
Accidents, Injuries, and Safety among Artisanal and Small-Scale Gold Miners in Zimbabwe

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. The Administered Questionnaire
2.3. Data Analysis
2.4. Ethical Approval
3. Results
3.1. Socio-Demographic Characteristics
3.2. Reported Occupational Safety and Health (OSH)
Observed Safety Practices (Observed by Chance during the Survey)
3.3. Reported Accidents
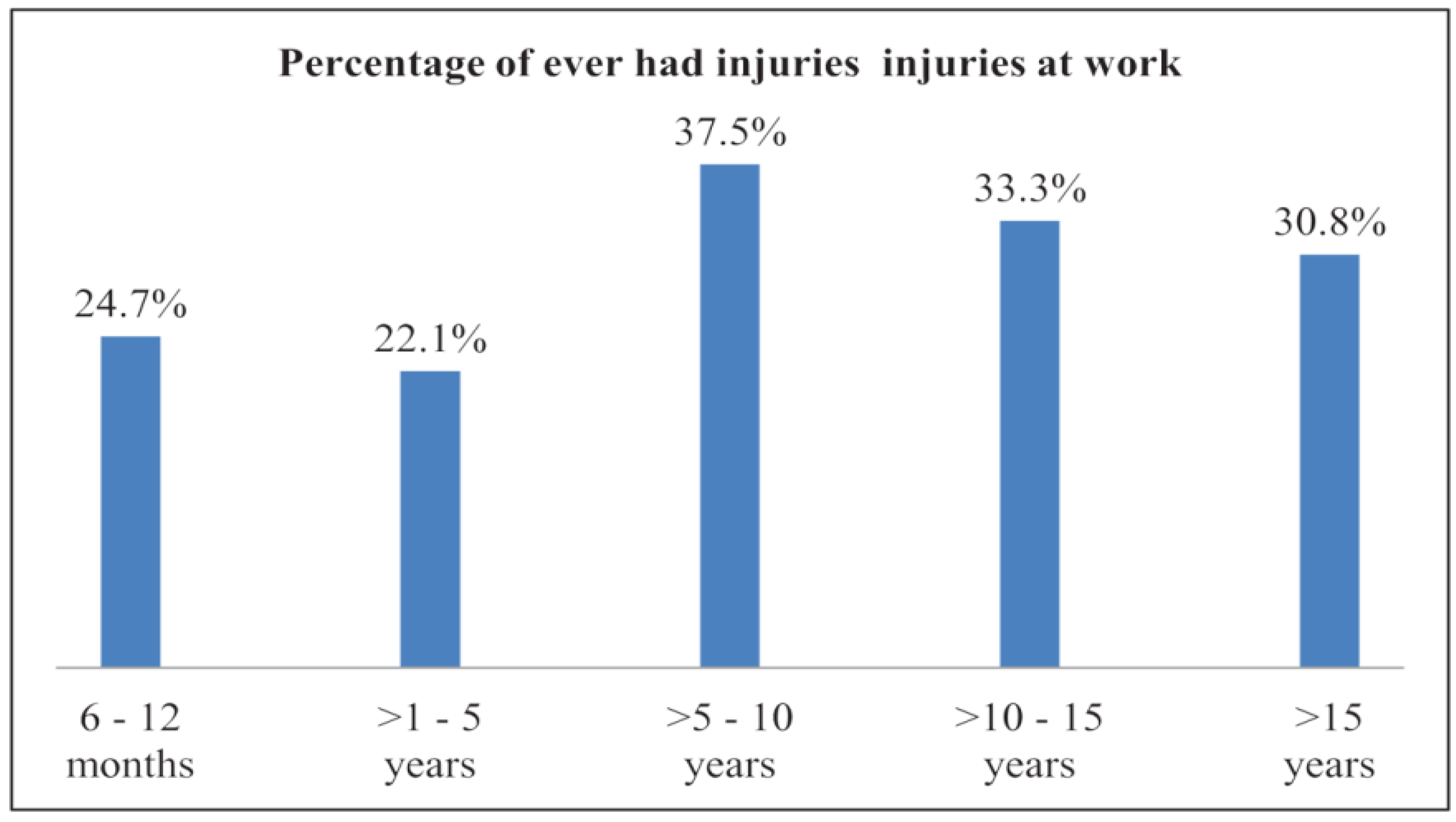
3.4. Reported Injuries
3.5. Risk Factors
3.6. Association between Ever-Had Injuries at Work and Exposure to Risk Factors
4. Discussion
Limitations and Strengths
5. Conclusions
Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Section 1: General Worker Information | |
| 1. Gender | 1 Female 2 Male |
| 2. Age | 1 18–35 2 36–50 3 >50 777 Other Specify __________ 999 Refuse to answer |
| 3. Highest level of education | 1 No formal school 2 Primary 3 Secondary 4 Tertiary 5 Vocational 777 Other Specify _______________ 999 Refuse to answer |
| 4. Knowledge and competence of your work in artisanal mining | 1 Low 2 Average 3 High 777 Other Specify________ 888 Don’t Know 999 Refuse to answer |
| 5. Marital status | 1 Single 2 Married 3 Separated 4Divorced 5 Widowed 999 Refuse to answer |
| 6. Household size (Number of people staying within your family) | 1 1 2 2–5 3 More than 5 777 Other, Specify _______________ 999 Refuse to answer |
| 7. Which assets have you owned through ASGM | 1 Television 2 Car 3 Radio 4 Bicycle 5 Smart phone 6 House 777 Other, Specify ____ 999 Refuse to answer |
| 8. Monthly household income | 1 100 USD and less 2 100–500 USD 3 500 USD-1000 USD 777 Other, Specify _______ 789 N/A 888 Don’t Know 999 Refuse to answer |
| 9. Have you moved and worked in different mining sites in the past 6 months | 0 No 1 Yes 789 N/A 999 Refuse to answer If yes, please indicate why.......................................................................... |
| 10. Which department do you work in? | 1 Digging 2 Blaster Blasting Licence 0 No 1 Yes 777 Other, Specify _______ 3 Lashing 4 Washing 5 Carrying/moving mined ore to the surface 6 Loading/off when transporting ore to the stamp mill 7 Sponsor 8Manager/Supervisor/Gang leader 9 Working at the Stamp Mill 10 Mine Owner 11 Amalgam burning 12Cooking 13Carrying ore manually to the stamp mill 14 Gold buying 777 Other, specify _____ 888 Don’t Know 999 Refuse to answer 789 N/A
|
| 11. How long have you worked in artisanal and small scale gold mining? | 1 1–5 years 2 6–10 years 3 11–15 years 4 >15 789 N/A 666 Don’t Remember 999 Refuse to answer |
| 12(a). Do you know of HIV/AIDS test center close to your work place | 0 No 1Yes 789 N/A 888 Don’t Know 999 Refuse to answer (b) Have you ever taken HIV test? 0 No 1 Yes 789 N/A 888 Don’t Know 999 Refused to answer (c) If yes and you are comfortable, may you share your status? 0 Negative 1 Positive 789 N/A 888 Don’t Know 1010 Uncomfortable to answer |
| 13(a). Have you ever experienced any health problems, became sick or got injured because of mining activities? | 0 No 1 Yes (b) If yes, please specify, 1 Respiratory problem 2 Memory problems 3 Skin problems 4 Reproductive problems 5 Hearing problems 6 Musculoskeletal Problems 7 Kidney problem 8 Sight problems 9 Digestive problems 10Stress 11 Injury 777 Other Specify ______ 789 N/A 888 Don’t Know 999 Refuse to answer |
| 14. How would you rate your health today from 1 to 100? 1 is the worst 100 is the best health state______ | |
| Section 2 Occupational Safety | |
| 15. Who is responsible for safety on your site | 1 Mine Owner (on site) 2 Supervisor 3 Gang leader 4 Employee 777 Other Specify__________ 789 N/A 888 Don’t Know 999 Refuse to answer |
| 16(a). Have you ever had safety issues at your workplace | 0 No 1 Yes (b) If yes, in which department/area? 1 Going down to the mine/returning to the ground 2 Excavation 3 Blasting 4 Lashing 5 Crushing 6 Removal of ore from shafts 7 Milling 8 Sluicing 9 Loading, carrying of ore to the mill and off loading 10 Amalgam burning 11 Delivery and selling of gold 12 Acquisition and delivery of equipment and chemicals 13 Storage of equipment and chemicals 14 Disposal of waste 777 Other, specify _________ 789 N/A 666 Don’t Remember 999 Refuse to answer (c) What was the safety issue? 1 Slipping /tripping/ falling 2 Hit by working tools/machines 3 Instant death 4 Hit by pieces of stone 5 Breaking rope (hoist) 6 Collapsing 7 Mine shaft collapse 8 Failing to breath 9 Trapped underground 999 Refuse to answer 777 Other, Specify_______________ 789 N/A 888 Don’t Know |
| 17. When an accident occurs at work how is it handled? | 1 Reported to area chief 2 Reported to County Director of Mines 3 Reported to Country Commissioner 4Not reported 5 Reported to the hospital 777 Other Specify_______________ 789 N/A 888 Don’t Know 999 Refuse to answer |
| 18. What actions are normally taken after an accident? | 1 Investigation into the cause 2 Temporary Mine closure 3 None 777 Other, specify _______________ 789 N/A 888 Don’t Know 999 Refuse to answer |
| 19(a). Have you ever been injured in the course of your work? | 0 No 1 Yes (b) If yes, what was the type of injury? 1 Cuts 2 Fractures 3 Bruises 4 Back/Chest injuries 777 Other, specify__________ 789 N/A 666 Don’t Remember 999 Refuse to answer |
| 20(a). What was the cause of the injury? | 1 Struck/hit by rock 2 Sharp (rock) edges 3 Fall 4 Vibration 5 Working tools/Machinery 6 Lifting heavy load 7 Awkward posture 777 Other, specify ________ 789 N/A 888 Don’t Know 999 Refuse to answer (b) Which part of your body was injured 1 Head 2 Legs 3 knee 4Feet 5 Back 6 Chest 7 Hand 8 Palm 777 Other, specify_______________ N/A 888 Don’t Know 999 Refuse to answer (c) Do you have access to compensation 0 No 1 Yes 789 N/A 888 Don’t Know 999 Refuse to answer 777 Other, Specify_______________ (d) Do you have access to health care insurance 0 No 1 Yes 789 N/A 888 Don’t Know 999 Refuse to answer 777 Other, Specify_______________ |
| 21(a). Have you ever heard about workplace safety and health? | No 0 1Yes (b) If yes, where did you get the information? 1 Fellow miner 2 Mine Site Manager 3 Radio/TV 4 Friend/Family 5 Social media (Facebook/Twitter) 6 Newspaper/Magazine 7 Training 789 N/A 777 Other, specify________ 666 Don’t Remember 999 Refuse to answer |
| 22(a). Do you use personal protective equipment (PPE) when working? | No 0 1 Yes (b) If yes, which PPE? 1 Helmets 2 Protective footwear 3 Protective glasses /face masks 4 Protective clothing(jackets) 5 Ear protection 6 Dust mask 7 Respirators 8 Protective belt 9 Sunhat 10 Raincoats 777 Other, specify _______________ 789 N/A 999 Refuse to answer (c) How did you get the PPE? 1 Provided by site manager 2 Bought for myself 3 Given by co-worker 4 Given by a friend/family 777 Other, Specify___________ 789 N/A 999 Refuse to answer (d) How often do you replace your PPE (dust masks, ear plugs, etc.)? 1 Frequently 2 Rarely 3 Never 789 N/A 999 Refuse to answer (e) What are the common reasons for not using Personal Protective Equipment? 1 Not provided 2 Not required 3 Not comfortable 4 Not affordable 5 Not aware of their importance 789 N/A 888 Don’t Know 777 Other, specify_______________ 999 Refuse to answer |
| 23. Have you ever experienced a case(s) of violence related to your work? | 0 No 1 Yes 888 Don’t Remember If yes, what kind of violence 1 People taking over shafts by force 2 Raiding of ore, gold, equipment etc. 3 Physical attacks 4 Fights at work 5 Gender based violence 777 Other [Specify] ___________________________________________ |
| 23(a). Have you ever been trained on OSH and/or first aid? | OSH 0 No 1 Yes First Aid 0 No 1 Yes (b) If yes, who was the trainer? 1 Mine/Site Manager(supervisor) 2 Safety expert 3 Workmate 4 NGO 777 Other, Specify_______________ 789 N/A 999 Refuse to answer |
| 24. Which services do you have access to | 1 Occupational Safety and Health training 2 Financial support 3 Mining services 4 Shops with PPE 5 Health Care 6 Social security 7 Emergency Services 8 Competitive gold markets 9 Schools 10 Partnerships/Associations 11 Communication Specify Telephone Radio Television 9 Newspaper Social Media Community Gatherings 777 Other services, Specify_______ 789 N/A 888 Don’t Know 999 Refuse to answer |
| 25. What do you consider the priority safety and health issues at your work place? | 1 Dust 2 Noise 3 Flooding 4 Injuries/accidents 5 Hot confined shaft 6 Workplace Violence 7Muscle and back pain 8 Explosive fumes 9 TB 10HIV 11Mercury burning 12Malaria 13Snakes 14 Hunger 15 Diarrheal diseases 16 Heat Stress 17 Cyanide 777 Other, Specify _____ 789 N/A 888 Don’t Know 999 Refuse to answer |
| Section 3. Standard Operating Procedures | |
| 26. Do you have specific ways of working safe before during or after when performing activities like entering the mining pit, drilling, working with explosives lashing after blasting with explosives, manual lifting or carrying heavy loads, burning amalgam, milling or tanks/ cyanidation | 0 No 1 Yes 888 Don’t Know If yes, please list them here_____________________________________________ ___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________ __________________________________________________________________ ___________________________________________________________________ |
| Section 4. Gendered Challenges | |
| 27. Would you indicate roles for men and women in the following activities Male Female Both | Prospecting (prospector/sampler) Male Female Both Digging Male Female Both Drilling Male Female Both Blasting Male Female Both Lashing Male Female Both Transportation of ore Male Female Both Crushing Male Female Both Milling Male Female Both Sluicing Male Female Both Washing/Panning Male Female Both Amalgamation Male Female Both Cyanidation Male Female Both |
| 28. Are there workplace challenges/difficulties common for men or women at your work? | Men 0 No 1 Yes Women 0 No 1 Yes If yes, please specify: Men_____________________________________________ ______________________________________________________________________________________________________________________________________ If yes, please specify: Women ____________ |
References
- Steckling, N.; Tobollik, M.; Plass, D.; Hornberg, C.; Ericson, B.; Fuller, R.; Bose-O’Reilly, S. Global burden of disease of mercury used in artisanal small-scale gold mining. Ann. Glob. Health 2017, 83, 234–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mkodzongi, G.; Spiegel, S. Artisanal gold mining and farming: Livelihood linkages and labour dynamics after land reforms in Zimbabwe. J. Dev. Stud. 2019, 55, 2145–2161. [Google Scholar] [CrossRef] [Green Version]
- National Social Security Authority. 2019 Annual Statistics Report; Government of Zimbabwe (GoZ): Harare, Zimbabwe, 2019. Available online: https://www.nssa.org.zw/downloads/ (accessed on 15 December 2021).
- Seccatore, J.; Veiga, M.; Origliasso, C.; Marin, T.; De Tomi, G. An estimation of the artisanal small-scale production of gold in the world. Sci. Total Environ. 2014, 496, 662–667. [Google Scholar] [CrossRef] [PubMed]
- Hentschel, T.; Hruschka, F.; Priester, M. Artisanal and Small-Scale Mining: Challenges and Opportunities; International Institute for Environment and Development: London, UK, 2003; Available online: https://pubs.iied.org/sites/default/files/pdfs/migrate/9268IIED.pdf? (accessed on 20 April 2020).
- International Labour Organisation. Mining: A Hazardous Work; International Labour Office: Geneva, Switzerland, 2015. [Google Scholar]
- World Bank. 2020 State of the Artisanal and Small-Scale Mining Sector; World Bank: Washington, DC, USA, 2020; Available online: https://delvedatabase.org/uploads/resources/Delve-2020-State-of-the-Sector-Report-0504.pdf (accessed on 5 May 2021).
- Elenge, M.; Leveque, A.; De Brouwer, C. Occupational accidents in artisanal mining in Katanga, DRC. Int. J. Occup. Med. Environ. Health 2013, 26, 265–274. [Google Scholar] [CrossRef]
- Long, R.N.; Sun, K.; Neitzel, R.L. Injury risk factors in a small-scale gold mining community in Ghana’s Upper East Region. Int. J. Environ. Res. Public Health 2015, 12, 8744–8761. [Google Scholar] [CrossRef] [Green Version]
- Kyeremateng-Amoah, E.; Clarke, E.E. Injuries among artisanal and small-scale gold miners in Ghana. Int. J. Environ. Res. Public Health 2015, 12, 10886–10896. [Google Scholar] [CrossRef]
- Becker, J.; Furu, P.; Singo, J.; Shoko, D.; Elbel, J.; Bose-O’Reilly, S.; Steckling-Muschack, N. Determinants of health and health needs assessment of artisanal and small-scale gold miners in Kadoma, Zimbabwe: A mixed method approach. Environ. Res. 2021, 197, 111081. [Google Scholar] [CrossRef]
- Singo, J.; Isunju, J.B.; Moyo, D.; Steckling-Muschack, N.; Bose-O’Reilly, S.; Mamuse, A. Hazards and control measures among artisanal and small-scale gold miners in Zimbabwe. Ann. Glob. Health 2022, 88, 21. [Google Scholar] [CrossRef]
- Abebil, F.; Tefera, Y.; Tefera, W.; Kumie, A.; Mulugeta, H.; Kassie, G. Nonfatal Occupational Injuries among Artisanal and Small-scale Gold Mining Workers in Ethiopia; Research Square: Durham, NC, USA, 2022. [Google Scholar] [CrossRef]
- Chimamise, C.; Gombe, N.T.; Tshimanga, M.; Chadambuka, A.; Shambira, G.; Chimusoro, A. Factors associated with severe occupational injuries at mining company in Zimbabwe, 2010: A cross-sectional study. Pan Afr. Med. J. 2013, 14. [Google Scholar] [CrossRef]
- Boese-O’Reilly, S.; Dahlmann, F.; Lettmeier, B.; Drasch, G. Removal of Barriers to the Introduction of Cleaner Artisanal Gold Mining and Extraction Technologie in Kadoma, Zimbabwe. Available online: https://iwlearn.net/resolveuid/886be3abb7f723d8653bf38e9e678e7b (accessed on 19 January 2022).
- Ajith, M.M.; Ghosh, A.K. Comparison of parameters for likelihood and severities of injuries in artisanal and small-scale mining (ASM). Saf. Sci. 2019, 118, 212–220. Available online: https://www.sciencedirect.com/science/article/abs/pii/S092575351831974X (accessed on 20 April 2022). [CrossRef]
- Chazingwa, L. Thirty Gold Panners Trapped, Feared Dead in Kadoma. Spotlight. 17 February 2021. Available online: https://spotlight.co.zw/thirty-gold-panners-trapped-feared-dead-in-kadoma/ (accessed on 16 May 2021).
- Janchiv, T.; Batseree, S. Mongolia Introduction to Mining: A Thematic Reference Book; Mining Rescue Service of Mongolia and Swiss Agency for Development and Cooperation (SDC): Ulaanbaatar, Mongolia, 2015; Available online: https://www.asmhub.mn/uploads/files/intromining-with-cover.pdf (accessed on 7 April 2022).
- Bansah, K.; Yalley, A.; Dumakor-Dupey, N. The hazardous nature of small scale underground mining in Ghana. J. Sustain. Min. 2016, 15, 8–25. [Google Scholar] [CrossRef] [Green Version]
- Nakua, E.K.; Owusu-Dabo, E.; Newton, S.; Koranteng, A.; Otupiri, E.; Donkor, P.; Mock, C. Injury rate and risk factors among small-scale gold miners in Ghana. BMC Public Health 2019, 19, 1368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reason, J. Human error: Models and management. BMJ 2000, 320, 768–770. [Google Scholar] [CrossRef] [Green Version]
- Griffin, S.C.; Bui, D.P.; Gowrisankaran, G.; Lutz, E.A.; He, C.; Hu, C.; Burgess, J.L. Risk management interventions to reduce injuries and maximize economic benefits in US mining. J. Occup. Environ. Med. 2018, 60, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Shalini, R.T. Economic cost of occupational accidents: Evidence from a small island economy. Saf. Sci. 2009, 47, 973–979. Available online: https://isiarticles.com/bundles/Article/pre/pdf/18143.pdf (accessed on 4 July 2021). [CrossRef]
- Wallace, K.; Prosser, B.; Stinnette, J.D. The practice of mine ventilation engineering. Int. J. Min. Sci. Technol. 2015, 25, 16. Available online: https://www.sciencedirect.com/science/article/abs/pii/S2095268615000099 (accessed on 7 April 2022). [CrossRef]
- Donoghue, A. Occupational health hazards in mining: An overview. Occup. Med. 2004, 54, 283–289. [Google Scholar] [CrossRef] [Green Version]
- The National Institute for Occupational Safety and Health (NIOSH). Hierarchy of Controls. 2015. Available online: https://www.cdc.gov/niosh/topics/hierarchy/ (accessed on 4 July 2021).
- Fogler, H.S. Process Safety across the Chemical Engineering Curriculum; University of Michigan: Ann Arbor, MI, USA, 2021; Available online: http://websites.umich.edu/~safeche/swiss_cheese.html (accessed on 4 July 2021).
- Bonsu, J.; Van Dyk, W.; FranzIDIs, J.; Petersen, F.; Isafiade, A. A systemic study of mining accident causality: An analysis of 91 mining accidents from a platinum mine in South Africa. J. South. Afr. Inst. Min. Metall. 2017, 117, 59–66. [Google Scholar] [CrossRef]
- Mensah, S.K.; Siabi, E.K.; Donkor, P.; Kurantin, N. Assessing the safety and health practices in the artisanal and small-scale gold mining sector of Ghana: A case of Ntotroso. Environ. Chall. 2022, 6, 100443. [Google Scholar] [CrossRef]
- Smith, N.M.; Ali, S.; Bofinger, C.; Collins, N. Human health and safety in artisanal and small-scale mining: An integrated approach to risk mitigation. J. Clean. Prod. 2016, 129, 43–52. [Google Scholar] [CrossRef]
- Elenge, M.M.; De Brouwer, C. Identification of hazards in the workplaces of artisanal mining in Katanga. Int. J. Occup. Med. Environ. Health 2011, 24, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Matsa, M.M.; Mazire, F.; Musasa, T.; Defe, R. Health and safety issues within artisanal and small-scale gold mining: A case for Penhalonga, Ward 21 Mutasa District, Zimbabwe. Afr. Geogr. Rev. 2022, 41, 93–107. [Google Scholar] [CrossRef]
- Grossel, S.S. Safety Management: Near Miss Identification, Recognition, and Investigation (2012) By Ron C, McKinnon, CRC Press, Boca Ration, FL, 197 pages, $99.95, ISBN: 978-1-4398–7946-7. Process Saf. Prog. 2013, 2, 224–225. Available online: https://www.academia.edu/37166448/Safety_Management_near_miss_identification_recognition_and_investigation_pdf (accessed on 10 May 2022). [CrossRef]
- Wright, L. Towards an empirical test of the iceberg model. Hum. Decis. Mak. Man. Control. EAM2000 EUR 2000, 19599, 145–152. [Google Scholar] [CrossRef]
- International Labour Organisation. Occupational Health and Safety Management System: A Tool for Continual Improvement; International Labour Office: Geneva, Switzerland, 2011; Available online: https://www.ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/---safework/documents/publication/wcms_153930.pdf (accessed on 4 July 2021).
- Government of Zimbabwe. Mining (Management and Safety) Regulations 1990 (SI 109 of 1990); Zimbabwean Government Gazette: Harare, Zimbabwe, 1990; pp. 605–784.
- Spiegel, S.J. Resource policies and small-scale gold mining in Zimbabwe. Resour. Policy 2009, 34, 39–44. Available online: https://www.sciencedirect.com/science/article/abs/pii/S030142070800072X (accessed on 10 May 2022). [CrossRef]
- Ncube, M. The Governance of Zimbabwe’s Artisanal and Small-Scale Gold Mining (ASGM) Sector: An Actor-Oriented Approach; Thesis Wageningen University and Research; Food Valley: Wageningen, The Netherlands, 2021; Available online: https://edepot.wur.nl/556671 (accessed on 10 May 2022).
- Dzimunya, N.; Mapamba, L.; Dembetembe, G.G.; Dzwiti, K.; Mukono, T. Formalization of a roadmap to maximize the contribution of artisanal and small-scale mining in Zimbabwe. In Proceedings of the ASGM Conference, Johannesburg, South Africa, 10–11 September 2018; Available online: https://ir.uz.ac.zw/handle/10646/3833 (accessed on 24 May 2021).
- Government of Zimbabwe, Environment Management Agency, United Nations Environment Program, Africa Institute. National Action Plan for Artisanal and Small-Scale Gold Mining Sector in Zimbabwe, in Accordance with the Minamata Convention on Mercury. 2019. Available online: https://www.mercuryconvention.org/Portals/11/documents/NAP/Zimbabwe-NAP-2019.pdf (accessed on 4 April 2021).
- Beth, A.A. Assessment of Occupational Safety Compliance in Small-Scale Gold Mines in Siaya County, Kenya. Thesis, University of Nairobi Environmental Planning and Management, Nairobi, Kenya. Available online: http://erepository.uonbi.ac.ke/bitstream/handle/11295/104630/BethAssessment%20Of%20Occupational%20Safety%20Compliance%20In%20SmallScale%20Gold%20Mines%20In%20Siaya%20County,%20Kenya..Pdf?sequence=1 (accessed on 12 November 2019).
- Bird, F.E.; Germain, G.L.; Clark, D. Loss Control Management: Practical Loss Control Leadership, Revised ed.; Det Norske Veritas: Katy, TX, USA, 1996. [Google Scholar]
- Swiss Agency for Development and Cooperation (SDC). Sustainable Artisanal Mining Project: Swiss Agency For Development And Cooperation In Mongolia... Facts. Project Name: Sdc’s Strategic Goal: The Third Sustainable Livelihoods; Swiss Agency for Development and Cooperation (SDC): Bern, Switzerland, 2017.
- Artisanal Gold Council. PlanetGold Mongolia. 2021. Available online: https://www.planetgold.org/promoting-health-and-safety-artisanal-and-small-scale-gold-mining (accessed on 10 May 2022).
- Pact. Training Handbook for Artisanal and Small-Scale Miners in Zimbabwe; Pact: Washington, DC, USA, 2019; Available online: https://www.pactworld.org/Training%20handbook%20for%20ASM%20in%20Zimbabwe (accessed on 16 November 2020).
- De Vaus, D.; de Vaus, D. Surveys in Social Research; Routledge: London, UK, 2013. [Google Scholar]
- Josephine, S. Health Challenges and Risk Factors in ASGM in Zimbabwe: 2020 Survey. Mendeley Data 2022, V1. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n (%) | Total | |
|---|---|---|---|
| Population per district | 401 (100) | 401 | |
| District n (%) | Kadoma | 220 (54.9) | |
| Shurugwi | 181(45.1) | 401 | |
| Mine category n (%) | Rudimentary | 78 (19.5) | |
| More mechanized | 323 (80.5) | 401 | |
| Sex n (%) | Female | 69 (17.2) | |
| Male | 332 (82.8) | 401 | |
| Marital status n (%) | Single | 126 (31.9) | |
| Married | 202 (51.1) | ||
| Separated | 17 (4.3) | ||
| Divorced | 28 (7.1) | ||
| Widowed | 22 (5.6) | 395 | |
| Age n (%) | 18–35 years | 212 (56.1) | |
| 36–50 years | 130 (34.4) | ||
| Above 50 years | 36 (9.5) | 378 | |
| Education level n (%) | No formal school | 28 (7.1) | |
| Primary | 59 (14.9) | ||
| Secondary | 241 (60.9) | ||
| Tertiary | 39 (9.8) | ||
| Vocational | 29 (7.3) | 396 | |
| Monthly Earnings n (%) | No Earnings | 7 (1.9) | |
| Less than $100 USD | 212 (56.7) | ||
| Above 100–500 USD | 13 (34.8) | ||
| Above 500–1000 USD | 24 (6.4) | ||
| Above 1000 USD | 1 (0.3) | 374 | |
| Roles n (% of cases) | Digging | 211 (65.3) | |
| Moving ore manually | 59 (18.3) | ||
| Blasting | 51 (15.8) | ||
| Loading | 44 (13.6) | ||
| Washing/panning | 33 (10) | ||
| Cooking | 26 (7.9) | ||
| Amalgam burning | 24 (7.3) | ||
| Milling | 24 (7.3) | ||
| Sponsoring | 22 (6.8) | ||
| Supervision | 22 (6.8) | ||
| Mine owner | 19 (5.9) | ||
| Gold buying | 14 (4.3) | 549 (Total cases) | |
| Daily working hours n (%) | 1–8 h | 259 (66.9) | |
| Above 8–16 h | 82 (21.2) | ||
| Above 16–24 h | 46 (11.9) | 387 | |
| Working underground n (%) | Working underground yes | 201(52.3) | 385 |
| Experience in ASGM n (%) | 6–12 months | 98 (26.7) | 367 |
| >1–5 years | 152 (41.4) | ||
| >5–10 years | 57 (15.5) | ||
| >10–15 years | 45 (12.3) | ||
| >15 years | 15(4.1) | ||
| Migration | 112 (27.9) | 394 | |
| Type of Accident | Number (N) | Percentage of Cases | Percentage of Injuries (N) |
|---|---|---|---|
| Slips, trips, and falls (STFs) | 43 | 40.2 | 52.6(20) |
| Hit by tools or machines | 23 | 21.4 | 40.9 (9) |
| Hit by pieces of stone | 28 | 26.2 | 50.0(13) |
| Breaking of winch rope | 12 | 11.2 | 54.5 (6) |
| Collapsing | 12 | 11.2 | 20.0 (2) |
| Mineshaft collapses | 16 | 15.0 | 53.3 (8) |
| Underground trappings | 06 | 5.6% | 80.0 (4) |
| Role | Total | Ever been Injured | Crude OR (95% CI) | p-Value | |
|---|---|---|---|---|---|
| Number | (%) † | ||||
| 370 | 103 | 25.7% | |||
| Digging | |||||
| Yes | 196 | 68 | 34.7 | 2.1 (1.3–3.4) | 0.02 ** |
| No | 174 | 35 | 20.1 | Reference | |
| Blasting | |||||
| Yes | 45 | 18 | 40.0 | 1.8 (0.9–3.6) | 0.05 ** |
| No | 325 | 85 | 26.2 | Reference | |
| Washing/Processing | |||||
| Yes | 30 | 10 | 33.3 | 1.3 (0.6–3.0) | 0.5 (ns) |
| No | 339 | 93 | 24.7 | Reference | |
| Moving ore Manually | |||||
| Yes | 55 | 27 | 49.1 | 3.0 (1.7–5.5) | <0.0001 ** |
| No | 315 | 76 | 24.1 | Reference | |
| Loading | |||||
| Yes | 38 | 18 | 47.4 | 2.6 (1.3–5.2) | 0.007 ** |
| No | 332 | 85 | 25.6 | Reference | |
| Sponsoring | |||||
| Yes | 18 | 6 | 33.3 | 1.3 (0.5–3.6) | 0.6 (ns) |
| No | 352 | 97 | 27.6 | Reference | |
| Manager/Supervisor/Gang leader | |||||
| Yes | 20 | 5 | 25.0 | 0.9 (0.3–2.4) | 0.7 (ns) |
| No | 350 | 98 | 28.0 | Reference | |
| Working at the Mill | |||||
| Yes | 22 | 8 | 36.4 | 1.5 (0.6–3.7) | 0.4 (ns) |
| No | 348 | 95 | 27.3 | Reference | |
| Mine Owner | |||||
| Yes | 15 | 4 | 26.7 | 0.9 (0.3–3) | 0.9 (ns) |
| No | 355 | 99 | 27.9 | Reference | |
| Amalgam Burning | |||||
| Yes | 20 | 7 | 35.0 | 1.4 (0.6–3.7) | 0.5 (ns) |
| No | 350 | 96 | 27.4 | Reference | |
| Cooking | |||||
| Yes | 22 | 5 | 22.7 | 0.8 (0.3–2.1) | 0.6 (ns) |
| No | 348 | 98 | 28.8 | Reference | |
| Gold Buying | |||||
| Yes | 13 | 5 | 27.5 | 1.7 (0.5–5.2) | 0.4 (ns) |
| No | 357 | 98 | 30.2 | Reference | |
| Characteristic | Total | Ever been Injured at Work | OR (95% CI) | AOR = (95% CI) | p-Value | |
|---|---|---|---|---|---|---|
| Number | (%) † | |||||
| 370 | 103 | (25.7) | ||||
| Sex (n = 370) | ||||||
| Male | 311 | 96 | (30.9) | 1.8 (1.02–3.3) ** | 4.3 (1.4–13.6) | 0.01 ** |
| Female | 59 | 7 | (11.5) | Reference | Reference | |
| Age (n = 349) | ||||||
| >50 | 31 | 5 | (16.1) | Reference | Reference | |
| 36–50 | 125 | 33 | (26.4) | 0.8(0.5–1.3) | 0.7(0.4–1.2) | 0.2 (ns) |
| 18–35 | 193 | 61 | (31.6) | 0.4(0.2–1.1) | 0.2 (0.07–0.9) | 0.03 ** |
| Shaft miners’ transportation (n = 356) | ||||||
| Yes | 38 | 22 | (57.9) | 4.5(2.3–9) ** | 4.9(2.1–11.2) | <0.001 ** |
| No | 318 | 74 | (23.3) | Reference | Reference | |
| Crushing (n = 356) | ||||||
| Yes | 21 | 14 | (66.7) | 6.1(2.4–16) ** | 9.4(2.6–34.0) | 0.001 ** |
| No | 335 | 82 | (24.5) | Reference | Reference | |
| Blasting (n = 356) | ||||||
| Yes | 17 | 10 | (58.8) | 4.2(1.6–11.3) ** | 9.2(2.6–33.0) | 0.001 ** |
| No | 339 | 86 | (25.4) | Reference | Reference | |
| Flying stone particles (n = 350) | ||||||
| Yes | 26 | 13 | (26.9) | 2.7(1.2–6.1) ** | 2.1(0.5–8.1) | 0.3 (ns) |
| No | 324 | 87 | (31.7) | Reference | Reference | |
| Removing ore from the shaft (n = 356) | ||||||
| Yes | 14 | 4 | (28.6) | 1.1(0.3–3.6) | 0.04(0.005–0.3) | 0.002 ** |
| No | 342 | 92 | (26.9) | Reference | Reference | |
| Working tools and machines (n = 350) | ||||||
| Yes | 22 | 9 | (40.9) | 1.8(0.7–4.4) | 2.2(0.6–8.4) | 0.3 (ns) |
| No | 328 | 91 | (27.3) | Reference | Reference | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singo, J.; Isunju, J.B.; Moyo, D.; Bose-O’Reilly, S.; Steckling-Muschack, N.; Mamuse, A. Accidents, Injuries, and Safety among Artisanal and Small-Scale Gold Miners in Zimbabwe. Int. J. Environ. Res. Public Health 2022, 19, 8663. https://doi.org/10.3390/ijerph19148663
Singo J, Isunju JB, Moyo D, Bose-O’Reilly S, Steckling-Muschack N, Mamuse A. Accidents, Injuries, and Safety among Artisanal and Small-Scale Gold Miners in Zimbabwe. International Journal of Environmental Research and Public Health. 2022; 19(14):8663. https://doi.org/10.3390/ijerph19148663
Chicago/Turabian StyleSingo, Josephine, John Bosco Isunju, Dingani Moyo, Stephan Bose-O’Reilly, Nadine Steckling-Muschack, and Antony Mamuse. 2022. "Accidents, Injuries, and Safety among Artisanal and Small-Scale Gold Miners in Zimbabwe" International Journal of Environmental Research and Public Health 19, no. 14: 8663. https://doi.org/10.3390/ijerph19148663
APA StyleSingo, J., Isunju, J. B., Moyo, D., Bose-O’Reilly, S., Steckling-Muschack, N., & Mamuse, A. (2022). Accidents, Injuries, and Safety among Artisanal and Small-Scale Gold Miners in Zimbabwe. International Journal of Environmental Research and Public Health, 19(14), 8663. https://doi.org/10.3390/ijerph19148663