
Histological and Immunohistochemical Analysis of Peri-Implant Soft and Hard Tissues in Patients with Peri-Implantitis

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Clinical Variables
2.3. Surgical Procedure
2.4. Histological and Immunohistochemical Processing and Analysis
2.5. Statistical Analysis
3. Results
3.1. Clinical Features
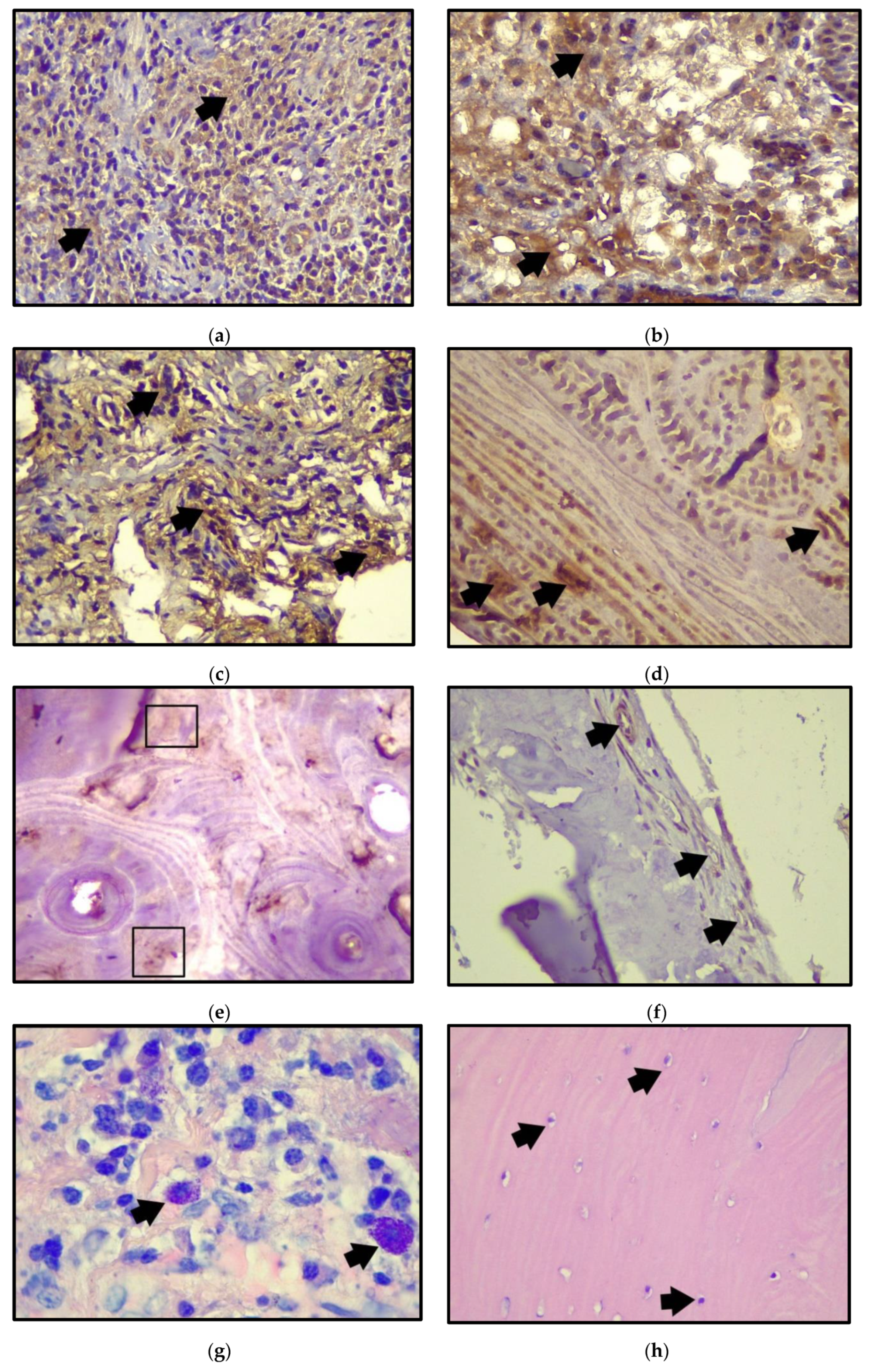
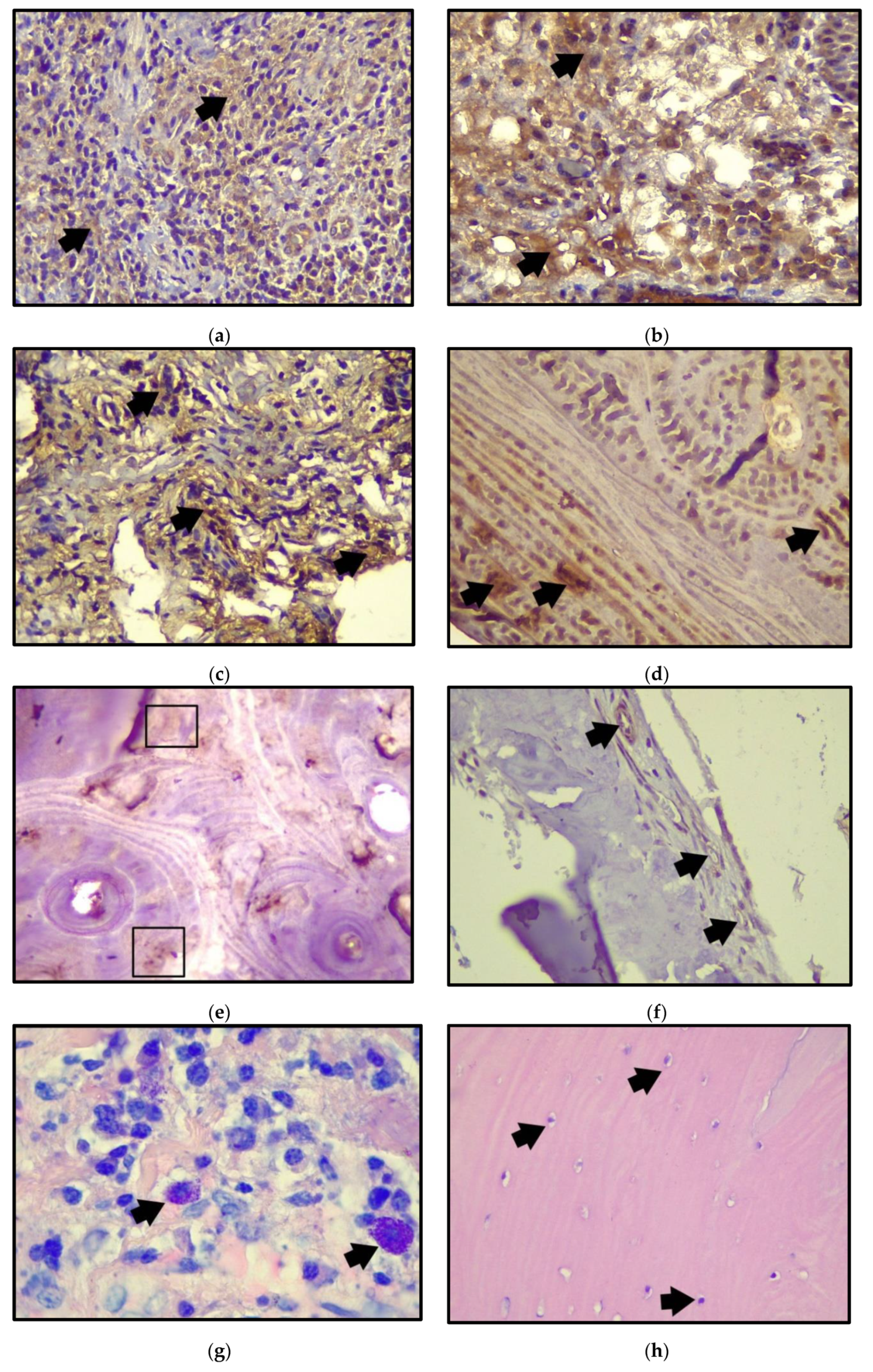
3.2. Histological and Immunohistochemical Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lee, C.; Huang, Y.; Zhu, L.; Weltman, R. Prevalences of peri-implantitis and peri-implant mucositis: Systematic review and meta-analysis. J. Dent. 2017, 62, 1–12. [Google Scholar] [CrossRef]
- Alassy, H.; Parachuru, P.; Wolff, L. Peri-Implantitis Diagnosis and Prognosis Using Biomarkers in Peri-Implant Crevicular Fluid: A Narrative Review. Diagnostics 2019, 9, 214. [Google Scholar] [CrossRef] [Green Version]
- Yaghobee, S.; Khorsand, A.; Ghohroudi, A.A.R.; Sanjari, K.; Kadkhodazadeh, M. Assessment of interleukin-1beta and interleukin-6 in the crevicular fluid around healthy implants, implants with peri-implantitis, and healthy teeth: A cross-sectional study. J. Korean Assoc. Oral Maxillofac. Surg. 2014, 40, 220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, L.; Xie, P.; Gong, P.; Tang, X.H.; Ding, Y.; Deng, L.X. Expression of HMGB1 and HMGN2 in Gingival Tissues, GCF and PICF of Periodontitis Patients and Peri-Implantitis. Arch. Oral Biol. 2011, 56, 1106–1111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Majid, A.; Alassiri, S.; Rathnayake, N.; Tervahartiala, T.; Gieselmann, D.R.; Sorsa, T. Matrix Metalloproteinase-8 as an Inflammatory and Prevention Biomarker in Periodontal and Peri-Implant Diseases. Int. J. Dent. 2018, 2018, 7891323. [Google Scholar] [CrossRef] [PubMed]
- Jamshidy, L.; Tadakamadla, S.K.; Choubsaz, P.; Sadeghi, M.; Tadakamadla, J. Association of IL-10 and TNF-α Polymorphisms with Dental Peri-Implant Disease Risk: A Meta-Analysis, Meta-Regression, and Trial Sequential Analysis. Int. J. Environ. Res. Public Health 2021, 18, 7697. [Google Scholar] [CrossRef]
- Mackay, F.; Schneider, P.; Rennert, P.; Browning, J. BAFF and APRIL: A tutorial on B cell survival. Ann. Rev. Immunol. 2003, 21, 231–264. [Google Scholar] [CrossRef]
- Cancro, M.P. Signalling crosstalk in B cells: Managing worth and need. Nat. Rev. Immunol. 2009, 9, 657–661. [Google Scholar] [CrossRef] [Green Version]
- Ospina, F.; Betancur, J.F.; Suso, J.P.; Muñoz-Buitron, E.; Cañas, C.; Tobón, G. Role of the cytokine BAFF in autoimmune diseases: Physiopathology and therapeutic targets. Rev. Colomb. Reumatol. 2016, 23, 177–194. [Google Scholar] [CrossRef]
- Kawai, T.; Matsuyama, T.; Hosokawa, Y.; Makihira, S.; Seki, M.; Karimbux, N.Y.; Goncalves, R.B.; Valverde, P.; Dibart, S.; Li, Y.P.; et al. B and T Lymphocytes Are the Primary Sources of RANKL in the Bone Resorptive Lesion of Periodontal Disease. Am. J. Pathol. 2006, 169, 987–998. [Google Scholar] [CrossRef] [Green Version]
- Gümüş, P.; Buduneli, E.; Biyikoǧlu, B.; Aksu, K.; Saraç, F.; Buduneli, N.; Lappin, D.F. Gingival Crevicular Fluid and Serum Levels of APRIL, BAFF and TNF-Alpha in Rheumatoid Arthritis and Osteoporosis Patients with Periodontal Disease. Arch. Oral Biol. 2013, 58, 1302–1308. [Google Scholar] [CrossRef]
- Gümüş, P.; Nizam, N.; Lappin, D.F.; Buduneli, N. Saliva and Serum Levels of B-Cell Activating Factors and Tumor Necrosis Factor-α in Patients with Periodontitis. J. Periodontol. 2014, 85, 270–280. [Google Scholar] [CrossRef]
- Abe, T.; AlSarhan, M.; Benakanakere, M.R.; Maekawa, T.; Kinane, D.F.; Cancro, M.P.; Korostoff, J.M. The B Cell–Stimulatory Cytokines BLyS and APRIL Are Elevated in Human Periodontitis and Are Required for B Cell–Dependent Bone Loss in Experimental Murine Periodontitis. J. Immunol. 2015, 195, 1427–1435. [Google Scholar] [CrossRef]
- Brekken, R.A.; Sage, E.H. SPARC, a matricellular protein: At the crossroads of cell-matrix communication. Matrix Biol. 2001, 19, 816–827. [Google Scholar] [CrossRef]
- Rosset, M.; Bradshaw, D. SPARC/osteonectin in mineralized tissue. Matrix Biol. 2016, 10, 4. [Google Scholar] [CrossRef] [Green Version]
- Brennan, P.; Umar, T.; Zaki, G.A.; Langdon, J.D.; Spedding, A.; Buckley, J.; Downie, P. Are myoepithelial cells responsible for the widespread expression of inducible nitric oxide synthase in pleomorphic adenoma? An immunohistochemical study. J. Oral Pathol. Med. 2000, 29, 279–283. [Google Scholar] [CrossRef]
- Kawasaki, Y.; Imaizumi, T.; Matsuura, H.; Ohara, S.; Takano, K.; Suyama, K.; Hashimoto, K.; Nozawa, R.; Suzuki, H.; Hosoya, M. Renal expression of alpha-smooth muscle actin and c-Met in children with Henoch-Schonlein purpura nephritis. Pediatr. Nephrol. 2008, 23, 913–919. [Google Scholar] [CrossRef]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S313–S318. [Google Scholar] [CrossRef]
- De Araújo, M.F.; Etchebehere, R.M.; de Melo, M.L.R.; Beghini, M.; Severino, V.O.; de Castro Côbo, E.; Rocha Rodrigues, D.B.; de Lima Pereira, S.A. Analysis of CD15, CD57 and HIF-1α in Biopsies of Patients with Peri-Implantitis. Pathol. Res. Pract. 2017, 213, 1097–1101. [Google Scholar] [CrossRef]
- De Araújo, M.F.; Filho, A.F.L.; Da Silva, G.P.; De Melo, M.L.R.; Napimoga, M.H.; Rodrigues, D.B.R.; Alves, P.M.; De Lima Pereira, S.A. Evaluation of Peri-Implant Mucosa: Clinical, Histopathological and Immunological Aspects. Arch. Oral Biol. 2014, 59, 470–478. [Google Scholar] [CrossRef]
- Borsani, E.; Salgarello, S.; Mensi, M.; Boninsegna, R.; Stacchiotti, A.; Rezzani, R.; Sapelli, P.; Bianchi, R.; Rodella, L.F. Histochemical and Immunohistochemical Evaluation of Gingival Collagen and Metalloproteinases in Peri-Implantitis. Acta Histochem. 2005, 107, 231–240. [Google Scholar] [CrossRef]
- Bullon, P.; Fioroni, M.; Goteri, G.; Rubini, C.; Battino, M. Immunohistochemical Analysis of Soft Tissues in Implants with Healthy and Peri-Implantitis Condition, and Aggressive Periodontitis. Clin. Oral Implant. Res. 2004, 15, 553–559. [Google Scholar] [CrossRef]
- Chaparro, A.; Sanz, A.; Wolnitzky, A.; Realini, O.; Bendek, M.J.; Betancur, D.; Albers, D.; Beltrán, V. Lymphocyte B and Th17 chemotacticcytokine levels in peri-implant crevicularfluid of patients with healthy, perimucositis, and peri-implantitis implants. J. Oral Res. 2020, 9, 20–25. [Google Scholar] [CrossRef]
- Scannapieco, F.A.; Ng, P.B.Y.; Hovey, K.; Hausmann, E.; Hutson, A.; WactawskiWende, J. Salivary biomarkers associated with alveolar bone loss. Ann. N. Y. Acad. Sci. 2007, 1098, 496–497. [Google Scholar] [CrossRef] [Green Version]
- Joseph, B.; Javali, M.A.; Khader, M.A.; AlQahtani, S.M.; Amanullah, M. Salivary Osteocalcin as Potential Diagnostic Marker of Periodontal Bone Destruction among Smokers. Biomolecules 2020, 110, 380. [Google Scholar] [CrossRef] [Green Version]
- Cakal, O.T.; Efeoglu, C.; Bozkurt, E. The evaluation of peri-implant sulcus fluid osteocalcin, osteopontin, and osteonectin levels in peri-implant diseases. J. Periodontol. 2018, 89, 418–423. [Google Scholar] [CrossRef]
- Lucarini, G.; Zizzi, A.; Rubini, C.; Ciolino, F.; Aspriello, S.D. VEGF, Microvessel Density, and CD44 as Inflammation Markers in Peri-implant Healthy Mucosa, Peri-implant Mucositis, and Peri-implantitis: Impact of Age, Smoking, PPD, and Obesity. Inflammation 2019, 42, 682–689. [Google Scholar] [CrossRef]
- Batista, A.C.; Rodini, C.O.; Lara, V.S. Quantification of mast cells in different stages of human periodontal disease. Oral Dis. 2005, 11, 249–254. [Google Scholar] [CrossRef]
- Lagdive, S.S.; Lagdive, S.B.; Mani, A.; Anarthe, R.; Pendyala, G.; Pawar, B.; Marawar, P.P. Correlation of mast cells in periodontal diseases. J. Indian Soc. Periodontol. 2013, 17, 63–67. [Google Scholar] [CrossRef]

{kind=link}
| Patients (n = 13) | |
|---|---|
| Sex (M:F) | 5:8 |
| Age (mean) | 60 |
| Smoking (not/yes) | 11:2 |
| Chronic Diseases (absent/present) | 8:5 |
| HTN | 4 |
| DM | 0 |
| HTN/DM | 1 |
| Implants (n = 21) | |
|---|---|
| BOP (−/+) | 0:21 |
| SOP (−/+) | 14:7 |
| Follow up (mean) | 38.5 |
| Location (mandibular/maxillar) | 11:10 |
| Type of abutment (cemented abutment/ball attachment) | 17:4 |
| APRIL (%) | BAFF (%) | Mast Cells | |
|---|---|---|---|
| Mean | 32.17 | 17.26 | 9.21 |
| Standard deviation | 6.39 | 12.90 | 2.86 |
| Minimum | 23.04 | 0.34 | 6 |
| Maximum | 47.69 | 41.89 | 18 |
| APRIL (%) | BAFF (%) | Osteonectin (%) | α-SMA (%) | Blood Vessels | Osteocytes | |
|---|---|---|---|---|---|---|
| Mean | 7.09 | 12.26 | 7.93 | 1.78 | 6.00 | 37.17 |
| Standard deviation | 5.94 | 6.30 | 3.79 | 0.718 | 2.708 | 10.420 |
| Minimum | 2 | 4 | 2 | 1 | 2 | 22 |
| Maximum | 17 | 19 | 13 | 2 | 8 | 53 |
| Variable 1 | Variable 2 | Value p |
|---|---|---|
| APRIL-ST a | BAFF-ST a | p = 0.001 * |
| APRIL-BT b | BAFF-BT b | p = 0.174 |
| OSTEONECTIN c | α-SMA c | p = 0.24 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flores, V.; Venegas, B.; Donoso, W.; Ulloa, C.; Chaparro, A.; Sousa, V.; Beltrán, V. Histological and Immunohistochemical Analysis of Peri-Implant Soft and Hard Tissues in Patients with Peri-Implantitis. Int. J. Environ. Res. Public Health 2022, 19, 8388. https://doi.org/10.3390/ijerph19148388
Flores V, Venegas B, Donoso W, Ulloa C, Chaparro A, Sousa V, Beltrán V. Histological and Immunohistochemical Analysis of Peri-Implant Soft and Hard Tissues in Patients with Peri-Implantitis. International Journal of Environmental Research and Public Health. 2022; 19(14):8388. https://doi.org/10.3390/ijerph19148388
Chicago/Turabian StyleFlores, Valentina, Bernardo Venegas, Wendy Donoso, Camilo Ulloa, Alejandra Chaparro, Vanessa Sousa, and Víctor Beltrán. 2022. "Histological and Immunohistochemical Analysis of Peri-Implant Soft and Hard Tissues in Patients with Peri-Implantitis" International Journal of Environmental Research and Public Health 19, no. 14: 8388. https://doi.org/10.3390/ijerph19148388
APA StyleFlores, V., Venegas, B., Donoso, W., Ulloa, C., Chaparro, A., Sousa, V., & Beltrán, V. (2022). Histological and Immunohistochemical Analysis of Peri-Implant Soft and Hard Tissues in Patients with Peri-Implantitis. International Journal of Environmental Research and Public Health, 19(14), 8388. https://doi.org/10.3390/ijerph19148388