
Which Aspects of Psychological Resilience Moderate the Association between Deterioration in Sleep and Depression in Patients with Prostate Cancer?


Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Measures
2.3. Procedure
2.4. Statistical Analyses
3. Results
3.1. Background Data
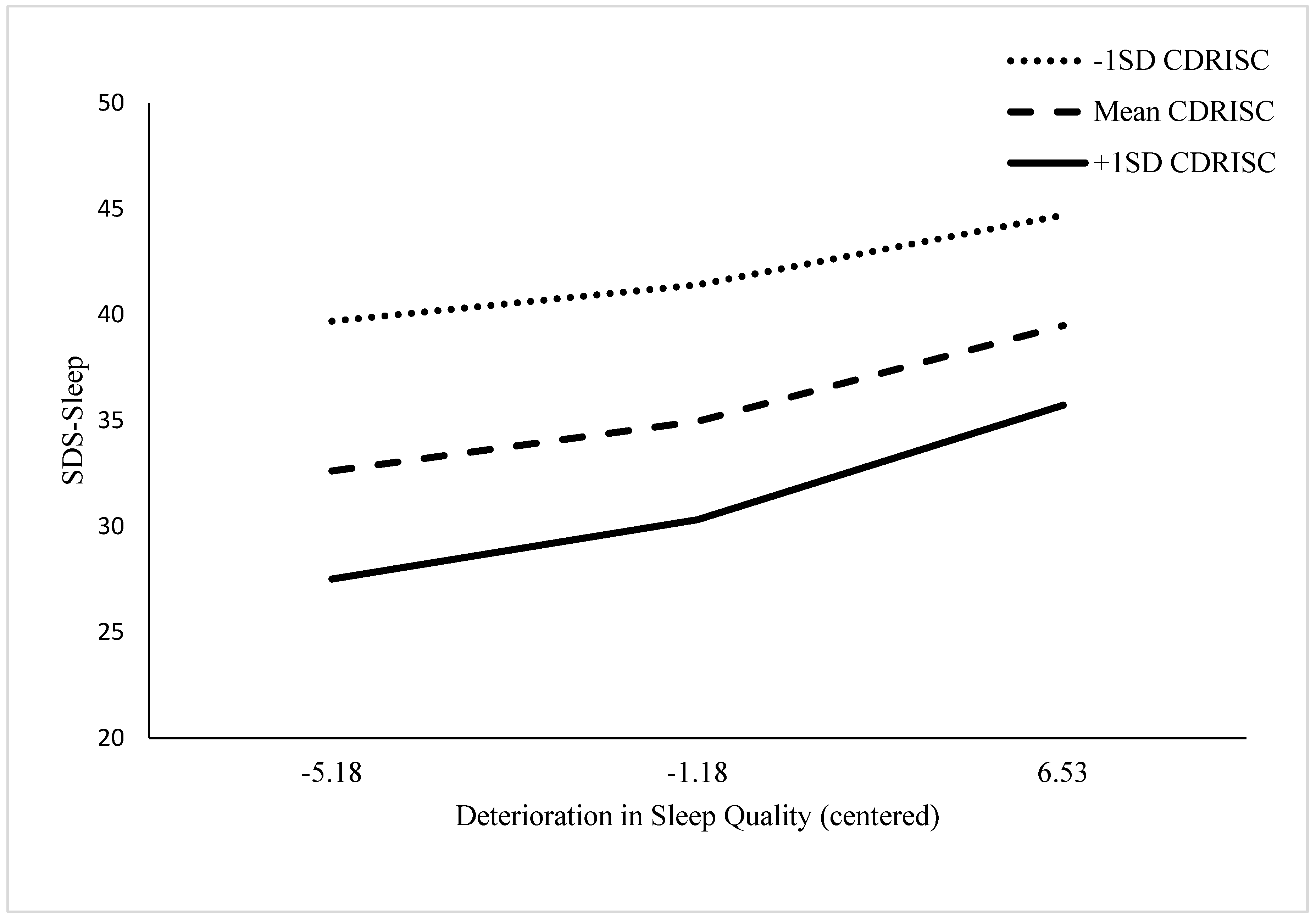
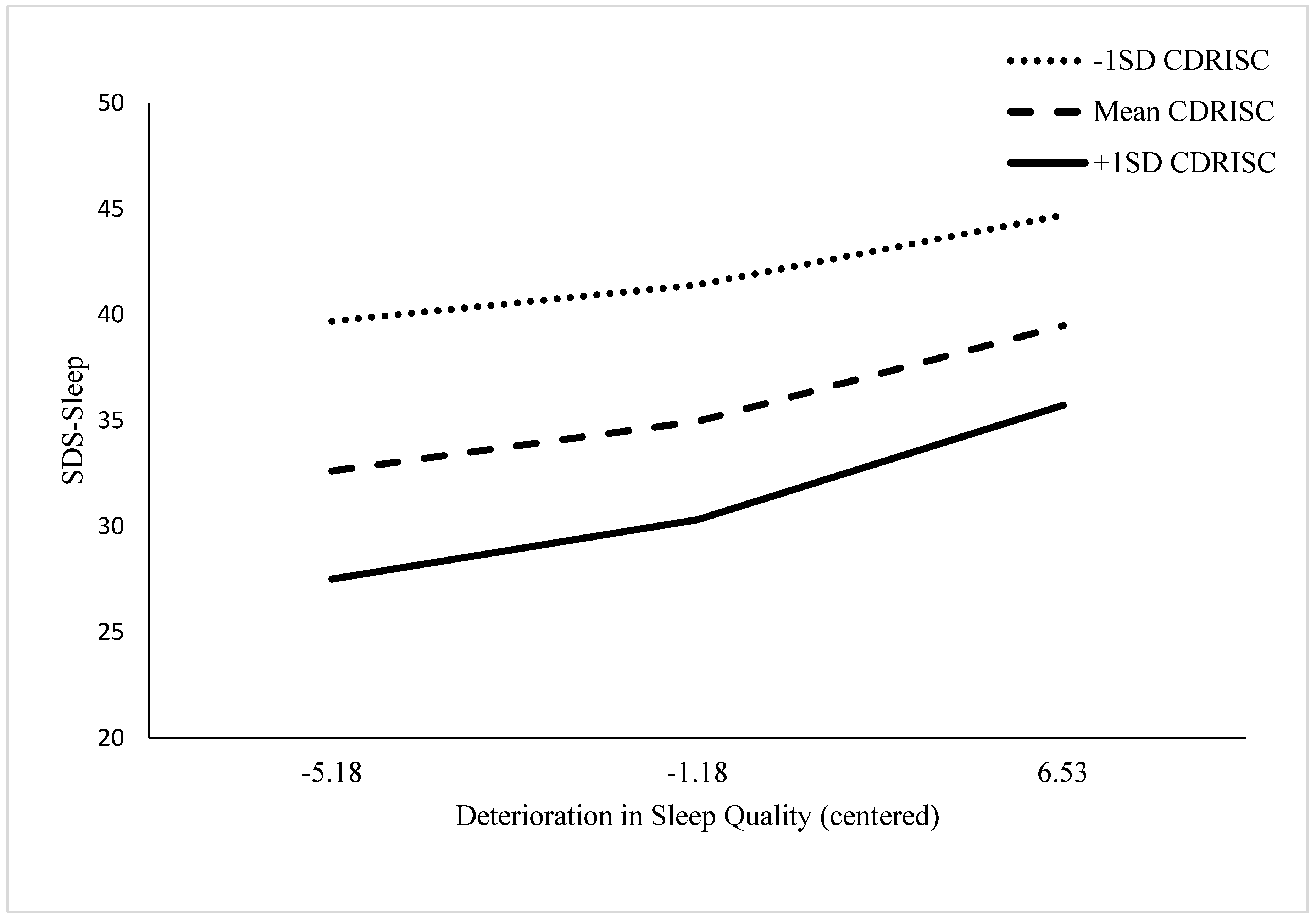
3.1.1. Influence of PR on the Association between Sleep Difficulties and Depression: Total Scores
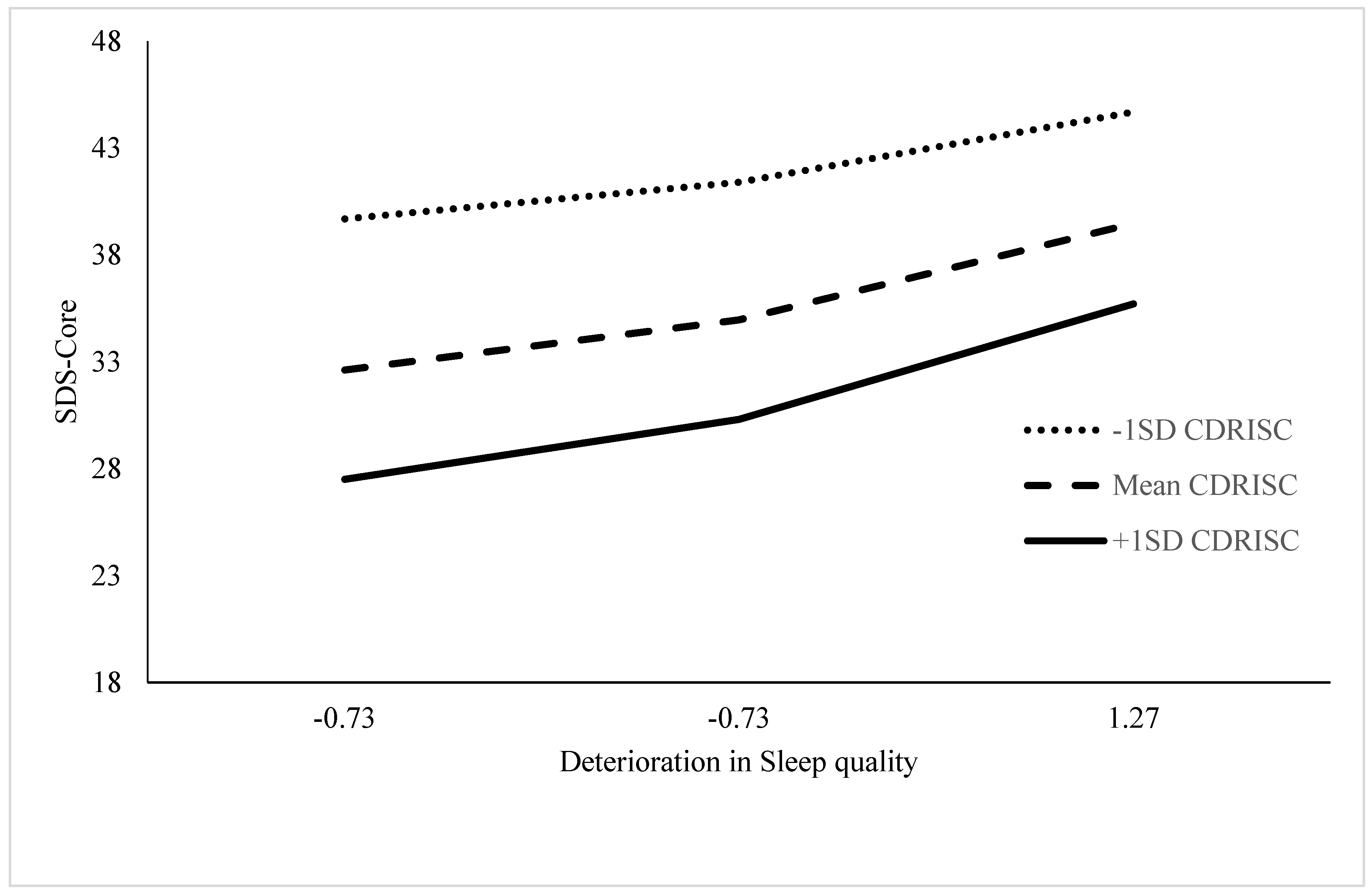
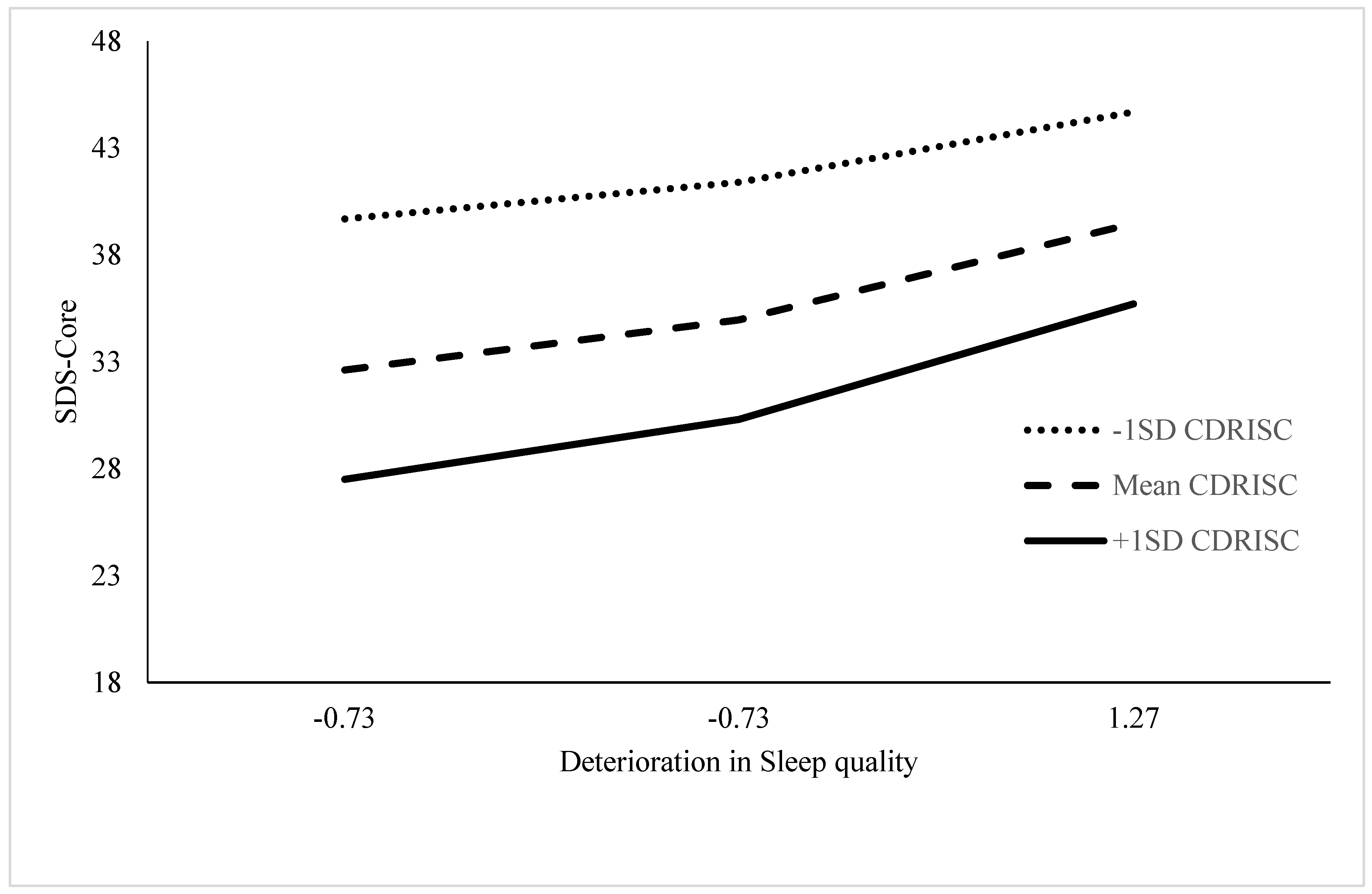
3.1.2. Influence of PR on the association between Sleep Difficulties and Depression: Specific Symptoms
Breakdown of Full-Scale Scores to Core Elements
3.2. Associations between Core Elements of Sleep Change, PR, and Depression
4. Discussion
4.1. Clinical Implications
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Ethics Statements
References
- Fervaha, G.; Izard, J.P.; Tripp, D.A.; Rajan, S.; Leong, D.P.; Siemens, D.R. Depression and prostate cancer: A focused review for the clinician. Urol. Oncol. Semin. Orig. Investig. 2019, 37, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Brunckhorst, O.; Hashemi, S.; Martic, A.; George, G.; Van Hemelrijck, M.; Dasgupta, P.; Stewart, R.; Ahmed, K. Depression, anxiety, and suicidality in patients with prostate cancer: A systematic review and meta-analysis of observational studies. Prostate Cancer Prostatic Dis. 2021, 24, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, S.; Sandin, F.; Fall, K.; Lambe, M.; Adolfsson, J.; Stattin, P.; Bill-Axelson, A. Risk of suicide in men with low-risk prostate cancer. Eur. J. Cancer 2013, 49, 1588–1599. [Google Scholar] [CrossRef] [Green Version]
- Jayadevappa, R.; Malkowicz, S.; Chhatre, S.; Johnson, J.; Gallo, J. The burden of depression in prostate cancer. Psycho-Oncology 2011, 21, 1338–1345. [Google Scholar] [CrossRef]
- Gieseler, F.; Gaertner, L.; Thaden, E.; Theobald, W. Cancer Diagnosis: A Trauma for Patients and Doctors Alike. Oncology 2018, 23, 752–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharpley, C.; Christie, D.; Bitsika, V.; Agnew, L.; Andronicos, N.; McMillan, M.; Richards, T. The use of salivary cortisol as an index of chronic stress that correlates with depression in prostate cancer patients. Psycho-Oncology 2017, 26, 1400–1402. [Google Scholar] [CrossRef] [PubMed]
- APA. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Maguire, R.; Drummond, F.; Hanly, P.; Gavin, A.; Sharp, L. Problems sleeping with prostate cancer: Exploring possible risk factors for sleep disturbance in a population-based sample of survivors. Supportive Care Cancer 2019, 27, 3365–3373. [Google Scholar] [CrossRef] [Green Version]
- Galvin, K.; Garland, S.; Wibowo, E. The relationship between sleep hygiene, mood, and insomnia symptoms in men with prostate cancer. Supportive Care Cancer 2022, 30, 4055–4064. [Google Scholar] [CrossRef]
- Riemann, D.; Krone, L.; Wulff, K.; Nissen, C. Sleep, insomnia, and depression. Neuropsychopharmacology 2020, 45, 74–89. [Google Scholar] [CrossRef]
- Denckla, C.; Cicchetti, D.; Kubzansky, L.; Seedat, S.; Teicher, M.; Williams, D.; Koenen, K. Psychological resilience: An update on definitions, a critical appraisal, and research recommendations. Eur. J. Psychotraumatol. 2020, 11, 1822064. [Google Scholar] [CrossRef]
- Andreescu, C.; Lenze, E.J.; Dew, M.A.; Begley, A.E.; Mulsant, B.H.; Dombrovski, A.Y.; Pollock, B.G.; Stack, J.; Miller, M.D.; Reynolds, C.F. Effect of comorbid anxiety on treatment response and relapse risk in late-life depression: Controlled study. Br. J. Psychiatry 2007, 190, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharpley, C.; Christie, D.; Bitsika, V.; Andronicos, N.; Agnew, L.; Richards, T.; McMillan, M. Comparing a genetic and a psychological factor as correlates of anxiety, depression, and chronic stress in men with prostate cancer. Supportive Care Cancer 2018, 26, 3195–3200. [Google Scholar] [CrossRef] [PubMed]
- Charney, D.S. Psychobiological Mechanisms of resilience and Vulnerability: Implications for Successful Adaptation to Extreme Stress. Focus 2004, 2, 368–391. [Google Scholar] [CrossRef]
- Jopp, D.; Rott, C. Adaptation in Very Old Age: Exploring the Role of Resources, Beliefs, and Attitudes for Centenarians’ Happiness. Psychol. Aging 2006, 21, 266–280. [Google Scholar] [CrossRef] [PubMed]
- Karoly, P.; Reuhlman, L. Psychological resilience and its correlates in chronic pain. Pain 2006, 123, 90–97. [Google Scholar] [CrossRef]
- Bonanno, G.A.; Galea, S.; Bucciarelli, A.; Vlahoz, D. What predicts psychological resilience after disaster? The role of demographics, resources, and life stress. J. Consult. Clin. Psychol. 2007, 75, 671–682. [Google Scholar] [CrossRef]
- Killgore, W.; Taylor, E.; Cloonan, S.; Dailey, N. Psychological resilience during the COVID-19 lockdown. Psychiatry Res. 2020, 291, 113216. [Google Scholar] [CrossRef]
- Liu, X.; Liu, C.; Tian, X.; Zou, G.; Li, G.; Kong, L.; Li, P. Associations of Perceived Stress, Resilience and Social Support with Sleep Disturbance Among Community-dwelling Adults. Stress Health 2016, 32, 578–586. [Google Scholar] [CrossRef]
- Haglund, M.E.M.; Nestadt, P.S.; Cooper, N.S.; Southwick, S.M.; Charney, D.S. Psychobiological mechanisms of resilience: Relevance to prevention and treatment of stress-related psychopathology. Dev. Psychopathol. 2007, 19, 889–920. [Google Scholar] [CrossRef]
- Liu, Y.; Collins, C.; Wang, K.; Xie, X.; Bie, R. The prevalence and trend of depression among veterans in the United States. J. Affect. Disord. 2019, 245, 724–727. [Google Scholar] [CrossRef]
- Insel, T. Transforming Diagnosis. Available online: www.nimh.nih.gov/about/director/2013/transforming-diagnosis-shtml (accessed on 27 May 2022).
- Kapur, S.; Phillips, A.; Insel, T. Why has it taken so long for biological psychiatry to develop clinical tests and what to do about it? Mol. Psychiatry 2012, 17, 1174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharpley, C.; Bitsika, V.; Christie, D. Change in Sleeping Patterns affects Cognitive Depression in Prostate Cancer Patients. Psycho-Oncology, 2022; submitted. [Google Scholar]
- Zung, W. A self-rating depression scale. Arch. Gen. Psychiatry 1965, 12, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Zung, W. From art to science: The diagnosis and treatment of depression. Arch. Gen. Psychiatry 1973, 29, 328–337. [Google Scholar] [CrossRef] [PubMed]
- DeJonge, J.; Baneke, J. The Zung Self-rating Depression Scale: A replication study on reliability, validity and prediction. Psychol. Rep. 1989, 64, 833–834. [Google Scholar] [CrossRef]
- Gabrys, J.; Peters, K. Reliability, discriminant and predictive validity of the Zung Self-Rating Depression Scale. Psychol. Rep. 1985, 57, 1091–1096. [Google Scholar] [CrossRef]
- Sharpley, C.; Bitsika, V.; Christie, D. Understanding the causes of depression among prostate cancer patients: Development of the Effects of Prostate Cancer on Lifestyle Questionnaire. Psycho-Oncology 2009, 18, 162–168. [Google Scholar] [CrossRef]
- Schaefer, A.; Brown, J.; Watson, C.; Plenel, D.; DeMotts, J.; Howard, M.; Petrik, N.; Ballweg, B. Comparison of the validities of the Beck, Zung and MMPI depression scales. J. Consult. Clin. Psychol. 1985, 53, 415–418. [Google Scholar] [CrossRef]
- Bastien, C.; Vallières, A.; Morin, C. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Dirksen, S.; Epstein, D.; Hoyt, M. Insomnia, depression, and distress among outpatients with prostate cancer. Appl. Nurs. Res. 2009, 22, 154–158. [Google Scholar] [CrossRef]
- Connor, K.; Davidson, J. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Sharpley, C.; Bitsika, V.; Wooten, A.; Christie, D. Does resilience “buffer” against depression in prostate cancer patients? A multi-site replication. Eur. J. Cancer Care 2014, 23, 545–552. [Google Scholar] [CrossRef] [PubMed]
- Howard, G.; Ralph, K.; Gulanik, N.; Nance, D.; Gerber, S. Internal validity in pre-test –post-test self-report evaluations and a re-evaluation of retrospective pre-tests. Appl. Psychol. Meas. 1979, 3, 1–23. [Google Scholar] [CrossRef]
- Campbell, D.; Stanley, J. Experimental and Quasi-Experimental Designs for Research; Rand McNally: Chicago, IL, USA, 1963. [Google Scholar]
- Sharpley, C.; Bitsika, V.; Wooten, A.; Christie, D. Predictors of depression in prostate cancer patients: A comparison of psychological resilience versus pre-existing anxiety and depression. J. Men’s Health 2014, 11, 115–120. [Google Scholar] [CrossRef]
- Hayes, A.; Rockwood, N. Regression-based statistical mediation and moderation analysis in clinical research: Observations, recommendations, and implementation. Behav. Res. Ther. 2017, 98, 39–57. [Google Scholar] [CrossRef]
- Hayes, A. Introduction to Mediation, Moderation and Conditional Process Analysis; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Aiken, L.; West, S. Multiple Regression: Testing and Interpreting Interactions; Sage: Thousand Oaks, CA, USA, 1991. [Google Scholar]
- Sharpley, C.; Christie, D.; Bitsika, V. Deterioration in Sleep Quality affects Cognitive Depression in Prostate Cancer Patients. Am. J. Men’s Health, 2021; in press. [Google Scholar]
- Bill-Axelson, A.; Garmo, H.; Nyberg, U.; Lamb, M.; Bratt, O.; Stattin, P.; Adolfsson, J.; Steineck, G. Psychiatric treatment in men with prostate cancer—Results from a Nation-wide, population-based cohort study. Eur. J. Cancer 2011, 47, 2195–2201. [Google Scholar] [CrossRef]
- Carlson, L.; Speca, M.; Patel, K.; Goodey, E. Mindfulness-based stress reduction in relation to quality of life, mood, symptoms of stress, and immune parameters in breast and prostate cancer outpatients. Psychosom. Med. 2003, 65, 571–581. [Google Scholar] [CrossRef] [Green Version]
- Baumann, F.; Zopf, E.; Bloch, W. Clinical exercise interventions in prostate cancer patients—A systematic review of randomized controlled trials. Supportive Care Cancer 2012, 20, 221–233. [Google Scholar] [CrossRef]
- Reivich, K.; Seligman, M.; McBride, S. Master resilience training in the U.S. Army. Am. Psychol. 2011, 66, 25–34. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Variable | Sample Characteristics |
|---|---|
| Age | M = 73.50 years (SD = 7.14 yr), range = 44 to 87 years |
| Relationship Status | |
| With wife/partner | 72.9% |
| Widowed | 6.8% |
| Divorced/separated | 11.9% |
| Never married/partnered | 8.5% |
| Time since diagnosis | M = 61.54 mo (SD = 24.27 mo), range = 1 to 197 mo |
| Treatments received | |
| Radiotherapy | 27.8% |
| Surgery | 7.4% |
| Hormone therapy | 11.1% |
| Combinations | 50.0% |
| Surveillance | 3.1% |
| Current treatment | |
| Radiotherapy | 52.6% |
| Hormone therapy | 31.6% |
| Combinations | 10.5% |
| Surveillance | 5.3% |
| Present status | |
| Cancer still present, undergoing treatment | 37.3% |
| In remission (no signs) | 37.3% |
| Cancer recurring after previous treatment | 25.4% |
| SDS | M = 36.14 (SD = 8.56), range = 20–57 |
| SDS-Sleep | M = 31.72 (SD = 7.45), range = 18–50 |
| SDS-Core | M = 11.02 (SD = 7.45), range = 18–50 |
| CDRISC | M = 77.42 (SD = 14.51), range = 41–100 |
| CDRISC-Core | M = 6.59 (SD = 1.64), range = 0–8 |
| ISI change | M = 5.93 (SD = 5.40), range = 1–21 |
| ISI Item 1 change | M = 0.73 (SD = 0.04), range = 1–4 |
| SDS-Sleep Items | Corrected Item–Total Correlation | Alpha If Item Deleted |
|---|---|---|
| 1. I feel downhearted and blue. | 0.469 | 0.807 |
| 2. Morning is when I feel the best. | 0.194 | 0.827 |
| 3. I have crying spells or feel like it. | 0.264 | 0.817 |
| 4. I eat as much as I used to. | 0.422 | 0.809 |
| 5. I still enjoy sex. | 0.190 | 0.825 |
| 6. I notice that I am losing weight. | 0.180 | 0.820 |
| 7. I have trouble with constipation. | 0.332 | 0.813 |
| 8. My heart beats faster than usual. | 0.172 | 0.819 |
| 9. My mind is as clear as it used to be. | 0.585 | 0.797 |
| 10. I find it easy to do the things I used to. | 0.610 | 0.796 |
| 11. I am restless and can’t keep still. | 0.389 | 0.810 |
| 12. I feel hopeful about the future. | 0.480 | 0.805 |
| 13. I am more irritable than usual. | 0.417 | 0.810 |
| 14. I find it easy to make decisions. | 0.614 | 0.795 |
| 15. I feel that I am useful and needed. | 0.570 | 0.798 |
| 16. My life is pretty full. | 0.515 | 0.803 |
| 17. I feel that others would be better off if I were dead. | 0.235 | 0.818 |
| 18. I still enjoy doing the things I used to. | 0.692 | 0.794 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharpley, C.F.; Christie, D.R.H.; Bitsika, V. Which Aspects of Psychological Resilience Moderate the Association between Deterioration in Sleep and Depression in Patients with Prostate Cancer? Int. J. Environ. Res. Public Health 2022, 19, 8505. https://doi.org/10.3390/ijerph19148505
Sharpley CF, Christie DRH, Bitsika V. Which Aspects of Psychological Resilience Moderate the Association between Deterioration in Sleep and Depression in Patients with Prostate Cancer? International Journal of Environmental Research and Public Health. 2022; 19(14):8505. https://doi.org/10.3390/ijerph19148505
Chicago/Turabian StyleSharpley, Christopher F., David R. H. Christie, and Vicki Bitsika. 2022. "Which Aspects of Psychological Resilience Moderate the Association between Deterioration in Sleep and Depression in Patients with Prostate Cancer?" International Journal of Environmental Research and Public Health 19, no. 14: 8505. https://doi.org/10.3390/ijerph19148505
APA StyleSharpley, C. F., Christie, D. R. H., & Bitsika, V. (2022). Which Aspects of Psychological Resilience Moderate the Association between Deterioration in Sleep and Depression in Patients with Prostate Cancer? International Journal of Environmental Research and Public Health, 19(14), 8505. https://doi.org/10.3390/ijerph19148505