An In Vitro Study. International Journal of Environmental Research and Public Health. 2022; 19(15):9162. https://doi.org/10.3390/ijerph19159162
Chicago/Turabian StyleTicona-Flores, Jesús, and Montserrat Diéguez-Pérez. 2022. "Cone-Beam Computed Tomography (CBTC) Applied to the Study of Root Morphological Characteristics of Deciduous Teeth: An In Vitro Study" International Journal of Environmental Research and Public Health 19, no. 15: 9162. https://doi.org/10.3390/ijerph19159162
APA StyleTicona-Flores, J., & Diéguez-Pérez, M. (2022). Cone-Beam Computed Tomography (CBTC) Applied to the Study of Root Morphological Characteristics of Deciduous Teeth: An In Vitro Study. International Journal of Environmental Research and Public Health, 19(15), 9162. https://doi.org/10.3390/ijerph19159162