
Two Years of COVID-19 in Austria—Exploratory Longitudinal Study of Mental Health Outcomes and Coping Behaviors in the General Population



Abstract
:1. Introduction
- Determine the point prevalence of AD, PTSD, depression, and anxiety in the general population of Austria in four pandemic stages;
- Compare the prevalence rates across the four stages;
- Examine pandemic-related coping behaviors employed by the general population of Austria; and
- Examine the differences in the use of coping behaviors across four pandemic stages.
2. Materials and Methods
2.1. Sampling
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Sample Characteristics
3.2. Longitudinal Changes in Mental Health Outcomes
3.3. Longitudinal Changes in Pandemic-Related Coping Behaviors
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
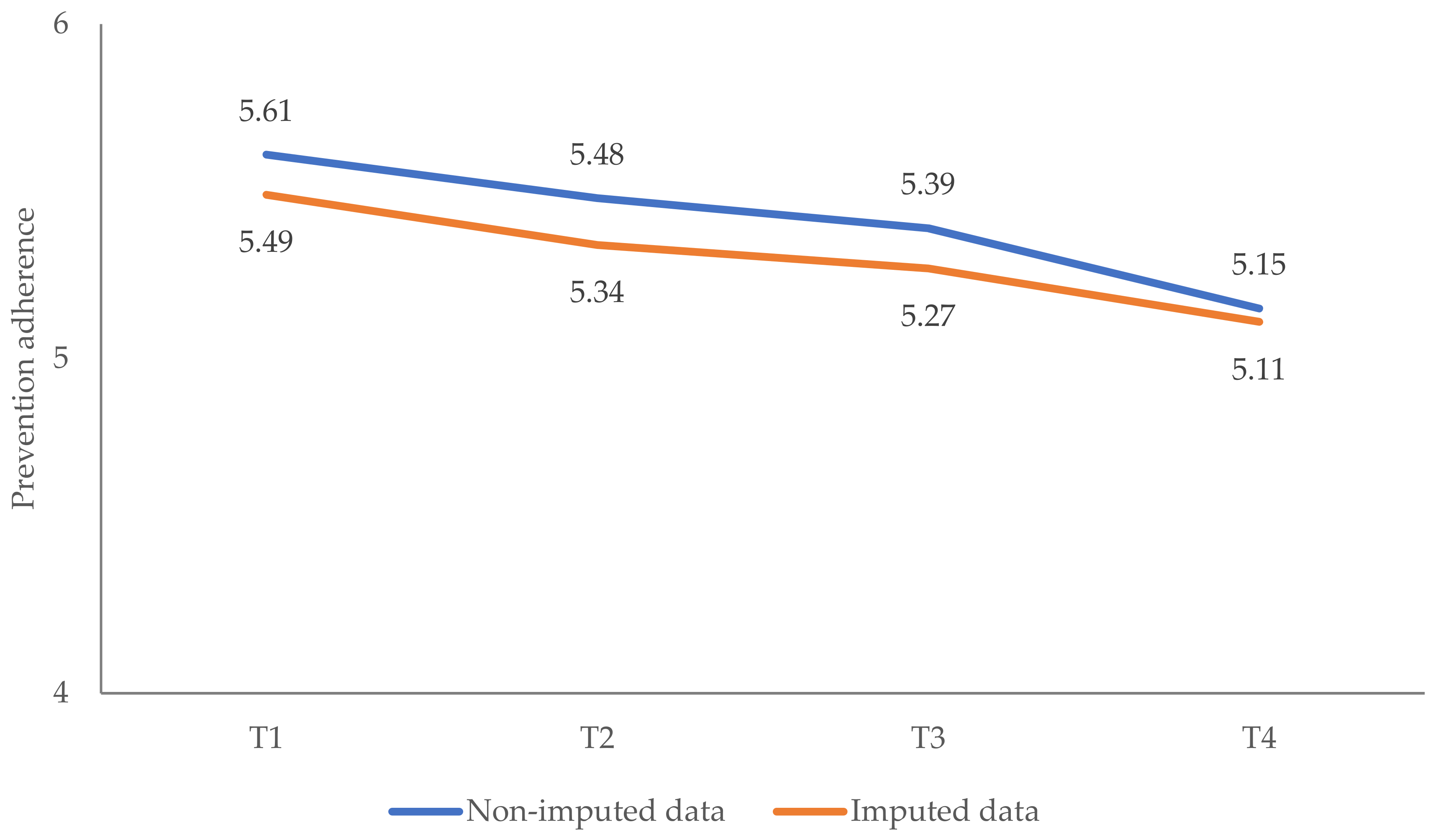
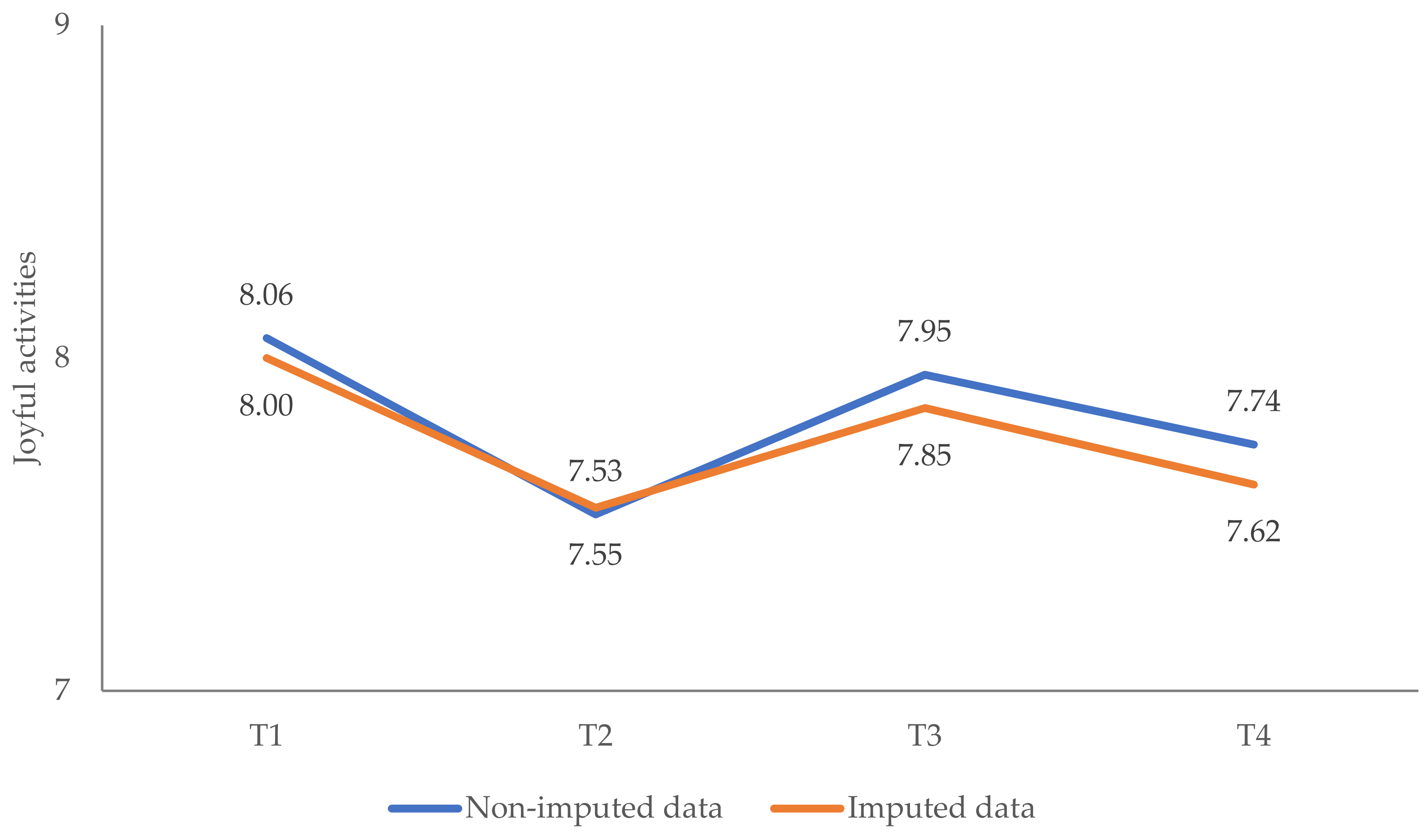
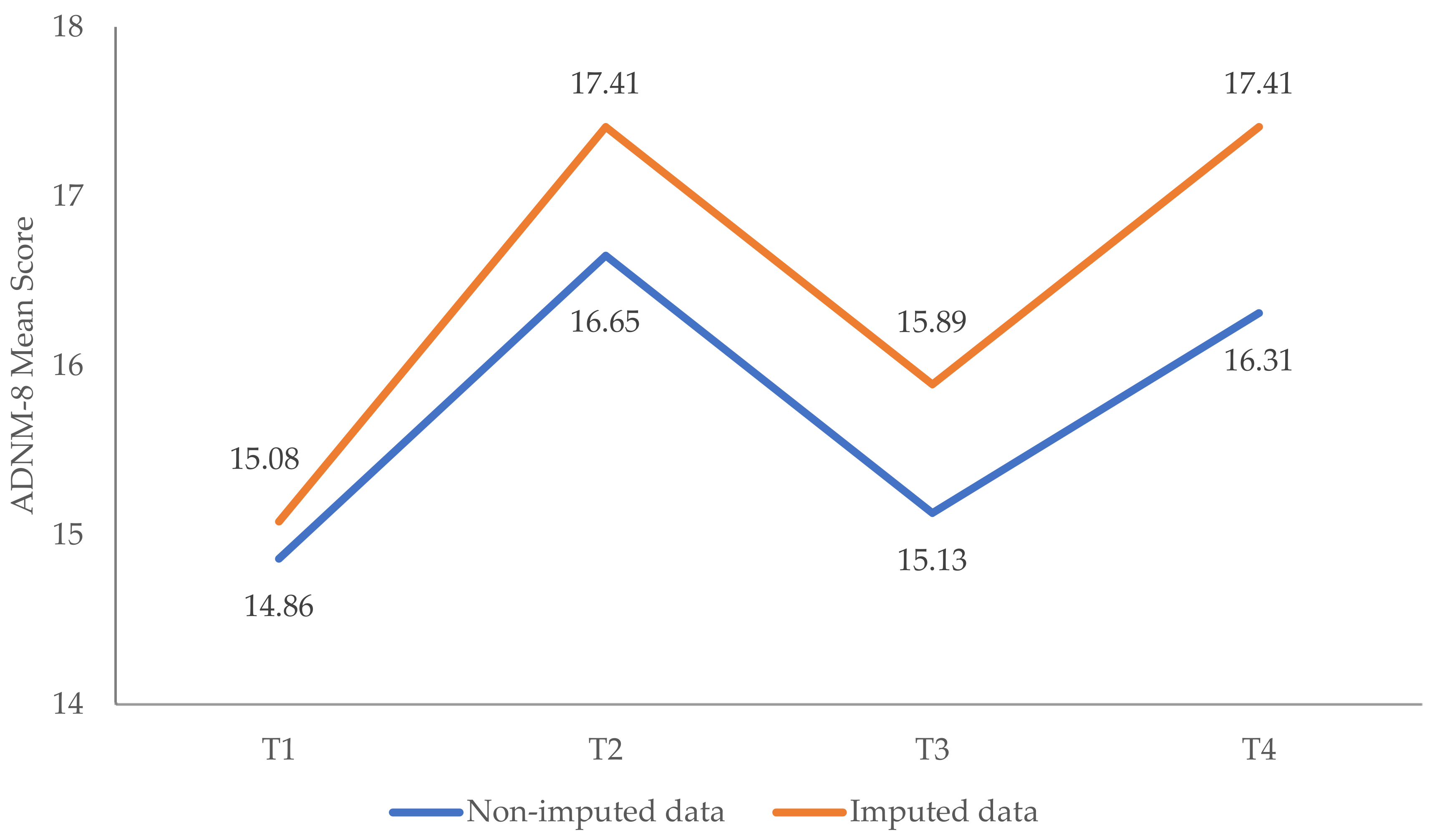
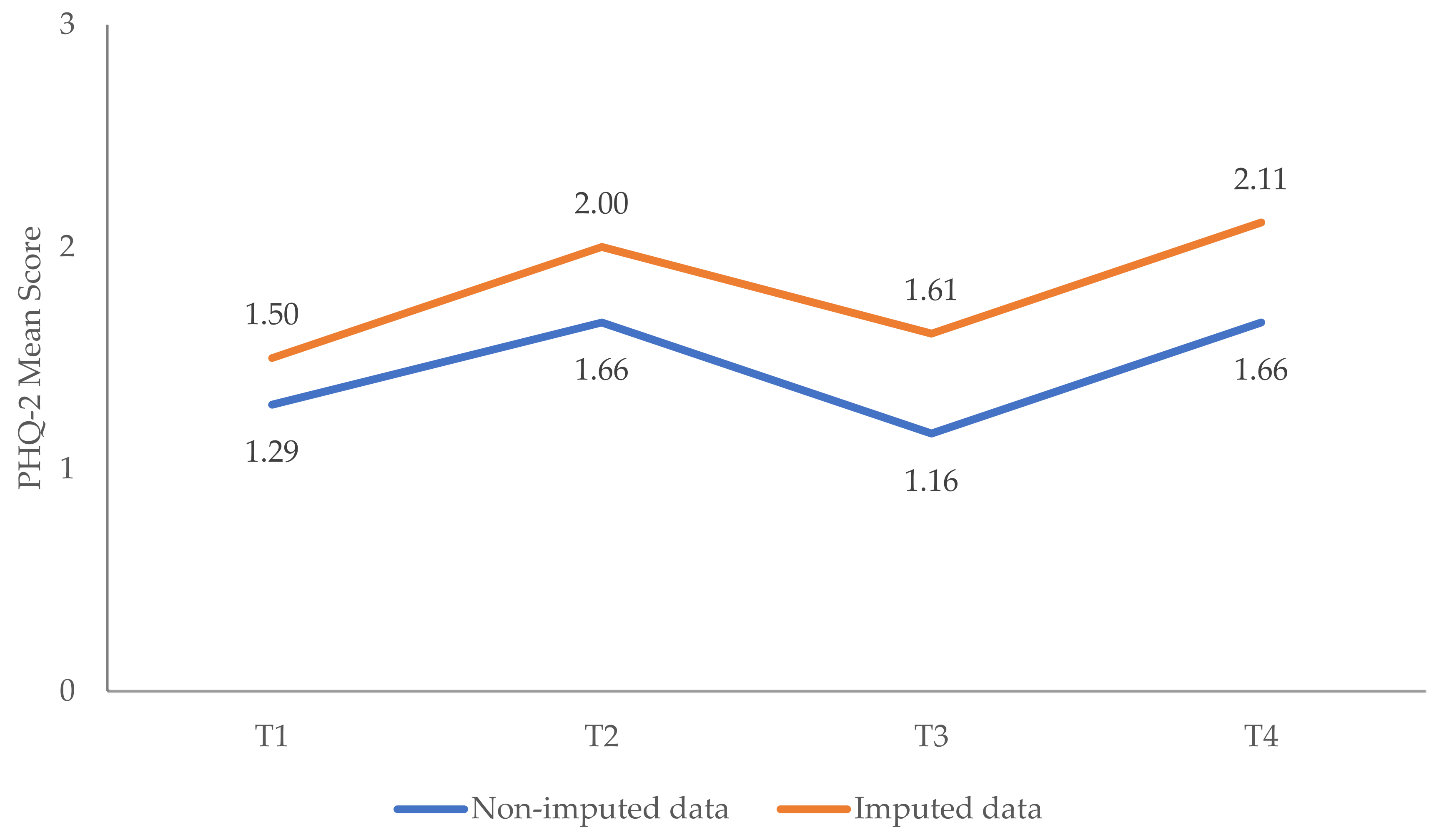
Appendix A.1. Multiple Imputation as Sensitivity Analysis
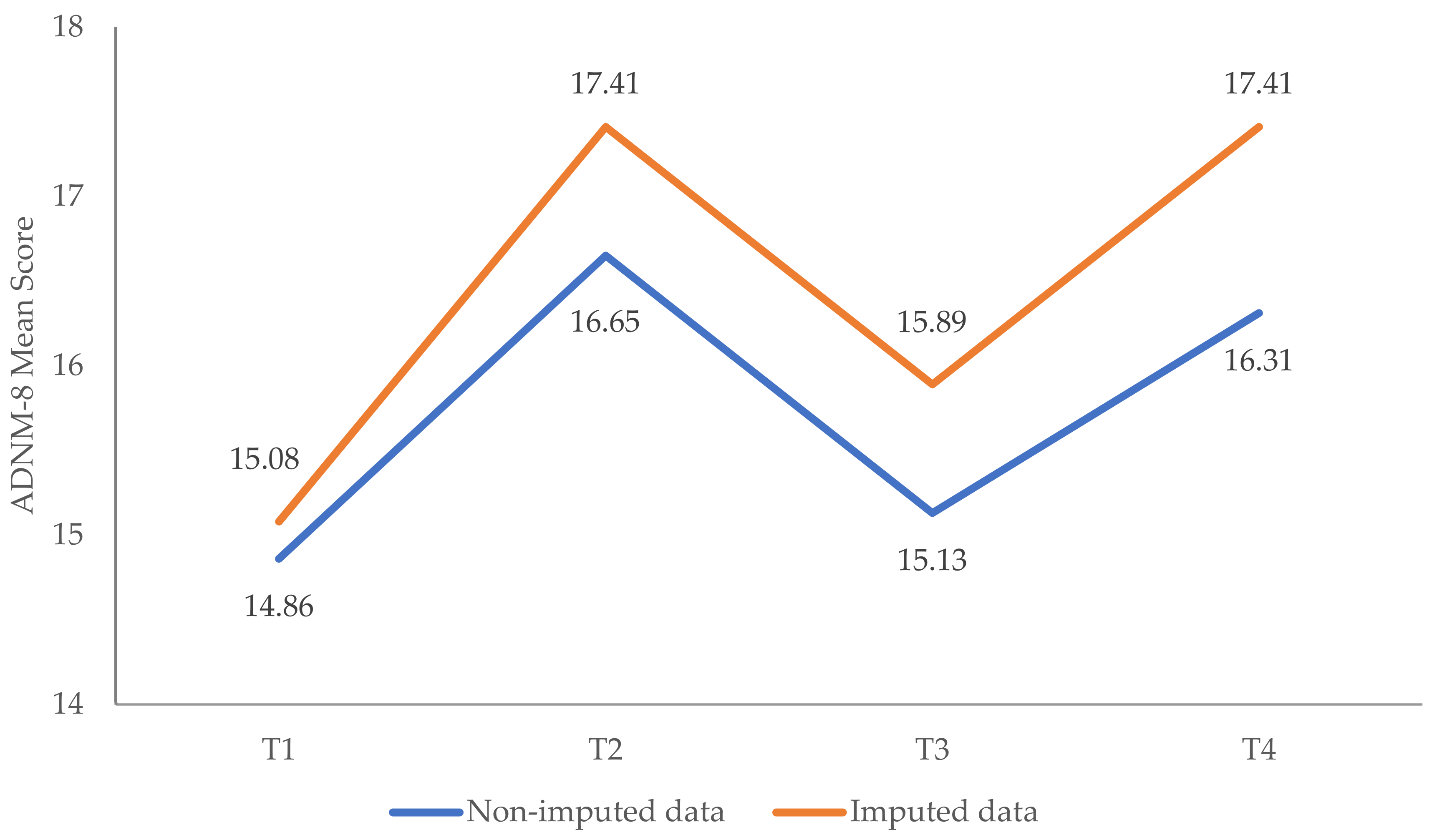
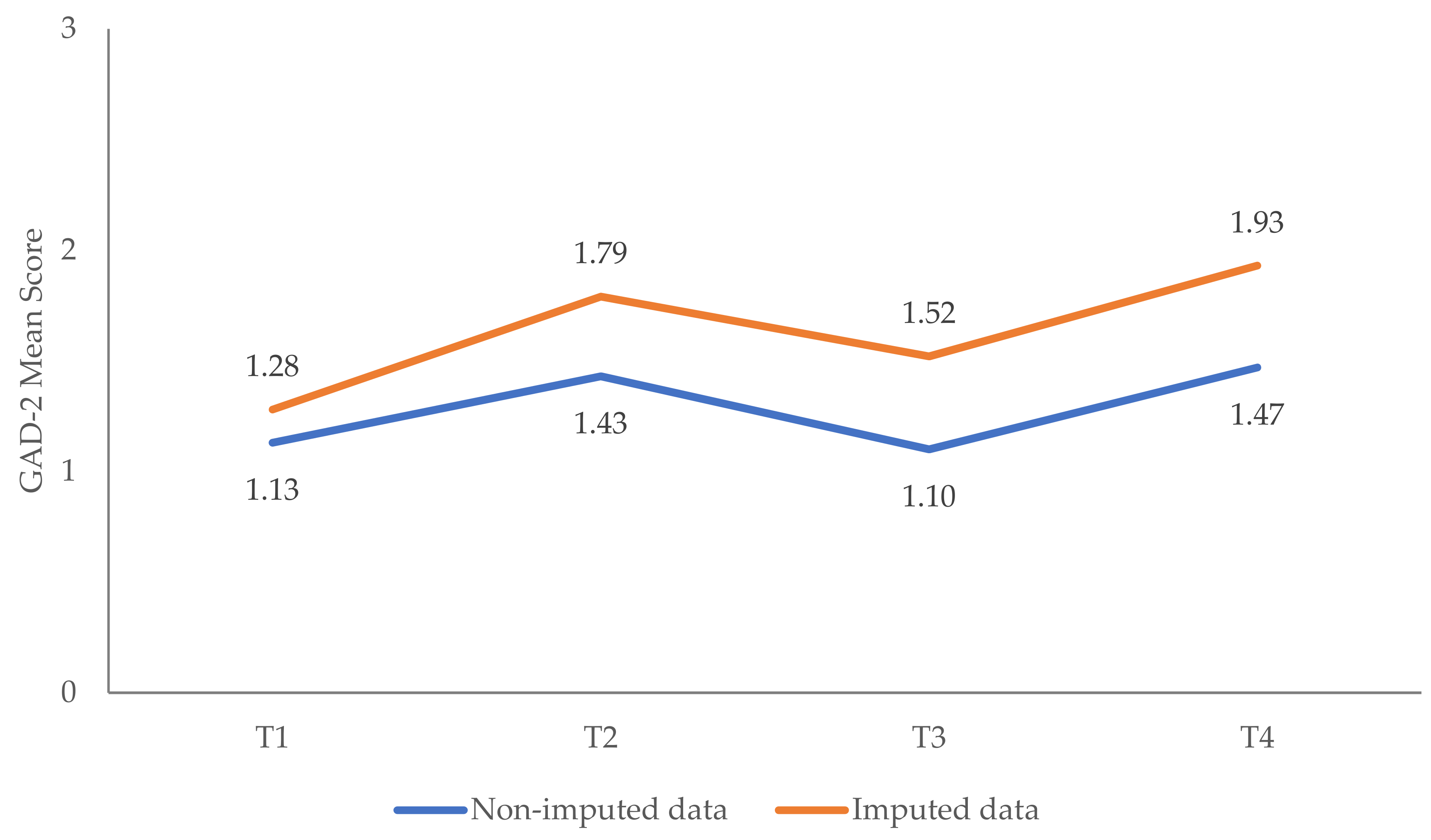
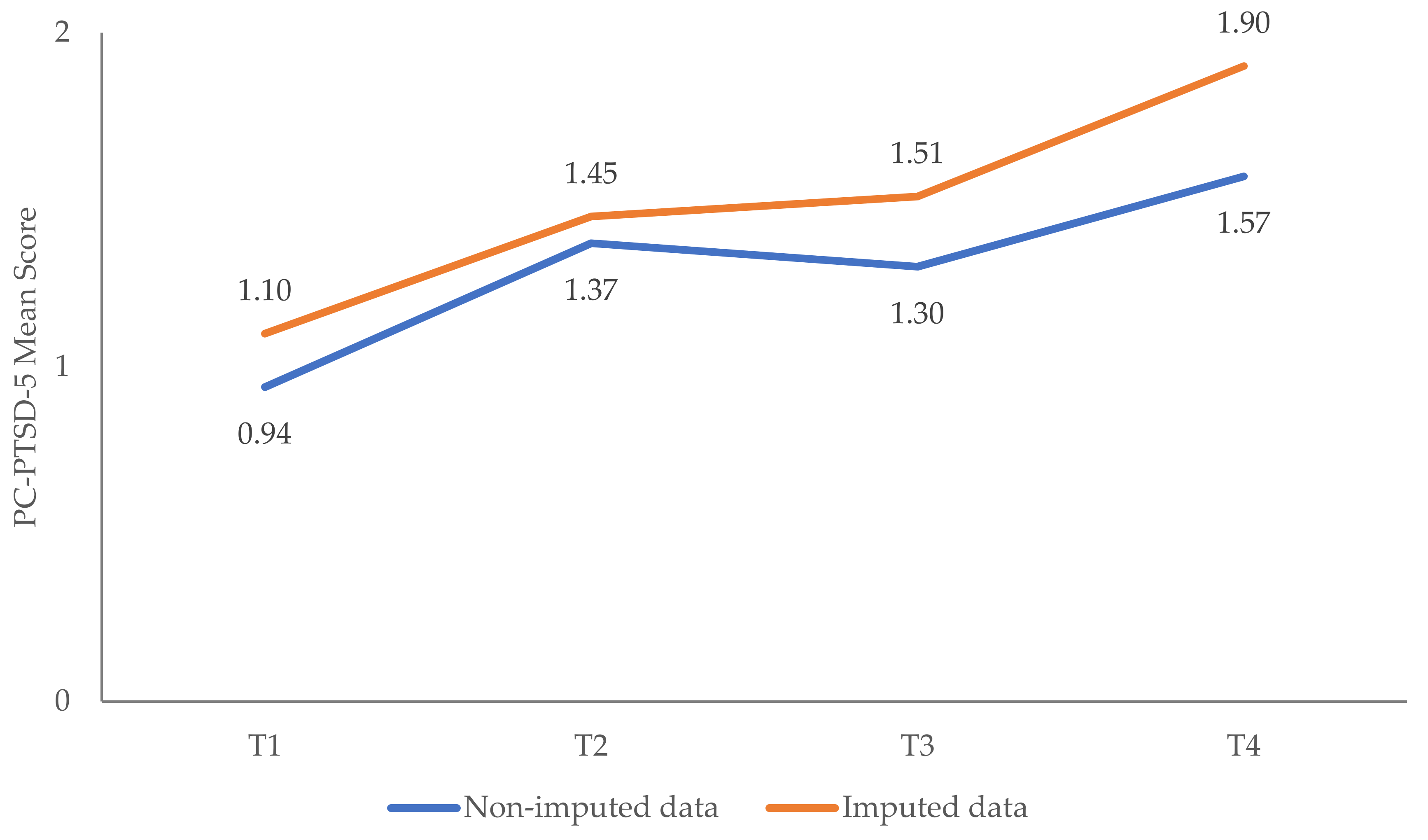
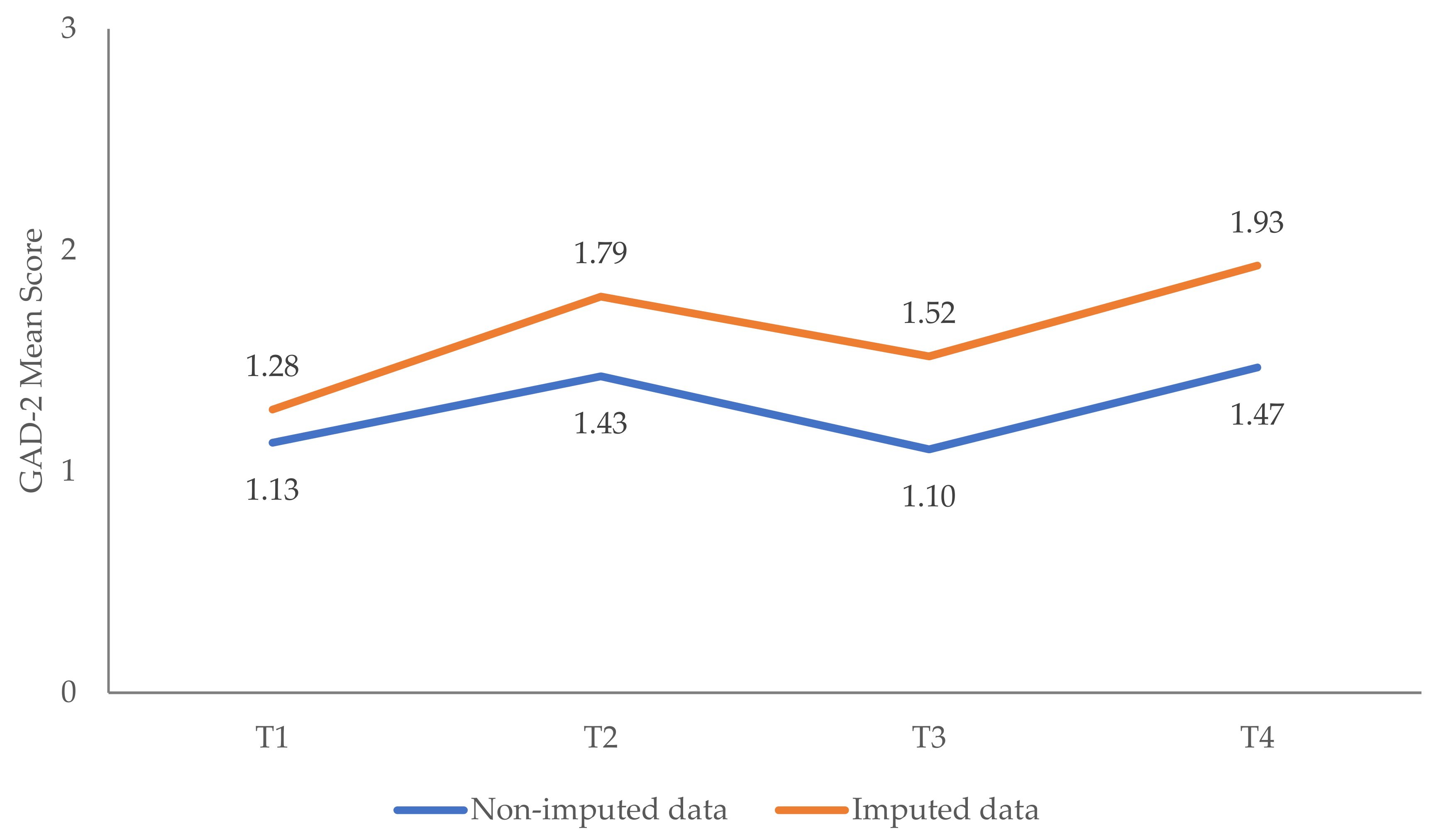
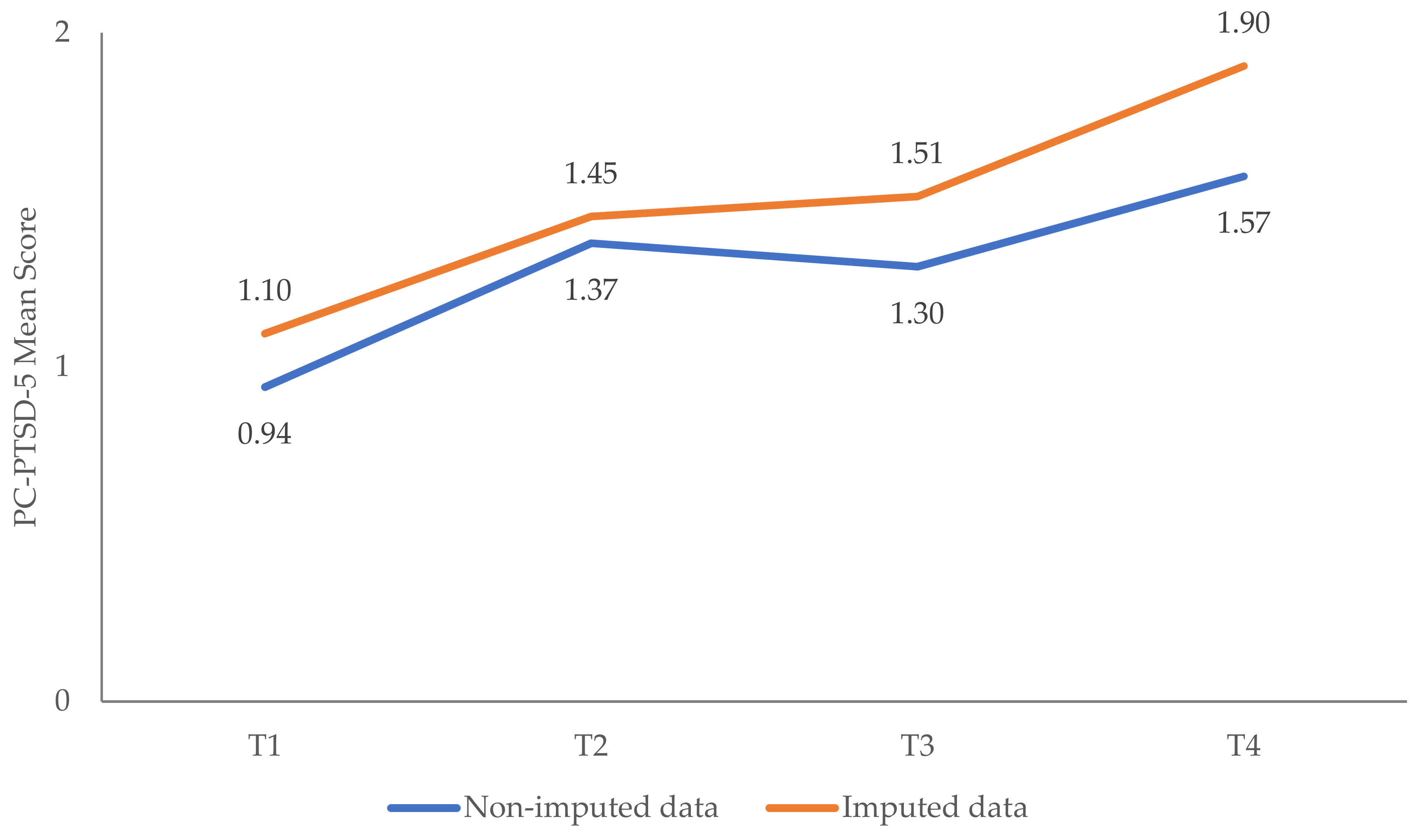
Appendix A.1.1. Changes in Mental Health Outcomes

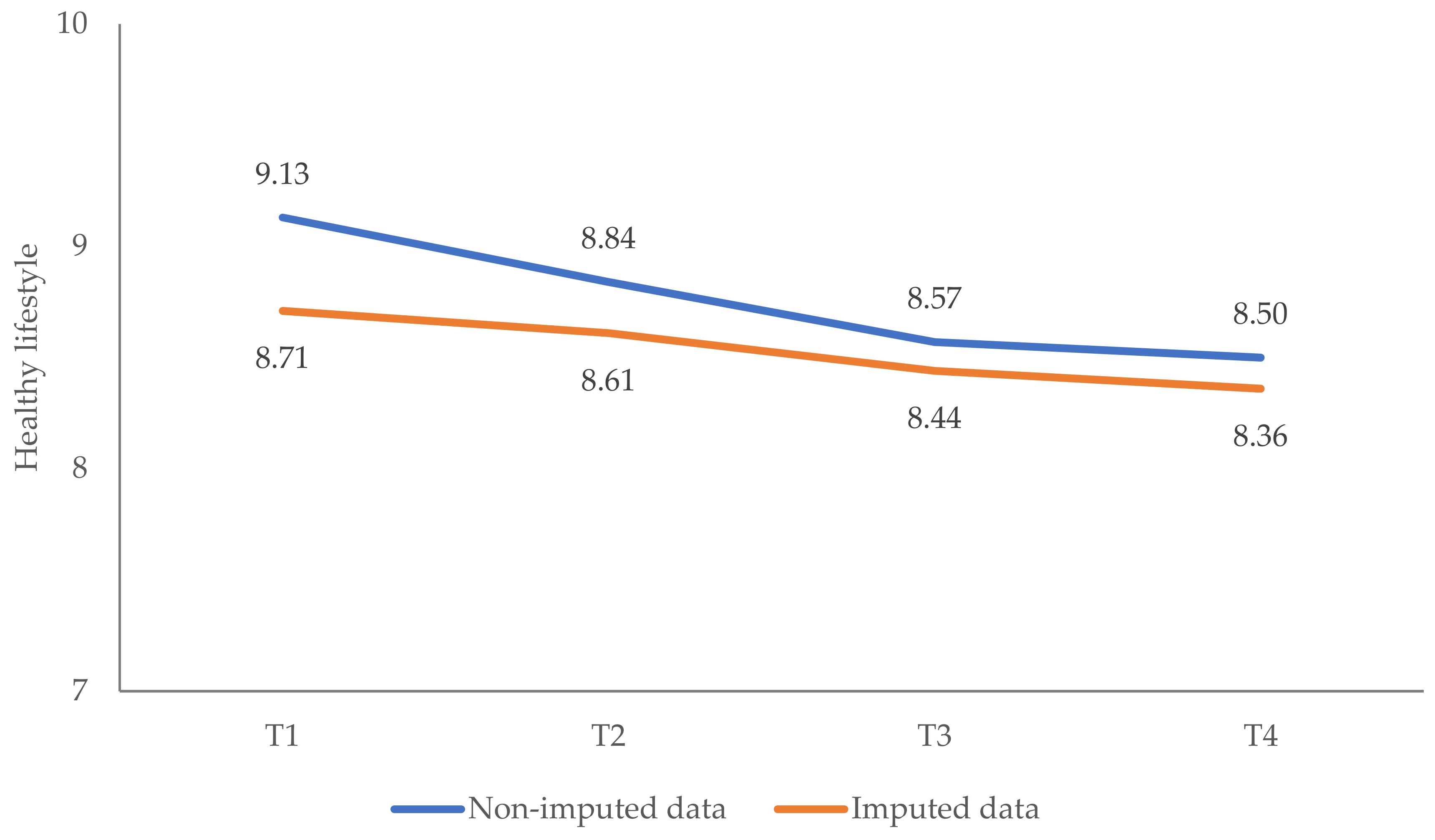
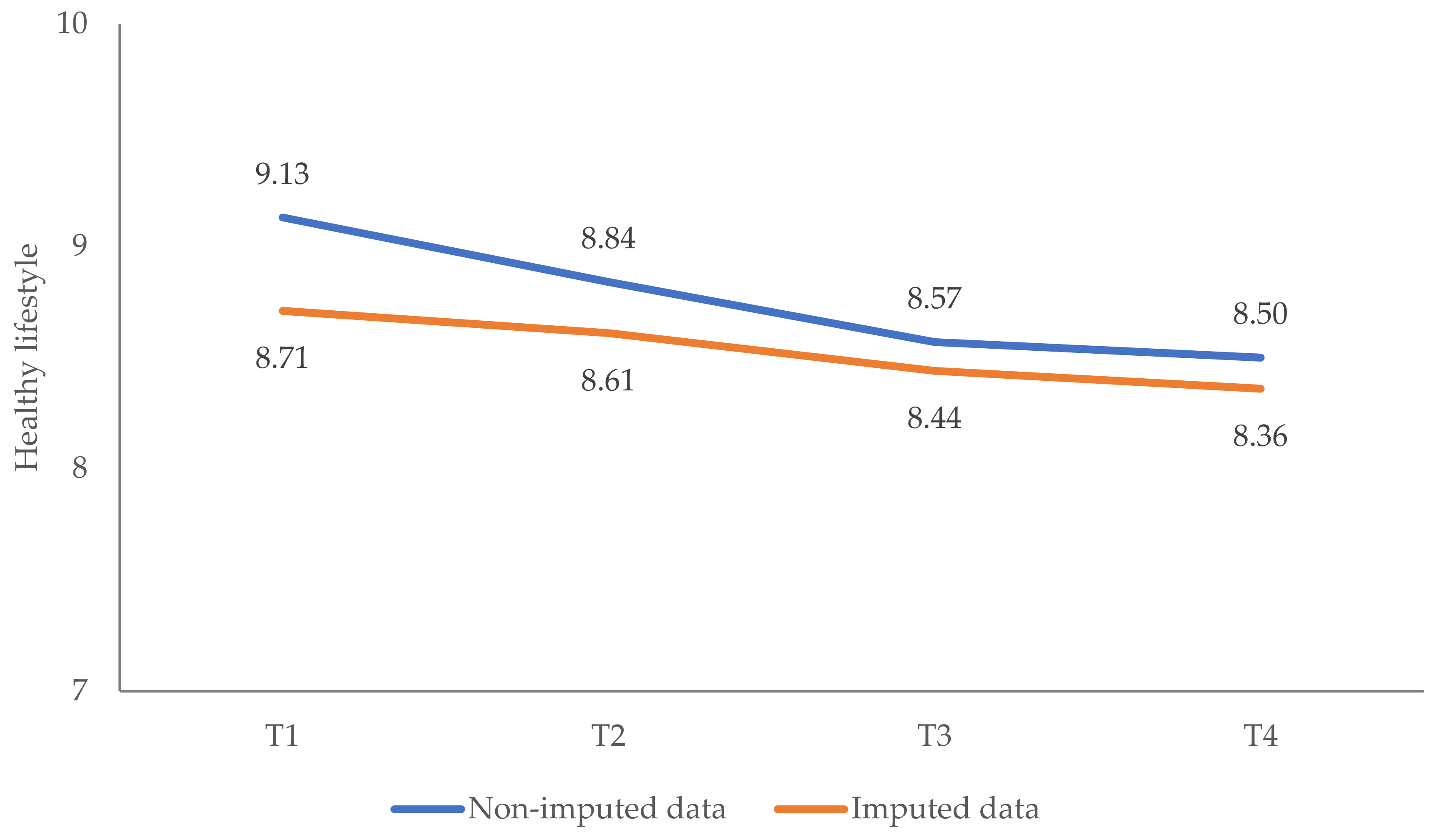
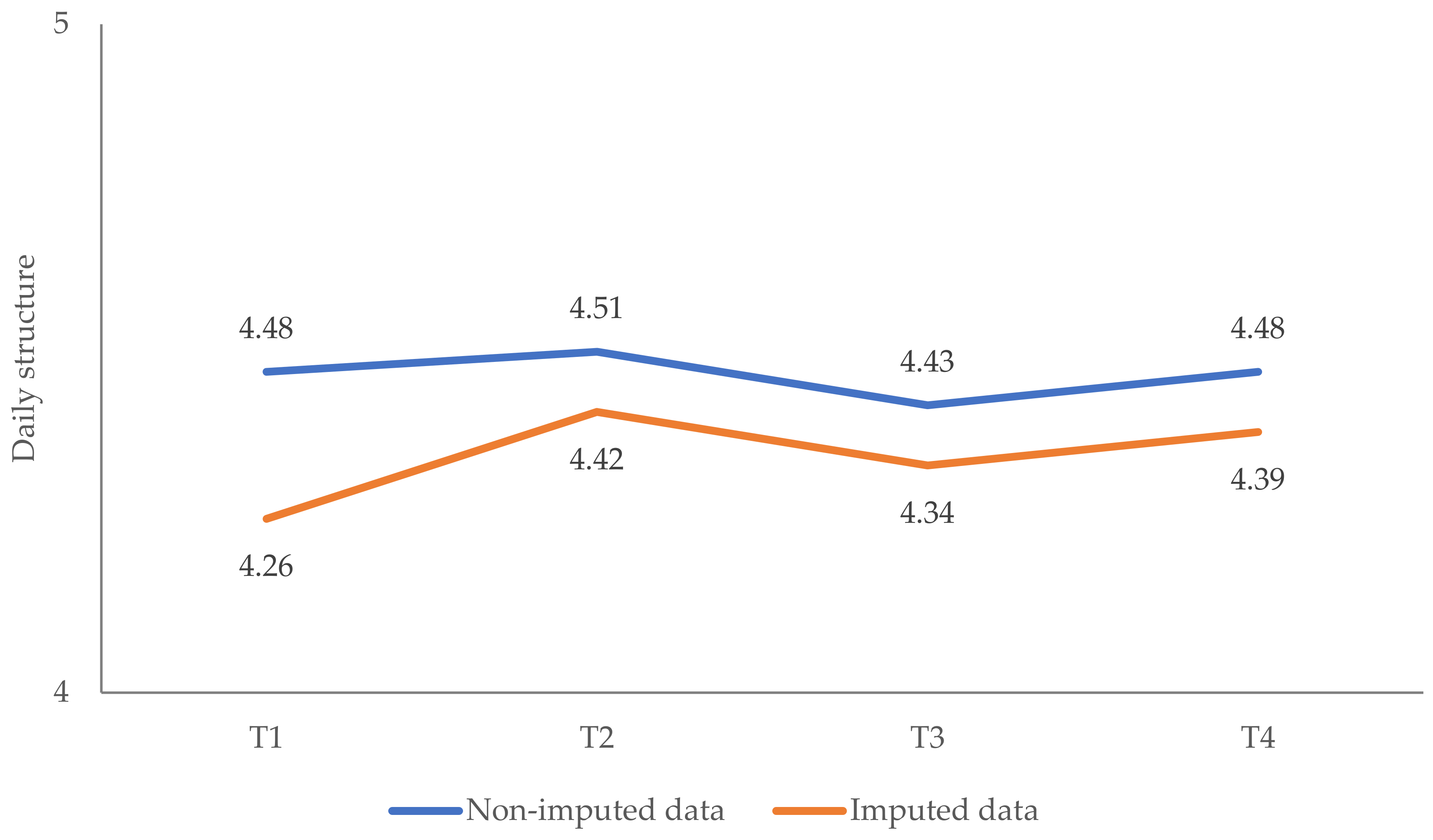
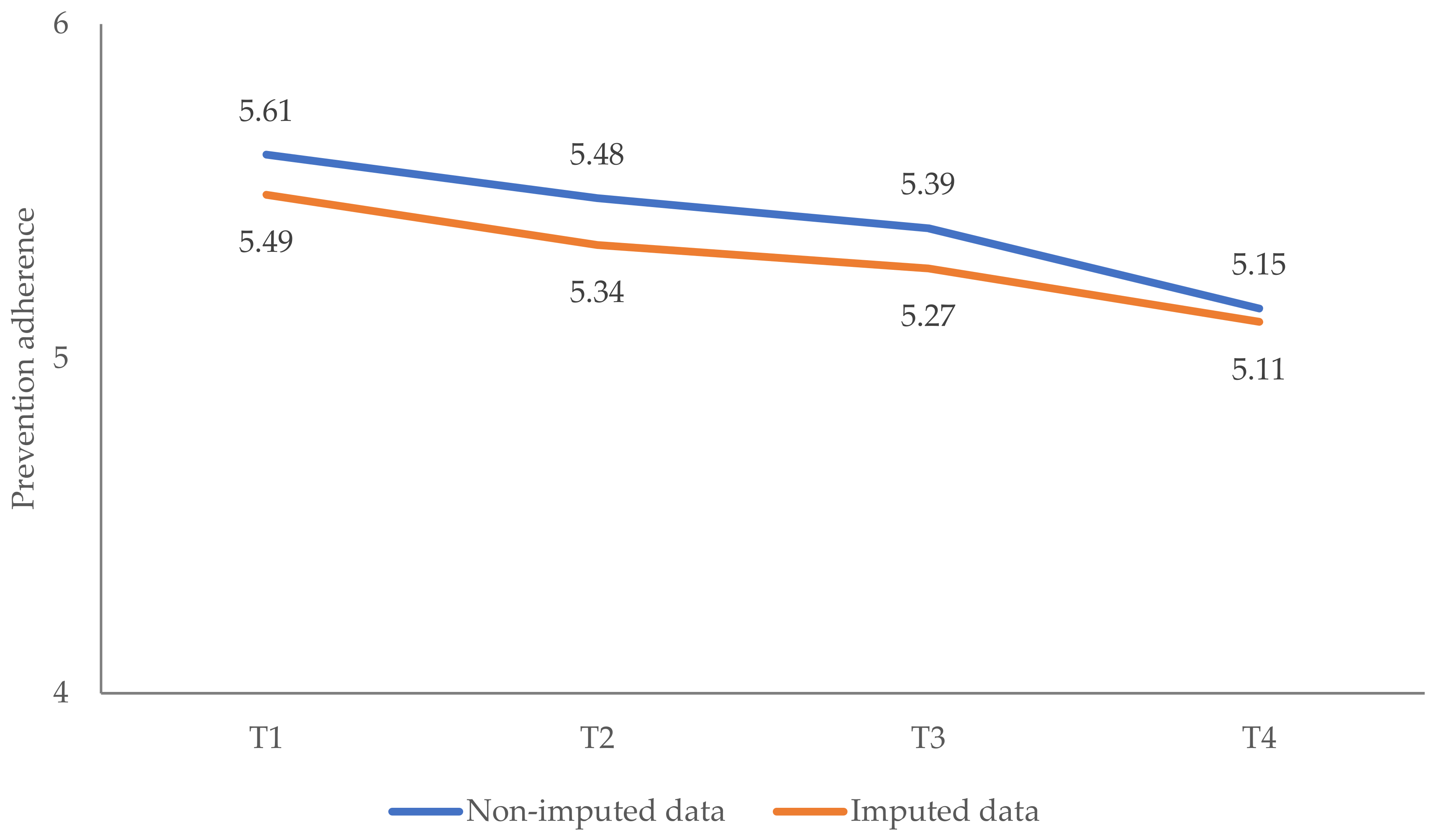
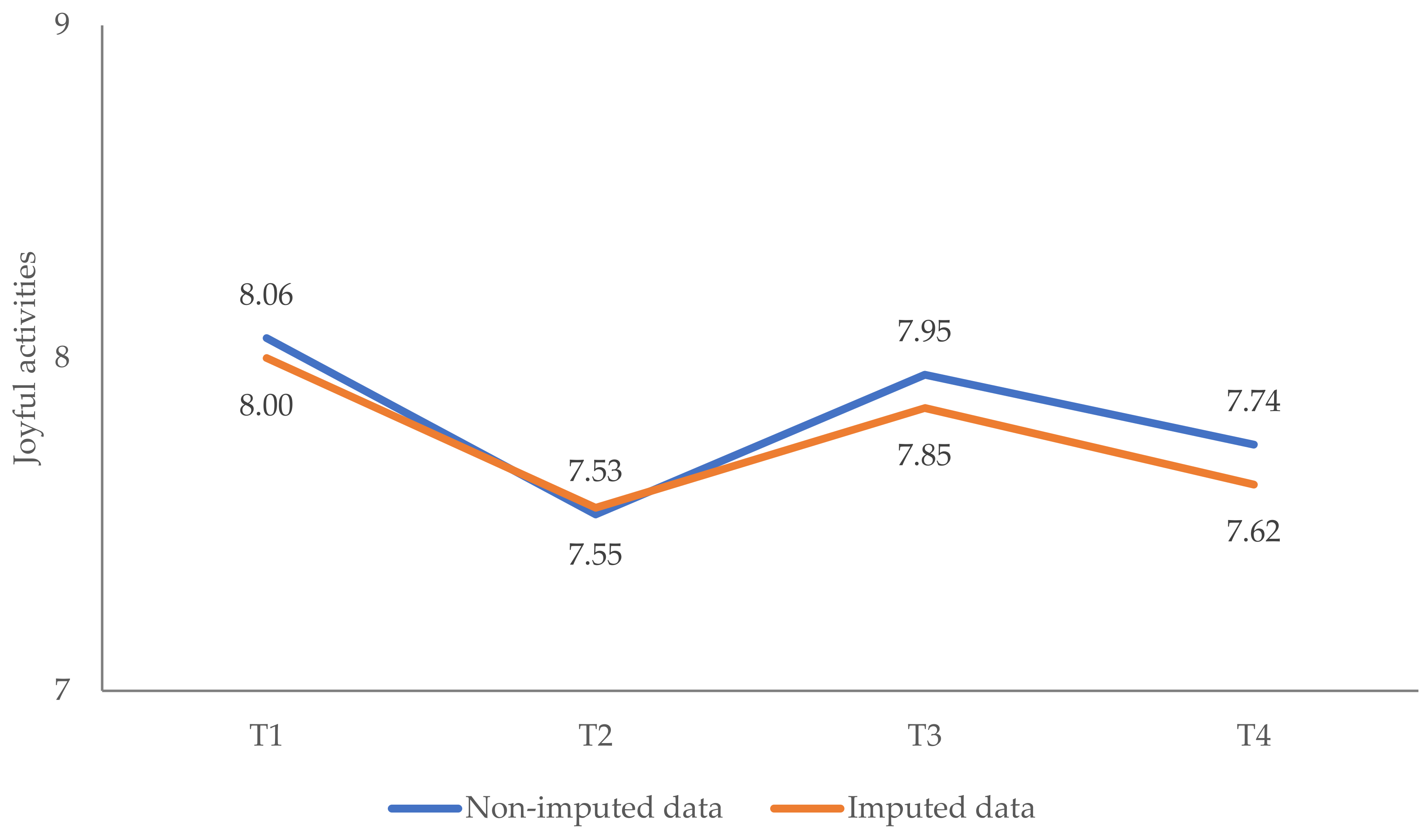
Appendix A.1.2. Changes in Pandemic-Related Coping Behaviors

References
- Felbermayr, G.; Hinz, J.; Chowdhry, S. Après-ski: The Spread of Coronavirus from Ischgl through Germany. Ger. Econ. Rev. 2021, 22, 415–446. [Google Scholar] [CrossRef]
- Pieh, C.; Budimir, S.; Probst, T. The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease [COVID-19] lockdown in Austria. J. Psychosom. Res. 2020, 136, 110186. Available online: http://www.sciencedirect.com/science/article/pii/S0022399920307480 (accessed on 1 June 2022). [CrossRef] [PubMed]
- Niederkrotenthaler, T.; Laido, Z.; Kirchner, S.; Braun, M.; Metzler, H.; Waldhör, T.; Strauss, M.; Garcia, D.; Till, B. Mental health over nine months during the SARS-CoV2 pandemic: Representative cross-sectional survey in twelve waves between April and December 2020 in Austria. J. Affect. Disord. 2022, 296, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Zandonella, M. Follow-Up zur Psychosozialen Situation der WienerInnen Während der Pandemie [Follow-Up on the Psychosocial Situation of the Viennese during the Pandemic]; SORA Institute for Social Research and Consulting: Vienna, Austria, 2021. Available online: https://www.digital.wienbibliothek.at/wbrup/download/pdf/3676800?originalFilename=true (accessed on 1 June 2022).
- Breslau, J.; Finucane, M.L.; Locker, A.R.; Baird, M.D.; Roth, E.A.; Collins, R.L. A longitudinal study of psychological distress in the United States before and during the COVID-19 pandemic. Prev. Med. 2021, 143, 106362. [Google Scholar] [CrossRef]
- González-Sanguino, C.; Ausín, B.; Castellanos, M.A.; Saiz, J.; Muñoz, M. Mental health consequences of the COVID-19 outbreak in Spain. A longitudinal study of the alarm situation and return to the new normality. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 107, 110219. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Wetherall, K.; Cleare, S.; McClelland, H.; Melson, A.J.; Niedzwiedz, C.L.; O’Carroll, R.E.; O’Connor, D.B.; Platt, S.; Scowcroft, E.; et al. Mental health and well-being during the COVID-19 pandemic: Longitudinal analyses of adults in the UK COVID-19 Mental Health & Wellbeing study. Br. J. Psychiatry 2020, 218, 326–333. [Google Scholar] [CrossRef]
- Mata, J.; Wenz, A.; Rettig, T.; Reifenscheid, M.; Möhring, K.; Krieger, U.; Friedel, S.; Fikel, M.; Cornesse, C.; Blom, A.G.; et al. Health behaviors and mental health during the COVID-19 pandemic: A longitudinal population-based survey in Germany. Soc. Sci. Med. 2021, 287, 114333. [Google Scholar] [CrossRef]
- Fancourt, D.; Steptoe, A.; Bu, F. Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID-19 in England: A longitudinal observational study. Lancet Psychiatry 2021, 8, 141–149. [Google Scholar] [CrossRef]
- Santomauro, D.F.; Herrera, A.M.M.; Shadid, J.; Zheng, P.; Ashbaugh, C.; Pigott, D.M.; Abbafati, C.; Adolph, C.; Amlag, J.O.; Aravkin, A.Y.; et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef]
- Rudenstine, S.; Schulder, T.; Bhatt, K.J.; McNeal, K.; Ettman, C.K.; Galea, S. Suicidal ideation during COVID-19: The contribution of unique and cumulative stressors. Psychiatry Res. 2022, 310, 114475. [Google Scholar] [CrossRef]
- Chen, S.; Bonanno, G.A. Psychological adjustment during the global outbreak of COVID-19: A resilience perspective. Psychol. Trauma 2020, 12, S51–S54. [Google Scholar] [CrossRef]
- Vazquez, C.; Valiente, C.; García, F.E.; Contreras, A.; Peinado, V.; Trucharte, A.; Bentall, R.P. Post-traumatic growth and stress-related responses during the COVID-19 pandemic in a national representative sample: The role of positive core beliefs about the world and others. J. Happiness Stud. 2021, 22, 2915–2935. [Google Scholar] [CrossRef]
- Sandbakken, E.M.; Moss, S.M. “Now We Are All in the Same Boat. At the Same Time, We Are Not.” Meaning-Making and Coping under COVID-19 Lockdown in Norway. Hu Arenas 2021, 1–25. [Google Scholar] [CrossRef]
- Santabárbara, J.; Lasheras, I.; Lipnicki, D.M.; Bueno-Notivol, J.; Pérez-Moreno, M.; López-Antón, R.; De la Cámara, C.; Lobo, A.; Gracia-García, P. Prevalence of anxiety in the COVID-19 pandemic: An updated meta-analysis of community-based studies. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 109, 110207. Available online: https://www.sciencedirect.com/science/article/pii/S0278584620305236 (accessed on 1 June 2022). [CrossRef]
- Dawson, D.L.; Golijani-Moghaddam, N. COVID-19: Psychological flexibility, coping, mental health, and wellbeing in the UK during the pandemic. J. Context. Behav. Sci. 2020, 17, 126–134. [Google Scholar] [CrossRef]
- Eisenbeck, N.; Carreno, D.F.; Wong, P.T.; Hicks, J.A.; María, R.-R.G.; Puga, J.L.; Greville, J.; Testoni, I.; Biancalani, G.; López, A.C.C.; et al. An international study on psychological coping during COVID-19: Towards a meaning-centered coping style. Int. J. Clin. Health Psychol. 2022, 22, 100256. [Google Scholar] [CrossRef]
- Quaglieri, A.; Lausi, G.; Fraschetti, A.; Burrai, J.; Barchielli, B.; Pizzo, A.; Cordellieri, P.; De Gennaro, L.; Gorgoni, M.; Ferlazzo, F.; et al. “Stay at Home” in Italy during the COVID-19 Outbreak: A Longitudinal Study on Individual Well-Being among Different Age Groups. Brain. Sci. 2021, 11, 993. [Google Scholar] [CrossRef]
- Gullo, S.; Misici, I.; Teti, A.; Liuzzi, M.; Chiara, E. Going through the lockdown: A longitudinal study on the psychological consequences of the coronavirus pandemic. Res. Psychother. 2020, 23, 494. [Google Scholar] [CrossRef]
- Galende, N.; Redondo, I.; Dosil-Santamaria, M.; Ozamiz-Etxebarria, N. Factors Influencing Compliance with COVID-19 Health Measures: A Spanish Study to Improve Adherence Campaigns. Int. J. Environ. Res. Public Health 2022, 19, 4853. Available online: https://www.mdpi.com/1660-4601/19/8/4853/htm (accessed on 1 June 2022). [CrossRef]
- Shi, L.; Lu, Z.-A.; Que, J.-Y.; Huang, X.-L.; Lu, Q.-D.; Liu, L.; Zheng, Y.-B.; Liu, W.-J.; Ran, M.-S.; Yuan, K.; et al. Long-Term Impact of COVID-19 on Mental Health among the General Public: A Nationwide Longitudinal Study in China. Int. J. Environ. Res. Public Health 2021, 18, 8790. [Google Scholar] [CrossRef]
- Lotzin, A.; Acquarini, E.; Ajdukovic, D.; Ardino, V.; Böttche, M.; Bondjers, K.; Bragesjö, M.; Dragan, M.; Grajewski, P.; Figueiredo-Braga, M.; et al. Stressors, coping and symptoms of adjustment disorder in the course of the COVID-19 pandemic—Study protocol of the European Society for Traumatic Stress Studies [ESTSS] pan-European study. Eur. J. Psychotraumatol. 2020, 11, 1780832. [Google Scholar] [CrossRef] [PubMed]
- Lotzin, A.; Krause, L.; Acquarini, E.; Ajdukovic, D.; Ardino, V.; Arnberg, F.; Böttche, M.; Bragesjö, M.; Dragan, M.; Figueiredo-Braga, M.; et al. Risk and protective factors, stressors, and symptoms of adjustment disorder during the COVID-19 pandemic—First results of the ESTSS COVID-19 pan-European ADJUST Study. Eur. J. Psychotraumatol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Kazlauskas, E.; Gegieckaite, G.; Eimontas, J.; Zelviene, P.; Maercker, A. A Brief Measure of the International Classification of Diseases—11 Adjustment Disorder: Investigation of Psychometric Properties in an Adult Help-Seeking Sample. Psychopathol. 2018, 51, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Ben-Ezra, M.; Mahat-Shamir, M.; Lorenz, L.; Lavenda, O.; Maercker, A. Screening of adjustment disorder: Scale based on the ICD-11 and the Adjustment Disorder New Module. J. Psychiatr. Res. 2018, 103, 91–96. Available online: https://www.sciencedirect.com/science/article/pii/S0022395618303595 (accessed on 1 June 2022). [CrossRef]
- Prins, A.; Bovin, M.J.; Kimerling, R.; Kaloupek, D.G.; Marx, B.P.; Pless-Kaiser, A.; Schnurr, P.P. The Primary Care PTSD Screen for DSM-5 [PC-PTSD-5]: National Center for PTSD. 2015. Available online: https://www.ptsd.va.gov/professional/assessment/screens/pc-ptsd.asp (accessed on 1 June 2022).
- Bovin, M.J.; Kimerling, R.; Weathers, F.W.; Prins, A.; Marx, B.P.; Post, E.P.; Schnurr, P.P. Diagnostic Accuracy and Acceptability of the Primary Care Posttraumatic Stress Disorder Screen for the Diagnostic and Statistical Manual of Mental Disorders [Fifth Edition] Among US Veterans. JAMA Netw. Open 2021, 4, e2036733. [Google Scholar] [CrossRef]
- Prins, A.; Bovin, M.; Smolenski, D.J.; Marx, B.P.; Kimerling, R.; Jenkins-Guarnieri, M.A.; Kaloupek, D.; Schnurr, P.P.; Kaiser, A.P.; Leyva, Y.E.; et al. The Primary Care PTSD Screen for DSM-5 [PC-PTSD-5]: Development and Evaluation within a Veteran Primary Care Sample. J. Gen. Intern. Med. 2016, 31, 1206–1211. [Google Scholar] [CrossRef]
- Spoont, M.R.; Williams, J.W.; Kehle-Forbes, S.; Nieuwsma, J.A.; Mann-Wrobel, M.C.; Gross, R. Does This Patient Have Posttraumatic Stress Disorder? Rational Clinical Examination Systematic Review. JAMA 2015, 314, 501–510. Available online: https://www.ptsd.va.gov/professional/articles/article-pdf/id44256.pdf (accessed on 1 June 2022). [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W.; Löwe, B. An ultra-brief screening scale for anxiety and depression: The PHQ-4. Psychosomatics 2009, 50, 613–621. [Google Scholar] [CrossRef]
- Khubchandani, J.; Brey, R.; Kotecki, J.; Kleinfelder, J.; Anderson, J. The Psychometric Properties of PHQ-4 Depression and Anxiety Screening Scale among College Students. Arch. Psychiatr. Nurs. 2016, 30, 457–462. [Google Scholar] [CrossRef]
- Lotzin, A.; Ketelsen, R.; Krause, L.; Schäfer, I. Pandemic Coping Scale-Validation of a Brief Measure of Coping in a German Sample during the COVID-19 Pandemic. Available online: https://www.researchsquare.com/article/rs-400361/latest.pdf (accessed on 1 June 2022).
- Knief, U.; Forstmeier, W. Violating the normality assumption may be the lesser of two evils. Behav. Res. Methods 2021, 53, 2576–2590. [Google Scholar] [CrossRef]
- Haynes, W. Bonferroni Correction. In Encyclopedia of Systems Biology; Dubitzky, W., Wolkenhauer, O., Cho, K.-H., Yokota, H., Eds.; Springer: New York, NY, USA, 2013; p. 154. [Google Scholar]
- Cheema, J.R. University of Illinois at Urbana-Champaign Some General Guidelines for Choosing Missing Data Handling Methods in Educational Research. J. Mod. Appl. Stat. Methods 2014, 13, 53–75. [Google Scholar] [CrossRef]
- Huque, H.; Carlin, J.B.; Simpson, J.A.; Lee, K.J. A comparison of multiple imputation methods for missing data in longitudinal studies. BMC Med. Res. Methodol. 2018, 18, 168. [Google Scholar] [CrossRef]
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2010, 30, 377–399. [Google Scholar] [CrossRef]
- Richardson, J.T.E. Eta squared and partial eta squared as measures of effect size in educational research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Fullana, M.A.; Hidalgo-Mazzei, D.; Vieta, E.; Radua, J. Coping behaviors associated with decreased anxiety and depressive symptoms during the COVID-19 pandemic and lockdown. J. Affect. Disord. 2020, 275, 80–81. [Google Scholar] [CrossRef]
- Fluharty, M.; Fancourt, D. How have people been coping during the COVID-19 pandemic? Patterns and predictors of coping strategies amongst 26,016 UK adults. BMC Psychol. 2021, 9, 107. [Google Scholar] [CrossRef]
- Brunet, A.; Rivest-Beauregard, M.; Lonergan, M.; Cipolletta, S.; Rasmussen, A.; Meng, X.; Nematollah, J.; Sara, R.; Julia, S.; Adam, D.B.; et al. PTSD is not the emblematic disorder of the COVID-19 pandemic; adjustment disorder is. BMC Psychiatry 2022, 22, 300. [Google Scholar] [CrossRef]
- Rodríguez-Rey, R.; Garrido-Hernansaiz, H.; Collado, S. Psychological impact and associated factors during the initial stage of the Coronavirus [COVID-19] Pandemic among the general population in Spain. Front. Psychol. 2020, 11, 1540. [Google Scholar] [CrossRef]
- WHO. WHO Characterizes COVID-19 as a Pandemic. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed on 1 June 2022).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| T1 | T2 | T3 | T4 a | |
|---|---|---|---|---|
| Recruitment period | 27 June 2020– 22 September 2020 | 14 January 2021– 29 March 2021 | 13 July 2021– 08 October 2021 | 26 November 2021– 13 December 2021 |
| Duration of data collection | 88 days ≈ 13 weeks | 75 days ≈ 11 weeks | 88 days ≈ 13 weeks | 18 days a ≈ 3 weeks |
| Stringency index | ||||
| First week of assessment | 50 | 82.41 | 49.07 | 64.81 |
| Last week of assessment | 37.04 | 73.15 | 51.85 | 64.81 |
| Stringency index mean | 38.59 | 77.58 | 53.63 | 67.13 |
| Stringency index median | 37.96 | 75.93 | 51.85 | 67.59 |
| Incidence | ||||
| First week of assessment | 4.06/1 M | 229.54/1 M | 17.71/1 M | 1482.74/1 M |
| Last week of assessment | 78.95/1 M | 362.96/1 M | 200.80/1 M | 459.72/1 M |
| Deaths | ||||
| First week of assessment | 0.19/1 M | 5.58/1 M | 0.10/1 M | 5.26/1 M |
| Last week of assessment | 0.22/1 M | 2.94/1 M | 1.11/1 M | 5.91/1 M |
| Case fatality rate | ||||
| First week of assessment | 3.98% | 1.78% | 1.65% | 1.10% |
| Last week of assessment | 1.96% | 1.72% | 1.46% | 1.07% |
| T1 | T2 | T3 | T4 | |
|---|---|---|---|---|
| Cronbach’s α (n) | Cronbach’s α (n) | Cronbach’s α (n) | Cronbach’s α (n) | |
| ADNM-8 a | 0.92 (902) | 0.92 (374) | 0.93 (341) | 0.92 (258) |
| Preoccupation | 0.89 b | 0.89 | 0.91 | 0.90 |
| Failure to adapt | 0.85 | 0.84 | 0.85 | 0.84 |
| PHQ-4 a | 0.83 (809) | 0.86 (373) | 0.89 (339) | 0.88 (256) |
| Depression | 0.75 | 0.81 | 0.83 | 0.83 |
| Anxiety | 0.76 | 0.80 | 0.84 | 0.84 |
| PCS a | 0.82 (827) | 0.81 (370) | 0.83 (335) | 0.81 (255) |
| Healthy lifestyle | 0.80 | 0.78 | 0.81 | 0.78 |
| Daily structure | 0.86 | 0.83 | 0.86 | 0.89 |
| Prevention adherence | 0.45 | 0.47 | 0.53 | 0.33 |
| Joyful activities | 0.65 | 0.62 | 0.67 | 0.63 |
| PC-PTSD | 0.79 (866) | 0.65 (59) | 0.71 (64) | 0.83 (54) |
| Characteristic | n | % |
|---|---|---|
| Gender | ||
| Male | 75 | 32.1 |
| Female | 158 | 67.5 |
| Other | 1 | 0.4 |
| Education | ||
| <10 years of schooling | 1 | 0.4 |
| ≥10 years of schooling | 31 | 13.2 |
| Vocational studies | 54 | 23.1 |
| University degree | 148 | 63.2 |
| Income a | ||
| Very low | 22 | 10.4 |
| Low | 70 | 33.0 |
| Medium | 20 | 9.4 |
| High | 100 | 47.2 |
| Work area | ||
| Health care | 60 | 25.6 |
| Public security | 2 | 0.9 |
| Retail/services | 6 | 2.6 |
| Maintenance/repair/construction | 2 | 0.9 |
| Education (e.g., teacher, lecturer) | 28 | 12.0 |
| Other | 92 | 39.3 |
| Not working | 44 | 18.8 |
| Community | ||
| Large city | 160 | 68.4 |
| Suburb near a large city | 16 | 6.8 |
| Small city or town | 39 | 16.7 |
| Rural area | 19 | 8.1 |
| Relationship status | ||
| Single | 58 | 24.8 |
| Temporary relationship(s) | 6 | 2.6 |
| Stable relationship, living separately | 30 | 12.8 |
| Stable relationship, living together | 140 | 59.8 |
| Children | ||
| Yes | 139 | 59.4 |
| No | 95 | 40.6 |
| T1 | T2 | T3 | T4 | |||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |
| Adjustment disorder (ADNM-8) a | 29 | 13.1 | 50 | 22.6 | 32 | 14.5 | 41 | 18.6 |
| Posttraumatic stress disorder (PC-PTSD-5) a | 17 | 7.7 | 1 | 0.5 | 5 | 2.3 | 10 | 4.5 |
| Depressive and anxiety disorders (PHQ-4) b: | ||||||||
| Depression subscale (PHQ-2) | 30 | 13.6 | 44 | 20.0 | 24 | 10.9 | 50 | 22.7 |
| Anxiety subscale (GAD-2) | 28 | 12.7 | 38 | 17.3 | 23 | 10.5 | 46 | 20.9 |
| T1 | T2 | T3 | T4 | ANOVA | Post Hoc Analysis | |||
|---|---|---|---|---|---|---|---|---|
| M (SD) | M (SD) | M (SD) | M (SD) | F Ratio | Partial η2 | Group Comparison | Mean Difference | |
| Adjustment disorder (ADNM-8) a | 14.86 (5.68) | 16.65 (6.41) | 15.13 (6.12) | 16.31 (6.33) | F(2.86, 628.33) = 11.99 *** | 0.05 | T1 vs. T2 | 1.79 *** |
| T1 vs. T3 | 0.27 | |||||||
| T1 vs. T4 | 1.45 ** | |||||||
| T2 vs. T3 | −1.53 *** | |||||||
| T2 vs. T4 | −0.34 | |||||||
| T3 vs. T4 | 1.18 ** | |||||||
| Depression subscale (PHQ-2) b | 1.29 (1.39) | 1.66 (1.46) | 1.16 (1.36) | 1.66 (1.56) | F(3, 657) = 14.62 *** | 0.06 | T1 vs. T2 | 0.38 ** |
| T1 vs. T3 | −0.13 | |||||||
| T1 vs. T4 | 0.37 ** | |||||||
| T2 vs. T3 | −0.51 *** | |||||||
| T2 vs. T4 | 0.01 | |||||||
| T3 vs. T4 | 0.50 *** | |||||||
| Anxiety subscale (GAD-2) b | 1.13 (1.39) | 1.43 (1.57) | 1.10 (1.38) | 1.47 (1.61) | F(2.86, 625.50) = 10.23 *** | 0.05 | T1 vs. T2 | 0.30 ** |
| T1 vs. T3 | 0.04 | |||||||
| T1 vs. T4 | 0.34 ** | |||||||
| T2 vs. T3 | −0.34 *** | |||||||
| T2 vs. T4 | 0.04 | |||||||
| T3 vs. T4 | 0.34 *** | |||||||
| Posttraumatic stress disorder (PC-PTSD-5) | 0.94 (1.37) a | 1.37 (1.24) c | 1.30 (1.47) d | 1.57 (1.81) d | ||||
| Male | Female | ANOVA | |||||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | Effect | F Ratio | Partial η2 | |
| ADNM-8 a | |||||||
| T1 | 13.14 | 4.54 | 15.63 | 5.99 | GxT | F(2.86, 623.36) = 0.63 | 0.003 |
| T2 | 15.27 | 6.33 | 17.25 | 6.37 | |||
| T3 | 14.09 | 5.36 | 15.57 | 6.41 | G | F(1, 218) = 6.6 * | 0.029 |
| T4 | 15.13 | 5.74 | 16.82 | 6.54 | |||
| PHQ-2 b | |||||||
| T1 | 1.09 | 1.17 | 1.36 | 1.46 | GxT | F(3, 651) = 1.39 | 0.006 |
| T2 | 1.35 | 1.15 | 1.81 | 1.57 | |||
| T3 | 0.78 | 0.97 | 1.33 | 1.49 | G | F(1, 217) = 4.74 * | 0.021 |
| T4 | 1.54 | 1.54 | 1.71 | 1.58 | |||
| GAD-2 b | |||||||
| T1 | 0.81 | 1.05 | 1.28 | 1.51 | GxT | F(2.85, 618.72) = 0.92 | 0.004 |
| T2 | 1.03 | 1.03 | 1.61 | 1.75 | |||
| T3 | 0.57 | 0.81 | 1.33 | 1.51 | G | F(1, 217) = 1.88 *** | 0.052 |
| T4 | 1.01 | 1.31 | 1.68 | 1.69 | |||
| PC-PTSD-5 | |||||||
| T1 a | 0.53 | 0.88 | 1.12 | 1.52 | |||
| T2 c | 1.09 | 1.14 | 1.50 | 1.29 | |||
| T3 d | 1.06 | 1.00 | 1.43 | 1.68 | |||
| T4 e | 1.29 | 1.64 | 1.65 | 1.91 | |||
| T1 | T2 | T3 | T4 | ANOVA | Post Hoc Analysis | |||
|---|---|---|---|---|---|---|---|---|
| M (SD) | M (SD) | M (SD) | M (SD) | F Ratio | Partial η2 | Group Comparison | Mean Difference | |
| Healthy lifestyle | 9.13 (3.59) | 8.84 (3.58) | 8.57 (3.73) | 8.50 (3.38) | F(3, 651) = 5.11 ** | 0.02 | T1 vs. T2 | −0.29 |
| T1 vs. T3 | −0.56 * | |||||||
| T1 vs. T4 | −0.63 ** | |||||||
| T2 vs. T3 | −0.27 | |||||||
| T2 vs. T4 | −0.34 | |||||||
| T3 vs. T4 | −0.07 | |||||||
| Daily structure | 4.48 (1.69) | 4.51 (1.56) | 4.43 (1.74) | 4.48 (1.69) | F(2.85, 617.29) = 0.16 | 0.00 | not conducted since ANOVA was not significant | |
| Prevention adherence | 5.61 (0.72) | 5.48 (0.88) | 5.39 (1.01) | 5.15 (1.11) | F(2.73, 592.35) = 21.88 *** | 0.09 | T1 vs. T2 | −0.12 |
| T1 vs. T3 | −0.22 ** | |||||||
| T1 vs. T4 | −0.50 *** | |||||||
| T2 vs. T3 | −0.10 | |||||||
| T2 vs. T4 | −0.34 *** | |||||||
| T3 vs. T4 | −0.24 ** | |||||||
| Joyful activities | 8.06 (2.50) | 7.53 (2.51) | 7.95 (2.45) | 7.74 (2.44) | F(3, 651) = 5.03 ** | 0.02 | T1 vs. T2 | −0.52 ** |
| T1 vs. T3 | −0.10 | |||||||
| T1 vs. T4 | −0.32 | |||||||
| T2 vs. T3 | 0.42 * | |||||||
| T2 vs. T4 | 0.21 | |||||||
| T3 vs. T4 | −0.22 | |||||||
| Male | Female | ANOVA | |||||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | Effect | F Ratio | Partial η2 | |
| Healthy lifestyle | |||||||
| T1 | 8.54 | 3.66 | 9.40 | 3.55 | GxT | F(3, 645) = 1.00 | 0.01 |
| T2 | 7.88 | 3.87 | 9.28 | 3.37 | |||
| T3 | 7.68 | 3.73 | 8.97 | 3.67 | G | F(1, 215) = 5.83 * | 0.03 |
| T4 | 7.90 | 3.58 | 8.79 | 3.27 | |||
| Daily structure | |||||||
| T1 | 4.23 | 1.78 | 4.62 | 1.62 | GxT | F(2.85, 611.90) = 2.52 | 0.01 |
| T2 | 3.96 | 1.87 | 4.76 | 1.33 | |||
| T3 | 3.77 | 1.90 | 4.76 | 1.56 | G | F(1, 215) = 15.42 *** | 0.07 |
| T4 | 3.91 | 1.82 | 4.74 | 1.57 | |||
| Prevention adherence | |||||||
| T1 | 5.57 | 0.70 | 5.63 | 0.73 | GxT | F(2.74, 587.98) = 0.25 | 0.00 |
| T2 | 5.41 | 0.88 | 5.52 | 0.88 | |||
| T3 | 5.28 | 1.04 | 5.45 | 0.99 | G | F(1, 215) = 0.99 | 0.01 |
| T4 | 5.07 | 1.10 | 5.18 | 1.11 | |||
| Joyful activities | |||||||
| T1 | 8.04 | 2.60 | 8.07 | 2.46 | GxT | F(3, 645) = 1.16 | 0.01 |
| T2 | 7.22 | 2.81 | 7.68 | 2.36 | |||
| T3 | 7.58 | 2.70 | 8.12 | 2.32 | G | F(1, 215) = 1.62 | 0.01 |
| T4 | 7.38 | 2.61 | 7.91 | 2.36 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lueger-Schuster, B.; Zrnić Novaković, I.; Lotzin, A. Two Years of COVID-19 in Austria—Exploratory Longitudinal Study of Mental Health Outcomes and Coping Behaviors in the General Population. Int. J. Environ. Res. Public Health 2022, 19, 8223. https://doi.org/10.3390/ijerph19138223
Lueger-Schuster B, Zrnić Novaković I, Lotzin A. Two Years of COVID-19 in Austria—Exploratory Longitudinal Study of Mental Health Outcomes and Coping Behaviors in the General Population. International Journal of Environmental Research and Public Health. 2022; 19(13):8223. https://doi.org/10.3390/ijerph19138223
Chicago/Turabian StyleLueger-Schuster, Brigitte, Irina Zrnić Novaković, and Annett Lotzin. 2022. "Two Years of COVID-19 in Austria—Exploratory Longitudinal Study of Mental Health Outcomes and Coping Behaviors in the General Population" International Journal of Environmental Research and Public Health 19, no. 13: 8223. https://doi.org/10.3390/ijerph19138223
APA StyleLueger-Schuster, B., Zrnić Novaković, I., & Lotzin, A. (2022). Two Years of COVID-19 in Austria—Exploratory Longitudinal Study of Mental Health Outcomes and Coping Behaviors in the General Population. International Journal of Environmental Research and Public Health, 19(13), 8223. https://doi.org/10.3390/ijerph19138223