
Exposure to Public Open Spaces and Leisure-Time Physical Activity: An Analysis of Adults in Primary Health Care in Brazil

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Characteristics, Local Contextualization, and Ethical Aspects
2.2. Sample Size, Number of Participants and Sample Power
2.3. Selection of Participants
2.4. Data Collectiom
2.5. Outcome Variable: Leisure-Time Physical Activity (LTPA)
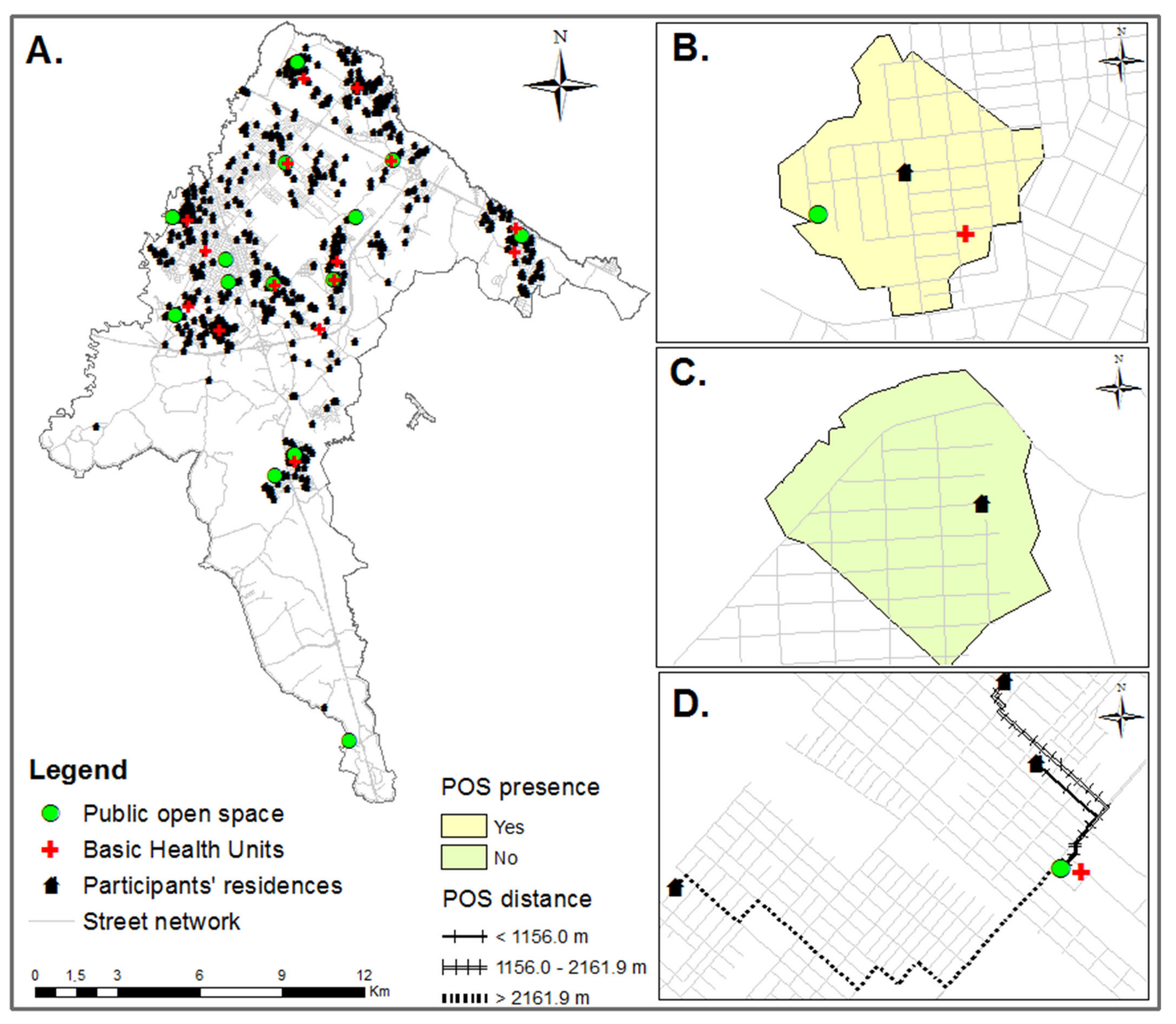
2.6. Predictors Variables: Exposure to Public Open Spaces (POS)
2.6.1. Presence of Public Open Spaces (POS)
2.6.2. Distance from Public Open Spaces (POS)
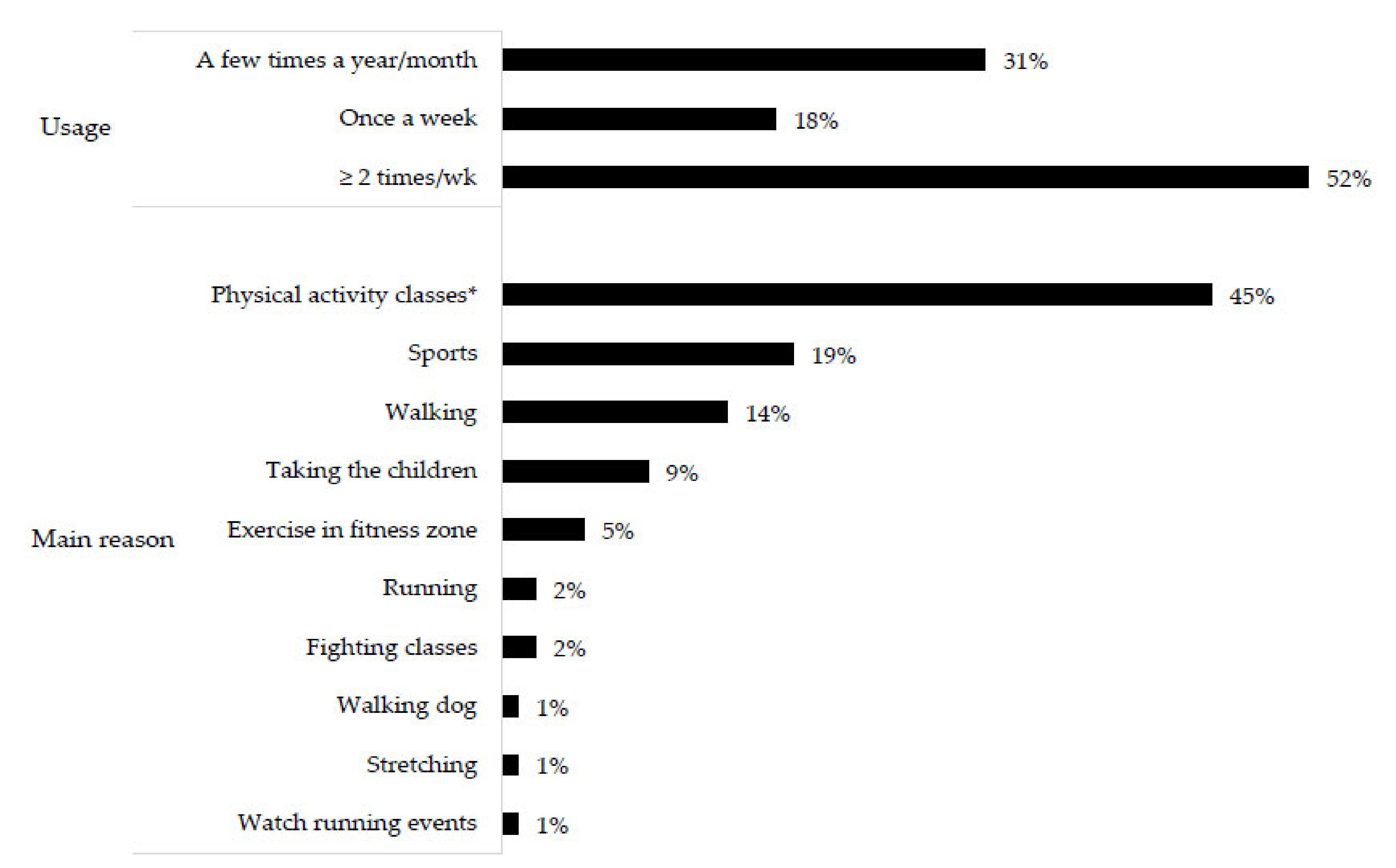
2.6.3. Public Open Spaces (POS) Usage
2.6.4. Frequency of Public Open Spaces (POS) Usage
2.7. Possible Confounders Variables
2.7.1. Sociodemographic Characteristics
2.7.2. Chronic Diseases
2.8. Data Quality Control
2.9. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health 2018, 6, 1077–1086. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Hallal, P.C.; Pratt, M. Physical activity: Moving from words to action. Lancet Glob. Health 2020, 8, e867–e868. [Google Scholar] [CrossRef]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Lancet Physical Activity Series Working Group. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Murray, C.J.L.; Aravkin, A.Y.; Zheng, P.; Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I.; et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Ding, D.; Lawson, K.D.; Kolbe-Alexander, T.L.; Finkelstein, E.A.; Katzmarzyk, P.T.; Van Mechelen, W.; Pratt, M.; Lancet Physical Activity Series 2 Executive Committee. The economic burden of physical inactivity: A global analysis of major non-communicable diseases. Lancet 2016, 388, 1311–1324. [Google Scholar] [CrossRef]
- Bielemann, R.M.; Silva, B.G.C.; Coll, C.V.N.; Xavier, M.O.; Silva, S.G. Burden of physical inactivity and hospitalization costs due to chronic diseases. Rev. Saude Publica 2015, 49, 75. [Google Scholar] [CrossRef]
- Paim, J.; Travassos, C.; Almeida, C.; Bahia, L.; MacInko, J. The Brazilian health system: History, advances, and challenges. Lancet 2011, 377, 1778–17797. [Google Scholar] [CrossRef]
- IBGE. Brazilian Institute of Geography and Statistics. National Health Survey 2019. Primary health care and anthropometric information. Available online: https://biblioteca.ibge.gov.br/visualizacao/livros/liv101748.pdf (accessed on 3 March 2022).
- Guibu, I.A.; Moraes, J.C.; Guerra Junior, A.A.; Costa, E.A.; Acurcio, F.A.; Costa, K.S.; Karnikowski, M.G.; Soeiro, O.M.; Leite, S.N.; Álvares, J. Main characteristics of patients of primary health care services in Brazil. Rev. Saude Publica 2017, 51, 1s–13s. [Google Scholar] [CrossRef]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.F.; Martin, B.W.; Lancet Physical Activity Series Working Group. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Sallis, J.F.; Bull, F.; Guthold, R.; Heath, G.W.; Inoue, S.; Kelly, P.; Oyeyemi, A.L.; Perez, L.G.; Richards, J.; Hallal, P.C. Progress in physical activity over the Olympic quadrennium. Lancet 2016, 38, 1325–1336. [Google Scholar] [CrossRef]
- Santos, L.P.; Silva, A.T.; Rech, C.R.; Fermino, R.C. Physical activity counseling among adults in Primary Health Care centers in Brazil. Int. J. Environ. Res. Public Health 2021, 18, 579. [Google Scholar] [CrossRef] [PubMed]
- Häfele, V.; Siqueira, F. Physical activity counseling and change of behavior in Basic Health Units. Rev. Bras. Ativ. Física Saúde 2016, 21, 581–592. [Google Scholar] [CrossRef]
- Hino, A.A.F.; Reis, R.S.; Sarmiento, O.L.; Parra, D.C.; Brownson, R.C. The built environment and recreational physical activity among adults in Curitiba, Brazil. Prev. Med. 2011, 52, 419–422. [Google Scholar] [CrossRef] [PubMed]
- Koohsari, M.J.; Mavoa, S.; Villianueva, K.; Sugiyama, T.; Badland, H.; Kaczynski, A.T.; Owen, N.; Giles-Corti, B. Public open space, physical activity, urban design and public health: Concepts, methods and research agenda. Health Place 2015, 33, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Elshahat, S.; O’Rorke, M.; Adlakha, D. Built environment correlates of physical activity in low-and middle-income countries: A systematic review. PLoS ONE 2020, 15, e0230454. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.; Ramirez-Varela, A.; Bauman, A.E.; Ekelund, U.; Lee, I.M.; Heath, G.; Katzmarzyk, P.T.; Reis, R.; Pratt, M. Towards better evidence-informed global action: Lessons learnt from the Lancet series and recent developments in physical activity and public health. Br. J. Sports Med. 2020, 54, 462–468. [Google Scholar] [CrossRef]
- Saelens, B.E.; Handy, S.L. Built environment correlates of walking: A review. Med. Sci. Sports Exerc. 2008, 40, s550–s566. [Google Scholar] [CrossRef]
- Fermino, R.C.; Reis, R.S. Individual, environmental and social variables associated with the use of public open spaces for physical activity practices: A systematic review. Rev. Bras. Ativ. Física Saúde 2013, 18, 523–535. [Google Scholar] [CrossRef][Green Version]
- McCormack, G.R.; Shiell, A. In search of causality: A systematic review of the relationship between the built environment and physical activity among adults. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 125. [Google Scholar] [CrossRef]
- Sugiyama, T.; Francis, J.; Middleton, N.J.; Owen, N.; Giles-Corti, B. Associations between recreational walking and attractiveness, size, and proximity of neighborhood open spaces. Am. J. Public Health 2010, 100, 1752–1757. [Google Scholar] [CrossRef] [PubMed]
- Cerin, E.; Vandelanotte, C.; Leslie, E.; Merom, D. Recreational facilities and leisure-time physical activity: An analysis of moderators and self-efficacy as a mediator. Health Psychol. 2008, 27, s126–s135. [Google Scholar] [CrossRef]
- Bedimo-Rung, A.L.; Mowen, A.J.; Cohen, D.A. The significance of parks to physical activity and public health: A conceptual model. Am. J. Prev. Med. 2005, 28, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Kajosaari, A.; Laatikainen, T.E. Adults’ leisure-time physical activity and the neighborhood built environment: A contextual perspective. Int. J. Health Geogr. 2020, 19, 35. [Google Scholar] [CrossRef] [PubMed]
- Koohsari, M.J. Access to public open space: Is distribution equitable across different socio-economic areas. J. Urban Env. Eng. 2011, 5, 67–72. [Google Scholar] [CrossRef]
- Manta, S.W.; Reis, R.S.; Benedetti, T.R.B.; Rech, C.R. Public open spaces and physical activity: Disparities of resources in Florianopolis. Rev. Saúde Pública 2019, 53, 112. [Google Scholar] [CrossRef]
- Silva, I.C.M.; Mielke, G.I.; Nunes, B.P.; Böhm, A.W.; Blanke, A.O.; Nachtigall, M.S. Public open spaces in Pelotas (Brazil): Distribution, quality and suitability for physical activity practice. Rev. Bras. Ativ. Física Saúde 2015, 31, 82–92. [Google Scholar] [CrossRef]
- Custódio, I.G. Quality of Sport and Leisure Centers and its association with the profile and physical activity level of the users in São José dos Pinhais, Paraná. Federal University of Technological–Paraná: Curitiba, Brazil, 2019. Available online: https://repositorio.utfpr.edu.br/jspui/handle/1/4382 (accessed on 19 December 2021).
- Vieira, M.C.; Sperandei, S.; Reis, A.; Silva, C.G.T. An analysis of the suitability of public spaces to physical activity practice in Rio de Janeiro, Brazil. Prev. Med. 2013, 57, 198–200. [Google Scholar] [CrossRef]
- Florindo, A.A.; Barrozo, L.V.; Cabral-Miranda, W.; Rodrigues, E.Q.; Turrell, G.; Goldbaum, M.; Cesar, C.L.G.; Giles-Corti, B. Public open spaces and leisure-time walking in Brazilian adults. Int. J. Env. Res. Public Health. 2017, 14, 553. [Google Scholar] [CrossRef]
- Custódio, I.G.; Lopes, A.A.S.; Kopp, D.; Silva, A.T.; Chaves, R.N.; Rodriguez-Añez, C.R.; Fermino, R.C. Pattern of use of public open spaces and physical activity levels in São José dos Pinhais, Brazil. Rev. Bras. Ciênc. Esporte. 2021, 43, e011220. [Google Scholar] [CrossRef]
- Hino, A.A.F.; Reis, R.S.; Ribeiro, I.C.; Parra, D.C.; Brownson, R.C.; Fermino, R.C. Using observational methods to evaluate public open spaces and physical activity in Brazil. J. Phys. Act. Health. 2010, 7 (Suppl. S2), S146–S154. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.T.; Santos, L.P.; Rodriguez-Añez, C.R.; Fermino, R.C. Logic model of “Cidade Ativa, Cidade Saudável Program” in São José dos Pinhais, Brazil. Rev. Bras. Ativ. Física Saúde 2021, 26, 1–6. [Google Scholar] [CrossRef]
- Reis, R.S.; Yan, Y.; Parra, D.C.; Brownson, R.C. Assessing participation in community-based physical activity programs in Brazil. Med. Sci. Sports Exerc. 2014, 46, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Heath, G.W.; Parra, D.C.; Sarmiento, O.L.; Andersen, L.B.; Owen, N.; Goenka, S.; Montes, F.; Brownson, R.C.; the Lancet Physical Activity Series Working Group. Evidence-based intervention in physical activity: Lessons from around the world. Lancet 2012, 380, 272–281. [Google Scholar] [CrossRef]
- Milton, K.; Cavill, N.; Chalkley, A.; Foster, C.; Gomersall, S.; Hagstromer, M.; Kelly, P.; Kolbe-Alexander, T.; Mair, J.; McLaughlin, M.; et al. Eight investments that work for physical activity. J. Phys. Act. Health 2021, 18, 625–630. [Google Scholar] [CrossRef]
- Umpierre, D.; Coelho-Ravagnani, C.; Tenório, M.C.; Andrade, D.R.; Autran, R.; Barros, M.V.G.; Benedetti, T.R.B.; Cavalcante, F.V.S.A.; Cyrino, E.S.; Dumith, S.C.; et al. Physical activity guidelines for the Brazilian population: Recommendations report. J. Phys. Act. Health 2022, 19, 374–381. [Google Scholar] [CrossRef]
- Vandenbrouck, J.P.; Von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Epidemiology 2007, 18, 805–835. [Google Scholar] [CrossRef]
- IBGE. Brazilian Institute of Geography and Statistics. Synthesis of Social Indicators: An Analysis of the Living Conditions of the Brazilian Population 2021. Available online: https://www.ibge.gov.br/estatisticas/multidominio/genero/9221-sintese-de-indicadores-sociais.html?=&t=resultados (accessed on 20 January 2022).
- IPARDES. Paraná Institute for Economic and Social Development. Statistical Reports of São José dos Pinhais. Available online: http://www.ipardes.gov.br/cadernos/MontaCadPdf1.php?Municipio=83000&btOk=ok (accessed on 15 February 2022).
- IBGE. Brazilian Institute of Geography and Statistics. Cidades@. Available online: https://cidades.ibge.gov.br/ (accessed on 20 April 2022).
- INEGI. National Institute of Statistics, Geography and Informatics. Population and Housing Census 2020. Available online: https://www.inegi.org.mx/programas/ccpv/2020/ (accessed on 10 April 2022).
- DANE. National Administrative Department of Statistics. National Population and Housing Census. Available online: https://sitios.dane.gov.co/cnpv/#!/ (accessed on 20 April 2022).
- Luiz, R.R.; Magnanini, M.M.F. The logic of sample size determination in epidemiological research. Cad Saúde Colet 2000, 8, 9–28. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Bowling, A. Mode of questionnaire administration can have serious effects on data quality. J. Public Health 2005, 27, 281–291. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Matsudo, S.; Araujo, T.; Matsudo, V.; Andrade, D.; Andrade, E.; Oliveira, L.C.; BRaggion, G. International Physical Activity Questionnaire (IPAQ): Validity and reproducibility study in Brazil. Rev. Bras. Ativ. Física Saúde 2001, 6, 5–18. [Google Scholar] [CrossRef]
- Hallal, P.C.; Gomez, L.F.; Parra, D.C.; Lobelo, F.; Mosquera, J.; Florindo, A.A.; Reis, R.; Pratt, M.; Sarmiento, O.L. Lessons learned after 10 years of IPAQ use in Brazil and Colombia. J. Phys. Act. Health 2010, 7, s259–s264. [Google Scholar] [CrossRef] [PubMed]
- Fermino, R.C.; Hallal, P.C.; Reis, R.S. Frequecy of park use and physical activity in adults from Curitiba, Brazil. Rev. Bras. Med. Esporte. 2017, 23, 264–269. [Google Scholar] [CrossRef]
- Schipperijn, J.; Cerin, E.; Adams, M.A.; Reis, R.; Smith, G.; Cain, K.; Christiansen, L.B.; van Dyck, D.; Gidlow, C.; Frank, L.D.; et al. Access to parks and physical activity: An eight country comparison. Urban For. Urban Green. 2017, 27, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Moran, M.R.; Rodríguez, D.A.; Cotinez-O’Ryan, A.; Miranda, J.J. Park use, perceived park proximity, and neighborhood characteristics: Evidence from 11 cities in Latin America. Cities 2020, 105, 102817. [Google Scholar] [CrossRef]
- Rech, C.R.; Camargo, E.M.; Araujo, P.A.B.; Loch, M.R.; Reis, R.S. Perceived barriers to leisure-time physical activity in the Brazilian population. Rev. Bras. Med. Esporte. 2018, 24, 303–309. [Google Scholar] [CrossRef]
- Fermino, R.C.; Reis, R.S.; Hallal, P.C.; Kaczynski, A.T. Who are the users of urban parks? A study with adults from Curitiba, Brazil. J. Phys. Act. Health 2015, 12, 58–67. [Google Scholar] [CrossRef]
- Veitch, J.; Ball, K.; Crawford, D.; Abbott, G.; Salmon, J. Is park visitation associated with leisure-time and transportation physical activity? Prev. Med. 2013, 57, 732–734. [Google Scholar] [CrossRef]
- Fermino, R.C.; Reis, R.S.; Hallal, P.C.; Farias Júnior, J.C. Perceived environment and public open space use: A study with adults from Curitiba, Brazil. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 1–10. [Google Scholar] [CrossRef]
- ABEP. Brazilian Association of Research Companies. Brazil economic classification criteria 2019. Available online: http://www.abep.org/criterio-brasil (accessed on 2 May 2020).
- Fonseca, M.J.M.; Faerstein, E.; Chor, D.; Lopes, C.S. Validity of self-reported weight and height and the body mass index within the “Pró-saúde” study. Rev. Saúde Pública. 2004, 38, 1–7. [Google Scholar] [CrossRef]
- WHO. World Health Organization expert committee on physical status: The use and interpretation of anthropometry. Report of a WHO expert committee. Available online: https://www.who.int/childgrowth/publications/physical_status/en/ (accessed on 17 April 2022).
- Brasil. Ministry of Health, Secretariat of Health Surveillance. Department of Health Analysis and Surveillance of Noncommunicable Diseases. VIGITEL Brasil 2021: Surveillance System for Risk and Protective Factors for Chronic Diseases by Telephone Survey. Brasilia-DF; 2022. Available online: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/publicacoes-svs/vigitel/relatorio-vigitel-2020-original.pdf/view (accessed on 28 March 2022).
- Barros, A.J.D.; Hirakata, V.N. Alternatives for logistic regression in cross-sectional studies: An empirical comparison of models that directly estimate the prevalence ratio. BMC Med. Res. Methodol. 2003, 3, 21. [Google Scholar] [CrossRef] [PubMed]
- Merlo, J.; Chaix, B.; Yang, M.; Lynch, J.; Rastam, L. A brief conceptual tutorial of multilevel analysis in social epidemiology: Linking the statistical concept of clustering to the idea of contextual phenomenon. J. Epidemiol. Community Health 2005, 59, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Sommet, N.; Morselli, D. Keep calm and learn multilevel logistic modeling: A simplified three-step procedure using Stata, R, Mplus, and SPSS. Int. Rev. Soc. Psychol. 2017, 30, 203–218. [Google Scholar] [CrossRef]
- United Nations, Department of Economic and Social Affairs, Population Division. The World’s Cities in 2016. 2016. Available online: https://digitallibrary.un.org/record/1634928 (accessed on 1 March 2022).
- Aliyas, Z. Built environment correlates of walking for recreation or exercise. J. Public Health 2019, 27, 349–356. [Google Scholar] [CrossRef]
- Chaix, B.; Simon, C.; Charreire, H.; Thomas, F.; Kestens, Y.; Karusisi, N.; Vallée, J.; Oppert, J.-M.; Weber, C.; Pannier, B. The environmental correlates of overall and neighborhood based recreational walking (a cross-sectional analysis of the RECORD Study). Int. J. Behav. Nutr. Phys. Act. 2014, 11, 20. [Google Scholar] [CrossRef]
- McCormack, G.R.; Giles-Corti, B.; Bulsara, M. The relationship between destination proximity, destination mix and physical activity behaviors. Prev. Med. 2008, 46, 33–40. [Google Scholar] [CrossRef]
- Paluch, A.E.; Bajpai, S.; Bassett, D.R.; Carnethon, M.R.; Ekelund, U.; Evenson, K.R.; Galuska, A.D.; Jefferis, B.J.; Kraus, E.W.; Lee, I.-M.; et al. Daily steps and all-cause mortality: A meta-analysis of 15 international cohorts. Lancet Public Health 2022, 7, e219–e228. [Google Scholar] [CrossRef]
- Smith, B.J.; MacKenzie-Stewart, R.; Newton, F.J.; Haregu, T.N.; Bauman, A.; Donovan, R.J.; Mahal, A.; Ewing, M.T.; Newton, J.D. A longitudinal study examining uptake of new recreation infrastructure by inactive adults. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 59. [Google Scholar] [CrossRef]
- Veitch, J.; Rodwell, L.; Abbott, G.; Carver, A.; Flowers, E.; Crawford, D. Are park availability and satisfaction with neighbourhood parks associated with physical activity and time spent outdoors? BMC Public Health 2021, 21, 1–10. [Google Scholar] [CrossRef]
- Mackenbach, J.D.; Matias de Pinho, M.G.; Faber, E.; Den Braver, N.; Groot, R.; Charreire, H.; Oppert, J.-M.; Bárdos, H.; Rutter, H.; Compernolle, S.; et al. Exploring the cross-sectional association between outdoor recreational facilities and leisure-time physical activity: The role of usage and residential self-selection. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 55. [Google Scholar] [CrossRef] [PubMed]
- Salvo, D.; Sarmiento, O.L.; Reis, R.S.; Hino, A.A.F.; Bolivar, M.A.; Lemoine, P.D.; Gonçalves, P.B.; Pratt, M. Where Latin Americans are physically active, and why does it matter? findings from the IPEN-adult study in Bogota, Colombia; Cuernavaca, Mexico; and Curitiba, Brazil. Prev. Med. 2017, 3, S27–S33. [Google Scholar] [CrossRef] [PubMed]
- Souza, A.L.K.; Santos, L.P.; Rech, C.R.; Rodriguez-Añez, C.R.; Alberico, C.O.; Borges, L.J.; Fermino, R.C. Barriers for physical activity in adults at Primary Healthcare Units in the Unified Health System: A cross-sectional study in Brazil. São Paulo Med. J. 2022. no prelo. [Google Scholar]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 compendium of physical activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Saelens, B.E. Assessment of physical activity by self-report: Status, limitations, and future directions. Res. Q. Exerc Sport. 2000, 71 (Suppl. S2), 1–14. [Google Scholar] [CrossRef] [PubMed]
- Bancroft, C.; Joshi, S.; Rundle, A.; Hutson, M.; Chong, C.; Weiss, C.C.; Genkinger, J.; Neckerman, K.; Lovasi, G. Association of proximity and density of parks and objectively measured physical activity in the United States: A systematic review. Soc. Scie. Med. 2015, 138, 22–30. [Google Scholar] [CrossRef]
- Dowd, K.; Maciaszek, J.; van der Ploeg, H.; Minetto, M.; Murphy, M.; Polito, A.; Szeklicki, R.; Ghigo, E.; Ekelund, U.; Stemplewski, R.; et al. A systematic literature review of reviews on techniques for physical activity measurement in adults: A DEDIPAC study. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 15. [Google Scholar] [CrossRef]
- Laporte, R.E.; Montoye, H.J.; Caspersen, C.J. Assessment of physical activity in epidemiologic research: Problems and prospects. Public Health Rep. 1985, 100, 131–146. [Google Scholar]



{kind=link}
{kind=link}
| Variable | Category | n | % | Average | S.D. |
|---|---|---|---|---|---|
| Sociodemographic | |||||
| Sex | Male | 163 | 26.5 | - | - |
| Female | 452 | 73.5 | - | - | |
| Age (years) | 18–39.9 | 334 | 54.3 | 38.4 | 12.4 |
| 40–59.9 | 281 | 45.7 | |||
| Marital status | Single | 220 | 35.8 | - | - |
| Married | 395 | 64.2 | - | - | |
| Skin color | White | 450 | 73.5 | - | - |
| Non-white | 162 | 26.5 | - | - | |
| Economic level | Low | 430 | 69.9 | - | - |
| High | 185 | 30.1 | - | - | |
| Chronic diseases | |||||
| Overweight | No | 196 | 32.2 | 27.7 | 5.2 |
| Yes | 413 | 67.8 | |||
| Hypertension | No | 440 | 71.5 | - | - |
| Yes | 175 | 28.5 | - | - | |
| Circulatory disease | No | 533 | 86.7 | - | - |
| Yes | 82 | 13.3 | - | - | |
| Dyslipidemia | No | 539 | 87.6 | - | - |
| Yes | 76 | 12.4 | - | - | |
| Diabetes | No | 540 | 87.8 | - | - |
| Yes | 75 | 12.2 | - | - | |
| Lung disease | No | 580 | 94.3 | - | - |
| Yes | 35 | 5.7 | - | - | |
| Coronary artery disease | No | 585 | 95.1 | - | - |
| Yes | 30 | 4.9 | - | - | |
| Number of chronic diseases * | 0 | 141 | 22.9 | 1.4 | 1.2 |
| 1 | 236 | 38.4 | |||
| ≥2 | 238 | 38.7 | |||
| Leisure time physical activity | |||||
| Walking | 0–9 min/week | 463 | 75.3 | 43.2 | 106.9 |
| ≥10 min/week | 152 | 24.7 | |||
| 0–149 min/week | 543 | 88.3 | |||
| ≥150 min/week | 72 | 11.7 | |||
| MVPA | 0–9 min/week | 484 | 78.7 | 72.4 | 215.8 |
| ≥10 min/week | 131 | 21.3 | |||
| 0–149 min/week | 530 | 86.2 | |||
| ≥150 min/week | 85 | 13.8 | |||
| Public open space exposure ** | |||||
| Presence *** | No | 552 | 89.8 | - | - |
| Yes | 63 | 10.2 | - | - | |
| Distance | <1156 m | 201 | 33.3 | 1880.7 | 1494.8 |
| 1156–2161 m | 202 | 33.4 | |||
| ≥2162 m (3rd tertile) | 201 | 33.3 | |||
| Usage | No | 518 | 84.2 | - | - |
| Yes | 97 | 15.8 | - | - | |
| Frequency of usage | No use | 518 | 84.2 | - | - |
| A few times a year/month | 30 | 4.9 | - | - | |
| Once a week | 17 | 2.8 | - | - | |
| ≥2 times/week | 50 | 8.1 | - | - | |
| Walking ≥ 10 min/week | Walking ≥ 150 min/week | MVPA ≥ 10 min/week | MVPA ≥ 150 min/week | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % | PR | 95% CI | p | % | PR | 95% CI | p | % | PR | 95% CI | p | % | PR | 95% CI | p | |
| Sex | ||||||||||||||||
| Male | 24.5 | 1 | 0.952 h | 12.9 | 1 | 0.585 h | 29.4 | 1 | 0.003 h | 17.2 | 1 | 0.145 h | ||||
| Female | 24.8 | 1.01 | 0.74–1.38 | 11.3 | 0.88 | 0.54–1.41 | 18.4 | 0.62 | 0.46–0.85 | 12.0 | 0.73 | 0.48–1.11 | ||||
| Age (years) | ||||||||||||||||
| 18–39.9 | 19.5 | 1 | <0.001 h | 8.4 | 1 | 0.006 h | 22.5 | 1 | 0.447 h | 14.4 | 1 | 0.667 h | ||||
| 40–59.9 | 31.0 | 1.59 | 1.20–2.10 | 15.7 | 1.87 | 1.19–2.92 | 19.9 | 0.89 | 0.65–1.21 | 13.2 | 0.92 | 0.61–1.36 | ||||
| Marital status | ||||||||||||||||
| Single | 23.2 | 1 | 0.513 h | 10.9 | 1 | 0.647 h | 22.7 | 1 | 0.518 h | 14.5 | 1 | 0.697 h | ||||
| Married | 25.6 | 1.10 | 0.82–1.48 | 12.2 | 1.11 | 0.70–1.77 | 20.5 | 0.90 | 0.66–1.23 | 13.4 | 0.92 | 0.61–1.39 | ||||
| Skin color | ||||||||||||||||
| White | 25.3 | 1 | 0.531 h | 11.8 | 1 | 0.987 h | 21.6 | 1 | 0.753 h | 14.0 | 1 | 0.895 h | ||||
| Non-white | 22.8 | 0.90 | 0.65–1.25 | 11.7 | 1.00 | 0.61–1.63 | 20.4 | 0.95 | 0.66–1.34 | 13.6 | 0.97 | 0.62–1.52 | ||||
| Economic level | ||||||||||||||||
| Low | 22.6 | 1 | 0.055 h | 10.0 | 1 | 0.044 h | 18.4 | 1 | 0.006 h | 11.6 | 1 | 0.016 h | ||||
| High | 29.7 | 1.32 | 0.99–1.75 | 15.7 | 1.57 | 1.01–2.43 | 28.1 | 1.53 | 1.13–2.07 | 18.9 | 1.63 | 1.10–2.42 | ||||
| Number of chronic diseases * | ||||||||||||||||
| 0 | 20.6 | 1 | 0.001 t | 8.5 | 1 | 0.012 t | 26.2 | 1 | 0.210 t | 15.6 | 1 | 0.836 t | ||||
| 1 | 16.9 | 0.82 | 0.54–1.27 | 8.5 | 1.00 | 0.50–1.97 | 18.6 | 0.71 | 0.48–1.04 | 12.3 | 0.79 | 0.47–1.32 | ||||
| ≥2 | 34.9 | 1.70 | 1.17–2.45 | 16.8 | 1.98 | 1.07–3.64 | 21.0 | 0.80 | 0.55–1.16 | 14.3 | 0.92 | 0.56–1.50 | ||||
| Walking ≥ 10 min/week | Walking ≥ 150 min/week | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bivariate Analysis | Multivariate Analysis * | Bivariate Analysis | Multivariate Analysis * | |||||||||||
| % | PR | 95% CI | p | PR | 95% CI | p | % | PR | 95% CI | p | PR | 95% CI | p | |
| Presence | ||||||||||||||
| No | 23.9 | 1 | 0.237 h | - | - | - | 10.9 | 1 | 0.076 h | 1 | 0.065 h | |||
| Yes | 31.7 | 1.33 | 0.80–2.10 | - | - | - | 19.0 | 1.75 | 0.90–3.14 | 1.79 | 0.92–3.21 | |||
| 0.011 (0.003) # | - | - | - | 0.000 (0.000) # | 0.000 (0.000) # | |||||||||
| Distance | ||||||||||||||
| <1156 m | 26.4 | 1 | 0.699 t | - | - | - | 13.9 | 1 | 0.189 t | - | - | - | ||
| 1156–2161 m | 22.3 | 0.85 | 0.57–1.26 | - | - | - | 11.4 | 0.82 | 0.47–1.42 | - | - | - | ||
| ≥2162 m | 24.4 | 0.93 | 0.63–1.40 | - | - | - | 9.5 | 0.68 | 0.37–1.21 | - | - | - | ||
| 0.003 (0.001) # | - | - | - | 0.000 (0.000) # | - | - | - | |||||||
| Usage | ||||||||||||||
| No | 22.8 | 1 | 0.027 h | 1 | 0.031 h | 10.8 | 1 | 0.136 h | - | - | - | |||
| Yes | 35.1 | 1.54 | 1.04–2.23 | 1.52 | 1.02–2.21 | 16.5 | 1.53 | 0.85–2.59 | - | - | - | |||
| 0.010 (0.003) # | 0.000 (0.000) # | 0.000 (0.000) # | - | - | - | |||||||||
| Frequency of usage | ||||||||||||||
| No use | 22.8 | 1 | <0.001 t | 1 | <0.001 t | 10.8 | 1 | 0.047 t | 0.076 t | |||||
| A few times a year/month | 20.0 | 0.88 | 0.34–1.84 | 0.95 | 0.37–1.97 | 10.0 | 0.93 | 0.23–2.50 | 1.02 | 0.25–2.79 | ||||
| Once a week | 17.6 | 0.77 | 0.19–2.05 | 0.84 | 0.21–2.23 | 11.8 | 1.09 | 0.18–3.49 | 1.14 | 0.19–3.69 | ||||
| ≥2 times/week | 50.0 | 2.20 | 1.39–3.32 | 2.01 | 1.28–3.05 | 22.0 | 2.04 | 1.01–3.73 | 1.85 | 0.92–3.41 | ||||
| 0.007 (0.002) # | 0.000 (0.000) # | 0.000 (0.000) # | 0.000 (0.000) # | |||||||||||
| MVPA ≥ 10 min/week | MVPA ≥ 150 min/week | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bivariate Analysis | Multivariate Analysis * | Bivariate Analysis | Multivariate Analysis § | |||||||||||
| % | PR | 95% CI | p | PR | 95% CI | p | % | PR | 95% CI | p | PR | 95% CI | p | |
| Presence | ||||||||||||||
| No | 20.7 | 1 | 0.279 h | - | - | - | 13.9 | 1 | 0.800 h | - | - | - | ||
| Yes | 27.0 | 1.34 | 0.77–2.20 | - | - | - | 12.7 | 0.91 | 0.40–1.80 | - | - | - | ||
| 0.019 (0.006) # | - | - | - | 0.000 (0.000) # | - | - | - | |||||||
| Distance | ||||||||||||||
| <1156 m | 20.9 | 1 | 0.797 t | - | - | - | 13.9 | 1 | 0.893 t | - | - | - | ||
| 1156–2161 m | 19.3 | 0.92 | 0.63–1.36 | - | - | - | 12.9 | 0.92 | 0.53–1.58 | - | - | - | ||
| ≥2162 m | 22.9 | 1.06 | 0.67–1.65 | - | - | - | 14.4 | 1.04 | 0.59–1.75 | - | - | - | ||
| 0.017 (0.005) # | - | - | - | 0.000 (0.000) # | - | - | - | |||||||
| Usage | ||||||||||||||
| No | 16.8 | 1 | <0.001 h | 1 | <0.001 h | 10.4 | 1 | <0.001 h | 1 | <0.001 h | ||||
| Yes | 45.4 | 2.85 | 1.96–4.13 | 2.73 | 1.86–3.97 | 32.0 | 3.13 | 1.97–4.89 | 3.03 | 1.92–4.74 | - | |||
| 0.054 (0.016) # | 0.047 (0.014) # | 0.026 (0.008) # | 0.008 (0.002) # | |||||||||||
| Frequency of usage | ||||||||||||||
| No use | 16.8 | 1 | <0.001 t | 1 | <0.001 t | 10.4 | 1 | <0.001 t | 1 | <0.001 t | ||||
| A few times a year/month | 33.3 | 2.09 | 1.01–3.89 | 1.77 | 0.84–3.35 | 20.0 | 1.95 | 0.75–4.24 | 1.76 | 0.67–3.85 | ||||
| Once a week | 47.1 | 2.87 | 1.27–5.96 | 2.58 | 1.14–5.07 | 35.3 | 3.45 | 1.32–7.48 | 3.15 | 1.21–6.82 | ||||
| ≥2 times/week | 52.0 | 3.31 | 2.06–5.16 | 3.45 | 2.14–5.42 | 38.0 | 3.71 | 2.12–6.21 | 3.81 | 2.19–6.38 | ||||
| 0.056 (0.0017) # | 0.046 (0.014) # | 0.024 (0.007) # | 0.000 (0.000) # | |||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mello, R.L.d.; Lopes, A.A.d.S.; Fermino, R.C. Exposure to Public Open Spaces and Leisure-Time Physical Activity: An Analysis of Adults in Primary Health Care in Brazil. Int. J. Environ. Res. Public Health 2022, 19, 8355. https://doi.org/10.3390/ijerph19148355
Mello RLd, Lopes AAdS, Fermino RC. Exposure to Public Open Spaces and Leisure-Time Physical Activity: An Analysis of Adults in Primary Health Care in Brazil. International Journal of Environmental Research and Public Health. 2022; 19(14):8355. https://doi.org/10.3390/ijerph19148355
Chicago/Turabian StyleMello, Rafael Luciano de, Adalberto Aparecido dos Santos Lopes, and Rogério César Fermino. 2022. "Exposure to Public Open Spaces and Leisure-Time Physical Activity: An Analysis of Adults in Primary Health Care in Brazil" International Journal of Environmental Research and Public Health 19, no. 14: 8355. https://doi.org/10.3390/ijerph19148355
APA StyleMello, R. L. d., Lopes, A. A. d. S., & Fermino, R. C. (2022). Exposure to Public Open Spaces and Leisure-Time Physical Activity: An Analysis of Adults in Primary Health Care in Brazil. International Journal of Environmental Research and Public Health, 19(14), 8355. https://doi.org/10.3390/ijerph19148355