
The Association between Working Hours Flexibility and Well-Being Prior to and during COVID-19 in South Korea



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Sample
2.2. Participants
2.3. Variables
2.4. Statistical Analysis
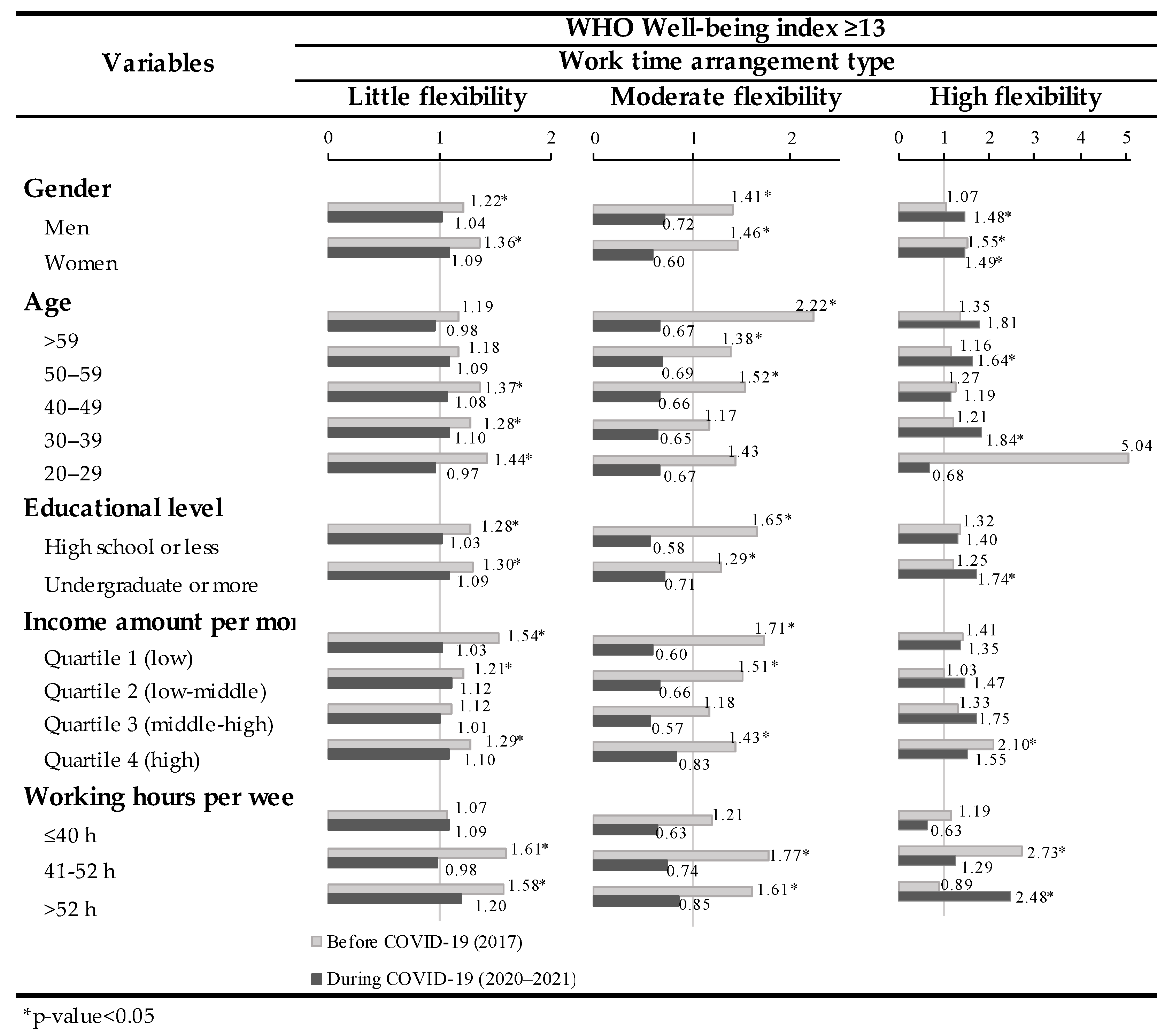
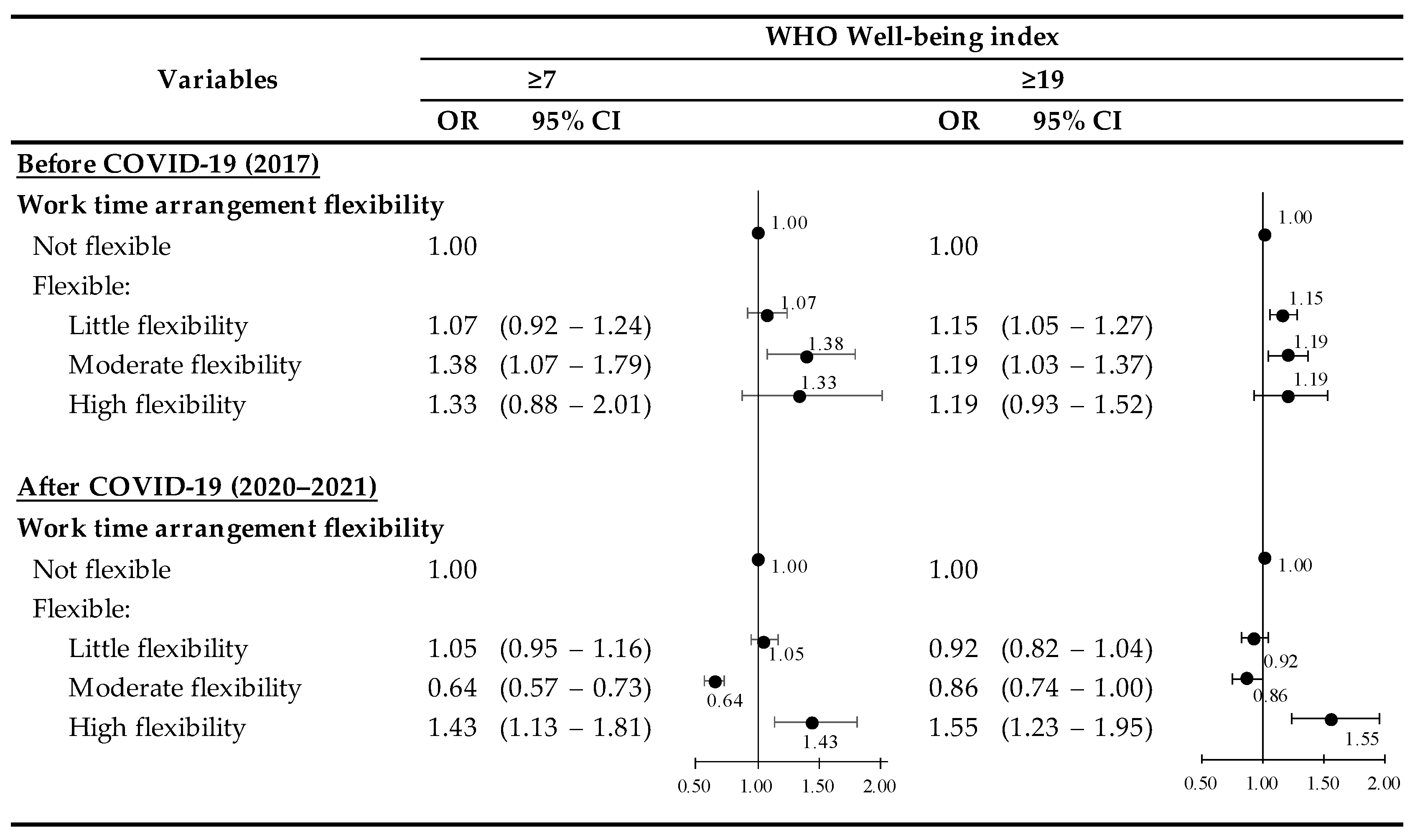
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cooper, R.; Baird, M. Bringing the “right to request” flexible working arrangements to life: From policies to practices. Empl. Relat. 2015, 37, 568–581. [Google Scholar] [CrossRef]
- Kattenbach, R.; Demerouti, E.; Nachreiner, F. Flexible working times: Effects on employees’ exhaustion, work-nonwork conflict and job performance. Career Dev. Int. 2010, 15, 279–295. [Google Scholar] [CrossRef]
- Demerouti, E.; Derks, D.; ten Brummelhuis, L.L.; Bakker, A.B. New ways of working: Impact on working conditions, work–family balance, and well-being. In The Impact of ICT on Quality of Working Life; Springer: New York, NY, USA, 2014; pp. 123–141. [Google Scholar]
- Costa, G.; Sartori, S.; Åkerstedt, T. Influence of flexibility and variability of working hours on health and well-being. Chronobiol. Int. 2006, 23, 1125–1137. [Google Scholar] [CrossRef] [PubMed]
- Berg, P.; Kalleberg, A.L.; Appelbaum, E. Balancing work and family: The role of high-commitment environments. Ind. Relat. J. Econ. Soc. 2003, 42, 168–188. [Google Scholar] [CrossRef]
- Kelliher, C.; Anderson, D. Doing more with less? Flexible working practices and the intensification of work. Hum. Relat. 2010, 63, 83–106. [Google Scholar] [CrossRef]
- Scandura, T.A.; Lankau, M.J. Relationships of gender, family responsibility and flexible work hours to organizational commitment and job satisfaction. J. Organ. Behav. Int. J. Ind. Occup. Organ. Psychol. Behav. 1997, 18, 377–391. [Google Scholar] [CrossRef]
- De Menezes, L.M.; Kelliher, C. Flexible working and performance: A systematic review of the evidence for a business case. Int. J. Manag. Rev. 2011, 13, 452–474. [Google Scholar] [CrossRef]
- Ryan, A.M.; Kossek, E.E. Work-life policy implementation: Breaking down or creating barriers to inclusiveness? Hum. Resour. Manag. Publ. Coop. Sch. Bus. Adm. Univ. Mich. Alliance Soc. Hum. Resour. Manag. 2008, 47, 295–310. [Google Scholar] [CrossRef]
- Shagvaliyeva, S.; Yazdanifard, R. Impact of flexible working hours on work-life balance. Am. J. Ind. Bus. Manag. 2014, 4, 42311. [Google Scholar] [CrossRef] [Green Version]
- Costa, G.; Åkerstedt, T.; Nachreiner, F.; Baltieri, F.; Carvalhais, J.; Folkard, S.; Dresen, M.F.; Gadbois, C.; Gartner, J.; Sukalo, H.G. Flexible working hours, health, and well-being in Europe: Some considerations from a SALTSA project. Chronobiol. Int. 2004, 21, 831–844. [Google Scholar] [CrossRef]
- Golden, L.; Henly, J.; Lambert, S. Work schedule flexibility: A contributor to employee happiness? J. Soc. Res. Policy 2014. [Google Scholar] [CrossRef]
- Azizi, M.R.; Atlasi, R.; Ziapour, A.; Abbas, J.; Naemi, R. Innovative human resource management strategies during the COVID-19 pandemic: A systematic narrative review approach. Heliyon 2021, 7, e07233. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Chin, M.; Sung, M. How has COVID-19 changed family life and well-being in Korea? J. Comp. Fam. Stud. 2020, 51, 301–313. [Google Scholar] [CrossRef]
- Wang, M.-T.; Henry, D.A.; Del Toro, J.; Scanlon, C.L.; Schall, J.D. COVID-19 employment status, dyadic family relationships, and child psychological well-being. J. Adolesc. Health 2021, 69, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Seong, H.; Hyun, H.J.; Yun, J.G.; Noh, J.Y.; Cheong, H.J.; Kim, W.J.; Song, J.Y. Comparison of the second and third waves of the COVID-19 pandemic in South Korea: Importance of early public health intervention. Int. J. Infect. Dis. 2021, 104, 742–745. [Google Scholar] [CrossRef]
- KCDC. The Updates of COVID-19 in Republic of Korea. 2020. Available online: https://www.cdc.go.kr/board/board (accessed on 22 April 2020).
- Buomprisco, G.; Ricci, S.; Perri, R.; De Sio, S. Health and telework: New challenges after COVID-19 pandemic. Eur. J. Environ. Public Health 2021, 5, em0073. [Google Scholar] [CrossRef]
- Del Boca, D.; Oggero, N.; Profeta, P.; Rossi, M. Women’s and men’s work, housework and childcare, before and during COVID-19. Rev. Econ. Househ. 2020, 18, 1001–1017. [Google Scholar] [CrossRef]
- Lee, H. Family conflicts, daily problems that being stuck at home created during COVID-19. Psychiatr. News 2020, 16. Available online: http://www.psychiatricnews.net/news/articleView.html?idxno=19365 (accessed on 23 April 2022).
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems: Alphabetical Index; World Health Organization: Geneva, Switzerland, 2004; Volume 3. [Google Scholar]
- Park, S.; Park, C.; Sung, J.H. How does the involuntary choice of self-employment affect subjective well-being in small-sized business workers? A cross-sectional study from the fifth Korean working conditions survey. Int. J. Environ. Res. Public Health 2022, 19, 1011. [Google Scholar] [CrossRef]
- Park, M.; Nari, F.; Jeong, W.; Park, E.-C.; Jang, S.-I. Association between occupational noise and vibration and anxiety in the South Korean working population: A cross-sectional study. J. Occup. Med. Toxicol. 2022, 17, 1. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Rhee, K.Y.; Oh, M.J.; Park, J. The validity and reliability of the second Korean working conditions survey. Saf. Health Work 2013, 4, 111–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, M.; Suh, C.; Choi, S.P.; Lee, C.K.; Son, B.C. Validation of the work engagement scale-3, used in the 5th Korean working conditions survey. Ann. Occup. Environ. Med. 2020, 32, e27. [Google Scholar] [CrossRef] [PubMed]
- Nari, F.; Kim, Y.K.; Kang, S.H.; Park, E.-C.; Jang, S.-I. Association between occupational noise and vibration exposure and insomnia among workers in Korea. Life 2020, 10, 46. [Google Scholar] [CrossRef] [PubMed]
- Awata, S.; Bech, P.; Yoshida, S.; Hirai, M.; Suzuki, S.; Yamashita, M.; Ohara, A.; Hinokio, Y.; Matsuoka, H.; Oka, Y. Reliability and validity of the Japanese version of the world health organization-five well-being index in the context of detecting depression in diabetic patients. Psychiatry Clin. Neurosci. 2007, 61, 112–119. [Google Scholar] [CrossRef]
- De Wit, M.; Pouwer, F.; Gemke, R.J.; Delemarre-Van De Waal, H.A.; Snoek, F.J. Validation of the WHO-5 Well-Being Index in adolescents with type 1 diabetes. Diabetes Care 2007, 30, 2003–2006. [Google Scholar] [CrossRef] [Green Version]
- Heun, R.; Bonsignore, M.; Barkow, K.; Jessen, F. Validity of the five-item WHO Well-Being Index (WHO-5) in an elderly population. Eur. Arch. Psychiatry Clin. Neurosci. 2001, 251, 27–31. [Google Scholar] [CrossRef]
- Carrozzino, D.; Christensen, K.S.; Patierno, C.; Woźniewicz, A.; Møller, S.B.; Arendt, I.-M.T.; Zhang, Y.; Yuan, Y.; Sasaki, N.; Nishi, D. Cross-cultural validity of the WHO-5 Well-Being Index and Euthymia Scale: A clinimetric analysis. J. Affect. Disord. 2022, 311, 276–283. [Google Scholar] [CrossRef]
- Kim, H.-J.; Moon, Y.-S.; Son, B.-K.; Lee, S.-K.; Rho, H.-J.; Kim, D.-H. The utility of Korean version of the WHO Five Well-Being Index in evaluating depressive symptoms and quality of life in the aged dwelling in community. J. Korean Geriatr. Psychiatry 2010, 14, 90–96. [Google Scholar]
- Lades, L.K.; Laffan, K.; Daly, M.; Delaney, L. Daily emotional well-being during the COVID-19 pandemic. Br. J. Health Psychol. 2020, 25, 902–911. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Wetherall, K.; Cleare, S.; McClelland, H.; Melson, A.J.; Niedzwiedz, C.L.; O’Carroll, R.E.; O’Connor, D.B.; Platt, S.; Scowcroft, E. Mental health and well-being during the COVID-19 pandemic: Longitudinal analyses of adults in the UK COVID-19 Mental Health & Wellbeing study. Br. J. Psychiatry 2021, 218, 326–333. [Google Scholar] [PubMed]
- Magnavita, N.; Chirico, F.; Garbarino, S.; Bragazzi, N.L.; Santacroce, E.; Zaffina, S. SARS/MERS/SARS-CoV-2 outbreaks and burnout syndrome among healthcare workers. An umbrella systematic review. Int. J. Environ. Res. Public Health 2021, 18, 4361. [Google Scholar] [CrossRef] [PubMed]
- Spurk, D.; Straub, C. Flexible Employment Relationships and Careers in Times of the COVID-19 Pandemic; Elsevier: Amsterdam, The Netherlands, 2020; Volume 119, p. 103435. [Google Scholar]
- McKeever, V. Coronavirus Lockdowns Are Making the Working Day Longer for Many; CNBC: Englewood Cliffs, NJ, USA, 2020. [Google Scholar]
- Agba, A.O.; Ocheni, S.I.; Agba, M.S. COVID-19 and the world of work dynamics: A critical review. J. Educ. Soc. Res. 2020, 10, 119. [Google Scholar] [CrossRef]
- Marino, L.; Capone, V. Smart working and well-being before and during the COVID-19 pandemic: A scoping review. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 1516–1536. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | WHO Well-Being Index-5 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Before COVID-19 (2017) | During COVID-19 (2020–2021) | |||||||||||
| TOTAL | Bad (Index < 13) | Good (Index ≥ 13) | TOTAL | Bad (Index < 13) | Good (Index ≥ 13) | |||||||
| N | % | N | % | N | % | N | % | N | % | N | % | |
| (N = 45,137) | 21,494 | 100.0 | 6466 | 30.1 | 15,028 | 69.9 | 23,643 | 100.0 | 8630 | 36.5 | 15,013 | 63.5 |
| Work time arrangement type | ||||||||||||
| Not flexible * | 17,292 | 80.5 | 5364 | 31.0 | 11,928 | 69.0 | 20,300 | 85.9 | 7322 | 36.1 | 12,978 | 63.9 |
| Flexible: | ||||||||||||
| Little flexibility ** | 2747 | 12.8 | 740 | 26.9 | 2007 | 73.1 | 1851 | 7.8 | 677 | 36.6 | 1174 | 63.4 |
| Moderate flexibility *** | 1101 | 5.1 | 265 | 24.1 | 836 | 75.9 | 1125 | 4.8 | 520 | 46.2 | 605 | 53.8 |
| High flexibility **** | 354 | 1.6 | 97 | 27.4 | 257 | 72.6 | 367 | 1.6 | 111 | 30.2 | 256 | 69.8 |
| Gender | ||||||||||||
| Men | 10,892 | 50.7 | 3268 | 30.0 | 7624 | 70.0 | 11,568 | 48.9 | 4302 | 37.2 | 7266 | 62.8 |
| Women | 10,602 | 49.3 | 3198 | 30.2 | 7404 | 69.8 | 12,075 | 51.1 | 4328 | 35.8 | 7747 | 64.2 |
| Age | ||||||||||||
| >59 | 1615 | 7.5 | 687 | 42.5 | 928 | 57.5 | 2691 | 11.4 | 1195 | 44.4 | 1496 | 55.6 |
| 50–59 | 4527 | 21.1 | 1466 | 32.4 | 3061 | 67.6 | 5624 | 23.8 | 2127 | 37.8 | 3497 | 62.2 |
| 40–49 | 6223 | 29.0 | 1870 | 30.0 | 4353 | 70.0 | 6429 | 27.2 | 2367 | 36.8 | 4062 | 63.2 |
| 30–39 | 5823 | 27.1 | 1642 | 28.2 | 4181 | 71.8 | 5973 | 25.3 | 2011 | 33.7 | 3962 | 66.3 |
| 20–29 | 3306 | 15.4 | 801 | 24.2 | 2505 | 75.8 | 2926 | 12.4 | 930 | 31.8 | 1996 | 68.2 |
| Educational level | ||||||||||||
| High school or less | 8161 | 38.0 | 2940 | 36.0 | 5221 | 64.0 | 8795 | 37.2 | 3687 | 41.9 | 5108 | 58.1 |
| Undergraduate or more | 13,333 | 62.0 | 3526 | 26.4 | 9807 | 73.6 | 14,848 | 62.8 | 4943 | 33.3 | 9905 | 66.7 |
| Income amount per month | ||||||||||||
| Quartile 1 (low) | 6021 | 28.0 | 2077 | 34.5 | 3944 | 65.5 | 6728 | 28.5 | 2770 | 41.2 | 3958 | 58.8 |
| Quartile 2 (low–middle) | 6075 | 28.3 | 1800 | 29.6 | 4275 | 70.4 | 5595 | 23.7 | 2105 | 37.6 | 3490 | 62.4 |
| Quartile 3 (middle–high) | 5629 | 26.2 | 1573 | 27.9 | 4056 | 72.1 | 6713 | 28.4 | 2233 | 33.3 | 4480 | 66.7 |
| Quartile 4 (high) | 3769 | 17.5 | 1016 | 27.0 | 2753 | 73.0 | 4607 | 19.5 | 1522 | 33.0 | 3085 | 67.0 |
| Working hours per week | ||||||||||||
| ≤40 h | 11,996 | 55.8 | 3315 | 27.6 | 8681 | 72.4 | 16,422 | 69.5 | 5770 | 35.1 | 10,652 | 64.9 |
| 41–52 h | 6412 | 29.8 | 1948 | 30.4 | 4464 | 69.6 | 5666 | 24.0 | 2172 | 38.3 | 3494 | 61.7 |
| >52 h | 3086 | 14.4 | 1203 | 39.0 | 1883 | 61.0 | 1555 | 6.6 | 688 | 44.2 | 867 | 55.8 |
| Commuting time | ||||||||||||
| >60 min | 2588 | 12.0 | 850 | 32.8 | 1738 | 67.2 | 3824 | 16.2 | 1470 | 38.4 | 2354 | 61.6 |
| 30–60 min | 9264 | 43.1 | 2660 | 28.7 | 6604 | 71.3 | 9608 | 40.6 | 3555 | 37.0 | 6053 | 63.0 |
| <30 min | 9642 | 44.9 | 2956 | 30.7 | 6686 | 69.3 | 10,118 | 42.8 | 3562 | 35.2 | 6556 | 64.8 |
| Self-perceived health status | ||||||||||||
| Good | 16,288 | 75.8 | 4127 | 25.3 | 12,161 | 74.7 | 17,452 | 73.8 | 5334 | 30.6 | 12,118 | 69.4 |
| Poor | 5206 | 24.2 | 2339 | 44.9 | 2867 | 55.1 | 6191 | 26.2 | 3296 | 53.2 | 2895 | 46.8 |
| Variables | WHO Well-Being Index ≥ 13 | |||
|---|---|---|---|---|
| Before COVID-19 (2017) | During COVID-19 (2020–2021) | |||
| OR | 95% CI | OR | 95% CI | |
| Work time arrangement flexibility | ||||
| Not flexible | 1.00 | 1.00 | ||
| Flexible: | ||||
| Little flexibility | 1.33 | (1.21–1.46) | 1.06 | (0.96–1.17) |
| Moderate flexibility | 1.48 | (1.28–1.71) | 0.66 | (0.59–0.75) |
| High flexibility | 1.35 | (1.06–1.72) | 1.49 | (1.18–1.88) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nerobkova, N.; Park, Y.S.; Park, E.-C.; Jang, S.-Y. The Association between Working Hours Flexibility and Well-Being Prior to and during COVID-19 in South Korea. Int. J. Environ. Res. Public Health 2022, 19, 8438. https://doi.org/10.3390/ijerph19148438
Nerobkova N, Park YS, Park E-C, Jang S-Y. The Association between Working Hours Flexibility and Well-Being Prior to and during COVID-19 in South Korea. International Journal of Environmental Research and Public Health. 2022; 19(14):8438. https://doi.org/10.3390/ijerph19148438
Chicago/Turabian StyleNerobkova, Nataliya, Yu Shin Park, Eun-Cheol Park, and Suk-Yong Jang. 2022. "The Association between Working Hours Flexibility and Well-Being Prior to and during COVID-19 in South Korea" International Journal of Environmental Research and Public Health 19, no. 14: 8438. https://doi.org/10.3390/ijerph19148438
APA StyleNerobkova, N., Park, Y. S., Park, E.-C., & Jang, S.-Y. (2022). The Association between Working Hours Flexibility and Well-Being Prior to and during COVID-19 in South Korea. International Journal of Environmental Research and Public Health, 19(14), 8438. https://doi.org/10.3390/ijerph19148438