
Regional Trends and Socioeconomic Predictors of Adolescent Pregnancy in Nigeria: A Nationwide Study

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Sample Composition
2.2. Dependent Variable
2.3. Independent Variables
2.4. Statistical Analysis
2.5. Ethics
3. Results
3.1. Characteristics of Study Population
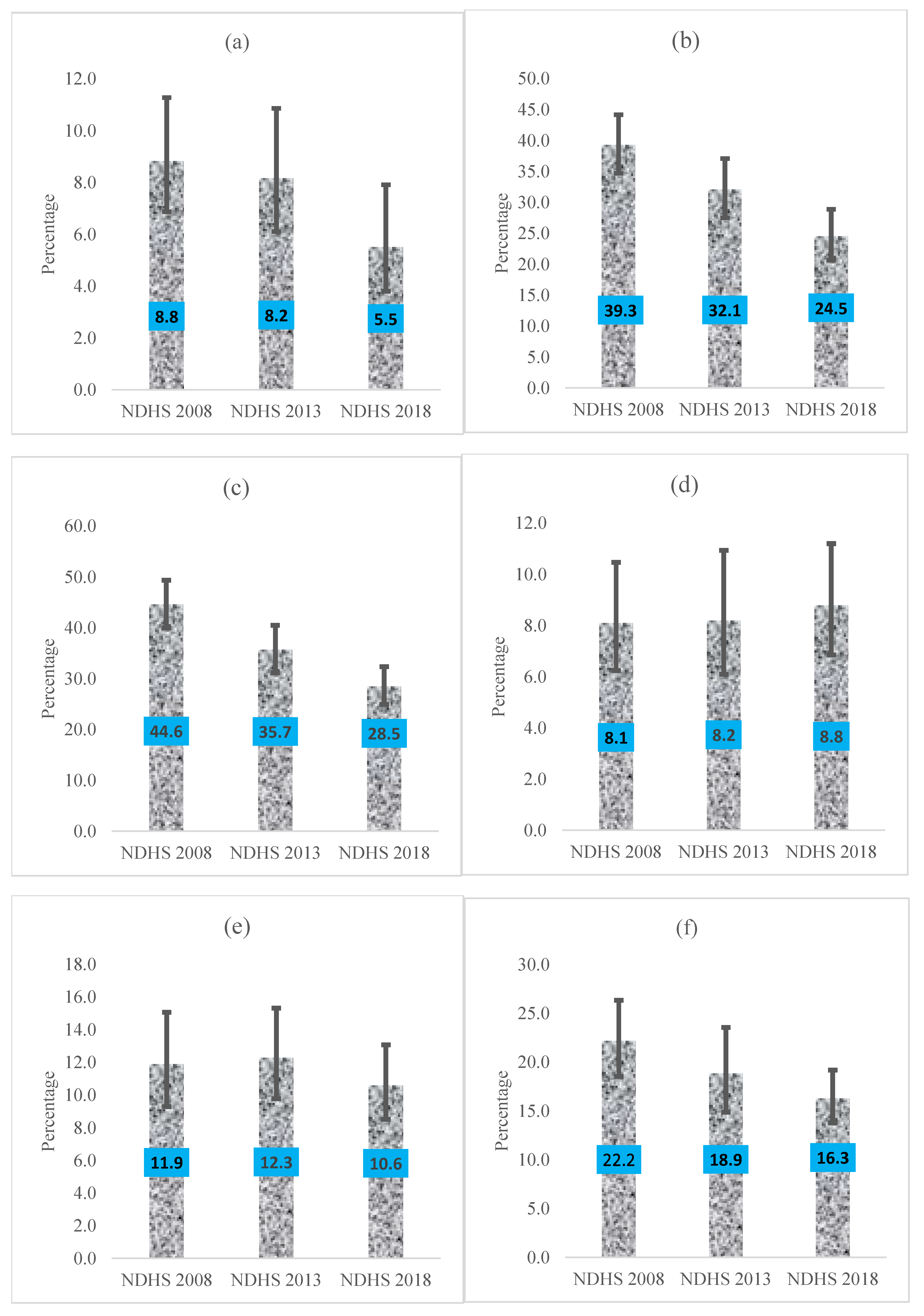
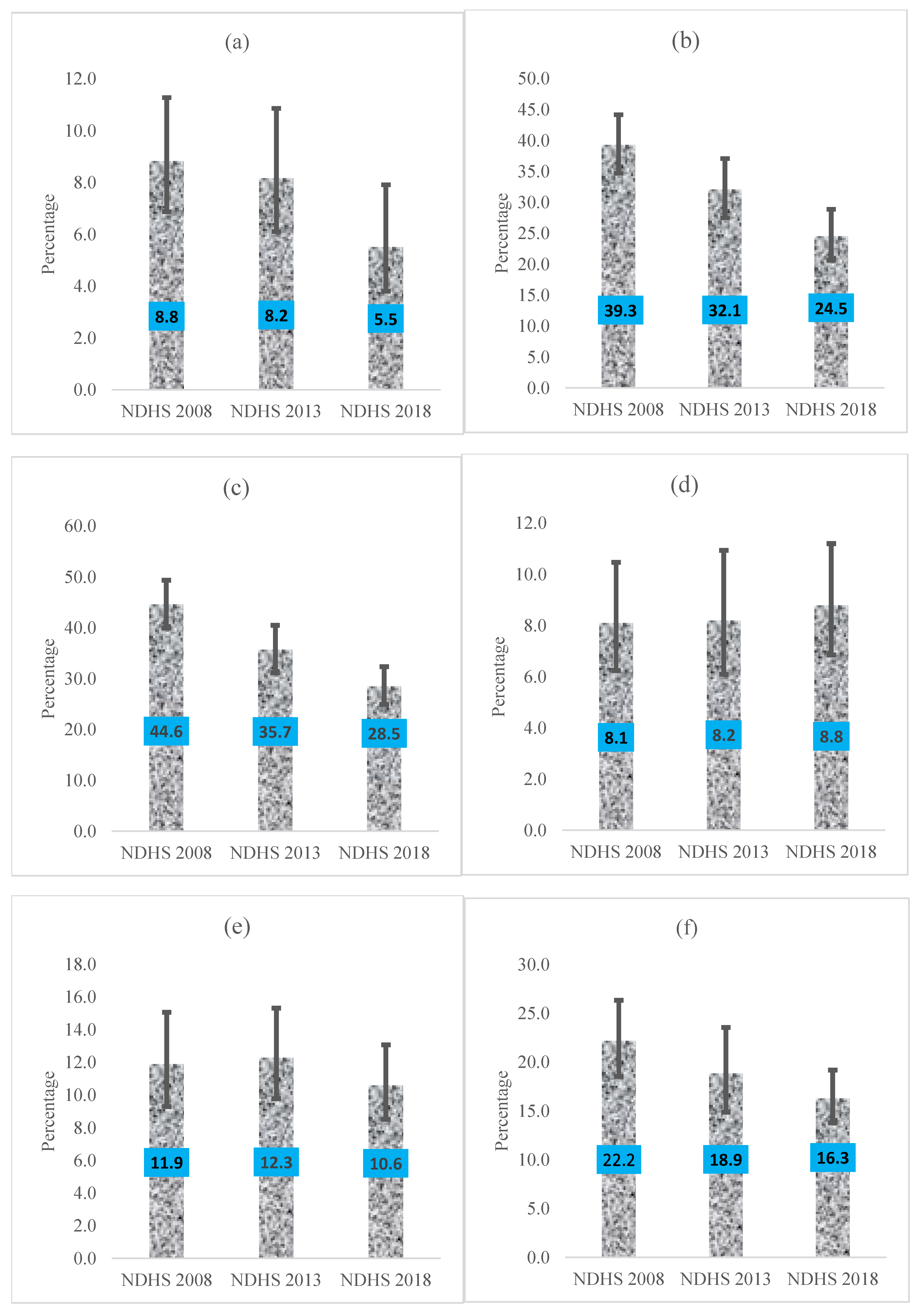
3.2. Trends in Adolescent Pregnancy
3.3. Regional Socioeconomic Predictors of Adolescent Pregnancy
4. Discussion
4.1. Study Limitations and Strengths
4.2. Policy Implication
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Early Marriages, Adolescent and Young Pregnancies; World Health Organization: Geneva, Switzerland, 2012; pp. 1–4. [Google Scholar]
- Kassa, G.M.; Arowojolu, A.O.; Odukogbe, A.A.; Yalew, A.W. Prevalence and determinants of adolescent pregnancy in Africa: A systematic review and Meta-analysis. Reprod. Health 2018, 15, 195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pradhan, R.; Wynter, K.; Fisher, J. Factors Associated with Pregnancy among Married Adolescents in Nepal: Secondary Analysis of the National Demographic and Health Surveys from 2001 to 2011. Int. J. Environ. Res. Public Health 2018, 15, 229. [Google Scholar] [CrossRef] [Green Version]
- Mehra, D.; Sarkar, A.; Sreenath, P.; Behera, J.; Mehra, S. Effectiveness of a community based intervention to delay early marriage, early pregnancy and improve school retention among adolescents in India. BMC Public Health 2018, 18, 732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sama, C.-B.; Ngasa, S.N.; Dzekem, B.S.; Choukem, S.-P. Prevalence, predictors and adverse outcomes of adolescent pregnancy in sub-Saharan Africa: A protocol of a systematic review. Syst. Rev. 2017, 6, 247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations, Department of Economic Social Affairs, Population Division. World Population Prospects: The 2015 Revision; Key Findings and Advance Tables; UN: New York, NY, USA, 2015. [Google Scholar]
- Adolescent Fertility Rate (Births Per 1000 Women Ages 15–19) [Internet]. 2019. Available online: https://data.worldbank.org/indicator/SP.ADO.TFRT (accessed on 10 November 2021).
- Mchunu, G.; Peltzer, K.; Tutshana, B.; Seutlwadi, L. Adolescent pregnancy and associated factors in South African youth. Afr. Health Sci. 2013, 12, 426–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- UNFPA. Adolescent Pregnancy: A Review of the Evidence; UNFPA: New York, NY, USA, 2013. [Google Scholar]
- Sedgh, G.; Finer, L.B.; Bankole, A.; Eilers, M.A.; Singh, S. Adolescent Pregnancy, Birth, and Abortion Rates Across Countries: Levels and Recent Trends. J. Adolesc. Health 2015, 56, 223–230. [Google Scholar] [CrossRef] [Green Version]
- Petroni, S.; Steinhaus, M.; Fenn, N.S.; Stoebenau, K.; Gregowski, A. New Findings on Child Marriage in Sub-Saharan Africa. Ann. Glob. Health 2017, 83, 781–790. [Google Scholar] [CrossRef] [Green Version]
- National Population Commission. Nigeria Demographic and Health Survey 2013; National Population Commission: Abuja, Nigeria; ICF International: Fairfax, VA, USA, 2013. [Google Scholar]
- Nigeria Population Commission. Nigeria Demographic and Health Survey 2018; National Population Commission: Abuja, Nigeria; ICF International: Fairfax, VA, USA, 2019. [Google Scholar]
- Ajala, A.O. Factors associated with teenage pregnancy and fertility in Nigeria. J. Econom. Sustain. Dev. 2014, 5, 62–70. [Google Scholar]
- Nour, N.M. Health Consequences of Child Marriage in Africa. Emerg. Infect. Dis. 2006, 12, 1644–1649. [Google Scholar] [CrossRef]
- Yakubu, I.; Salisu, W.J. Determinants of adolescent pregnancy in sub-Saharan Africa: A systematic review. Reprod. Health 2018, 15, 12978. [Google Scholar] [CrossRef] [Green Version]
- Edukugbo, E. Teenage-Pregnancy-Anatomy-Number-One-Killer-Girls. 2015. Available online: https://www.vanguardngr.com/2015/02/teenage-pregnancy-anatomy-number-one-killer-girls/ (accessed on 10 November 2021).
- Odewale, B.J.; OIadosun, M.; Amoo, E.O. Fertility desire and contraceptive use among women in Nigeria. In 3rd International Conference on African Development Issues; Covenant University Press: Ota, Nigeria, 2016. [Google Scholar]
- Cortez, R.; Saadat, S.; Marinda, E.; Odutolu, O. Adolescent Fertility and Sexual Health in Nigeria. Health Nutr. Popul. Discuss. Pap. 2016, 2016, 24041. [Google Scholar] [CrossRef]
- ICF Macro; National Population Commission. Nigeria Demographic and Health Survey 2008; National Population Commission: Abuja, Nigeria; ICF Macro: Fairfax, VA, USA, 2009. [Google Scholar]
- ICF. The DHS Program. Funded by USAID. Available online: https://dhsprogram.com/data/available-datasets.cfm (accessed on 20 December 2021).
- Filmer, D.; Pritchett, L.H. Estimating wealth effects without expenditure data—Or tears: An application to educational enrol-ments in states of India. Demography 2001, 38, 115–132. [Google Scholar] [PubMed] [Green Version]
- Oke, Y.F. Poverty and teenage pregnancy: The dynamics in developing countries. OIDA Int. J. Sustain. Dev. 2010, 29, 63–66. [Google Scholar]
- Worku, M.G.; Tessema, Z.T.; Teshale, A.B.; Tesema, G.A.; Yeshaw, Y. Prevalence and associated factors of adolescent pregnancy (15–19 years) in East Africa: A multilevel analysis. BMC Preg. Childbirth 2021, 21, 253. [Google Scholar] [CrossRef]
- Birhanu, B.E.; Kebede, D.L.; Kahsay, A.B.; Belachew, A.B. Predictors of teenage pregnancy in Ethiopia: A multilevel analysis. BMC Public Health 2019, 19, 601. [Google Scholar] [CrossRef] [Green Version]
- Wado, Y.D.; Sully, E.A.; Mumah, J.N. Pregnancy and early motherhood among adolescents in five East African countries: A multi-level analysis of risk and protective factors. BMC Preg. Childbirth 2019, 19, 59. [Google Scholar] [CrossRef]
- Gordon, C.P. Adolescent decision making: A broadly based theory and its application to the prevention of early pregnancy. Adolescence 1996, 31, 561. [Google Scholar]
- Odimegwu, C.; Mkwananzi, S. Factors Associated with Teen Pregnancy in sub-Saharan Africa: A Multi-Country Cross-Sectional Study. Afr. J. Reprod. Health 2016, 20, 94–107. [Google Scholar] [CrossRef] [Green Version]
- Undie, C.-C.; MacKenzie, I.; Birungi, H.; Barongo, S.; Ahindukha, D.; Omondi, C. Education sector response to early and unintended pregnancy: A policy dialogue in Homa Bay County, Kenya. Knowl. Commons 2015. [Google Scholar] [CrossRef]
- Mohr, R.; Carbajal, J.; Sharma, B.B. The influence of educational attainment on teenage pregnancy in low-income countries: A systematic literature review. J. Soc. Work Glob. Commun. 2019, 4, 2. [Google Scholar] [CrossRef]
- Ayele, B.G.; Gebregzabher, T.G.; Hailu, T.T.; Assefa, B.A. Determinants of teenage pregnancy in Degua Tembien District, Tigray, Northern Ethiopia: A community-based case-control study. PLoS ONE 2018, 13, e0200898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayanaw Habitu, Y.; Yalew, A.; Azale Bisetegn, T. Prevalence and factors associated with teenage pregnancy, northeast Ethio-pia, 2017: A cross-sectional study. J. Preg. 2018, 2018, 1. [Google Scholar] [CrossRef] [PubMed]
- Bolarinwa, O.A.; Tessema, Z.T.; Frimpong, J.B.; Babalola, T.O.; Ahinkorah, B.O.; Seidu, A.-A. Spatial distribution and factors associated with adolescent pregnancy in Nigeria: A multi-level analysis. Arch. Public Health 2022, 80, 1–13. [Google Scholar] [CrossRef]
- Coppens, J. Effects of Sex Education and Media on Teenage Pregnancy. Counselor Education Capstones. 15. 2014. Available online: https://openriver.winona.edu/counseloreducationcapstones/15 (accessed on 24 June 2022).
- Kearney, M.S.; Levine, P.B. Media influences on social outcomes: The impact of MTV’s 16 and pregnant on teen childbearing. Am. Econ. Rev. 2015, 105, 3597–3632. [Google Scholar] [CrossRef] [Green Version]
- Harris, A.L. Media and Technology in Adolescent Sexual Education and Safety. J. Obstet. Gynecol. Neonatal Nurs. 2011, 40, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Hust, S.J.T.; Brown, J.D.; L’Engle, K.L. Boys Will Be Boys and Girls Better Be Prepared: An Analysis of the Rare Sexual Health Messages in Young Adolescents’ Media. Mass Commun. Soc. 2008, 11, 3–23. [Google Scholar] [CrossRef]
- UNICEF. Ending Child Marriage: Progress and Prospects; UNICEF: New York, NY, USA, 2013. [Google Scholar]
- Fatema, K.; Lariscy, J.T. Mass media exposure and maternal healthcare utilization in South Asia. SSM Popul. Health 2020, 11, 100614. [Google Scholar] [CrossRef]
- Izugbara, C. Household characteristics and unintended pregnancy among ever-married women in Nigeria. Soc. Med. 2013, 25, 4–10. [Google Scholar]
- Baruwa, O.J.; Mkwananzi, S.; Amoateng, A.Y.; Naidoo, N. Teenage pregnancy among unmarried teenagers in Malawi: Does sex of the household head matter? Afr. J. Reprod. Health 2020, 24, 51–57. [Google Scholar]
- Kimweri, A. Assessing the Association between Gender of the Household Head and Teenage Pregnancy In Tanzania. 2012. Available online: http://www.intrec.info/Training%20material/Block%205/INTREC%20paper%20draft%20Angela%20Kimweri.pdf (accessed on 4 April 2022).
- Sánchez-Páez, D.A.; Ortega, J.A. Reported patterns of pregnancy termination from Demographic and Health Surveys. PLoS ONE 2019, 14, e0221178. [Google Scholar] [CrossRef] [Green Version]
- Psaki, S. Addressing child marriage and adolescent pregnancy as barriers to gender parity and equality in education. Prospects 2016, 46, 109–129. [Google Scholar] [CrossRef]
- The Demographic and Health Survey. Available online: http://dhsprogram.com/data/available-datasets.cfm (accessed on 7 March 2022).



{kind=link}
{kind=link}
{kind=link}
| South-West (n = 3656) | North-East (n = 3543) | North-West (n = 6544) | South-East (n = 2674) | South South (n = 3048) | North Central (n = 3296) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Characteristics | n | % * | n | % | n | % | n | % | n | % | n | % |
| Year of survey | ||||||||||||
| 2008 | 1321 | 36.1 | 856 | 24.2 | 1379 | 21.1 | 852 | 31.9 | 1127 | 37.0 | 959 | 29.1 |
| 2013 | 1121 | 30.7 | 1190 | 33.6 | 2428 | 37.1 | 894 | 33.4 | 1033 | 33.9 | 1154 | 35.0 |
| 2018 | 1215 | 33.2 | 1497 | 42.3 | 2737 | 41.8 | 928 | 34.7 | 888 | 29.1 | 1183 | 35.9 |
| Types of residence | ||||||||||||
| Urban | 2629 | 71.9 | 1059 | 29.9 | 2012 | 30.7 | 1662 | 62.2 | 1092 | 35.8 | 936 | 28.4 |
| Rural | 1027 | 28.1 | 2484 | 70.1 | 4532 | 69.3 | 1011 | 37.8 | 1956 | 64.2 | 2360 | 71.6 |
| State of residence | ||||||||||||
| State 1 | 657 | 18.0 | 640 | 18.1 | 573 | 8.8 | 637 | 23.8 | 455 | 14.9 | 671 | 20.4 |
| State 2 | 570 | 15.6 | 851 | 24.0 | 693 | 10.6 | 560 | 20.9 | 357 | 11.7 | 176 | 5.3 |
| State 3 | 278 | 7.6 | 518 | 14.6 | 1081 | 16.5 | 618 | 23.1 | 558 | 18.3 | 316 | 9.6 |
| State 4 | 480 | 13.1 | 334 | 9.4 | 670 | 10.2 | 344 | 12.9 | 344 | 25.4 | 442 | 13.4 |
| State 5 | 1286 | 35.2 | 724 | 20.4 | 1704 | 26.0 | 515 | 19.3 | 515 | 9.1 | 785 | 23.8 |
| State 6 | 385 | 10.5 | 476 | 13.4 | 1259 | 19.2 | 20.5 | 528 | 16.0 | |||
| State 7 | 565 | 8.6 | 378 | 11.5 | ||||||||
| Wealth index | ||||||||||||
| Richest | 1727 | 47.2 | 249 | 7.0 | 634 | 9.7 | 707 | 26.4 | 911 | 29.9 | 493 | 15.0 |
| Richer | 1037 | 28.4 | 462 | 13.0 | 980 | 15.0 | 785 | 29.4 | 949 | 31.1 | 667 | 20.2 |
| Middle | 522 | 14.3 | 612 | 17.3 | 1244 | 19.0 | 720 | 26.9 | 748 | 24.5 | 902 | 27.4 |
| Poorer | 285 | 7.8 | 903 | 25.5 | 1924 | 29.4 | 328 | 12.3 | 337 | 11.1 | 746 | 22.6 |
| Poorest | 86 | 2.3 | 1317 | 37.2 | 1760 | 26.9 | 134 | 5.0 | 104 | 3.4 | 488 | 14.8 |
| Age of respondents | ||||||||||||
| 15 | 918 | 25.1 | 856 | 24.2 | 1685 | 25.8 | 627 | 23.4 | 756 | 24.8 | 811 | 24.6 |
| 16 | 751 | 20.6 | 656 | 18.5 | 1135 | 17.4 | 515 | 19.3 | 605 | 19.9 | 600 | 18.2 |
| 17 | 664 | 18.2 | 656 | 18.5 | 1212 | 18.5 | 498 | 18.6 | 502 | 16.5 | 557 | 16.9 |
| 18 | 732 | 20.0 | 906 | 25.6 | 1649 | 25.2 | 583 | 21.8 | 641 | 21.0 | 791 | 24.0 |
| 19 | 591 | 16.2 | 469 | 13.2 | 862 | 13.2 | 452 | 16.9 | 544 | 17.9 | 535 | 16.2 |
| Education level | ||||||||||||
| Secondary or higher | 3219 | 88.0 | 1234 | 34.8 | 2383 | 36.4 | 2383 | 89.1 | 2722 | 89.3 | 2081 | 63.1 |
| Primary | 312 | 8.5 | 512 | 14.5 | 773 | 11.8 | 275 | 10.3 | 299 | 9.8 | 612 | 18.6 |
| No education | 125 | 3.4 | 1797 | 50.7 | 3388 | 51.8 | 16 | 0.6 | 27 | 0.9 | 603 | 18.3 |
| Access to radio | ||||||||||||
| Yes | 2923 | 80.0 | 1206 | 34.0 | 3315 | 50.7 | 2029 | 75.9 | 2148 | 70.5 | 1881 | 57.1 |
| No | 729 | 19.9 | 2331 | 65.8 | 3219 | 49.2 | 640 | 23.9 | 894 | 29.3 | 1411 | 42.8 |
| Access to television | ||||||||||||
| Yes | 3140 | 85.9 | 979 | 27.6 | 2125 | 32.5 | 2005 | 75.0 | 2507 | 82.2 | 1781 | 54.0 |
| No | 509 | 13.9 | 2558 | 72.2 | 4408 | 67.4 | 664 | 24.8 | 534 | 17.5 | 1507 | 45.7 |
| Access to newspapers | ||||||||||||
| Yes | 1146 | 31.3 | 287 | 8.1 | 816 | 12.5 | 1047 | 39.2 | 958 | 31.4 | 595 | 18.0 |
| No | 2503 | 68.5 | 3229 | 91.1 | 5693 | 87.0 | 1622 | 60.7 | 2082 | 68.3 | 2678 | 81.3 |
| Sex of household head | ||||||||||||
| Female | 1023 | 28.0 | 294 | 8.3 | 519 | 7.9 | 883 | 33.0 | 997 | 32.7 | 630 | 19.1 |
| Male | 2633 | 72.0 | 3249 | 91.7 | 6025 | 92.1 | 1791 | 67.0 | 2051 | 67.3 | 2666 | 80.9 |
| South-West | North-East | North-West | South-East | South South | North Central | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study Variables | aOR (95% CI) | p-Value | aOR (95% CI) | p-Value | aOR (95% CI) | p-Value | aOR (95% CI) | p-Value | aOR (95% CI) | p-Value | aOR (95% CI) | p-Value |
| Year of survey | ||||||||||||
| 2008 | Reference | Reference | Reference | Reference | ||||||||
| 2013 | 0.74 (0.55, 1.00) | 0.053 | 0.90 (0.72, 1.13) | 0.378 | 1.44 (1.01, 2.05) | 0.045 | 0.99 (0.71, 1.39) | 0.973 | ||||
| 2018 | 0.58 (0.44, 0.76) | <0.001 | 0.62 (0.49, 0.77) | <0.001 | 1.12 (0.77, 1.62) | 0.561 | 0.74 (0.56, 0.98) | 0.038 | ||||
| Types of residence | ||||||||||||
| Urban | Reference | Reference | ||||||||||
| Rural | 2.19 (1.59, 3.02) | <0.001 | 2.02 (1.48, 2.77) | <0.001 | ||||||||
| State of residence | ||||||||||||
| State 1 | Reference | Reference | Reference | Reference | Reference | |||||||
| State 2 | 0.37 (0.21, 0.66) | 0.001 | 1.51 (0.99, 2.30) | 0.058 | 1.31 (0.90, 1.89) | 0.154 | 2.88 (1.71, 4.85) | <0.001 | 0.83 (0.50, 1.37) | 0.464 | ||
| State 3 | 0.96 (0.53, 1.75) | 0.899 | 1.67 (1.08, 2.60) | 0.022 | 1.88 (1.36, 2.59) | <0.001 | 3.15 (1.83, 5.43) | <0.001 | 0.96 (0.62, 1.47) | 0.839 | ||
| State 4 | 0.85 (0.49, 1.47) | 0.559 | 1.93 (1.30, 2.86) | 0.001 | 1.17 (0.84, 1.64) | 0.348 | 1.83 (1.01, 3.30) | 0.047 | 0.69 (0.42, 1.15) | 0.155 | ||
| State 5 | 0.46 (0.22, 0.93) | 0.032 | 3.41 (2.34, 4.97) | <0.001 | 1.40 (1.01, 1.94) | 0.041 | 5.15 (3.09, 8.59) | <0.001 | 1.57 (1.03, 2.38) | 0.036 | ||
| State 6 | 0.82 (0.46, 1.47) | 0.507 | 1.66 (1.12, 2.44) | 0.011 | 1.86 (1.32, 2.63) | <0.001 | 1.62 (0.91, 2.86) | 0.098 | 2.49 (1.60, 3.87) | 0.000 | ||
| State 7 | 0.83 (0.59, 1.17) | 0.290 | 1.05 (0.61, 1.79) | 0.872 | ||||||||
| Wealth index | ||||||||||||
| Richest | Reference | Reference | Reference | Reference | Reference | Reference | ||||||
| Richer | 2.34 (1.41, 3.86) | 0.001 | 2.64 (1.29, 5.38) | 0.008 | 1.93 (1.19, 3.12) | 0.007 | 2.77 (1.65, 4.63) | <0.001 | 2.27 (1.42, 3.62) | 0.001 | 2.45 (1.42, 4.22) | 0.001 |
| Middle | 2.25 (1.27, 4.00) | 0.006 | 2.57 (1.18, 5.61) | 0.018 | 2.47 (1.50, 4.06) | 0.000 | 3.25 (1.82, 5.83) | <0.001 | 2.88 (1.77, 4.69) | <0.001 | 2.40 (1.34, 4.28) | 0.003 |
| Poorer | 3.45 (1.65, 7.18) | 0.001 | 2.98 (1.38, 6.42) | 0.005 | 2.06 (1.23, 3.45) | 0.006 | 3.73 (1.68, 8.28) | 0.001 | 2.94 (1.66, 5.23) | <0.001 | 2.58 (1.45, 4.59) | 0.001 |
| Poorest | 4.06 (1.15, 14.37) | 0.030 | 2.22 (1.02, 4.84) | 0.045 | 2.14 (1.27, 3.58) | 0.004 | 2.06 (0.64, 6.58) | 0.223 | 7.91 (3.99, 15.67) | <0.001 | 3.80 (1.99, 7.26) | <0.001 |
| Age of respondents | ||||||||||||
| 15 | Reference | Reference | Reference | Reference | Reference | Reference | ||||||
| 16 | 2.28 (0.99, 5.28) | 0.054 | 3.15 (2.15, 4.63) | <0.001 | 4.55 (3.35, 6.18) | <0.001 | 4.11 (1.25, 13.54) | 0.020 | 3.45 (1.73, 6.87) | <0.001 | 1.96 (1.06, 3.63) | 0.032 |
| 17 | 3.63 (1.60, 8.22) | 0.002 | 9.84 (6.76, 14.31) | <0.001 | 11.29 (8.51, 14.97) | <0.001 | 8.8 (2.83, 27.36) | <0.001 | 6.91 (3.5, 13.64) | <0.001 | 6.65 (4.06, 10.89) | <0.001 |
| 18 | 11.77 (5.78, 23.93) | <0.001 | 16.47 (11.6, 23.38) | <0.001 | 21.68 (16.38, 28.69) | <0.001 | 24.01 (7.91, 72.93) | <0.001 | 10.15 (5.54, 18.61) | <0.001 | 15.89 (9.79, 25.79) | <0.001 |
| 19 | 21.68 (9.92, 47.39) | <0.001 | 40.12 (26.41, 60.97) | <0.001 | 40.81 (29.59, 56.29) | <0.001 | 38.22 (12.67, 115.27) | <0.001 | 24.05 (12.87, 44.92) | <0.001 | 30.75 (18.29, 51.7) | <0.001 |
| Education level | ||||||||||||
| Secondary or higher | Reference | Reference | Reference | Reference | Reference | Reference | ||||||
| Primary | 4.51 (2.77, 7.32) | <0.001 | 3.60 (2.60, 4.97) | <0.001 | 4.65 (3.47, 6.24) | <0.001 | 2.26 (1.32, 3.85) | 0.003 | 2.81 (1.92, 4.11) | <0.001 | 2.48 (1.74, 3.54) | <0.001 |
| No education | 5.83 (3.04, 11.18) | <0.001 | 7.9 (5.86, 10.64) | <0.001 | 8.16 (6.23, 10.68) | <0.001 | 3.84 (1.47, 10.02) | 0.006 | 1.80 (0.54, 5.96) | 0.334 | 5.57 (3.83, 8.10) | <0.001 |
| Access to Radio | ||||||||||||
| Yes | ||||||||||||
| No | ||||||||||||
| Access to Television | ||||||||||||
| Yes | Reference | Reference | ||||||||||
| No | 1.61 (1.25, 2.07) | <0.001 | 1.48 (1.10, 1.99) | 0.010 | ||||||||
| Access to Newspaper | ||||||||||||
| Yes | Reference | Reference | Reference | Reference | ||||||||
| No | 2.13 (1.32, 3.46) | 0.002 | 1.95 (1.29, 2.94) | 0.002 | 2.20 (1.45, 3.34) | <0.001 | 2.55 (1.58, 4.10) | <0.001 | ||||
| Sex of household head | ||||||||||||
| Female | Reference | Reference | Reference | |||||||||
| Male | 2.79 (1.76, 4.43) | <0.001 | 1.67 (1.26, 2.21) | <0.001 | 2.06 (1.45, 2.94) | <0.001 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akombi-Inyang, B.J.; Woolley, E.; Iheanacho, C.O.; Bayaraa, K.; Ghimire, P.R. Regional Trends and Socioeconomic Predictors of Adolescent Pregnancy in Nigeria: A Nationwide Study. Int. J. Environ. Res. Public Health 2022, 19, 8222. https://doi.org/10.3390/ijerph19138222
Akombi-Inyang BJ, Woolley E, Iheanacho CO, Bayaraa K, Ghimire PR. Regional Trends and Socioeconomic Predictors of Adolescent Pregnancy in Nigeria: A Nationwide Study. International Journal of Environmental Research and Public Health. 2022; 19(13):8222. https://doi.org/10.3390/ijerph19138222
Chicago/Turabian StyleAkombi-Inyang, Blessing Jaka, Emma Woolley, Chinonyerem Ogadi Iheanacho, Khulan Bayaraa, and Pramesh Raj Ghimire. 2022. "Regional Trends and Socioeconomic Predictors of Adolescent Pregnancy in Nigeria: A Nationwide Study" International Journal of Environmental Research and Public Health 19, no. 13: 8222. https://doi.org/10.3390/ijerph19138222
APA StyleAkombi-Inyang, B. J., Woolley, E., Iheanacho, C. O., Bayaraa, K., & Ghimire, P. R. (2022). Regional Trends and Socioeconomic Predictors of Adolescent Pregnancy in Nigeria: A Nationwide Study. International Journal of Environmental Research and Public Health, 19(13), 8222. https://doi.org/10.3390/ijerph19138222