
Cutaneous Manifestations of COVID-19 in the Lower Limbs: A Narrative Review

 , and
, and 
Abstract
:1. Introduction
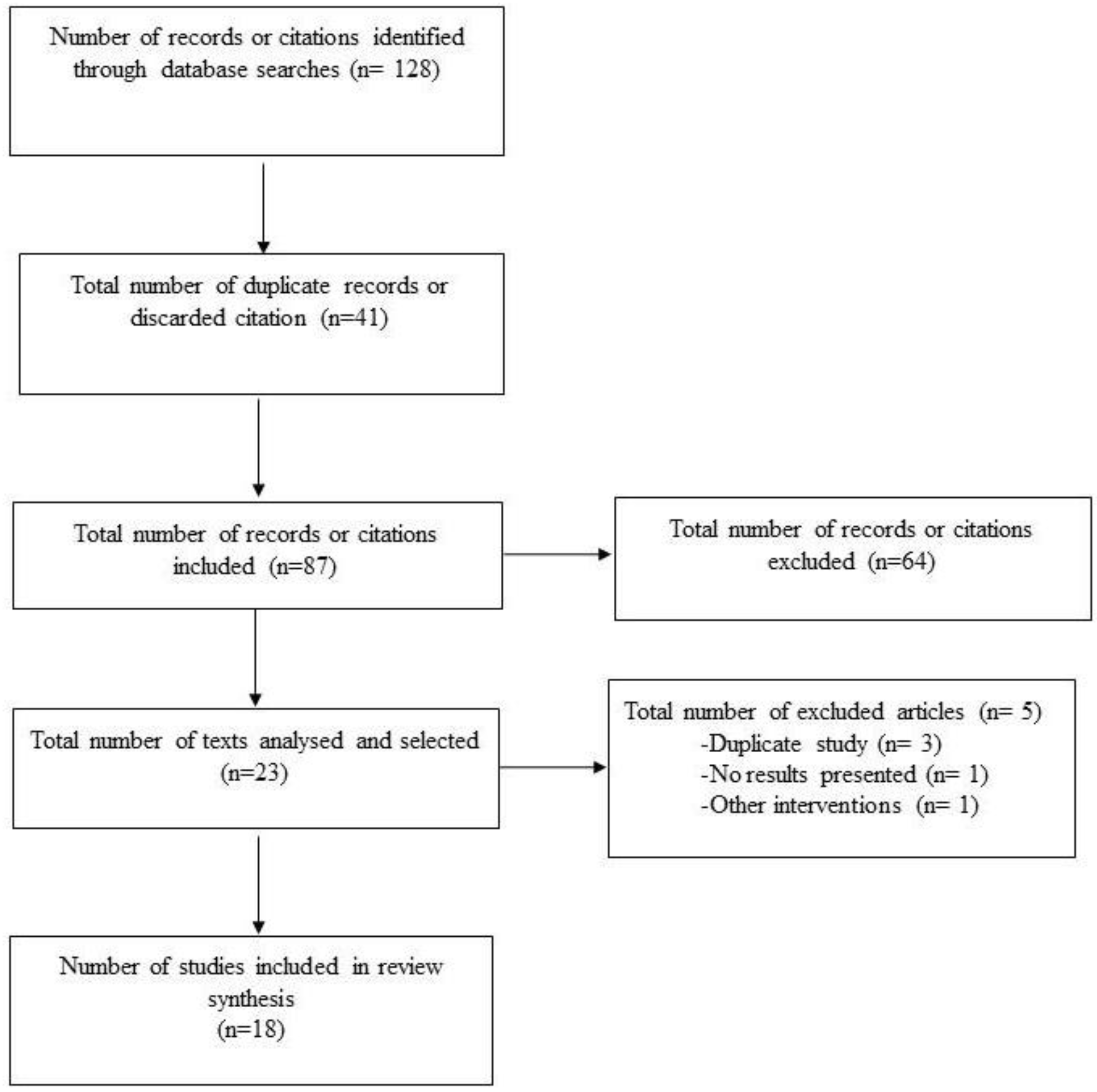
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Severe Acute Respiratory Syndrome (SARS). Available online: https://www.who.int/health-topics/severe-acute-respiratory-syndrome#tab=tab_1 (accessed on 3 December 2021).
- Greenberg, S.B. Update on Human Rhinovirus and Coronavirus Infections. Semin. Respir. Crit. Care Med. 2016, 37, 555–571. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Peng, F.; Wang, R.; Guan, K.; Jiang, T.; Xu, G.; Sun, J.; Chang, C. The deadly coronaviruses: The 2003 SARS pandemic and the 2020 novel coronavirus epidemic in China. J. Autoimmun. 2020, 109, 102434. [Google Scholar] [CrossRef]
- Martín-Sánchez, V.; Barquilla-García, A.; Vitelli-Storelli, F.; Segura-Fragoso, A.; Ruiz-García, A.; Serrano-Cumplido, A.; Olmo-Quintana, V.; Calderón-Montero, A. Analysis of fatality rates case of SARS-CoV-2 infection in the Autonomous Communities of Spain. Semergen 2020, 46, 12–19. [Google Scholar] [CrossRef]
- Chen, Y.; Peng, H.; Wang, L.; Zhao, Y.; Zeng, L.; Gao, H.; Liu, Y. Infants Born to Mothers With a New Coronavirus (COVID-19). Front. Pediatr. 2020, 8, 104. [Google Scholar] [CrossRef]
- Yesudhas, D.; Srivastava, A.; Gromiha, M.M. COVID-19 outbreak: History, mechanism, transmission, structural studies and therapeutics. Infection 2021, 49, 199–213. [Google Scholar] [CrossRef]
- Suchonwanit, P.; Leerunyakul, K.; Kositkuljorn, C. Cutaneous manifestations in COVID-19: Lessons learned from current evidence. J. Am. Acad. Dermatol. 2020, 83, e57–e60. [Google Scholar] [CrossRef]
- Gül, Ü. COVID-19 and dermatology. Turk. J. Med. Sci. 2020, 50, 1751–1759. [Google Scholar] [CrossRef]
- Jimenez-Cebrian, A.M.; Castro-Mendez, A.; García-Podadera, B.; Romero-Galisteo, R.; Medina-Alcántara, M.; Garcia-Paya, I.; Páez-Moguer, J.; Córdoba-Fernández, A. Clinical manifestations of covid-19 in the feet: A review of reviews. J. Clin. Med. 2021, 10, 2201. [Google Scholar] [CrossRef]
- Vilar-Palomo, S.; Pabón-Carrasco, M.; Gonzalez-Elena, M.L.; Ramírez-Baena, L.; Rodríguez-Gallego, I.; Castro-Méndez, A. Assessment of the anxiety level of andalusian podiatrists during the covid-19 pandemic: The increase phase. Healthcare 2020, 8, 432. [Google Scholar] [CrossRef]
- Rahimi, H.; Tehranchinia, Z. A Comprehensive Review of Cutaneous Manifestations Associated with COVID-19. BioMed Res. Int. 2020, 2020, 1236520. [Google Scholar] [CrossRef]
- Tao, J.; Song, Z.; Yang, L.; Huang, C.; Feng, A.; Man, X. Emergency management for preventing and controlling nosocomial infection of the 2019 novel coronavirus: Implications for the dermatology department. Br. J. Dermatol. 2020, 182, 1477–1478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, S.; Lin, J.; Zhang, Z.; Xiao, L.; Jiang, Z.; Chen, J.; Hu, C.; Luo, S. Alert for non-respiratory symptoms of coronavirus disease 2019 patients in epidemic period: A case report of familial cluster with three asymptomatic COVID-19 patients. J. Med. Virol. 2021, 93, 518–521. [Google Scholar] [CrossRef] [PubMed]
- Manalo, I.F.; Smith, M.K.; Cheeley, J.; Jacobs, R. A dermatologic manifestation of COVID-19: Transient livedo reticularis. J. Am. Acad. Dermatol. 2020, 83, 700. [Google Scholar] [CrossRef] [PubMed]
- Galván Casas, C.; Català, A.; Carretero Hernández, G.; Rodríguez-Jiménez, P.; Fernández-Nieto, D.; Rodríguez-Villa Lario, A.; Navarro Fernández, I.; Ruiz-Villaverde, R.; Falkenhain-López, D.; Llamas Velasco, M.; et al. Classification of the cutaneous manifestations of COVID-19: A rapid prospective nationwide consensus study in Spain with 375 cases. Br. J. Dermatol. 2020, 183, 71–77. [Google Scholar] [CrossRef]
- Carrascosa, J.M.; Morillas, V.; Bielsa, I.; Munera-Campos, M. Cutaneous Manifestations in the Context of SARS-CoV-2 Infection (COVID-19). Actas Dermosifiliogr. 2020, 111, 734–742. [Google Scholar] [CrossRef]
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Recalcati, S.; Barbagallo, T.; Frasin, L.A.; Prestinari, F.; Cogliardi, A.; Provero, M.C.; Dainese, E.; Vanzati, A.; Fantini, F. Acral cutaneous lesions in the time of COVID-19. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e346–e347. [Google Scholar] [CrossRef]
- Estébanez, A.; Pérez-Santiago, L.; Silva, E.; Guillen-Climent, S.; García-Vázquez, A.; Ramón, M.D. Cutaneous manifestations in COVID-19: A new contribution. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e250–e251. [Google Scholar] [CrossRef] [Green Version]
- Henry, D.; Ackerman, M.; Sancelme, E.; Finon, A.; Esteve, E. Urticarial eruption in COVID-19 infection. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e244–e245. [Google Scholar] [CrossRef] [Green Version]
- De Masson, A.; Bouaziz, J.D.; Sulimovic, L.; Cassius, C.; Jachiet, M.; Ionescu, M.A.; Rybojad, M.; Bagot, M.; Duong, T.A.; Denjean, D.; et al. Chilblains is a common cutaneous finding during the COVID-19 pandemic: A retrospective nationwide study from France. J. Am. Acad. Dermatol. 2020, 83, 667–670. [Google Scholar] [CrossRef]
- Duong, T.A.; Velter, C.; Rybojad, M.; Comte, C.; Bagot, M.; Sulimovic, L.; Bouaziz, J.D. Did Whatsapp® reveal a new cutaneous COVID-19 manifestation? J. Eur. Acad. Dermatol. Venereol. 2020, 34, e348–e350. [Google Scholar] [CrossRef] [PubMed]
- Roca-Ginés, J.; Torres-Navarro, I.; Sánchez-Arráez, J.; Abril-Pérez, C.; Sabalza-Baztán, O.; Pardo-Granell, S.; Martínez I Cózar, V.; Botella-Estrada, R.; Évole-Buselli, M. Assessment of Acute Acral Lesions in a Case Series of Children and Adolescents during the COVID-19 Pandemic. JAMA Dermatol. 2020, 156, 992–997. [Google Scholar] [CrossRef] [PubMed]
- Marzano, A.V.; Genovese, G.; Fabbrocini, G.; Pigatto, P.; Monfrecola, G.; Piraccini, B.M.; Veraldi, S.; Rubegni, P.; Cusini, M.; Caputo, V.; et al. Varicella-like exanthem as a specific COVID-19–associated skin manifestation: Multicenter case series of 22 patients. J. Am. Acad. Dermatol. 2020, 83, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Cao, W.; Xiao, M.; Li, Y.J.; Yang, Y.; Zhao, J.; Zhou, X.; Jiang, W.; Zhao, Y.Q.; Zhang, S.Y.; et al. Clinical and coagulation characteristics of 7 patients with critical COVID-2019 pneumonia and acro-ischemia. Zhonghua Xue Ye Xue Za Zhi 2020, 41, E006. [Google Scholar] [PubMed]
- Piccolo, V.; Neri, I.; Filippeschi, C.; Oranges, T.; Argenziano, G.; Battarra, V.C.; Berti, S.; Manunza, F.; Fortina, A.B.; Di Lernia, V.; et al. Chilblain-like lesions during COVID-19 epidemic: A preliminary study on 63 patients. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e291–e293. [Google Scholar] [CrossRef] [PubMed]
- Massey, P.R.; Jones, K.M. Going viral: A brief history of Chilblain-like skin lesions («COVID toes») amidst the COVID-19 pandemic. Semin. Oncol. 2020, 47, 330–334. [Google Scholar] [CrossRef] [PubMed]
- Jamshidi, P.; Hajikhani, B.; Mirsaeidi, M.; Vahidnezhad, H.; Dadashi, M.; Nasiri, M.J. Skin Manifestations in COVID-19 Patients: Are They Indicators for Disease Severity? A Systematic Review. Front. Med. 2021, 8, 634208. [Google Scholar] [CrossRef]
- Fernandez-Nieto, D.; Jimenez-Cauhe, J.; Suarez-Valle, A.; Moreno-Arrones, O.M.; Saceda-Corralo, D.; Arana-Raja, A.; Ortega-Quijano, D. Characterization of acute acral skin lesions in nonhospitalized patients: A case series of 132 patients during the COVID-19 outbreak. J. Am. Acad. Dermatol. 2020, 83, e61–e63. [Google Scholar] [CrossRef]
- Mazzotta, F.; Troccoli, T. Acute acro-ischemia in the child at the time of COVID-19. Eur. J. Pediatr. Dermatol. 2020, 30, 71–74. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Study Participants (n) | Average Age (Years) Men Women | Aim | Types of Skin Manifestations on the Foot | |
|---|---|---|---|---|
| Guan 2020 [17] | Cross-sectional study (n = 1099) | 47 M = 637 W = 462 | To describe the clinical characteristics of patients with COVID-19 | Not specified. Skin findings were missed on initial COVID-19. |
| Recalcati 2020 [18] | Case series study (n = 107) | 72 M = 58 W = 49 | To summarise perniosis-like dermatological lesions in young patients with COVID-19. | Acrocyanosis due to respiratory failure. Foot thrombosis. Maculo-papular lesions on feet and hands. 90% of the lesions were located on the fingers and toes and 81.8% were located on the feet. |
| Estébanez 2020 [19] | Report case (n = 1) | 28 M = 0 W = 1 | To describe a new skin manifestation on the heel of the foot caused by COVID-19. | Dermatological sign of confluent erythematous-yellowish papules on the heels. (COVID-19 positive). |
| Carrascosa 2020 [16] | - | - | To summarise the prevalence of dermatological manifestations associated with COVID-19. | Acral lesions, vesicular rashes, urticarial rashes, maculopapular rashes, and livedoid/necrotic lesions. |
| Lu 2020 [13] | Case series study (n = 3) | M = 2 W = 1 | To report clinical features on the foot in a quasi-symptomatic patient. | Urticaria on the lower extremities, with no other symptoms associated with COVID-19. |
| Henry 2020 [20] | Report case (n = 1) | 27 M = 0 W = 1 | To report a case of onset of urticarial rash before the onset of fever or respiratory symptom after diagnosis of COVID-19. | Pruritic rash of disseminated erythematous plaques with facial and acral involvement. |
| Masson 2020 [21] | Retrospective cross-sectional study (n = 277) | 27 M = 114 W = 113 | To analyse the dermatological manifestations associated with COVID-19. | Urticaria (n = 26); vesicular lesion (n = 41); acral lesion (n = 142); morbilliform lesion (n = 25); petechiae (n = 7); livedo. Reticularis (n= 4); and other types of dermatological lesions (n = 41); acral lesions in 28%. |
| Fernández-Nieto 2020 [15] | Narrative review (n = 132) | - | To analyse and observe the predominance of dermatological lesions on the foot and hand. | Two different patterns of acral lesions; chilblains (72%) and erythema multiforme-like pattern. Acral lesions are predominantly on the toes and are rarely seen in other areas of the body. |
| Galván-Casas 2020 [15] | Prospective study (N = 375) | M = 153 W = 222 | To describe the cutaneous manifestations of COVID-19 disease and relate them to other clinical findings. | Chilblains = 19%, urticarial lesions = 19% and maculopapular lesions = 47%, necrosis = 6%. |
| Duong 2020 [22] | Retrospective study (N = 219) | - | To establish the prevalence of dermatological lesions on the foot. | Chilblains are predominant as a dermatological sign in patients diagnosed with COVID-19. |
| Roca-Gines 2020 [23] | Case series study (N = 20) | 1–18 M = 13 W = 7 | To report skin lesions as possible symptoms of COVID-19 infection. | Dermatological lesions on hands and feet, being more predominant on the foot. Acral erythema = 30%, dactylitis = 20% maculopapular lesions = 35% and mixed pattern = 15%. |
| Marzano 2020 [24] | Multicentre case series study (n = 22) | 60 M = 16 W = 6 | To define the cutaneous manifestations of COVID-19. | Scattered papulovesicular lesions, with different symptoms and not predominantly on the foot but present on the trunk. |
| Zhang 2020 [25] | Case series study (N = 7) | 59 M = 4 W = 3 | To investigate the clinical and coagulation characteristics of patients with coronavirus critical illness 2019 (COVID-19) with acroischemia in the intensive care unit. | Acroischemia accompanied by cyanosis of the toes. |
| Piccolo 2020 [26] | Case series study (N = 63) | 14 M = 27 W = 36 | To report preliminary results on dermatological lesions in children. | Lesions on feet = 85.7%, and on feet and hands together = 7%. Foot lesions are predominant in children with suspected SARS-CoV-2 infection. |
| Massey 2020 [27] | Narrative review (n = 566) | - | To review the literature on chilblain-like skin lesions in the early stages of the global COVID-19 pandemic. | A multitude of chilblain-like skin manifestations on the foot by COVID-19. |
| Jamshidi 2021 [28] | Narrative review (n= 1847) | - | To assess the temporal relationship between different types of skin lesions and the severity of COVID-19. | Cutaneous manifestations = 5.95%. Patients with vascular lesions had the highest mortality rate. |
| Jiménez-Cebrian 2021 [9] | Review of reviews (n = 10) | - | To review the literature on the clinical manifestations of COVID-19 in the foot. | The most relevant manifestations were Kawasaki disease, acral perniosis lesions, pernio erythema and ischaemia, and necrosis. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palomo-Toucedo, I.C.; López-Sánchez, M.J.; Reina-Bueno, M.; Coheña-Jiménez, M. Cutaneous Manifestations of COVID-19 in the Lower Limbs: A Narrative Review. Int. J. Environ. Res. Public Health 2022, 19, 8861. https://doi.org/10.3390/ijerph19148861
Palomo-Toucedo IC, López-Sánchez MJ, Reina-Bueno M, Coheña-Jiménez M. Cutaneous Manifestations of COVID-19 in the Lower Limbs: A Narrative Review. International Journal of Environmental Research and Public Health. 2022; 19(14):8861. https://doi.org/10.3390/ijerph19148861
Chicago/Turabian StylePalomo-Toucedo, Inmaculada C., Manuel Jesús López-Sánchez, María Reina-Bueno, and Manuel Coheña-Jiménez. 2022. "Cutaneous Manifestations of COVID-19 in the Lower Limbs: A Narrative Review" International Journal of Environmental Research and Public Health 19, no. 14: 8861. https://doi.org/10.3390/ijerph19148861
APA StylePalomo-Toucedo, I. C., López-Sánchez, M. J., Reina-Bueno, M., & Coheña-Jiménez, M. (2022). Cutaneous Manifestations of COVID-19 in the Lower Limbs: A Narrative Review. International Journal of Environmental Research and Public Health, 19(14), 8861. https://doi.org/10.3390/ijerph19148861