
Is Silver Diamine Fluoride Effective in Arresting Enamel Caries? A Randomized Clinical Trial


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Size Calculation
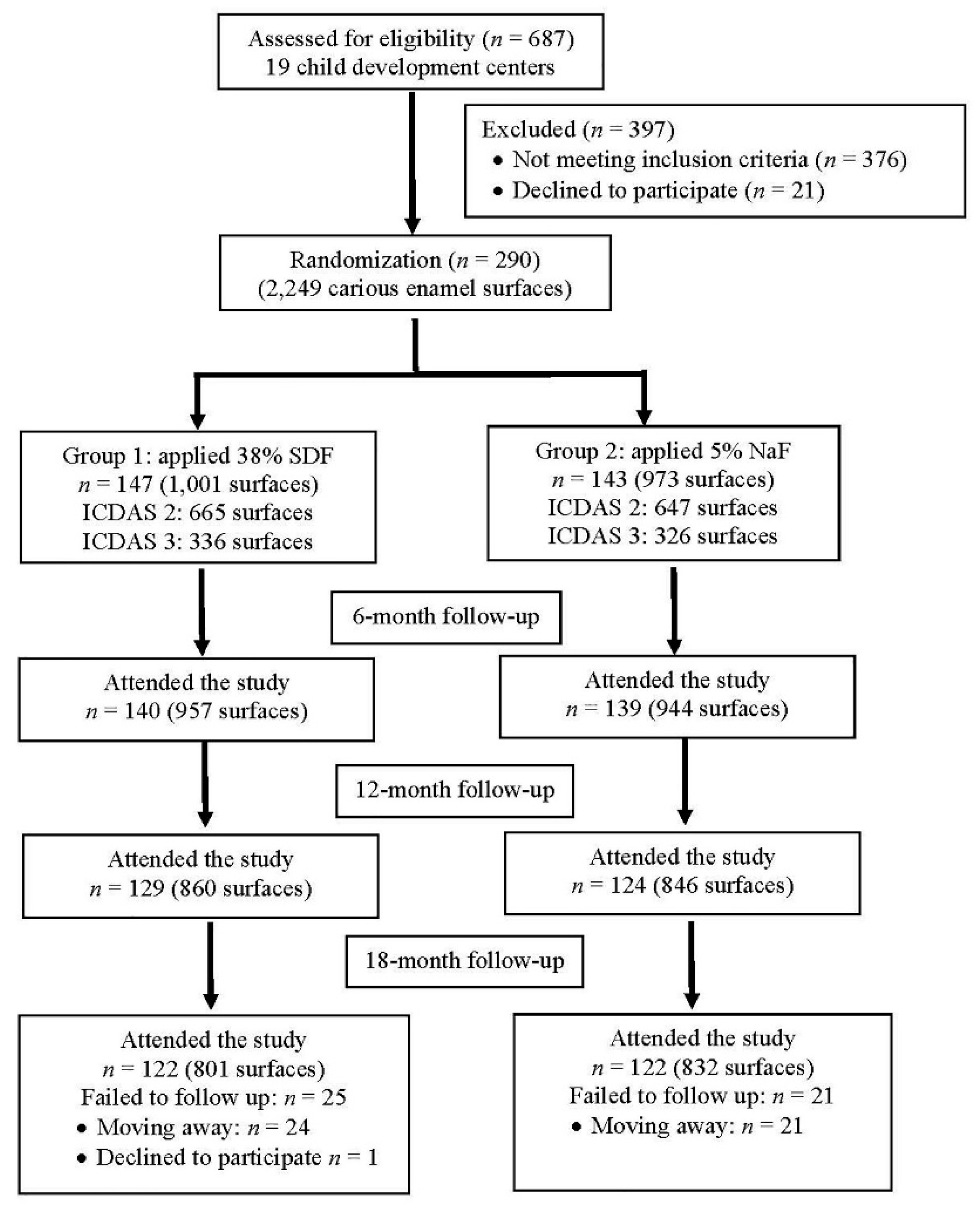
2.2. Participants, Inclusion Criteria, and Setting
2.3. Randomization
2.4. Intervention
2.5. Outcome Assessment
2.6. Data Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thitasomakul, S.; Thearmontree, A.; Piwat, S.; Chankanka, O.; Pithpornchaiyakul, W.; Teanpaisan, R.; Madyusoh, S. A longitudinal study of early childhood caries in 9- to 18-month-old Thai infants. Community Dent. Oral Epidemiol. 2006, 34, 429–436. [Google Scholar] [CrossRef]
- Tinanoff, N.; Baez, R.J.; Diaz Guillory, C.; Donly, K.J.; Feldens, C.A.; McGrath, C.; Phantumvanit, P.; Pitts, P.B.; Seow, W.K.; Sharkov, N.; et al. Early childhood caries epidemiology, aetiology, risk assessment, societal burden, management, education, and policy: Global perspective. Int. J. Paediatr. Dent. 2019, 29, 238–248. [Google Scholar] [CrossRef]
- Duangthip, D.; Gao, S.S.; Chen, K.J.; Lo, E.C.M.; Chu, C.H. Oral health related quality of life and caries experience of Hong Kong preschool children. Int. Dent. J. 2020, 70, 100–107. [Google Scholar] [CrossRef]
- Zaror, C.; Matamala-Santander, A.; Ferrer, M.; Rivera-Mendoza, F.; Espinoza-Espinoza, G.; Martínez-Zapata, M.J. Impact of early childhood caries on oral health-related quality of life: A systematic review and meta-analysis. Int. J. Dent. Hyg. 2021, 20, 120–135. [Google Scholar] [CrossRef]
- Gao, S.S.; Zhang, S.; Mei, M.L.; Lo, E.C.M.; Chu, C.H. Caries remineralisation and arresting effect in children by professionally applied fluoride treatment–A systematic review. BMC Oral Health 2016, 16, 12. [Google Scholar] [CrossRef] [Green Version]
- Ma, X.; Lin, X.; Zhong, T.; Xie, F. Evaluation of the efficacy of casein phosphopeptide-amorphous calcium phosphate on remineralization of white spot lesions in vitro and clinical research: A systematic review and meta-analysis. BMC Oral Health 2019, 19, 295. [Google Scholar] [CrossRef] [Green Version]
- Wierichs, R.J.; Carvalho, T.S.; Wolf, T.G. Efficacy of a self-assembling peptide to remineralize initial caries lesions–A systematic review and meta-analysis. J. Dent. 2021, 109, 103652. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.; Worthington, H.V.; Glenny, A.M.; Marinho, V.C.; Jeroncic, A. Fluoride toothpastes of different concentrations for preventing dental caries. Cochrane Database Syst. Rev. 2019, CD007868. [Google Scholar] [CrossRef] [PubMed]
- Marinho, V.C.; Worthington, H.V.; Walsh, T.; Chong, L.Y. Fluoride gels for preventing dental caries in children and adolescents. Cochrane Database Syst. Rev. 2015, CD002280. [Google Scholar] [CrossRef]
- Urquhart, O.; Tampi, M.P.; Pilcher, L.; Slayton, R.L.; Araujo, M.W.B.; Fontana, M.; Guzmán-Armstrong, S.; Nascimento, M.M.; Nový, B.B.; Tinanoff, N.; et al. Nonrestorative treatments for caries: Systematic review and network meta-analysis. J. Dent. Res. 2019, 98, 14–26. [Google Scholar] [CrossRef]
- Lussi, A.; Buzalaf, M.A.R.; Duangthip, D.; Anttonen, V.; Ganss, C.; João-Souza, S.H.; Baumann, T.; Carvalho, T.S. The use of fluoride for the prevention of dental erosion and erosive tooth wear in children and adolescents. Eur. Arch. Paediatr. Dent. 2019, 20, 517–527. [Google Scholar] [CrossRef] [PubMed]
- Ludovichetti, F.S.; Zambon, G.; Cimolai, M.; Gallo, M.; Signoriello, A.G.; Pezzato, L.; Bertolini, R.; Mazzoleni, S. Efficacy of two toothpaste in preventing tooth erosive lesions associated with gastroesophageal reflux disease. Appl. Sci. 2022, 12, 1023. [Google Scholar] [CrossRef]
- Buzalaf, M.A.R.; Pessan, J.P.; Honório, H.M.; Ten Cate, J.M. Mechanisms of action of fluoride for caries control. Fluoride Oral Environ. 2011, 22, 97–114. [Google Scholar] [CrossRef]
- Lenzi, T.L.; Montagner, A.F.; Soares, F.Z.; de Oliveira Rocha, R. Are topical fluorides effective for treating incipient carious lesions? A systematic review and meta-analysis. J. Am. Dent. Assoc. 2016, 147, 84–91.e1. [Google Scholar] [CrossRef]
- Weyant, R.J.; Tracy, S.L.; Anselmo, T.; Beltrán-Aguilar, E.J.; Donly, K.J.; Frese, W.A. Topical fluoride for caries prevention: Executive summary of the updated clinical recommendations and supporting systematic review. J. Am. Dent. Assoc. 2013, 144, 1279–1291. [Google Scholar] [CrossRef]
- Slayton, R.L.; Urquhart, O.; Araujo, M.W.B.; Fontana, M.; Guzmán-Armstrong, S.; Nascimento, M.M.; Nový, B.B.; Tinanoff, N.; Weyant, R.J.; Wolff, M.S.; et al. Evidence-based clinical practice guideline on nonrestorative treatments for carious lesions: A report from the American Dental Association. J. Am. Dent. Assoc. 2018, 149, 837–849.e19. [Google Scholar] [CrossRef] [Green Version]
- Rosenblatt, A.; Stamford, T.C.M.; Niederman, R. Silver diamine fluoride: A caries “silver-fluoride bullet”. J. Dent. Res. 2009, 88, 116–125. [Google Scholar] [CrossRef]
- Seifo, N.; Cassie, H.; Radford, J.R.; Innes, N. Silver diamine fluoride for managing carious lesions: An umbrella review. BMC Oral Health 2019, 19, 145. [Google Scholar] [CrossRef]
- Gao, S.S.; Amarquaye, G.; Arrow, P.; Bansal, K.; Bedi, R.; Campus, G.; Chen, K.; Chibinski, A.C.; Chinzorig, T.; Crystal, Y.O.; et al. Global Oral Health Policies and Guidelines: Using Silver Diamine Fluoride for Caries Control. Front. Oral Health 2021, 2, 685557. [Google Scholar] [CrossRef]
- Sutthavong, S.; Taebanpakul, S.; Kuruchitkosol, C.; Ayudhya, T.I.; Chantveerawong, T.; Fuangroong, S.; Cae-Ngow, S.; Rangsin, R. Oral health status, dental caries risk factors of the children of public kindergarten and schools in Phranakornsriayudhya, Thailand. J. Med. Assoc. Thai 2010, 93, S71–S78. [Google Scholar]
- Masood, M.; Masood, Y.; Newton, J.T. The clustering effects of surfaces within the tooth and teeth within individuals. J. Dent. Res. 2015, 94, 281–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Twisk, J.W.R. Applied Multilevel Analysis: Practical Guides to Biostatistics and Epidemiology; Cambridge University Press: Cambridge, UK, 2006. [Google Scholar]
- Mabangkhru, S.; Duangthip, D.; Chu, C.H.; Phonghanyudh, A.; Jirarattanasopha, V. A randomized clinical trial to arrest dentin caries in young children using silver diamine fluoride. J. Dent. 2020, 99, 103375. [Google Scholar] [CrossRef] [PubMed]
- Duangthip, D.; Wong, M.C.M.; Chu, C.H.; Lo, E.C.M. Caries arrest by topical fluorides in preschool children: 30-month results. J. Dent. 2018, 70, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.Y.; Lo, E.C.M.; Li, C.M.T. Effect of silver and fluoride ions on enamel demineralization: A quantitative study using micro-computed tomography. Aust. Dent. J. 2012, 57, 65–70. [Google Scholar] [CrossRef]
- Duangthip, D.; Chu, C.H.; Lo, E.C.M. A randomized clinical trial on arresting dentine caries in preschool children by topical fluorides--18 month results. J. Dent. 2016, 44, 57–63. [Google Scholar] [CrossRef]
- Duangthip, D.; Fung, M.H.T.; Wong, M.C.M.; Chu, C.H.; Lo, E.C.M. Adverse Effects of Silver Diamine Fluoride Treatment among Preschool Children. J. Dent. Res. 2018, 97, 395–401. [Google Scholar] [CrossRef]
- Whitford, G.M. Fluoride in dental products: Safety considerations. J. Dent. Res. 1987, 66, 1056–1060. [Google Scholar] [CrossRef]
- Horst, J.A.; Ellenikiotis, H.; Milgrom, P.M. UCSF Protocol for caries arrest using silver diamine fluoride: Rationale, indications and consent. J. Calif. Dent. Assoc. 2016, 44, 16. [Google Scholar]
- Crystal, Y.O.; Janal, M.N.; Hamilton, D.S.; Niederman, R. Parental perceptions and acceptance of silver diamine fluoride staining. J. Am. Dent. Assoc. 2017, 148, 510–518.e4. [Google Scholar] [CrossRef]
- Sabbagh, H.; Othman, M.; Khogeer, L.; Al-Harbi, H.; Al Harthi, A.; Abdulgader Yaseen Abdulgader, A. Parental acceptance of silver Diamine fluoride application on primary dentition: A systematic review and meta-analysis. BMC Oral Health 2020, 20, 227. [Google Scholar] [CrossRef]

{kind=link}
| Group 1: 38% SDF (n = 147) | Group 2: 5% NaF (n = 143) | p-Value | |
|---|---|---|---|
| Demographic background | Mean (SD) | Mean (SD) | |
| Age(months) (min-max) | 37 (7) (21–46) | 37 (6) (18–47) | 0.485 |
| Demographic background | n (%) | n (%) | |
| Gender | 0.577 | ||
| Male | 60 (40.8) | 63 (44.1) | |
| Female | 87 (59.2) | 80 (55.9) | |
| Mother’s education level | 0.014 | ||
| Primary school or lower | 74 (50.3) | 94 (65.7) | |
| Secondary school | 58 (39.5) | 34 (23.8) | |
| College or university | 15 (10.2) | 15 (10.5) | |
| Monthly family income | 0.841 | ||
| <10,000 Baht | 86 (58.5) | 82 (57.3) | |
| ≥10,000 Baht | 61 (41.5) | 61 (42.7) | |
| Oral health-related habits | n (%) | n (%) | |
| Daily milk feeding | 0.939 | ||
| None | 27 (18.4) | 27 (18.9) | |
| 1–3 times | 74 (50.3) | 74 (51.7) | |
| >3 times | 46 (31.3) | 42 (29.4) | |
| Sleep with bottle | 0.300 | ||
| Yes | 60 (40.8) | 67(46.9) | |
| No | 87 (59.2) | 76 (53.1) | |
| Daily snack taking | 0.154 | ||
| <1 time | 15 (10.2) | 12 (8.4) | |
| 1–2 times | 104 (70.7) | 90 (62.9) | |
| ≥3 times | 28 (19.0) | 41 (28.7) | |
| Daily tooth brushing | 0.697 | ||
| <2 time | 16(10.9) | 13 (9.4) | |
| ≥2 times | 131 (89.1) | 130 (90.9) | |
| Brushing with fluoride toothpaste | 0.941 | ||
| Yes | 134(91.2) | 130 (90.9) | |
| No | 13 (8.8) | 13 (9.1) | |
| Clinical characteristics | Mean (SD) | Mean (SD) | |
| dmft | 5.0 (3.1) | 5.8 (4.0) | 0.247 |
| dmfs | 8.6 (7.1) | 10.5 (10.7) | 0.422 |
| visible plaque index | 0.7 (0.2) | 0.7 (0.2) | 0.526 |
| Caries characteristics | n = 1001 n (%) | n = 973 n (%) | |
| Extent of caries | 0.977 | ||
| Non-cavitated enamel caries (ICDAS 2) | 665 (66.4) | 647 (66.5) | |
| Cavitated enamel caries (ICDAS 3) | 336 (33.6) | 326 (33.5) | |
| Tooth position | 0.067 | ||
| Upper anterior teeth | 435 (43.5) | 388 (39.9) | |
| Upper posterior teeth | 218 (21.8) | 242 (24.9) | |
| Lower anterior teeth | 143 (14.3) | 117 (12.0) | |
| Lower posterior teeth | 205 (20.5) | 226 (23.2) | |
| Tooth surface type | 0.409 | ||
| Buccal/lingual | 750 (74.9) | 709 (72.9) | |
| Proximal | 66 (6.6) | 61 (6.3) | |
| Occlusal | 185 (18.5) | 203 (20.8) |
| Group 1: 38% SDF %(n/N) | Group 2: 5% NaF %(n/N) | p-Value | |
|---|---|---|---|
| Overall | |||
| 6 months | 86.5 (866/1001) | 82.7 (805/973) | 0.020 |
| 12 months | 68.5 (686/1001) | 63.7 (620/973) | 0.024 |
| 18 months | 59.1 (592/1001) | 58.8 (572/973) | 0.873 |
| Non-cavitated enamel caries (ICDAS 2) | |||
| 6 months | 92.6 (617/666) | 90.6 (587/648) | 0.178 |
| 12 months | 77.9 (519/666) | 73.3 (475/648) | 0.051 |
| 18 months | 68.2 (454/666) | 69.6 (451/648) | 0.576 |
| Cavitated enamel caries (ICDAS 3) | |||
| 6 months | 74.3 (249/335) | 67.1 (218/325) | 0.041 |
| 12 months | 49.9 (167/335) | 44.6 (145/325) | 0.178 |
| 18 months | 41.2 (138/335) | 37.2 (121/325) | 0.297 |
| Explanatory Variables | Adjusted Odds Ratio a | 95% CI | p-Value |
|---|---|---|---|
| Group | |||
| 38% SDF | 1.13 | 0.79–1.60 | 0.501 |
| 5% NaF | 1 | ||
| Tooth position | |||
| Lower anterior | 1.83 | 1.29–2.61 | 0.001 |
| Lower posterior | 0.77 | 0.58–1.01 | 0.060 |
| Upper posterior | 1.02 | 0.77–1.34 | 0.909 |
| Upper anterior | 1 | ||
| Tooth surface type | |||
| Buccal/lingual | 1.47 | 1.10–1.95 | 0.009 |
| Proximal | 0.39 | 0.22–0.67 | 0.001 |
| Occlusal | 1 | ||
| ICDAS baseline | |||
| ICDAS = 2 | 2.89 | 2.31–3.60 | <0.001 |
| ICDAS = 3 | 1 | ||
| Use Fluoride toothpaste | |||
| Yes | 2.39 | 1.21–4.74 | 0.012 |
| No | 1 | ||
| Baseline dmfs | 0.97 | 0.96–0.99 | 0.001 |
| Group 1: 38%SDF | Group 2: 5%NaF | p-Value | |
|---|---|---|---|
| %(n/N) | %(n/N) | ||
| Baseline | N = 147 | N = 143 | 0.504 * |
| Satisfied | 63.9 (94/147) | 60.1 (86/143) | |
| Unsatisfied | 36.1 (53/147) | 39.9 (57/143) | |
| 18-month | N = 122 | N = 122 | 0.896 * |
| Satisfied | 59.8 (73/122) | 60.7 (74/122) | |
| Unsatisfied | 40.2 (49/122) | 39.3 (48/122) | |
| p-value | 0.775 ** | 1.00 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phonghanyudh, A.; Duangthip, D.; Mabangkhru, S.; Jirarattanasopha, V. Is Silver Diamine Fluoride Effective in Arresting Enamel Caries? A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2022, 19, 8992. https://doi.org/10.3390/ijerph19158992
Phonghanyudh A, Duangthip D, Mabangkhru S, Jirarattanasopha V. Is Silver Diamine Fluoride Effective in Arresting Enamel Caries? A Randomized Clinical Trial. International Journal of Environmental Research and Public Health. 2022; 19(15):8992. https://doi.org/10.3390/ijerph19158992
Chicago/Turabian StylePhonghanyudh, Araya, Duangporn Duangthip, Sirinan Mabangkhru, and Varangkanar Jirarattanasopha. 2022. "Is Silver Diamine Fluoride Effective in Arresting Enamel Caries? A Randomized Clinical Trial" International Journal of Environmental Research and Public Health 19, no. 15: 8992. https://doi.org/10.3390/ijerph19158992
APA StylePhonghanyudh, A., Duangthip, D., Mabangkhru, S., & Jirarattanasopha, V. (2022). Is Silver Diamine Fluoride Effective in Arresting Enamel Caries? A Randomized Clinical Trial. International Journal of Environmental Research and Public Health, 19(15), 8992. https://doi.org/10.3390/ijerph19158992