
School Food Environment in Urban Zambia: A Qualitative Analysis of Drivers of Adolescent Food Choices and Their Policy Implications



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
Conceptual Framework
2.2. Study Sites
2.3. Study Tools
2.4. Sampling and Data Collection
2.5. Data Analysis
2.5.1. Focus Group Discussions
2.5.2. School Environment Mapping
3. Results
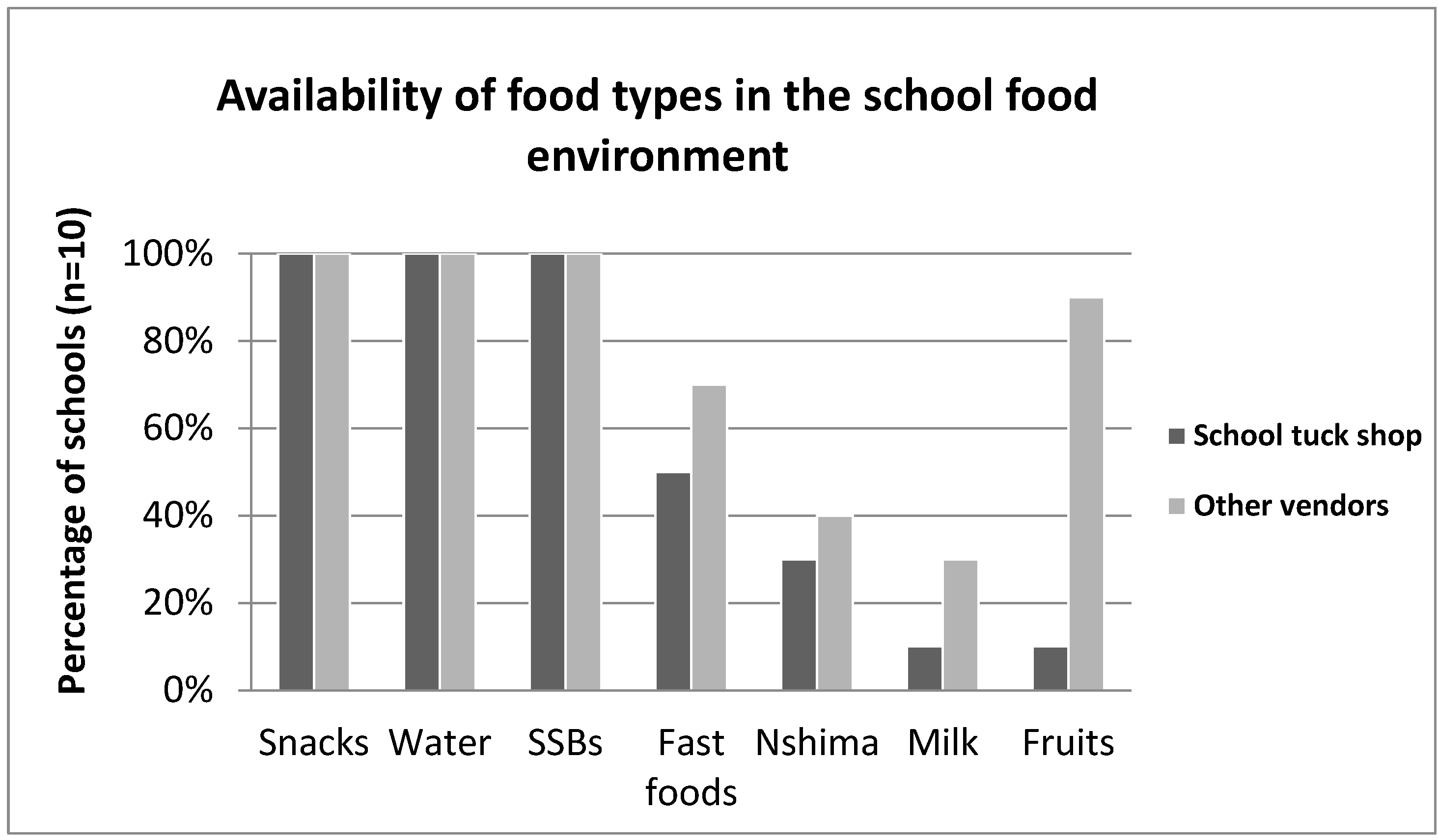
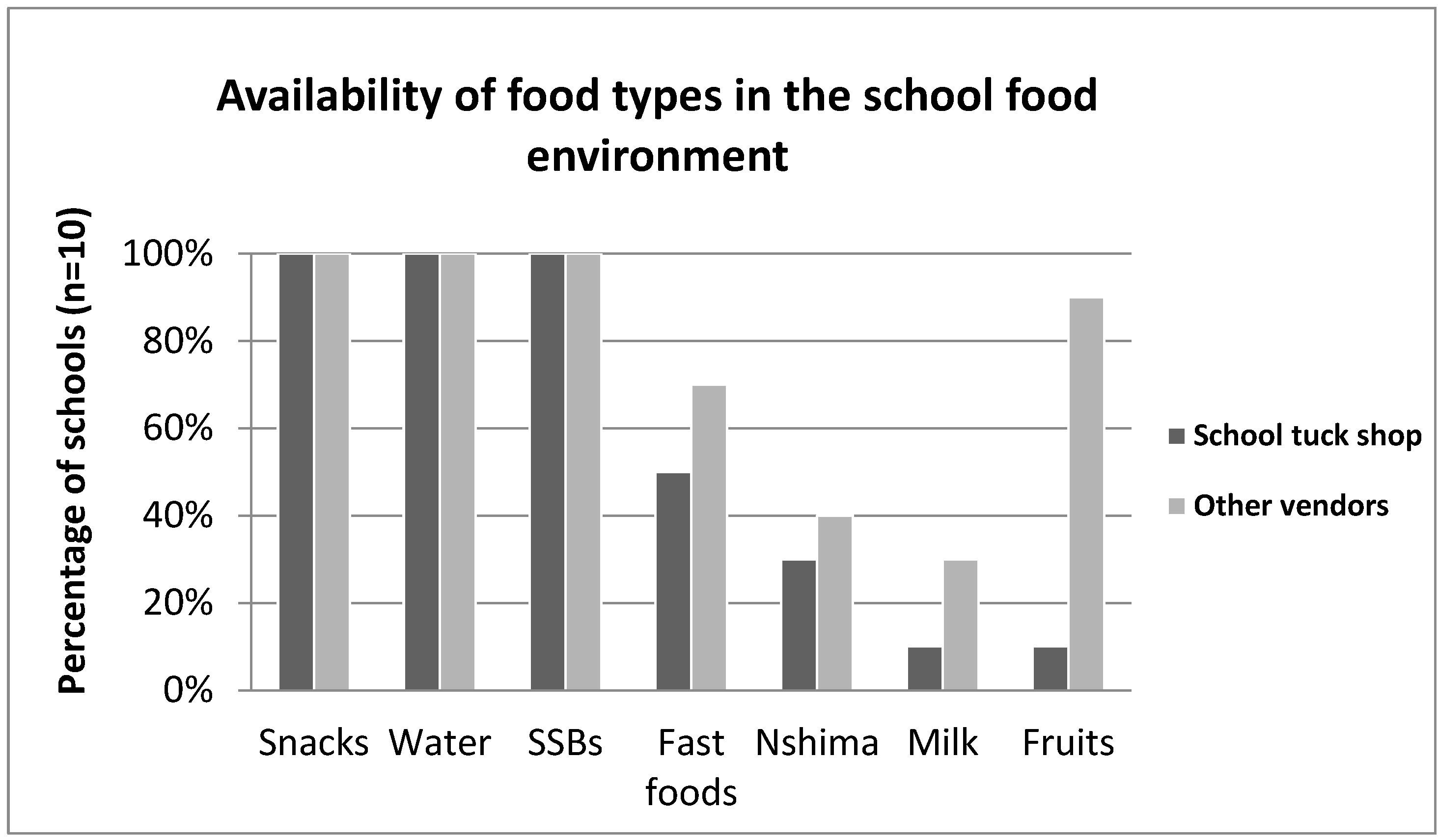
3.1. Description of Food Sold in the School Environment
3.2. Focus Group Participants’ Characteristics
3.3. Drivers of Food Choice
3.3.1. Internal Drivers of Food Choice
- Desirability
“Purchasing healthy food is also nice because you get to standout because most people like to eat junk food and when you are just eating healthy food you look unique and it’s just nice when you feel good about yourself.” Female, 15 years, Low density neighborhood school.
“Mostly people my age are not actually aware of what healthy foods they need to eat because mostly parents or guardians are usually busy and they don’t have time for us to educate us on what we are supposed to eat” Female, 16 years, Medium density neighborhood school.
- Affordability
- Accessibility
“When they [parents] were younger I think the availability of junk foods wasn’t as common as it is here for us. For them it was harder and more expensive to find junk foods like burgers unlike foods that is more traditional. For us you can just go anywhere and you find a Hungry Lion store”. Male participant, 17 years, High density neighborhood school.
- Convenience
3.3.2. External Drivers of Food Choice
- Price
“Healthy foods are very expensive when you compare them to these junky foods that we like to buy. For example, one apple is K3 and then I think if am going to buy Jiggies which are K0.50, I am going to have maybe about six! So I’ll decide to buy those ones [jiggies] which I am going to have more rather than buying the apple” Male, 15 years, Medium density neighborhood school.
- Availability
“Personally, I would like them to sell fruits in school because some of us are just gaining weight at school because of the junk foods they are selling.” Female, 14 years, Low density neighborhood school.
- Marketing
“As for me, let me give an example of tamarind: I heard Kim Kardashian on that show [Keeping up with the Kardashians] say that for her body to be like that, she eats tamarind. If she eats that, even us to keep our bodies the way she looks, now we start eating tamarind” Female, 14 years, Medium density neighborhood school.
“I have seen road shows… It’s when they bring trucks with music such that when you go up on the platform in the truck and dance; you are given mojo [a brand of carbonated drink] so that know that there are drinks like mojo.” Male, 17 Years, Medium density neighborhood school.
- Vendor and product properties
“We look at the quality, the way products are looking. This is important because I cannot buy food anyhow; I have to buy food that is profitable to my health, not eating because you just want to eat. Nowadays there are a lot of cheap things that are of low quality.” Female, 15, High density neighborhood school.
4. Discussion
4.1. Improving Availability of Healthy Food
4.2. Improving Affordability of Healthy Food
4.3. Regulating the Marketing of Unhealthy Foods
4.4. Improving Desirability of Healthy Food
4.5. Strengths and Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baird, J.; Jacob, C.; Barker, M.; Fall, C.H.D.; Hanson, M.; Harvey, N.C.; Inskip, H.M.; Kumaran, K.; Cooper, C. Developmental origins of health and disease: A lifecourse approach to the prevention of non-communicable diseases. Healthcare 2017, 5, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Adolescent Health. World Health Organization. Published 2021. Available online: https://www.who.int/health-topics/adolescent-health#tab=tab_1 (accessed on 25 October 2021).
- Fitzgerald, A.; Heary, C.; Nixon, E.; Kelly, C. Factors influencing the food choices of Irish children and adolescents: A qualitative investigation. Health Promot. Int. 2010, 25, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Munt, A.E.; Partridge, S.R.; Allman-Farinelli, M. The barriers and enablers of healthy eating among young adults: A missing piece of the obesity puzzle: A scoping review. Obes. Rev. 2017, 18, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Majabadi, H.A.; Solhi, M.; Montazeri, A.; Shojaeizadeh, D.; Nejat, S.; Farahani, F.K.; Djazayeri, A. Factors Influencing Fast-Food Consumption Among Adolescents in Tehran: A Qualitative Study. Iran Red Crescent Med. J. 2016, 18, e23890. [Google Scholar] [CrossRef] [Green Version]
- Trübswasser, U.; Baye, K.; Holdsworth, M.; Loeffen, M.; Feskens, E.J.; Talsma, E.F. Assessing factors influencing adolescents’ dietary behaviours in urban Ethiopia using participatory photography. Public Health Nutr. 2021, 24, 3615–3623. [Google Scholar] [CrossRef] [PubMed]
- Counihan, C.; Van Esterik, P. Food and Culture: A Reader; Routledge: London, UK, 2012; pp. 1–19. [Google Scholar]
- Atkins, P.; Bowler, I. Food in Society: Economy, Culture, Geography; Routledge: London, UK, 2016; pp. 255–296. [Google Scholar]
- FAO. Influencing Food Environments for Healthy Diets; Food and Agriculture Organization of the United Nations: Rome, Italy, 2016; Available online: http://www.fao.org/3/a-i6484e.pdf (accessed on 12 December 2019).
- Martins, B.G.; Ricardo, C.Z.; Machado, P.P.; Rauber, F.; Azeredo, C.M.; Levy, R.B. Eating meals with parents is associated with better quality of diet for Brazilian adolescents. Cad. Saude Publica 2019, 35, e00153918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andreyeva, T.; Kelly, I.R.; Harris, J.L. Exposure to food advertising on television: Associations with children’s fast food and soft drink consumption and obesity. Econ. Hum. Biol. 2011, 9, 221–233. [Google Scholar] [CrossRef]
- Norman, J.; Kelly, B.; Boyland, E.; McMahon, A.T. The Impact of Marketing and Advertising on Food Behaviours: Evaluating the Evidence for a Causal Relationship. Curr. Nutr. Rep. 2016, 5, 139–149. [Google Scholar] [CrossRef] [Green Version]
- Potvin Kent, M.; Pauzé, E.; Roy, E.A.; de Billy, N.; Czoli, C. Children and adolescents’ exposure to food and beverage marketing in social media apps. Pediatr. Obes. 2019, 14, e12508. [Google Scholar] [CrossRef] [Green Version]
- Qutteina, Y.; Hallez, L.; Mennes, N.; De Backer, C.; Smits, T. What Do Adolescents See on Social Media? A Diary Study of Food Marketing Images on Social Media. Front. Psychol. 2019, 10, 2637. [Google Scholar] [CrossRef]
- Cruz, L. Legal Guide on School Food and Nutrition—Legislating for a Healthy School Food Environment; Food and Agriculture Organization of the United Nations: Rome, Italy, 2020; Available online: http://www.fao.org/3/ca9730en/CA9730EN.pdf (accessed on 5 May 2021).
- Azeredo, C.M.; de Rezende, L.F.M.; Canella, D.S.; Claro, R.M.; Peres, M.F.T.; Luiz, O.D.C.; França-Junior, I.; Kinra, S.; Hawkesworth, S.; Levy, R.B. Food environments in schools and in the immediate vicinity are associated with unhealthy food consumption among Brazilian adolescents. Prev. Med. 2016, 88, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Kelly, C.; Callaghan, M.; Molcho, M.; Nic Gabhainn, S.; Alforque Thomas, A. Food environments in and around post-primary schools in Ireland: Associations with youth dietary habits. Appetite 2019, 132, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Güngör, N.K. Overweight and obesity in children and adolescents. J. Clin. Res. Pediatr. Endocrinol. 2014, 6, 129–143. [Google Scholar] [CrossRef]
- Driessen, C.E.; Cameron, A.J.; Thornton, L.E.; Lai, S.K.; Barnett, L.M. Effect of changes to the school food environment on eating behaviours and/or body weight in children: A systematic review. Obes. Rev. 2014, 15, 968–982. [Google Scholar] [CrossRef] [PubMed]
- High Level Panel of Experts. Nutrition and Food Systems. A Report by the High Level Panel of Experts on Food Security and Nutrition of the Committee on World Food Security. 2017. Available online: http://www.fao.org/3/a-i7846e.pdf (accessed on 20 September 2019).
- Battersby, J.; Watson, V. Urban Food Systems Governance and Poverty in African Cities; Routledge: London, UK, 2019; Available online: http://library.oapen.org/handle/20.500.12657/29590 (accessed on 28 February 2022).
- WHO. Report of the Commission on Ending Childhood Obesity. 2016. Available online: http://apps.who.int/iris/bitstream/handle/10665/204176/9789241510066_eng.pdf (accessed on 24 November 2021).
- Laar, A.; Barnes, A.; Aryeetey, R.; Tandoh, A.; Bash, K.; Mensah, K.; Zotor, F.; Vandevijvere, S.; Holdsworth, M. Implementation of healthy food environment policies to prevent nutrition-related non-communicable diseases in Ghana: National experts’ assessment of government action. Food Policy 2020, 93, 101907. [Google Scholar] [CrossRef] [PubMed]
- McIsaac, J.-L.D.; Spencer, R.; Chiasson, K.; Kontak, J.; Kirk, S.F.L. Factors Influencing the Implementation of Nutrition Policies in Schools: A Scoping Review. Health Educ. Behav. 2019, 46, 224–250. [Google Scholar] [CrossRef]
- Ng, S.; Yeatman, H.; Kelly, B.; Sankaranarayanan, S.; Karupaiah, T. Identifying barriers and facilitators in the development and implementation of government-led food environment policies: A systematic review. Nutr. Rev. 2022, nuac016. [Google Scholar] [CrossRef]
- Nguyen, B.; Cranney, L.; Bellew, B.; Thomas, M. Implementing Food Environment Policies at Scale: What Helps? What Hinders? A Systematic Review of Barriers and Enablers. Int. J. Environ. Res. Public Health 2021, 18, 10346. [Google Scholar] [CrossRef]
- Harris, J.; Chisanga, B.; Drimie, S.; Kennedy, G. Nutrition transition in Zambia: Changing food supply, food prices, household consumption, diet and nutrition outcomes. Food Secur. 2019, 11, 371–387. [Google Scholar] [CrossRef] [Green Version]
- MOH. WHO STEPs Survey for Non-Communicable Diseases and Risk Factors 2017; Minstry of Health: Lusaka, Zambia, 2018. Available online: https://www.afro.who.int/sites/default/files/2019-05/Zambia%20NCD%20STEPS%20Survey%20Report%202018.pdf (accessed on 21 September 2019).
- Central Statistical Office, Ministry of Health, ICF. Zambia Demographic and Health Survey 2018: Key Indicators; Central Statistical Office: Lusaka, Zambia; Ministry of Health: Lusaka, Zambia; ICF: Rockville, MD, USA, 2019. Available online: https://dhsprogram.com/pubs/pdf/PR113/PR113.pdf (accessed on 21 September 2019).
- Mukanu, M.; Mchiza, Z.; Delobelle, P.; Thow, A.M. Status of healthy diets and food environments policies in Zambia: A policy content analysis. Unpublished.
- Turner, C.; Kalamatianou, S.; Drewnowski, A.; Kulkarni, B.; Kinra, S.; Kadiyala, S. Food Environment Research in Low- and Middle-Income Countries: A Systematic Scoping Review. Adv. Nutr. 2020, 11, 387–397. [Google Scholar] [CrossRef]
- Turner, C.; Aggarwal, A.; Walls, H.; Herforth, A.; Drewnowski, A.; Coates, J.; Kalamatianou, S.; Kadiyala, S. Concepts and critical perspectives for food environment research: A global framework with implications for action in low-and middle-income countries. Glob. Food Secur. 2018, 18, 93–101. [Google Scholar] [CrossRef]
- Simwanda, M.; Murayama, Y. Integrating Geospatial Techniques for Urban Land Use Classification in the Developing Sub-Saharan African City of Lusaka, Zambia. ISPRS Int. J. Geo-Inf. 2017, 6, 102. [Google Scholar] [CrossRef] [Green Version]
- Mweemba, A.M.; Webb, E. Residential area as proxy for socio-economic status, paediatric mortality and birth weight in Lusaka, Zambia. J. Trop. Pediatrics 2008, 54, 406–409. [Google Scholar] [CrossRef] [PubMed]
- Sofaer, S. Qualitative research methods. Int. J. Qual. Health Care 2002, 14, 329–336. [Google Scholar] [CrossRef] [Green Version]
- Phellas, C.N.; Bloch, A.; Seale, C. Structured methods: Interviews, questionnaires and observation. Res. Soc. Cult. 2011, 3, 23–32. [Google Scholar]
- Jamshed, S. Qualitative research method-interviewing and observation. J. Basic Clin. Pharm. 2014, 5, 87. [Google Scholar] [CrossRef] [Green Version]
- Fereday, J.; Muir-Cochrane, E. Demonstrating rigor using thematic analysis: A hybrid approach of inductive and deductive coding and theme development. Int. J. Qual. Methods 2006, 5, 80–92. [Google Scholar] [CrossRef]
- StataCorp. Stata Statistical Software; StataCorp LLC: College Station, TX, USA, 2017. [Google Scholar]
- Wojcicki, J.M.; Elwan, D. Primary school nutrition and tuck shops in Hhoho, Swaziland. J. Child Nutr. Manag. Internet. 2014, 38. [Google Scholar]
- Faber, M.; De Villiers, A.; Hill, J.; Van Jaarsveld, P.J.; Okeyo, A.P.; Seekoe, E. Nutrient profile and energy cost of food sold by informal food vendors to learners in primary and secondary schools in the Eastern Cape, South Africa. Public Health Nutr. 2019, 22, 521–530. [Google Scholar] [CrossRef]
- Brambila-Macias, J.; Shankar, B.; Capacci, S.; Mazzocchi, M.; Perez-Cueto, F.J.; Verbeke, W.; Traill, W.B. Policy Interventions to Promote Healthy Eating: A Review of What Works, What Does Not, and What is Promising. Food Nutr. Bull. 2011, 32, 365–375. [Google Scholar] [CrossRef]
- Bihan, H.; Méjean, C.; Castetbon, K.; Faure, H.; Ducros, V.; Sedeaud, A.; Galan, P.; Le Clésiau, H.; Péneau, S.; Hercberg, S. Impact of fruit and vegetable vouchers and dietary advice on fruit and vegetable intake in a low-income population. Eur. J. Clin. Nutr. 2012, 66, 369–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budd, N.; Cuccia, A.; Jeffries, J.K.; Prasad, D.; Frick, K.D.; Powell, L.; Katz, F.A.; Gittelsohn, J. B’More Healthy: Retail Rewards--design of a multi-level communications and pricing intervention to improve the food environment in Baltimore City. BMC Public Health 2015, 15, 283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global Panel. Improving Nutrition through Enhanced Food Environments; Global Panel on Agriculture and Food Systems for Nutrition: London, UK, 2017; Available online: https://glopan.org/sites/default/files/FoodEnvironmentsBrief.pdf (accessed on 6 May 2021).
- Micha, R.; Karageorgou, D.; Bakogianni, I.; Trichia, E.; Whitsel, L.P.; Story, M.; Peñalvo, J.L.; Mozaffarian, D. Effectiveness of school food environment policies on children’s dietary behaviors: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0194555. [Google Scholar] [CrossRef]
- Bekker, F.; Marais, M.; Koen, N. The provision of healthy food in a school tuck shop: Does it influence primary-school students’ perceptions, attitudes and behaviours towards healthy eating? Public Health Nutr. 2017, 20, 1257–1266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MoE. National School Health and Nutrition Policy. Published online 2006. Available online: https://extranet.who.int/nutrition/gina/sites/default/files/ZMB%202006%20School%20Health%20and%20Nutrition%20Policy%20%202006.pdf (accessed on 28 October 2019).
- Rathi, N.; Riddell, L.; Worsley, A. Food consumption patterns of adolescents aged 14–16 years in Kolkata, India. Nutr. J. 2017, 16, 50. [Google Scholar] [CrossRef]
- Reeve, E.; Thow, A.M.; Bell, C.; Engelhardt, K.; Gamolo-Naliponguit, E.C.; Go, J.J.; Sacks, G. Implementation lessons for school food policies and marketing restrictions in the Philippines: A qualitative policy analysis. Glob. Health 2018, 14, 8. [Google Scholar] [CrossRef]
- Demmler, K.M.; Ecker, O.; Qaim, M. Supermarket shopping and nutritional outcomes: A panel data analysis for urban Kenya. World Dev. 2018, 102, 292–303. [Google Scholar] [CrossRef]
- Westbury, S.; Ghosh, I.; Jones, H.M.; Mensah, D.; Samuel, F.; Irache, A.; Azhar, N.; Al-Khudairy, L.; Iqbal, R.; Oyebode, O. The influence of the urban food environment on diet, nutrition and health outcomes in low-income and middle-income countries: A systematic review. BMJ Glob. Health 2021, 6, e006358. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, L.; Zhu, J.; Gao, L.; Wang, Y. Growing fast food consumption and obesity in Asia: Challenges and implications. Soc. Sci. Med. 2021, 269, 113601. [Google Scholar] [CrossRef]
- Fisher, L.; Dahal, M.; Hawkes, S.; Puri, M.; Buse, K. Barriers and opportunities to restricting marketing of unhealthy foods and beverages to children in Nepal: A policy analysis. BMC Public Health 2021, 21, 1351. [Google Scholar] [CrossRef]
- Mukanu, M.M.; Zulu, J.M.; Mweemba, C.; Mutale, W. Responding to non-communicable diseases in Zambia: A policy analysis. Health Res. Policy Syst. 2017, 15, 34. [Google Scholar] [CrossRef] [PubMed]
- Steyn, N.P.; Labadarios, D.; Nel, J.H. Factors which influence the consumption of street foods and fast foods in South Africa--a national survey. Nutr. J. 2011, 10, 104. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.C.; Muñoz-Mora, J.C.; Rasmussen, L.V.; Zezza, A. Do Trees on Farms Improve Household Well-Being? Evidence From National Panel Data in Uganda. Front. For. Glob. Chang. 2020, 3, 101. [Google Scholar] [CrossRef]
- Mukanu, M.; Delobelle, P.; Thow, A.M.; Mutale, W.; Mchiza, Z. Dietary patterns and school food environment of school going adolescents in Urban Zambia. Unpublished.
- WHO. Fiscal Policies for Diet and Prevention of Noncommunicable Diseases; World Health Organization: Geneva, Switzerland, 2015; Available online: https://apps.who.int/iris/bitstream/handle/10665/250131/9789241511247-eng.pdf?sequence=1 (accessed on 28 April 2019).
- Colchero, M.A.; Rivera-Dommarco, J.; Popkin, B.M.; Ng, S.W. In Mexico, evidence of sustained consumer response two years after implementing a sugar-sweetened beverage tax. Health Aff. 2017, 36, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Pell, D.; Mytton, O.; Penney, T.L.; Briggs, A.; Cummins, S.; Penn-Jones, C.; Rayner, M.; Rutter, H.; Scarborough, P.; Sharp, S.J.; et al. Changes in soft drinks purchased by British households associated with the UK soft drinks industry levy: Controlled interrupted time series analysis. BMJ 2021, 372, n254. [Google Scholar] [CrossRef]
- Essman, M.; Taillie, L.S.; Frank, T.; Ng, S.W.; Popkin, B.M.; Swart, E.C. Taxed and untaxed beverage intake by South African young adults after a national sugar-sweetened beverage tax: A before-and-after study. PLoS Med. 2021, 18, e1003574. [Google Scholar] [CrossRef]
- Tselengidis, A.; Östergren, P.O. Lobbying against sugar taxation in the European Union: Analysing the lobbying arguments and tactics of stakeholders in the food and drink industries. Scand. J. Public Health 2019, 47, 565–575. [Google Scholar] [CrossRef]
- Kruger, P.; Abdool Karim, S.; Tugendhaft, A.; Goldstein, S. An Analysis of the Adoption and Implementation of A Sugar-Sweetened Beverage Tax in South Africa: A Multiple Streams Approach. Health Syst. Reform. 2021, 7, e1969721. [Google Scholar] [CrossRef]
- Hangoma, P.; Bulawayo, M.; Chewe, M.; Stacey, N.; Downey, L.; Chalkidou, K.; Hofman, K.; Kamanga, M.; Kaluba, A.; Surgey, G. The potential health and revenue effects of a tax on sugar sweetened beverages in Zambia. BMJ Glob. Health 2020, 5, e001968. [Google Scholar] [CrossRef]
- Mukanu, M.M.; Abdool Karim, S.; Hofman, K.; Erzse, A.; Thow, A.M. Nutrition related non-communicable diseases and sugar sweetened beverage policies: A landscape analysis in Zambia. Glob. Health Action 2020, 14, 1872172. [Google Scholar] [CrossRef]
- Bosire, E.N.; Stacey, N.; Mukoma, G.; Tugendhaft, A.; Hofman, K.; Norris, S.A. Attitudes and perceptions among urban South Africans towards sugar-sweetened beverages and taxation. Public Health Nutr. 2020, 23, 374–383. [Google Scholar] [CrossRef] [PubMed]
- An, R. Effectiveness of Subsidies in Promoting Healthy Food Purchases and Consumption: A Review of Field Experiments. Public Health Nutr. 2013, 16, 1215–1228. [Google Scholar] [CrossRef] [PubMed]
- Herman, D.R.; Harrison, G.G.; Afifi, A.A.; Jenks, E. Effect of a Targeted Subsidy on Intake of Fruits and Vegetables Among Low-Income Women in the Special Supplemental Nutrition Program for Women, Infants, and Children. Am. J. Public Health 2008, 98, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Jomaa, L.H.; McDonnell, E.; Probart, C. School feeding programs in developing countries: Impacts on children’s health and educational outcomes. Nutr. Rev. 2011, 69, 83–98. [Google Scholar] [CrossRef]
- Drake, L.; Woolnough, A.; Bundy, D.; Burbano, C. Global School Feeding Sourcebook: Lessons from 14 Countries; World Scientific: Singapore, 2016. [Google Scholar]
- Chakrabarti, S.; Scott, S.P.; Alderman, H.; Menon, P.; Gilligan, D.O. Intergenerational nutrition benefits of India’s national school feeding program. Nat. Commun. 2021, 12, 4248. [Google Scholar] [CrossRef] [PubMed]
- Nikoi, C.; Cammelbeeck, S. Country Programmes Zambia; World Food Programme: Rome, Italy, 2020. [Google Scholar]
- Ustjanauskas, A.E.; Harris, J.L.; Schwartz, M.B. Food and beverage advertising on children’s web sites. Pediatr. Obes. 2014, 9, 362–372. [Google Scholar] [CrossRef]
- Sacks, G.; Looi, E.S.Y. The Advertising Policies of Major Social Media Platforms Overlook the Imperative to Restrict the Exposure of Children and Adolescents to the Promotion of Unhealthy Foods and Beverages. Int. J. Environ. Res. Public Health 2020, 17, 4172. [Google Scholar] [CrossRef]
- WHO. Set of Recommendations on the Marketing of Foods and Non-Alcoholic Beverages to Children. Published online 2010. Available online: http://apps.who.int/iris/bitstream/handle/10665/44416/9789241500210_eng.pdf?sequence=1 (accessed on 6 May 2021).
- Kovic, Y.; Noel, J.K.; Ungemack, J.A.; Burleson, J.A. The impact of junk food marketing regulations on food sales: An ecological study. Obes. Rev. 2018, 19, 761–769. [Google Scholar] [CrossRef]
- Correa, T.; Reyes, M.; Taillie, L.S.; Corvalán, C.; Dillman Carpentier, F.R. Food Advertising on Television Before and After a National Unhealthy Food Marketing Regulation in Chile, 2016–2017. Am. J. Public Health 2020, 110, 1054–1059. [Google Scholar] [CrossRef]
- Phulkerd, S.; Sacks, G.; Vandevijvere, S.; Worsley, A.; Lawrence, M. Barriers and potential facilitators to the implementation of government policies on front-of-pack food labeling and restriction of unhealthy food advertising in Thailand. Food Policy 2017, 71, 101–110. [Google Scholar] [CrossRef]
- Hebden, L.A.; King, L.; Grunseit, A.; Kelly, B.; Chapman, K. Advertising of fast food to children on Australian television: The impact of industry self-regulation. Med. J. Aust. 2011, 195, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Ronit, K.; Jensen, J.D. Obesity and industry self-regulation of food and beverage marketing: A literature review. Eur. J. Clin. Nutr. 2014, 68, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Erzse, A.; Christofides, N.; Stacey, N.; Lebard, K.; Foley, L.; Hofman, K. Availability and advertising of sugar sweetened beverages in South African public primary schools following a voluntary pledge by a major beverage company: A mixed methods study. Glob. Health Action 2021, 14, 1898130. [Google Scholar] [CrossRef] [PubMed]
- Funduluka, P.; Bosomprah, S.; Chilengi, R.; Mugode, R.H.; Bwembya, P.A.; Mudenda, B. Marketing of breast-milk substitutes in Zambia: Evaluation of compliance to the international regulatory code. J. Public Health 2018, 40, e1–e7. [Google Scholar] [CrossRef]
- Dunlop, S.; Freeman, B.; Jones, S.C. Marketing to Youth in the Digital Age: The Promotion of Unhealthy Products and Health Promoting Behaviours on Social Media. Media Commun. 2016, 4, 35–49. [Google Scholar] [CrossRef]
- De Veirman, M.; Hudders, L.; Nelson, M.R. What Is Influencer Marketing and How Does It Target Children? A Review and Direction for Future Research. Front. Psychol. 2019, 10, 2685. [Google Scholar] [CrossRef] [Green Version]
- van der Bend, D.L.M.; Jakstas, T.; van Kleef, E.; Shrewsbury, V.A.; Bucher, T. Making sense of adolescent-targeted social media food marketing: A qualitative study of expert views on key definitions, priorities and challenges. Appetite 2022, 168, 105691. [Google Scholar] [CrossRef]
- Chau, M.M.; Burgermaster, M.; Mamykina, L. The use of social media in nutrition interventions for adolescents and young adults—A systematic review. Int. J. Med. Inf. 2018, 120, 77–91. [Google Scholar] [CrossRef]
- Januraga, P.P.; Izwardi, D.; Crosita, Y.; Indrayathi, P.A.; Kurniasari, E.; Sutrisna, A.; Tumilowicz, A. Qualitative evaluation of a social media campaign to improve healthy food habits among urban adolescent females in Indonesia. Public Health Nutr. 2021, 24, s98–s107. [Google Scholar] [CrossRef]
- Boles, M.; Adams, A.; Gredler, A.; Manhas, S. Ability of a mass media campaign to influence knowledge, attitudes, and behaviors about sugary drinks and obesity. Prev. Med. 2014, 67 (Suppl. 1), S40–S45. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| School Code | Population Density of School Neighborhood | Ownership |
|---|---|---|
| 1 | High density | Government |
| 2 | High Density | Government |
| 3 | High Density | Government |
| 4 | Medium density | Government |
| 5 | Medium density | Government |
| 6 | Medium density | Government |
| 7 | Low density | Government |
| 8 | Low density | Government |
| 9 | Low density | Government |
| 10 | Low density | Private |
| Example of Codes | Sub Themes | Themes (Based on the Conceptual Framework) |
|---|---|---|
| Taste and preference | Desirability |
| Culture | Desirability |
| Nutrition related knowledge | Desirability |
| Affordability | |
| Accessibility | |
| Convenience | |
| Price | |
| Availability | |
| Marketing | |
| Vendor and product properties |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mukanu, M.M.; Thow, A.M.; Delobelle, P.; Mchiza, Z.J.-R. School Food Environment in Urban Zambia: A Qualitative Analysis of Drivers of Adolescent Food Choices and Their Policy Implications. Int. J. Environ. Res. Public Health 2022, 19, 7460. https://doi.org/10.3390/ijerph19127460
Mukanu MM, Thow AM, Delobelle P, Mchiza ZJ-R. School Food Environment in Urban Zambia: A Qualitative Analysis of Drivers of Adolescent Food Choices and Their Policy Implications. International Journal of Environmental Research and Public Health. 2022; 19(12):7460. https://doi.org/10.3390/ijerph19127460
Chicago/Turabian StyleMukanu, Mulenga Mary, Anne Marie Thow, Peter Delobelle, and Zandile June-Rose Mchiza. 2022. "School Food Environment in Urban Zambia: A Qualitative Analysis of Drivers of Adolescent Food Choices and Their Policy Implications" International Journal of Environmental Research and Public Health 19, no. 12: 7460. https://doi.org/10.3390/ijerph19127460
APA StyleMukanu, M. M., Thow, A. M., Delobelle, P., & Mchiza, Z. J.-R. (2022). School Food Environment in Urban Zambia: A Qualitative Analysis of Drivers of Adolescent Food Choices and Their Policy Implications. International Journal of Environmental Research and Public Health, 19(12), 7460. https://doi.org/10.3390/ijerph19127460