
Determinants of Delayed Initiation of Breastfeeding: A Cross-Sectional Multicenter Study in Abu Dhabi, the United Arab Emirates

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Data Collection
2.2. Study Instrument
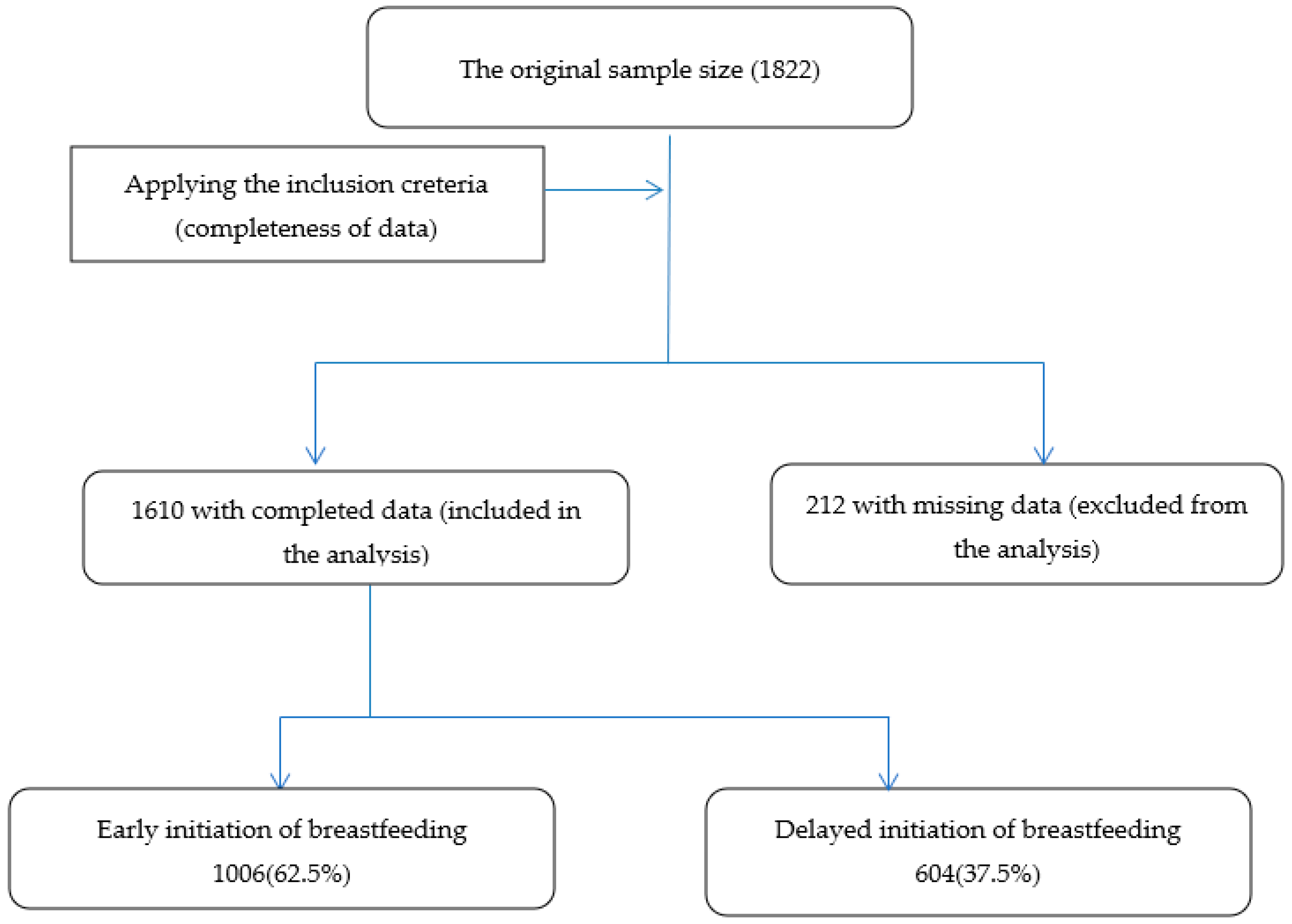
2.3. Study Inclusion and Exclusion Criteria
2.4. Statistical Analysis
2.5. Ethics
2.6. Definitions
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Committee on Sustainable Development Goals. UAE and the 2030 agenda for sustainable development excellence in implemenetation. Dev. Issues 2017, 4, 1–141. [Google Scholar]
- Births Attended by Skilled Health Staff (% of Total)—United Arab Emirates. Available online: https://data.worldbank.org/indicator/SH.STA.BRTC.ZS?locations=AE (accessed on 15 January 2022).
- Sharma, I.K.; Byrne, A. Early initiation of breastfeeding: A systematic literature review of factors and barriers in South Asia. Int. Breastfeed. J. 2016, 11, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taha, Z. Trends of breastfeeding in the United Arab Emirates (UAE). Arab J. Nutr. Exerc. 2017, 2, 152–159. [Google Scholar] [CrossRef]
- Taha, Z.; Garemo, M.; Nanda, J. Patterns of breastfeeding and complementary feeding practices among infants and young children in Abu Dhabi, United Arab Emirates. Int. Breastfeed. J. 2018, 13, 48. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Early Initiation of Breastfeeding to Promote Exclusive Breastfeeding; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Al-Nuaimi, N.; Katende, G.; Arulappan, J. Breastfeeding trends and determinants: Implications and recommendations for gulf cooperation council countries. Sultan Qaboos Univ. Med. J. 2017, 17, e155–e161. [Google Scholar] [CrossRef]
- Victora, C.G.; Bahl, R.; Barros, A.J.D.; França, G.V.A.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C.; et al. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [Green Version]
- Hassan, A.A.; Taha, Z.; Abdulla, M.A.; Ali, A.A.A.; Adam, I. Assessment of bottle-feeding practices in kassala, eastern sudan: A community-based study. Maced. J. Med. Sci. 2019, 7, 651–656. [Google Scholar] [CrossRef] [Green Version]
- Hassan, A.A.; Taha, Z.; Ahmed, M.A.A.; Ali, A.A.A.; Adam, I. Assessment of initiation of breastfeeding practice in Kassala, Eastern Sudan: A community-based study. Int. Breastfeed. J. 2018, 13, 34. [Google Scholar] [CrossRef] [Green Version]
- Hassan, A.A.; Taha, Z.; Ahmed, M.A.A.; Ali, A.A.A.; Adam, I. Causes and risk factors of hospitalization among under-five children in Kassala, Eastern Sudan. Open Access Maced. J. Med. Sci. 2020, 8, 451–457. [Google Scholar] [CrossRef]
- Account, L.M.; Guidelines, S.; Access, O. Time to initiation of breastfeeding and neonatal mortality and morbidity: A systematic review. BMC Public Health 2018, 13, S19. [Google Scholar]
- Edmond, K.M.; Zandoh, C.; Quigley, M.A.; Amenga-Etego, S.; Owusu-Agyei, S.; Kirkwood, B.R. Delayed breastfeeding initiation increases risk of neonatal mortality. Pediatrics 2006, 117, e380–e386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Victora, C.G.; Horta, B.L.; de Mola, C.L.; Quevedo, L.; Pinheiro, R.T.; Gigante, D.P.; Gonçalves, H.; Barros, F.C. Association between breastfeeding and intelligence, educational attainment, and income at 30 years of age: A prospective birth cohort study from Brazil. Lancet Glob. Health 2015, 3, e199–e205. [Google Scholar] [CrossRef] [Green Version]
- Qoronfeh, M.W.; Essa, M.M.; Alharahsheh, S.T.; Al-Farsi, Y.M.; Al-Adawi, S. Autism in the Gulf states: A regional overview. Front. Biosci. Landmark 2019, 24, 334–346. [Google Scholar] [CrossRef]
- GIFA: Geneva Infant Feeding Association. The Convention on the Rights of the Child Report on the Situation of Infant and Young Child Feeding in Baharian. 2011. Available online: https://archive.crin.org/en/docs/Bahrain_IBFAN_CRC%20Report.pdf (accessed on 17 April 2022).
- Radwan, H. Patterns and determinants of breastfeeding and complementary feeding practices of Emirati Mothers in the United Arab Emirates. BMC Public Health 2013, 13, 171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taha, Z.; Hassan, A.A.; Wikkeling-Scott, L.; Papandreou, D. Prevalence and associated factors of caesarean section and its impact on early initiation of breastfeeding in Abu Dhabi, United Arab Emirates. Nutrients 2019, 11, 2723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tilahun, G.; Degu, G.; Azale, T.; Tigabu, A. Prevalence and associated factors of timely initiation of breastfeeding among mothers at Debre Berhan town, Ethiopia: A cross-sectional study. Int. Breastfeed. J. 2016, 11, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azzeh, F.S.; Alazzeh, A.Y.; Hijazi, H.H.; Wazzan, H.Y.; Jawharji, M.T.; Jazar, A.S.; Filimban, A.M.; Alshamrani, A.S.; Labani, M.S.; Hasanain, T.A.; et al. Factors Associated with Not Breastfeeding and Delaying the Early Initiation of Breastfeeding in Mecca Region, Saudi Arabia. Children 2018, 5, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abu Dhabi Government. Abu Dhabi Emirate: Facts and Figures; Abu Dhabi Government: Abu Dhabi, United Arab Emirates, 2018. Available online: https://www.abudhabi.ae/portal/public/en/abu_dhabi_emirate/facts_figure_background?_adf.ctrlstate=ki3p4o0qf_4&_afrLoop=18541566215609417# (accessed on 11 February 2022).
- Alzaheb, R.A. A Review of the factors associated with the timely initiation of breastfeeding and exclusive breastfeeding in the Middle East. Clin. Med. Insights Pediatr. 2017, 11, 1179556517748912. [Google Scholar] [CrossRef] [Green Version]
- Bruno Tongun, J.; Sebit, M.B.; Mukunya, D.; Ndeezi, G.; Nankabirwa, V.; Tylleskar, T.; Tumwine, J.K. Factors associated with delayed initiation of breastfeeding: A cross-sectional study in South Sudan. Int. Breastfeed. J. 2018, 13, 28. [Google Scholar] [CrossRef]
- Maria, T.; Esteves, B.; Daumas, R.P.; Leite, I.C. Factors associated to breastfeeding in the first hour of life: Systematic review. Rev. Saúde Pública 2014, 48, 697–708. [Google Scholar] [CrossRef] [Green Version]
- McKinney, C.O.; Hahn-Holbrook, J.; Chase-Lansdale, P.L.; Ramey, S.L.; Krohn, J.; Reed-Vance, M.; Raju, T.N.K.; Shalowitz, M.U. Racial and ethnic differences in breastfeeding. Pediatrics 2016, 138, e20152388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alzaheb, R.A. Factors influencing exclusive breastfeeding in Tabuk, Saudi Arabia. Clin. Med. Insights Pediatr. 2017, 11, 1179556517698136. [Google Scholar] [CrossRef] [PubMed]
- Grajeda, R.; Pérez-Escamilla, R. Stress during labor and delivery is associated with delayed onset of lactation among urban Guatemalan women. J. Nutr. 2002, 132, 3055–3060. [Google Scholar] [CrossRef] [PubMed]
- Betran, A.P.; Torloni, M.R.; Zhang, J.; Ye, J.; Mikolajczyk, R.; Deneux-Tharaux, C.; Oladapo, O.T.; Souza, J.P.; Tunçalp, Ö.; Vogel, J.P.; et al. What is the optimal rate of caesarean section at population level? A systematic review of ecologic studies. Reprod. Health 2015, 12, 57. [Google Scholar] [CrossRef] [Green Version]
- Bandeira de Sá, N.N.; Gubert, M.B.; Santos, W.D.; Santos, L.M.P. Factors related to health services determine breastfeeding within one hour of birth in the Federal District of Brazil, 2011. Rev. Bras. Epidemiol. 2016, 19, 509–524. [Google Scholar] [CrossRef]
- World Health Organization and Unicef. Baby-Friendly Hospital Initiative Revised, Updated and Expanded for Integrated Care; WHO Press: Geneva, Switzerland, 2009; ISBN 9789241594950. Available online: http://www.who.int/nutrition/topics/bfhi/en/ (accessed on 18 February 2022).
- Elander, G.; Lindberg, T. Short mother-infant separation during first week of life influences the duration of breastfeeding. Acta Pædiatrica 1984, 73, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Escamilla, R.; Martinez, J.L.; Segura-Pérez, S. Impact of the Baby-friendly Hospital Initiative on breastfeeding and child health outcomes: A systematic review. Matern. Child Nutr. 2016, 12, 402–417. [Google Scholar] [CrossRef] [Green Version]
- Bystrova, K.; Widström, A.M.; Matthiesen, A.S.; Ransjö-Arvidson, A.B.; Welles-Nyström, B.; Vorontsov, I.; Uvnäs-Moberg, K. Early lactation performance in primiparous and multiparous women in relation to different maternity home practices. A randomised trial in St. Petersburg. Int. Breastfeed. J. 2007, 2, 9. [Google Scholar] [CrossRef] [Green Version]
- Declercq, E.R.; Sakala, C.; Corry, M.P.; Applebaum, S. Listening to mothers II: Report of the second National U.S. Survey of women’s childbearing experiences. J. Perinat. Educ. 2006, 16, 9–14. Available online: https://www.childbirthconnection.org/pdfs/LTMII_report.pdf (accessed on 13 March 2022). [CrossRef] [Green Version]
- Mikiel-Kostyra, K.; Mazur, J.; Wojdan-Godek, E. Factors affecting exclusive breastfeeding in Poland: Cross-sectional survey of population-based samples. Soz. Und Präventivmedizin/Soc. Prev. Med. 2005, 50, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Rashed, K.E. Infant and Young Child Feeding: Model Chapter for Textbooks for Medical Students and Allied Health Professionals; Session 2, The Physiological Basis of Breastfeeding; World Health Organization: Geneva, Switzerland, 2009. Available online: https://www.ncbi.nlm.nih.gov/bo (accessed on 20 March 2022).
- Primo, C.C.; De Oliveira Nunes, B.; De Fátima Almeida Lima, E.; Leite, F.M.C.; De Pontes, M.B.; Brandão, M.A.G. Which factors influence women in the decision to breastfeed? Investig. Educ. Enferm. 2016, 34, 198–210. [Google Scholar] [CrossRef] [Green Version]
- ACOG Committee Opinion. Breastfeeding in underserved women: Increasing initiation and continuation of breastfeeding. Obs. Gynecol. 2013, 122, 423–428. Available online: https://www.acog.org/-/media/Committee-Opinions/Committee-on-Health-Care-for-Underserved-Women/co570.pdf?dmc=1&ts=20160226T1125160305 (accessed on 23 February 2022). [CrossRef] [PubMed]
- Li, G.; Cong, J.; Li, L.; Li, Y. Effects of nursing with information support and behavior intervention on lactation and breastfeeding success rate for primiparas. Int. J. Clin. Exp. Med. 2018, 11, 2617–2623. [Google Scholar]
- Elmugabil, A.; Rayis, D.A.; Hassan, A.A.; Ali, A.A.; Adam, I. Epidemiology of cesarean delivery in Kassala, eastern Sudan: A community-based study 2014–2015. Sudan J. Med. Sci. 2016, 11, 49–54. [Google Scholar]
- Andayasari, L.; Opitasari, C. Parity and risk of low birth weight infant in full term pregnancy. Health Sci. J. Indones. 2016, 7, 13–16. [Google Scholar] [CrossRef]
- Hassan, A.A.; Abubaker, M.S.; Radi, E.A.; Adam, I. Education, prenatal care, and poor perinatal outcome in Khartoum, Sudan. Int J Gynaecol. Obs. 2009, 105, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Baruah, C. A comparative study of obstetric complications among primigravida and multigravida attending labour room of a tertiary care hospital. Indian J. Basic Appl. Med. Res. 2016, 5, 147–153. [Google Scholar]
- Gardner, H.; Green, K.; Gardner, A.S.; Geddes, D. Observations on the health of infants at a time of rapid societal change: A longitudinal study from birth to fifteen months in Abu Dhabi. BMC Pediatr. 2018, 18, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khanal, V.; Scott, J.; Lee, A.; Karkee, R.; Binns, C. Factors associated with Early Initiation of Breastfeeding in Western Nepal. Int. J. Environ. Res. Public Health 2015, 12, 9562–9574. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Feeding of Low-Birth-Weight Infants in Low- and Middle-Income Countries; World Health Organization: Geneva, Switzerland, 2018; Available online: https://www.who.int/elena/titles/full_recommendations/feeding_lbw/en/ (accessed on 18 April 2022).
- Mukunya, D.; Tumwine, J.K.; Nankabirwa, V.; Ndeezi, G.; Tumuhamye, J.; Tongun, J.B.; Kizito, S.; Achora, V.; Odongkara, B.; Tylleskar, T.; et al. Factors associated with delayed initiation of breastfeeding: A survey in Northern Uganda. Glob. Health Action 2017, 10, 1410975. [Google Scholar] [CrossRef]
- Sharma, A.; Thakur, P.S.; Tiwari, R.; Kasar, P.K.; Sharma, R.; Kabirpanthi, V. Factors associated with early initiation of breastfeeding among mothers of tribal area of Madhya Pradesh, India: A community based cross sectional study. Int. J. Community Med. Public Heal 2016, 3, 194–199. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Total (n = 1610) | Initiation of Breastfeeding | ||
|---|---|---|---|---|
| Early (n = 1006) | Delayed (n = 604) | |||
| Mean (SD) | Mean (SD) | Mean (SD) | p-Value | |
| Maternal age, years | 30.1 (5.1) | 30.0 (5.3) | 30.3 (4.8) | 0.293 |
| Child age, months | 8.1 (5.9) | 8.7 (6.1) | 7.1 (5.5) | <0.001 |
| Birth order | 2.2 (1.2) | 2.3 (1.3) | 2.1 (1.2) | <0.001 |
| Gestational age at delivery, weeks | 39.1 (1.9) | 39.3 (1.6) | 38.8 (2.2) | <0.001 |
| Birth weight at delivery, grams | 3080 (518) | 3159 (449) | 2948 (594) | <0.001 |
| Pre-pregnancy BMI, kg/m2 | 23.9 (3.9) | 23.9 (3.8) | 23.9 (4.0) | 0.451 |
| Variables | Total (n = 1610) | Time of Breastfeeding Initiation | |||
|---|---|---|---|---|---|
| Early (n = 1006) | Delayed (n = 604) | ||||
| N (%) | N (%) | N (%) | p-Value | ||
| Maternal education | Not educated <Secondary level | 64 (4.0) | 49 (4.9) | 15 (2.5) | 0.018 |
| Educated ≥ Secondary level | 1546 (96.0) | 957 (95.1) | 589 (97.5) | ||
| Paternal education | Not educated <Secondary level | 31 (1.9) | 26 (2.6) | 5 (0.8) | 0.013 |
| Educated ≥ Secondary level | 1579 (98.1) | 980 (97.4) | 599 (99.2) | ||
| Maternal occupation | Unemployed | 996 (62.2) | 610 (61.2) | 386 (38.8) | 0.121 |
| Employed | 606 (37.8) | 393 (64.9) | 213 (35.1) | ||
| Nationality | Arab | 1049 (65.2) | 686 (68.2) | 363 (60.1) | 0.001 |
| Non-Arab | 561 (34.8) | 320 (31.8) | 241 (39.9) | ||
| Marital status | Married | 1588 (98.6) | 993 (98.7) | 595 (98.5) | 0.741 |
| Unmarried | 22 (1.4) | 13 (1.3) | 9 (1.5) | ||
| Received breastfeeding advice during pregnancy | Yes | 1408 (87.5) | 859 (85.4) | 549 (90.9) | 0.001 |
| No | 202 (12.5) | 147 (14.6) | 55 (9.1) | ||
| Received breastfeeding support | Yes | 1489 (92.5) | 914 (90.9) | 575 (95.2) | 0.001 |
| No | 121 (7.5) | 92 (9.1) | 29 (4.8) | ||
| Mode of delivery | Vaginal delivery | 1121 (69.6) | 796 (79.1) | 325 (53.8) | <0.001 |
| Caesarean delivery | 489 (30.4) | 210 (20.9) | 279 (46.2) | ||
| Child gender | Male | 790 (49.1) | 485 (48.2) | 305 (50.5) | 0.374 |
| Female | 820 (50.9) | 521 (51.8) | 299 (49.5) | ||
| Rooming-in | Yes | 1549 (96.2) | 986 (98.0) | 563 (93.2) | <0.001 |
| No | 61 (3.8) | 20 (2.0) | 41 (6.8) | ||
| Variables | Crude OR with (95% CI) | Adjusted OR with (95% CI) | p-Value | |
|---|---|---|---|---|
| Maternal education status | Educated ≥ Secondary level | 2.01 (1.12, 3.62) | 1.64 (0.88, 3.09) | 0.123 |
| Not educated <Secondary level (Reference) | ||||
| Paternal education status | Educated ≥ Secondary level | 3.18 (1.21, 8.32) | 2.61 (0.94, 7.28) | 0.066 |
| Not educated <Secondary level (Reference) | ||||
| Nationality | Non-Arab | 1.42 (1.15, 1.76) | 1.30 (1.03, 1.63) | 0.027 |
| Arab (Reference) | ||||
| Receiving of breastfeeding advice during pregnancy | Not received | 0.59 (0.42, 0.81) | 0.73 (0.50, 1.07) | 0.111 |
| Received (Reference) | ||||
| Received breastfeeding support | No | 0.50 (0.33, 0.77) | O.77 (0.47, 1.26) | 0.298 |
| Yes (Reference) | ||||
| Mode of delivery | Caesarean delivery | 3.25 (2.61, 4.06) | 2.85 (2.26, 3.58) | <0.001 |
| Vaginal delivery (Reference) | ||||
| Rooming-in | No | 3.59 (2.08, 6.19) | 2.82 (1.53, 5.21) | 0.001 |
| Yes (Reference) | ||||
| Birth order | First | 1.53 (1.25, 1.89) | 1.34 (1.07, 1.69) | 0.011 |
| Second and more (Reference) | ||||
| Gestational age in weeks | Preterm (<37 weeks) | 2.53 (1.68, 3.81) | 1.02 (0.61, 1.71) | 0.941 |
| Term (≥37 weeks) (Reference) | ||||
| Birth weight in grams | L.B.W. (<2500 g) | 4.55 (3.16, 6.55) | 3.30 (2.18, 4.99) | <0.001 |
| Normal birth weight (≥2500 g) (Reference) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taha, Z.; Al Dhaheri, A.I.; Wikkeling-Scott, L.; Ali Hassan, A.; Papandreou, D. Determinants of Delayed Initiation of Breastfeeding: A Cross-Sectional Multicenter Study in Abu Dhabi, the United Arab Emirates. Int. J. Environ. Res. Public Health 2022, 19, 9048. https://doi.org/10.3390/ijerph19159048
Taha Z, Al Dhaheri AI, Wikkeling-Scott L, Ali Hassan A, Papandreou D. Determinants of Delayed Initiation of Breastfeeding: A Cross-Sectional Multicenter Study in Abu Dhabi, the United Arab Emirates. International Journal of Environmental Research and Public Health. 2022; 19(15):9048. https://doi.org/10.3390/ijerph19159048
Chicago/Turabian StyleTaha, Zainab, Aysha Ibrahim Al Dhaheri, Ludmilla Wikkeling-Scott, Ahmed Ali Hassan, and Dimitrios Papandreou. 2022. "Determinants of Delayed Initiation of Breastfeeding: A Cross-Sectional Multicenter Study in Abu Dhabi, the United Arab Emirates" International Journal of Environmental Research and Public Health 19, no. 15: 9048. https://doi.org/10.3390/ijerph19159048
APA StyleTaha, Z., Al Dhaheri, A. I., Wikkeling-Scott, L., Ali Hassan, A., & Papandreou, D. (2022). Determinants of Delayed Initiation of Breastfeeding: A Cross-Sectional Multicenter Study in Abu Dhabi, the United Arab Emirates. International Journal of Environmental Research and Public Health, 19(15), 9048. https://doi.org/10.3390/ijerph19159048