
NBI and Laryngeal Papillomatosis: A Diagnostic Challenge: A Systematic Review


Abstract
:Highlights
- ▪
- Laryngeal papillomatosis (LP) is considered a benign lesion, caused by HPV low-risk subtypes 6 and 11.
- ▪
- Narrow-band imaging (NBI) endoscopy is a useful diagnostic tool for distinguishing between benign and malignant laryngeal lesions.
- ▪
- Laryngeal squamous cell carcinoma (LSCC) and LP show the same type V pattern according to Ni classification on NBI.
- ▪
- Epithelial surface and clinical features of LP should be researched to determine a correct differential diagnosis between LP and LSCC.
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Methodology
2.2. Eligibility Criteria
2.3. Data Analysis
3. Results
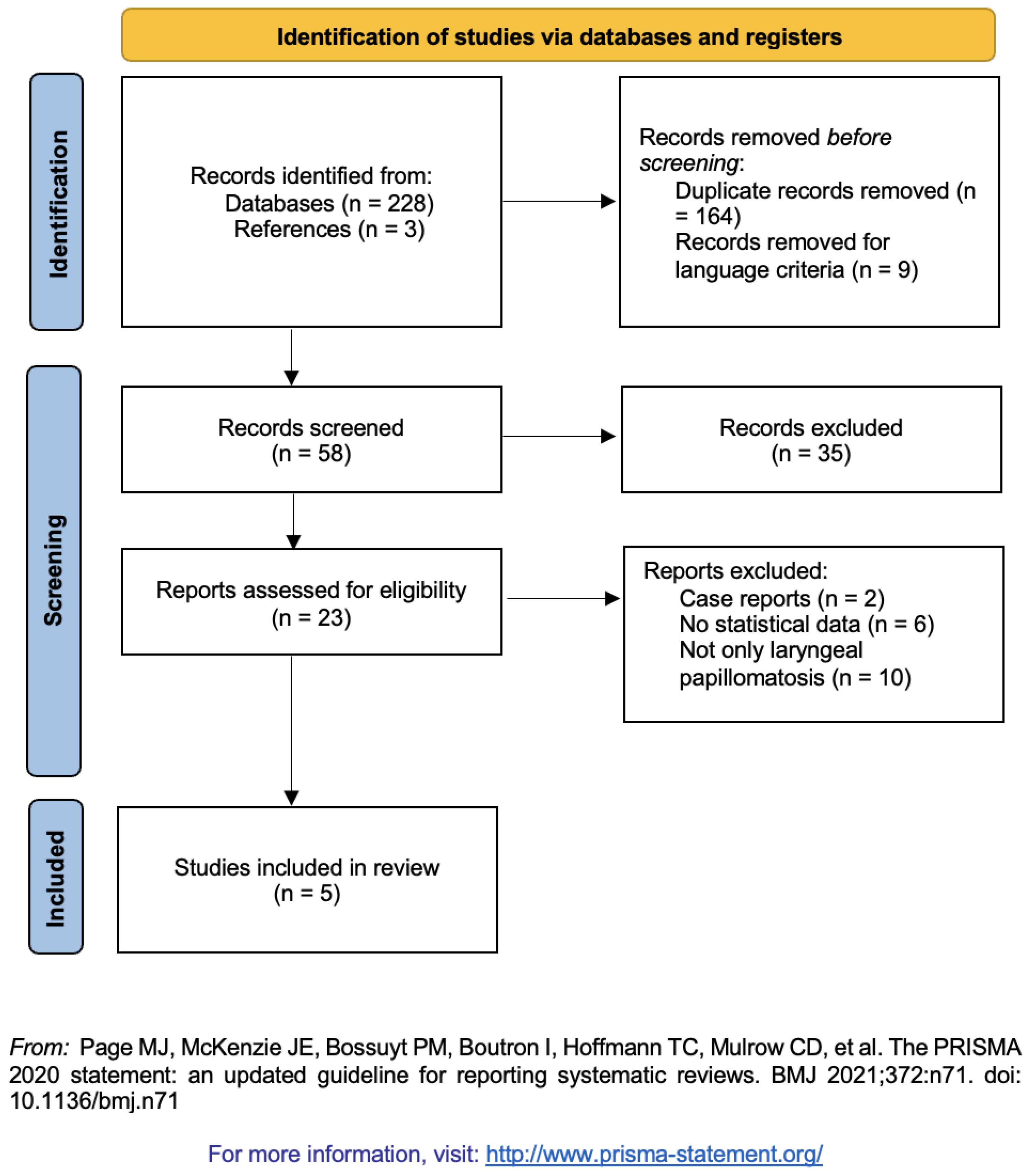
3.1. Study Selection
3.2. Laryngeal Papillomatosis vs. Laryngeal Squamous Cell Carcinoma
3.3. Laryngeal Papillomatosis: WLE vs. NBI
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, H.-T.; Baizhumanova, A.S. Is recurrent respiratory papillomatosis a manageable or curable disease? Laryngoscope 2015, 126, 1359–1364. [Google Scholar] [CrossRef]
- Ballestas, S.A.; Shelly, S.; Soriano, R.M.; Klein, A. Tendencias en el tratamiento de la papilomatosis respiratoria recurrente. Acta Otorrinolaringol. Esp. 2021, 72, 109–120. [Google Scholar] [CrossRef]
- Benedict, P.A.; Ruiz, R.; Yoo, M.; Verma, A.; Ahmed, O.H.; Wang, B.; Dion, G.; Voigt, A.; Merati, A.; Rosen, C.A.; et al. Laryngeal distribution of recurrent respiratory papillomatosis in a previously untreated cohort. Laryngoscope 2017, 128, 138–143. [Google Scholar] [CrossRef]
- Piazza, C.; Del Bon, F.; Peretti, G.; Nicolai, P. Narrow band imaging in endoscopic evaluation of the larynx. Curr. Opin. Otolaryngol. Head Neck Surg. 2012, 20, 472–476. [Google Scholar] [CrossRef]
- Ni, X.-G.; He, S.; Xu, Z.-G.; Gao, L.; Lu, N.; Yuan, Z.; Lai, S.-Q.; Zhang, Y.-M.; Yi, J.-L.; Wang, X.-L.; et al. Endoscopic diagnosis of laryngeal cancer and precancerous lesions by narrow band imaging. J. Laryngol. Otol. 2010, 125, 288–296. [Google Scholar] [CrossRef]
- Saraniti, C.; Chianetta, E.; Greco, G.; Lazim, N.M.; Verro, B. The Impact of Narrow-band Imaging on the Pre- and Intra- operative Assessments of Neoplastic and Preneoplastic Laryngeal Lesions. A Systematic Review. Int. Arch. Otorhinolaryngol. 2020, 25, e471–e478. [Google Scholar] [CrossRef]
- Lukeš, P.; Zabrodsky, M.; Lukesova, E.; Chovanec, M.; Astl, J.; Betka, J.A.; Plzák, J. The Role of NBI HDTV Magnifying Endoscopy in the Prehistologic Diagnosis of Laryngeal Papillomatosis and Spinocellular Cancer. BioMed Res. Int. 2014, 2014, 285486. [Google Scholar] [CrossRef]
- Imundić, A.M. Measures of Diagnostic Accuracy: Basic Definitions. EJIFCC 2009, 19, 203–211. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 88, 105906. [Google Scholar] [CrossRef]
- Lin, C.; Zhang, S.; Lu, L.; Wang, M.; Qian, X. Diagnostic Value and Pathological Correlation of Narrow Band Imaging Classification in Laryngeal Lesions. Ear Nose Throat J. 2020, 100, 737–741. [Google Scholar] [CrossRef]
- Gi, R.E.A.T.P.; Halmos, G.B.; van Hemel, B.M.; Msc, E.R.V.D.H.; Van Der Laan, B.F.A.M.; Plaat, B.E.C.; Dikkers, F.G. Narrow band imaging is a new technique in visualization of recurrent respiratory papillomatosis. Laryngoscope 2012, 122, 1826–1830. [Google Scholar] [CrossRef]
- Valls-Mateus, M.; Nogués-Sabaté, A.; Blanch, J.L.; Bernal-Sprekelsen, M.; Avilés-Jurado, F.X.; Vilaseca, I. Narrow band imaging for head and neck malignancies: Lessons learned from mistakes. Head Neck 2018, 40, 1164–1173. [Google Scholar] [CrossRef]
- Zwakenberg, M.A.; Dikkers, F.G.; Wedman, J.; Van Der Laan, B.F.A.M.; Halmos, G.B.; Plaat, B.E.C. Detection of high-grade dysplasia, carcinoma in situ and squamous cell carcinoma in the upper aerodigestive tract: Recommendations for optimal use and interpretation of narrow-band imaging. Clin. Otolaryngol. 2018, 44, 39–46. [Google Scholar] [CrossRef]
- Šifrer, R.; Šereg-Bahar, M.; Gale, N.; Hočevar-Boltežar, I. The diagnostic value of perpendicular vascular patterns of vocal cords defined by narrow-band imaging. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 1715–1723. [Google Scholar] [CrossRef]
- Kraft, M.; Fostiropoulos, K.; Gürtler, N.; Arnoux, A.; Davaris, N.; Arens, C. Value of narrow band imaging in the early diagnosis of laryngeal cancer. Head Neck 2014, 38, 15–20. [Google Scholar] [CrossRef]
- Cosway, B.; Drinnan, M.; Paleri, V. Narrow band imaging for the diagnosis of head and neck squamous cell carcinoma: A systematic review. Head Neck 2016, 38, E2358–E2367. [Google Scholar] [CrossRef]
- Saraniti, C.; Greco, G.; Verro, B.; Lazim, N.M.; Chianetta, E. Impact of Narrow Band Imaging in Pre-Operative Assessment of Suspicious Oral Cavity Lesions: A Systematic Review. Iran. J. Otorhinolaryngol. 2021, 33, 127–135. [Google Scholar] [CrossRef]
- Wen, Y.-H.; Zhu, X.-L.; Lei, W.-B.; Zeng, Y.-H.; Sun, Y.-Q.; Wen, W.-P. Narrow-Band ImagingA Novel Screening Tool for Early Nasopharyngeal Carcinoma. Arch. Otolaryngol. Head Neck Surg. 2012, 138, 183–188. [Google Scholar] [CrossRef]
- Karatayli-Ozgursoy, S.; Bishop, J.A.; Hillel, A.; Akst, L.; Best, S.R. Risk Factors for Dysplasia in Recurrent Respiratory Papillomatosis in an Adult and Pediatric Population. Ann. Otol. Rhinol. Laryngol. 2015, 125, 235–241. [Google Scholar] [CrossRef]
- Orita, Y.; Gion, Y.; Tachibana, T.; Ikegami, K.; Marunaka, H.; Makihara, S.; Yamashita, Y.; Miki, K.; Makino, T.; Akisada, N.; et al. Laryngeal squamous cell papilloma is highly associated with human papillomavirus. Jpn. J. Clin. Oncol. 2018, 48, 350–355. [Google Scholar] [CrossRef]
- Bolontrade, M.; Stern, M.C.; Binder, R.L.; Zenklusen, J.C.; Gimenez-Conti, I.B.; Conti, C.J. Angiogenesis is an early event in the development of chemically induced skin tumors. Carcinogenesis 1998, 19, 2107–2113. [Google Scholar] [CrossRef] [Green Version]
- Gi, R.E.A.T.P.; Giorgi, M.R.M.S.; Slagter-Menkema, L.; van Hemel, B.M.; Van Der Laan, B.F.A.M.; Heuvel, E.R.V.D.; Dikkers, F.G.; Schuuring, E.M. Clinical course of recurrent respiratory papillomatosis: Comparison between aggressiveness of human papillomavirus-6 and human papillomavirus-11. Head Neck 2014, 37, 1625–1632. [Google Scholar] [CrossRef]
- Arens, C.; Betz, C.; Kraft, M.; Voigt-Zimmermann, S. Narrow band imaging for early diagnosis of epithelial dysplasia and microinvasive tumors in the upper aerodigestive tract. HNO 2016, 65, 5–12. [Google Scholar] [CrossRef]
- Arens, C.; Piazza, C.; Andrea, M.; Dikkers, F.G.; Gi, R.E.A.T.P.; Voigt-Zimmermann, S.; Peretti, G. Proposal for a descriptive guideline of vascular changes in lesions of the vocal folds by the committee on endoscopic laryngeal imaging of the European Laryngological Society. Eur. Arch. Oto-Rhino-Laryngol. 2015, 273, 1207–1214. [Google Scholar] [CrossRef] [PubMed]
- Šifrer, R.; Rijken, J.A.; Leemans, C.R.; Eerenstein, S.E.J.; van Weert, S.; Hendrickx, J.-J.; Bloemena, E.; Heuveling, D.A.; Rinkel, R.N.P.M. Evaluation of vascular features of vocal cords proposed by the European Laryngological Society. Eur. Arch. Oto-Rhino-Laryngol. 2017, 275, 147–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piazza, C.; Cocco, D.; Del Bon, F.; Mangili, S.; Nicolai, P.; Majorana, A.; Villaret, A.B.; Peretti, G. Narrow band imaging and high definition television in evaluation of oral and oropharyngeal squamous cell cancer: A prospective study. Oral Oncol. 2010, 46, 307–310. [Google Scholar] [CrossRef]
- Talari, K.; Goyal, M. Retrospective Studies—Utility and Caveats. J. R. Coll. Phys. Edinb. 2020, 50, 398–402. [Google Scholar] [CrossRef]

{kind=link}
| Keywords | PubMed | Scopus | Web of Science |
|---|---|---|---|
| Papillomatosis and NBI | 28 | 21 | 16 |
| Papillomatosis and Narrow-Band Imaging | 35 | 35 | 19 |
| Laryngeal papilloma and NBI | 13 | 13 | 8 |
| Laryngeal papilloma and Narrow-Band Imaging | 15 | 17 | 8 |
| Authors | Lukes P et al. [7] | Lin C et al. [10] | Tjon Pian Gi RE et al. [11] | Valls-Mateus M et al. [12] | Zwakenberg MA et al. [13] |
|---|---|---|---|---|---|
| Year of publication | 2014 | 2021 | 2012 | 2018 | 2019 |
| Study design | Not clear | Not clear | Prospective | Retrospective | Retrospective |
| N° lesions | 109 | 123 | 86 | 41 | 178 |
| Ni classification [5] | Type V | Types Va-Vb | Type V | Type V | Types Va-Vb |
| Sensitivity | 94% (LP) 100% (LSCC) | 41.67% (LP) 93.51% (LSCC) | 97% (NBI) 80% (WLE) | / | 92% (LP + LSCC) 92 (LSCC) |
| Specificity | 100% (LP) 82% (LSCC) | 92.93% (LP) 65.22% (LSCC) | 28% (NBI) 32% (WLE) | / | 68% (LP + LSCC) 88% (LSCC) |
| Accuracy NBI | / | / | / | 95.32% (LP) 88.71% (LSCC) | 77% (LP + LSCC) 84% (LSCC) |
| Accuracy WLE | / | / | / | 82.92% (LP) 79.4% (LSCC) | / |
| Positive predictive value | / | 52.82% (LP) 91.14% (LSCC) | / | / | 61% (LP + LSCC) 73% (LSCC) |
| Negative predictive value | / | 86.79% (LP) 68.18% (LSCC) | / | / | 94% (LP + LSCC) 94% (LSCC) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saraniti, C.; Gallina, S.; Verro, B. NBI and Laryngeal Papillomatosis: A Diagnostic Challenge: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 8716. https://doi.org/10.3390/ijerph19148716
Saraniti C, Gallina S, Verro B. NBI and Laryngeal Papillomatosis: A Diagnostic Challenge: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(14):8716. https://doi.org/10.3390/ijerph19148716
Chicago/Turabian StyleSaraniti, Carmelo, Salvatore Gallina, and Barbara Verro. 2022. "NBI and Laryngeal Papillomatosis: A Diagnostic Challenge: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 14: 8716. https://doi.org/10.3390/ijerph19148716
APA StyleSaraniti, C., Gallina, S., & Verro, B. (2022). NBI and Laryngeal Papillomatosis: A Diagnostic Challenge: A Systematic Review. International Journal of Environmental Research and Public Health, 19(14), 8716. https://doi.org/10.3390/ijerph19148716