
Physical Activity in Pulmonary Arterial Hypertension during Pandemic COVID-19 and the Potential Impact of Mental Factors


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Methods
2.3. Statistical Analysis
3. Results
3.1. Study Group
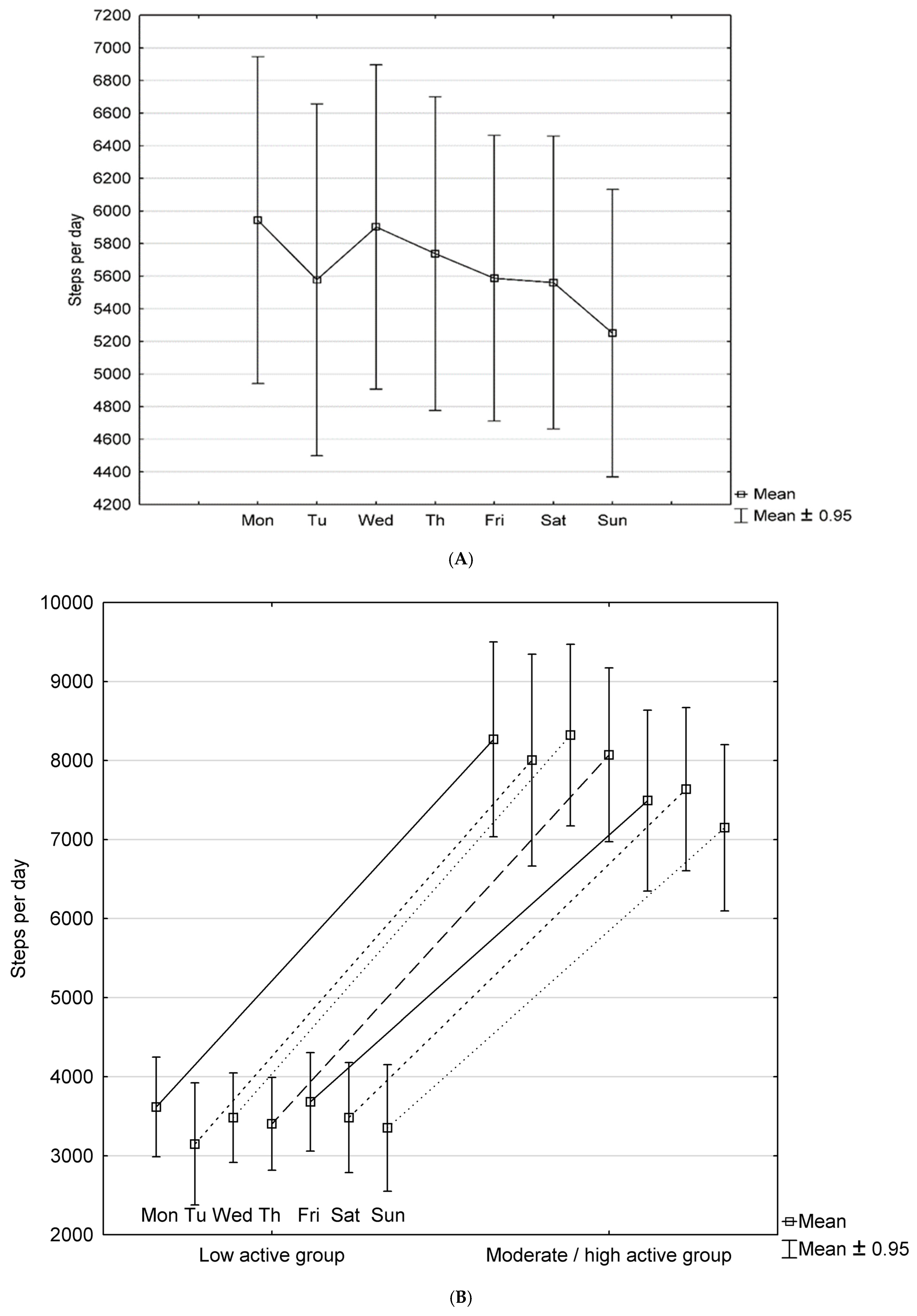
3.2. Physical Activity in Study Group
3.3. Fear of COVID-19, Anxiety and Depression and Quality of Life in Study Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Galie, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Noordegraaf, A.V.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The joint task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Heart J. 2016, 37, 67–119. [Google Scholar] [CrossRef]
- Saxer, S.; Lichtblau, M.; Berlier, C.; Hasler, E.D.; Schwarz, E.I.; Ulrich, S. Physical activity in incident patients with pulmonary arterial and chronic thromboembolic hypertension. Lung 2019, 197, 617–625. [Google Scholar] [CrossRef]
- Matura, L.A.; Shou, H.; Fritz, J.S.; Smith, K.A.; Vaidya, A.; Pinder, D.; Archer-Chicko, C.; Dubow, D.; Palevsky, H.I.; Sommers, M.S.; et al. Physical activity and symptoms in pulmonary arterial hypertension. Chest 2016, 150, 46–56. [Google Scholar] [CrossRef] [Green Version]
- Grünig, E.; Eichstaedt, C.; Barberà, J.-A.; Benjamin, N.; Blanco, I.; Bossone, E.; Cittadini, A.; Coghlan, G.; Corris, P.; D’Alto, M.; et al. ERS statement on exercise training and rehabilitation in patients with severe chronic pulmonary hypertension. Eur. Respir. J. 2019, 53, 1800332. [Google Scholar] [CrossRef] [Green Version]
- Grünig, E.; MacKenzie, A.; Peacock, A.J.; Eichstaedt, C.A.; Benjamin, N.; Nechwatal, R.; Ulrich, S.; Saxer, S.; Bussotti, M.; Sommaruga, M.; et al. Standardized exercise training is feasible, safe, and effective in pulmonary arterial and chronic thromboembolic pulmonary hypertension: Results from a large European multicentre randomized controlled trial. Eur. Heart J. 2021, 42, 2284–2295. [Google Scholar] [CrossRef]
- Hemnes, A.R.; Silverman-Lloyd, L.G.; Huang, S.; MacKinnon, G.; Annis, J.; Whitmore, C.S.; Mallugari, R.; Oggs, R.N.; Hekmat, R.; Shan, R.; et al. A Mobile health intervention to increase physical activity in pulmonary arterial hypertension. Chest 2021, 160, 1042–1052. [Google Scholar] [CrossRef]
- Nakazato, L.; Mendes, F.; Paschoal, I.A.; Oliveira, D.C.; Moreira, M.M.; Pereira, M.C. Association of daily physical activity with psychosocial aspects and functional capacity in patients with pulmonary arterial hypertension: A cross-sectional study. Pulm. Circ. 2021, 11, 1–9. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Mchorney, C.A.; Ware, J.E., Jr.; Raczek, A.E. The MOS 36-item short-form health survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Med. Care 1993, 31, 247–263. [Google Scholar] [CrossRef] [Green Version]
- Ahorsu, D.K.; Lin, C.-Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The fear of COVID-19 Scale: Development and initial validation. Int. J. Ment. Health Addict. 2020, 20, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Pisula, E.; Nowakowska, I. Skala Lęku przed Koronawirusem FCV-19S (Ahorsu I in., 2020)–Polskie Tłumaczenie, 2020. OSF. 2020. Available online: https://OSF.IO/39JR8 (accessed on 2 June 2022).
- Pilch, I.; Kurasz, Z.; Turska-Kawa, A. Experiencing fear during the pandemic: Validation of the fear of COVID-19 scale in Polish. PeerJ 2021, 9, e11263. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatry Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Wichowicz, H.M.; Wieczorek, D. Screening post-stroke depression using the hospital anxiety and depression scale. Psychiatr. Polska 2011, 45, 505–514. [Google Scholar]
- Juczyński, Z. Acceptance of Ilness scale-AIS. Measurement Tools in the Promotion and Psychology of Health; Laboratory of Psychological Tests of the Polish Psychological Association: Warsaw, Poland, 2012; pp. 162–165. [Google Scholar]
- Rogon, I.; Kasprzak, Z.; Szcześniak, L. Perceived quality of life and acceptance of illness in people with type 2 diabetes mellitus. Menopausal Rev. 2017, 3, 79–85. [Google Scholar] [CrossRef] [Green Version]
- Omron. Instruction Manual 2012. Pedometer Model: HJ-321. Available online: https://omronhealthcare.com/wp-content/uploads/HJ-321-IM-WEB-03212012.pdf (accessed on 31 December 2021).
- Huang, Y.; Xu, J.; Yu, B.; Shull, P.B. Validity of FitBit, Jawbone UP, Nike+ and other wearable devices for level and stair walking. Gait Posture 2016, 48, 36–41. [Google Scholar] [CrossRef]
- Sampaio, L.M.; Subramaniam, S.; Arena, R.; Bhatt, T. Does virtual reality-based kinect dance training paradigm improve autonomic nervous system modulation in individuals with chronic stroke? J. Vasc. Interv. Neurol. 2016, 9, 21–29. [Google Scholar]
- Marvin-Peek, J.; Hemnes, A.; Huang, S.; Silverman-Loyd, L.; MacKinnon, G.; Annis, J.; Martin, S.S.; Blaha, M.J.; Brittain, E.L. Daily step counts are associated with hospitalization risk in pulmonary arterial hypertension. Am. J. Respir. Crit. Care Med. 2021, 204, 1338–1340. [Google Scholar] [CrossRef]
- Izawa, K.P.; Watanabe, S.; Oka, K.; Hiraki, K.; Morio, Y.; Kasahara, Y.; Brubaker, P.H.; Osada, N.; Omiya, K.; Shimizu, H. Usefulness of step counts to predict mortality in Japanese patients with heart failure. Am. J. Cardiol. 2013, 111, 1767–1771. [Google Scholar] [CrossRef]
- Lee, J.D.; Burger, C.D.; Delossantos, G.B.; Grinnan, D.; Ralph, D.D.; Rayner, S.G.; Ryan, J.J.; Safdar, Z.; Ventetuolo, C.E.; Zamanian, R.T.; et al. A survey-based Estimate of COVID-19 incidence and outcomes among patients with pulmonary arterial hypertension or chronic thromboembolic pulmonary hypertension and impact on the process of care. Ann. Am. Thorac. Soc. 2020, 17, 1576–1582. [Google Scholar] [CrossRef]
- Belge, C.; Quarck, R.; Godinas, L.; Montani, D.; Subias, P.E.; Vachiéry, J.-L.; Nashat, H.; Pepke-Zaba, J.; Humbert, M.; Delcroix, M. COVID-19 in pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension: A reference centre survey. ERJ Open Res. 2020, 6, 2020. [Google Scholar] [CrossRef]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Wieteska-Miłek, M.S.; Florczyk, M.; Kuśmierczyk-Droszcz, B.; Ryczek, R.; Dzienisiewicz, M.; Torbicki, A.; Kurzyna, M. Fear of COVID-19, anxiety and depression in patients with pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension during the pandemic. J. Clin. Med. 2021, 10, 4195. [Google Scholar] [CrossRef]
- Park, D.H.; Fuge, J.; Meltendorf, T.; Kahl, K.G.; Richter, M.J.; Gall, H.; Ghofrani, H.A.; Kamp, J.C.; Hoeper, M.M.; Olsson, K.M. Impact of SARS-CoV-2-pandemic on mental disorders and quality of life in patients with pulmonary arterial hypertension. Front. Psychiatry 2021, 12, 668647. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Craig, C.L.; Thyfault, J.; Spence, J.C. A step-defined sedentary lifestyle index: <5000 steps/day. Appl. Physiol. Nutr. Metab. 2013, 38, 100–114. [Google Scholar] [CrossRef]
- Saint-Maurice, P.F.; Troiano, R.P.; Bassett, D.R.; Graubard, B.I.; Carlson, S.A.; Shiroma, E.J.; Fulton, J.E.; Matthews, C.E. Association of daily step count and step intensity with mortality among US adults. J. Am. Med. Assoc. 2020, 323, 1151–1160. [Google Scholar] [CrossRef]
- Paluch, A.E.; Bajpai, S.; Bassett, D.R.; Carnethon, M.R.; Ekelund, U.; Evenson, K.R.; Galuska, D.A.; Jefferis, B.J.; Kraus, W.E.; Lee, I.-M.; et al. Daily steps and all-cause mortality: A meta-analysis of 15 international cohorts. Lancet Public Health 2022, 7, e219–e228. [Google Scholar] [CrossRef]
- Aslan, G.K.; Akinci, B.; Yeldan, I.; Okumus, G.; Akıncı, B. Respiratory muscle strength in patients with pulmonary hypertension: The relationship with exercise capacity, physical activity level, and quality of life. Clin. Respir. J. 2018, 12, 699–705. [Google Scholar] [CrossRef]
- Mainguy, V.; Provencher, S.; Maltais, F.; Malenfant, S.; Saey, D. Assessment of Daily Life Physical Activities in Pulmonary Arterial Hypertension. PLoS ONE 2011, 6, e27993. [Google Scholar] [CrossRef]
- Kopeć, G.; Kurzyna, M.; Mroczek, E.; Chrzanowski, Ł.; Mularek-Kubzdela, T.; Skoczylas, I.; Kuśmierczyk, B.; Pruszczyk, P.; Błaszczak, P.; Lewicka, E.; et al. Characterization of patients with pulmonary arterial hypertension: Data from the Polish registry of pulmonary hypertension (BNP-PL). J. Clin. Med. 2020, 9, 173. [Google Scholar] [CrossRef] [Green Version]
- Sigmundová, D.; Badura, P.; Sigmund, E.; Bucksch, J. Weekday–weekend variations in mother-/father–child physical activity and screen time relationship: A cross-sectional study in a random sample of Czech families with 5- to 12-year-old children. Eur. J. Sport Sci. 2018, 18, 1158–1167. [Google Scholar] [CrossRef]
- Sigmundová, D.; Sigmund, E.; Badura, P.; Vokáčová, J.; Trhlíková, L.; Bucksch, J. Weekday-weekend patterns of physical activity and screen time in parents and their pre-schoolers. BMC Public Health 2016, 16, 898. [Google Scholar] [CrossRef] [Green Version]
- Alsalhe, T.A.; Aljaloud, S.O.; Chalghaf, N.; Guelmami, N.; Alhazza, D.W.; Azaiez, F.; Bragazzi, N.L. Moderation effect of physical activity on the relationship between fear of COVID-19 and general distress: A pilot case study in Arabic countries. Front. Psychol. 2020, 11, 570085. [Google Scholar] [CrossRef]
- Wieteska-Miłek, M.; Szmit, S.; Florczyk, M.; Kuśmierczyk-Droszcz, B.; Ryczek, R.; Kurzyna, M. COVID-19 Vaccination in patients with pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension: Safety profile and reasons for opting against vaccination. Vaccines 2021, 9, 1395. [Google Scholar] [CrossRef]
- Sehgal, S.; Chowdhury, A.; Rabih, F.; Gadre, A.; Park, M.M.; Li, M.; Wang, X.; Highland, K.B. STep-count using an Accelerometer for Monitoring PAH—STAMP Study group. Counting Steps: A new way to monitor patients with pulmonary arterial hypertension. Lung 2019, 197, 501–508. [Google Scholar] [CrossRef]
- Ludwig, V.M.; Bayley, A.; Cook, D.; Stahl, D.; Treasure, J.L.; Asthworth, M.; Greenough, A.; Winkley, K.; Bornstein, S.R.; Ismail, K. Association between depressive symptoms and objectively measured daily step count in individuals at high risk of cardiovascular disease in South London, UK: A cross-sectional study. BMJ Open 2018, 8, 20942. [Google Scholar] [CrossRef]
- Somaini, G.; Hasler, E.D.; Saxer, S.; Huber, L.C.; Lichtblau, M.; Speich, R.; Bloch, K.E.; Ulrich, S. Prevalence of Anxiety and Depression in Pulmonary Hypertension and Changes during Therapy. Respiration 2016, 91, 359–366. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Clinical Parameters | Total PAH Study Group n (%) or Mean (SD) | Low-Activity PAH Subgroup n (%) or Mean (SD) | Moderate–High-Activity PAH Subgroup n (%) or Mean (SD) | Low-Activity vs. Moderate–High-Activity Subgroup p-Value |
|---|---|---|---|---|
| Number of patients | 40 (100%) | 19 (47.5%) | 21 (52.5%) | |
| Age, years | 45.5 (24.7–64.4) | 44.3 (27.8–64.4) | 46.5 (24.7–61.3) | 0.5 |
| Sex, female | 32 (80%) | 13 (68%) | 19 (90%) | 0.2 |
| Duration of disease, years | 7.6 (6.7) | 7.6 (6.9) | 7.7 (6.7) | 0.96 |
| Idiopathic PAH | 22 (55%) | 10 (53%) | 12 (57%) | 1.0 |
| Heritable PAH | 3 (7.5%) | 0 | 3 (14%) | |
| PAH associated with CHD | 5 (12.5%) | 3 (16%) | 2 (9.5%) | |
| PAH associated with CTD | 9 (22.5%) | 6 (32%) | 3 (14%) | |
| PAH porto-pulmonary | 1 (2.5%) | 0 | 1 (5%) | |
| PDE5/sCG | 35 (87.5%) | 19 (100%) | 16 (76%) | 0.2 |
| ERA | 30 (75%) | 13 (68%) | 17 (81%) | 0.5 |
| Prostacyclin/IP receptor agonist | 20 (50%) | 13 (68%) | 7 (33%) | 0.06 |
| One PAH drug | 11 (27.5%) | 4 (21%) | 7 (33%) | 0.1 |
| Two PAH drugs | 13 (32.5%) | 4 (21%) | 9 (43%) | |
| Three PAH drugs | 16 (40%) | 11 (58%) | 5 (24%) | |
| WHO functional class | 2.1 (0.42) | 2.2 (0.37) | 2.0 (0.45) | 0.4 |
| 1 | 2 (5%) | 0 | 2 (9.5%) | |
| 2 | 33 (82.5%) | 16 (84%) | 17 (81%) | |
| 3 | 5 (12.5%) | 4 (16%) | 2 (9.5%) | |
| History of COVID-19 disease | 4 (10%) | 2 (10%) | 2 (9.5%) | 0.96 |
| Vaccination against COVID-19 | 30 (75%) | 15 (79%) | 15 (71%) | 0.7 |
| Working | 25 (62.5%) | 8 (42%) | 17 (81%) | 0.03 * |
| Concomitant disease # | 18 (45%) | 7 (37%) | 11 (52%) | 0.4 |
| Obesity, BMI ≥ 30 kg/m2 | 8 (20%) | 2 (10%) | 6 (29%) | 0.3 |
| Functional Parameters | Total Study Group n (%) or Mean (SD) or Median (IQR) | Low-Activity Subgroup n (%) or Mean (SD) or Median (IQR) | Moderate/ High-Active Subgroup n (%) or Mean (SD) or Median (IQR) | Low-Activity Subgroup vs. Moderate–High-Activity Subgroup p-Value |
|---|---|---|---|---|
| WHO functional class | 2.1 ± 0.42 | 2.15 ± 0.37 | 2.0 ± 0.45 | 0.4 |
| NT-proBNP, ng/L | 150.5 (91–351) | 211.5 (93–452) | 110 (82–255) | 0.07 |
| 6MWT distance, m | 527.1 ± 68.7 | 502.7 ± 65.5 | 549.1 ± 65.4 | 0.03 * |
| Oxygen saturation before 6MWT, % | 95.5 ± 3.6 | 94.8 ± 4.2 | 96.1 ± 2.3 | 0.3 |
| Oxygen saturation a after 6MWT, % | 91.1 ± 7.3 | 89.7 ± 8.7 | 92.2 ± 5.7 | 0.5 |
| Borg before 6MWT, points | 0.2 ± 0.4 | 0.2 ± 0.5 | 0.2 ± 0.4 | 0.7 |
| Borg at the end of 6MWT, points | 2.4 ± 1.2 | 2.2 ± 1.3 | 2.5 ± 1.2 | 0.7 |
| sPAP, mmHg | n = 20; 62.8 | n = 11; 62.2 | n = 9; 63.3 | 0.6 |
| TAPSE, mm | n = 23; 22.9 | n = 13; 21.8 | n = 10; 24.4 | 0.3 |
| RAA, cm2 | n = 23; 23.0 | n = 13; 23.5 | n = 10; 22.5 | 0.8 |
| Presence of fluid in pericardium, yes/no | n = 23; 4 (10%) | n = 13; 3 (16%) | n = 10; 1 (5%) | 0.6 |
| Variables | Total PAH Study Group Median (IQR) n = 40 | Low-Activity PAH Group Median (IQR) n = 19 | Moderate–High-Activity PAH Group Median (IQR) n = 21 | Low-Activity vs. Moderate/ High Active PAH Group p-Value |
|---|---|---|---|---|
| PCS-SF-36, points | 44.9 (38.1–49.5) | 45.2 (37.7–49.4) | 54.7 (38.3–51.6) | 0.6 |
| MCS-SF-36, points | 49.8 (44.6–57.2) | 49.9 (44.3–59.1) | 48.6 (47.2–55.9) | 0.7 |
| FCV-19S, points | 15.0 (12.0–22.5) | 14 (12–20) | 17 (12–23) | 0.4 |
| HADS-A, points | 5.0 (2.5–6.5) | 5 (2–6) | 5 (3–7) | 0.8 |
| HADS-D, points | 2 (1–4) | 2 (1–5) | 2 (1–3) | 0.8 |
| HADS-A ≥ 8 | 9 (22.5%) | 4 (21%) | 5 (24%) | 0.9 |
| HADS-D ≥ 8 | 4 (10%) | 1 (5%) | 3 (14%) | 0.6 |
| AIS, points | 29 (23.5–33.5) | 28 (25–33) | 30 (23–34) | 0.5 |
| Variables | Steps/Day | p-Value | 6MWT Distance, m | p-Value |
|---|---|---|---|---|
| 6MWT distance, m | 0.41 | <0.01 * | - | - |
| PCS-SF36, points | 0.08 | 0.6 | 0.27 | 0.09 |
| MCS-SF-36, points | −0.17 | 0.3 | −0.007 | 0.9 |
| FCV-19S, points | 0.02 | 0.9 | −0.02 | 0.8 |
| HADS-A, points | 0.19 | 0.2 | 0.005 | 0.9 |
| HADS-D, points | 0.17 | 0.3 | −0.18 | 0.3 |
| AIS, points | 0.03 | 0.9 | 0.08 | 0.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wieteska-Miłek, M.; Szmit, S.; Florczyk, M.; Witowicz, A.; Kurzyna, M. Physical Activity in Pulmonary Arterial Hypertension during Pandemic COVID-19 and the Potential Impact of Mental Factors. Int. J. Environ. Res. Public Health 2022, 19, 8343. https://doi.org/10.3390/ijerph19148343
Wieteska-Miłek M, Szmit S, Florczyk M, Witowicz A, Kurzyna M. Physical Activity in Pulmonary Arterial Hypertension during Pandemic COVID-19 and the Potential Impact of Mental Factors. International Journal of Environmental Research and Public Health. 2022; 19(14):8343. https://doi.org/10.3390/ijerph19148343
Chicago/Turabian StyleWieteska-Miłek, Maria, Sebastian Szmit, Michał Florczyk, Anna Witowicz, and Marcin Kurzyna. 2022. "Physical Activity in Pulmonary Arterial Hypertension during Pandemic COVID-19 and the Potential Impact of Mental Factors" International Journal of Environmental Research and Public Health 19, no. 14: 8343. https://doi.org/10.3390/ijerph19148343
APA StyleWieteska-Miłek, M., Szmit, S., Florczyk, M., Witowicz, A., & Kurzyna, M. (2022). Physical Activity in Pulmonary Arterial Hypertension during Pandemic COVID-19 and the Potential Impact of Mental Factors. International Journal of Environmental Research and Public Health, 19(14), 8343. https://doi.org/10.3390/ijerph19148343