
A Systematic Review of Associations between Energy Use, Fuel Poverty, Energy Efficiency Improvements and Health


Abstract
:1. Introduction
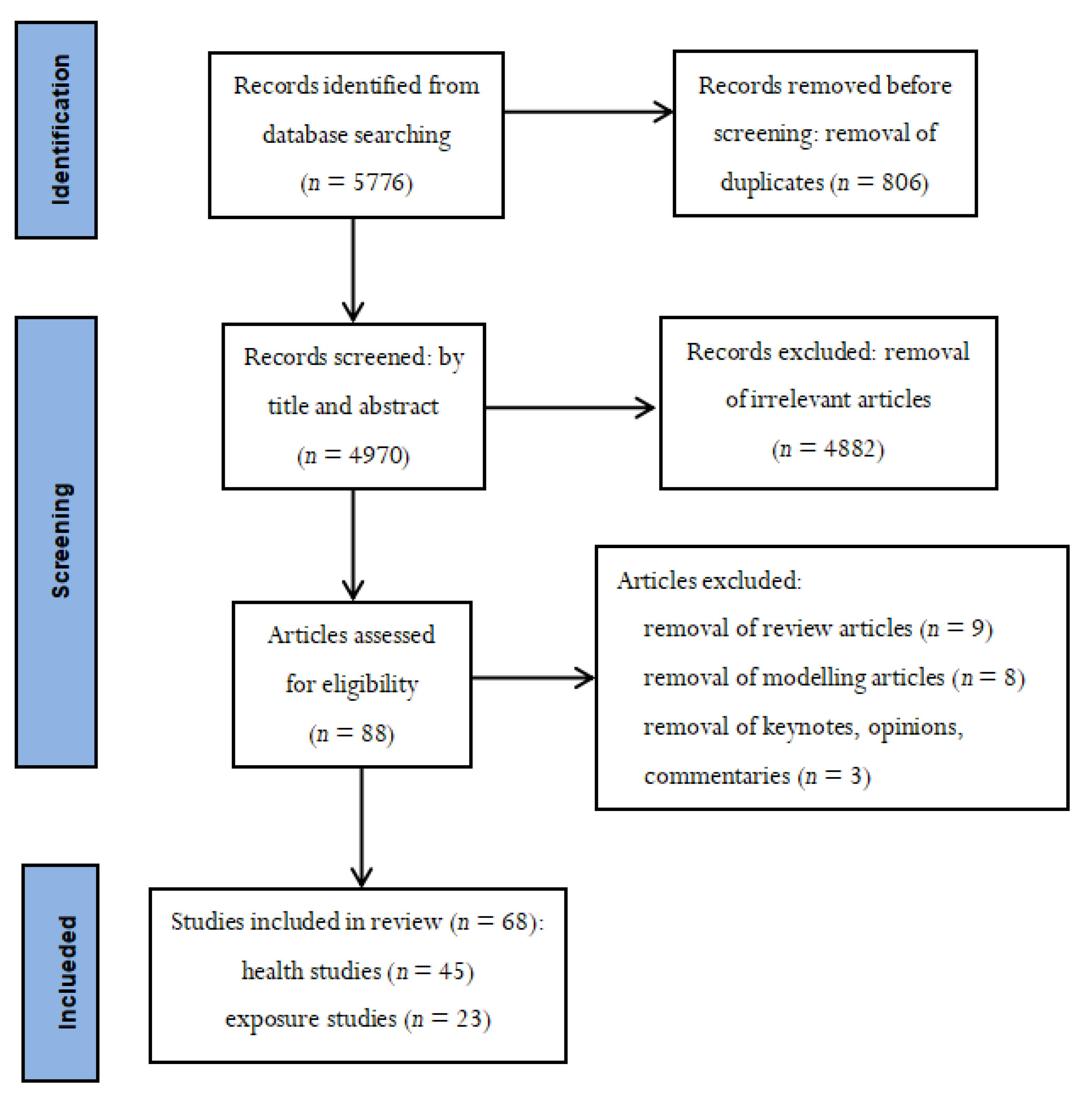
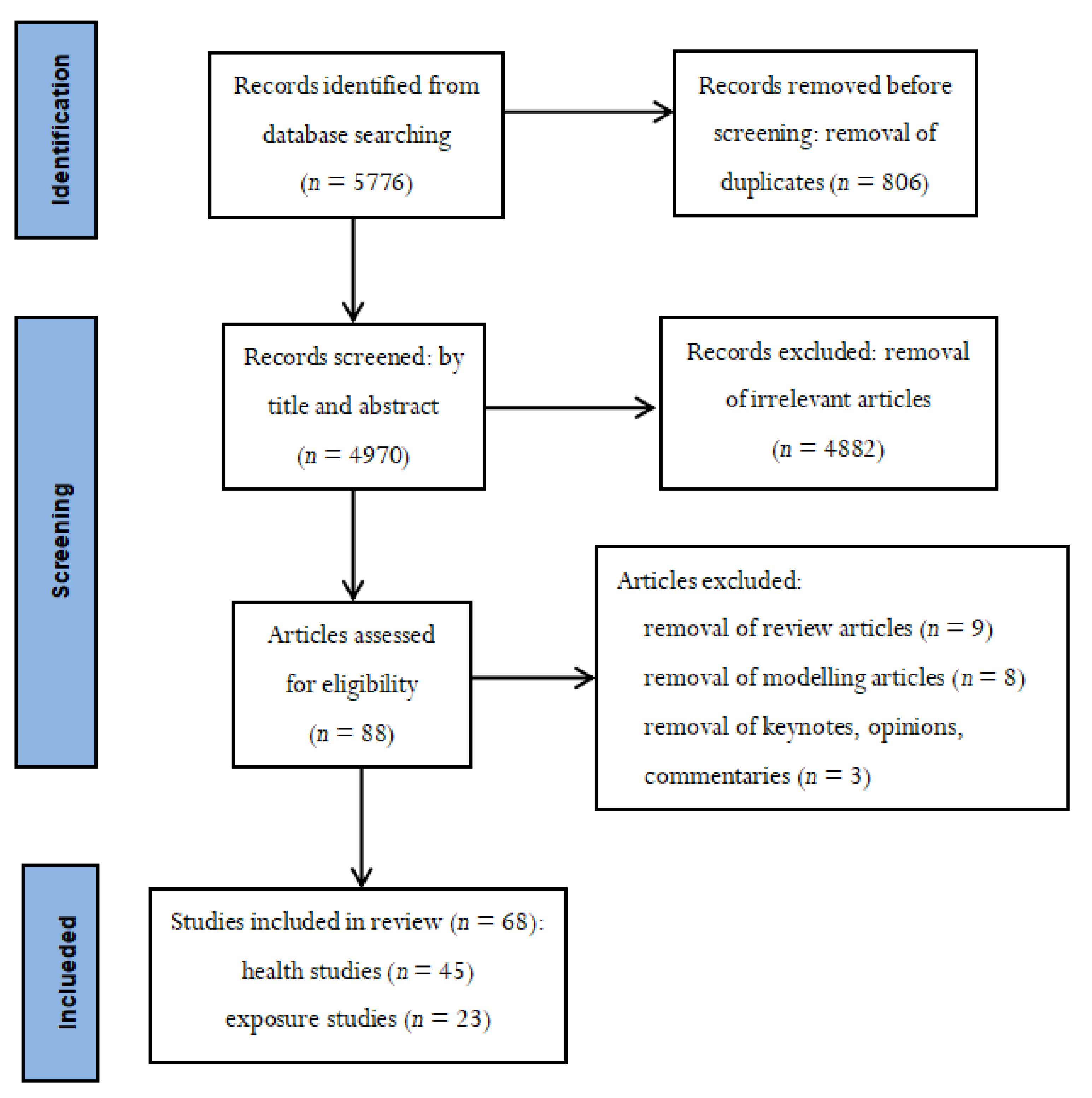
2. Methods
- The articles should have studied associations between energy aspects in buildings and health;
- The articles should be written in English;
- The articles should not be keynotes, opinions, commentaries, reviews, or modelling studies.
3. Results
3.1. Exposure Studies
3.1.1. Radon
3.1.2. Biological Agents
3.1.3. Chemical Substances and Particles
3.2. Health Studies
3.2.1. Green Building Health Studies
3.2.2. Fuel Poverty Studies
3.2.3. Cross-Sectional Health Studies
3.2.4. Longitudinal Health Studies
3.2.5. Intervention Health Studies
3.2.6. Energy Factors and Health
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

{kind=link}
| Author | Year | Country | Energy Aspects | Type of Study | Type of Buildings | Measured Exposure | Changes of Measured Exposure | Number of Households or Buildings | Main Results |
|---|---|---|---|---|---|---|---|---|---|
| Collignan et al. [19] | 2016 | France | Improved insulation, ventilation and window replacement | One time measurement | Residential buildings | Radon | 21% increase (median 147 Bq/m3) | 3233 households or 3233 buildings | Energy efficiency thermal retrofit (linked to reduced air permeability of the building envelope) can increase indoor radon concentration. |
| Symonds et al. [20] | 2019 | United Kingdom | Insulation in loft and wall, double glazing | Longitudinal | Residential buildings | Radon | Arith. Mean > 132–159.3 Bq/m3− | 470,689 households | Energy efficiency retrofit by improving insulation in loft and wall, and/or double glazing can increase radon concentrations, possibly due to increased airtightness. |
| Du et al. [29] | 2019 | Finland and Lithuania | Improved insulation in wall, roof, windows or balconies | Intervention | Residential buildings | Radon | Mean increase of 13.8 Bq/m3 (<100 Bq/m3) | 336 households or 65 buildings | In homes in Lithuania, energy efficiency retrofits without installation of mechanical ventilation increased indoor radon concentrations. |
| Pigg et al. [27] | 2018 | United States | Weatherization services | Intervention | Residential buildings | Radon | Increased by 0.14 ± 0.13 pCi/L (>100 Bq/m3 in high zone) | 514 households | Energy efficiency weatherization services (retrofits) can increase radon concentration. However, energy efficiency weatherization services with improved ventilation or ground covers can reduce radon concentration. |
| Meyer et al. [21] | 2019 | Germany | Air tightness windows and insulation of outer walls | One time measurement | Residential buildings | Radon | 40 Bq/m3 in non-refurbished vs. 69 Bq/m3 in refurbished | 150 households | Energy efficiency refurbishments of existing buildings without installation of ventilation systems can increase radon concentration, as compared to non-refurbished conventional buildings. |
| Pressyanov et al. [22] | 2015 | Bulgaria | New energy-efficient windows with plastic joinery | Intervention | Residential buildings | Radon | Rooms with radon increase was 193 Bq/m3 and rooms with no change was 45 Bq/m3 | 20 rooms or 16 buildings | Energy-efficient reconstructions with installation of new energy-efficient windows (linked to air tightness) can increase radon levels. |
| Vasilyev et al. [23] | 2017 | Russia | Energy efficiency insulation | One time measurement | Residential buildings | Radon | Arithmetic mean 38 Bq/m3 in conventional vs. 93 Bq/m3 in modern buildings | 81 buildings | Energy efficiency measures in buildings (linked to low indoor air exchange rate) can increase indoor radon concentration. |
| Yarmoshenko et al. [24] | 2014 | Russia | Energy efficiency insulation | Before-after | Residential buildings | Radon | Arithmetic mean 42 Bq/m3 in conventional vs. 133 Bq/m3 in modern buildings | 7 households or 7 buildings | Energy efficiency measures in buildings (linked to low indoor air exchange rate) can increase indoor radon concentration. |
| Vasilyev et al. [25] | 2015 | Russia | Energy efficiency insulation | Before-after | Residential buildings | Radon | Arithmetic mean 42 Bq/m3 in conventional vs. 166 Bq/m3 in modern buildings | 5 rooms or 5 buildings | Energy efficiency measures in buildings (linked to low indoor air exchange rate) can increase indoor radon concentration. |
| Burghele et al. [26] | 2020 | Romania | Installation of centralized and decentralized mechanical ventilation with heat recovery | Intervention | Residential buildings | Radon | Reduction was between 25% to 95% (Before >100 Bq/m3) | 10 households or 10 buildings | Sub-slab and sump depressurization, installation of centralized and decentralized mechanical ventilation with heat recovery can reduce radon concentrations. |
| Wallner et al. [28] | 2015 | Austria | Existing mechanical ventilation and natural ventilation | Before-after | Residential buildings | Radon | 17 Bq/m3 mechanical ventilation vs. 31 Bq/m3 natural ventilation | 123 households | Energy-efficient buildings with existing mechanical ventilation can reduce radon concentrations, as compared to conventional buildings without installation of mechanical ventilation, especially for radon. |
| Author | Year | Country | Energy Aspects | Type of Study | Type of Buildings | Measured Exposure | Changes of Measured Exposure | Number of Households | Main Results |
|---|---|---|---|---|---|---|---|---|---|
| Hirsch et al. [30] | 2000 | Germany | Installation of insulated windows and central heating systems | Intervention | Residential buildings | House dust mite Der f 1 and mould | Der f 1 in carpets 0.65 vs. 1.28, mattresses 1.56 vs. 2.40 μg/g; Aspergillus fumigatus 20 vs. 60 units/g | 98 households | Installation of insulated windows and central heating systems (linked to reduced ventilation) increased the concentration of the house dust mite allergen Der f 1 and the mould species Aspergillus fumigatus. |
| Sharpe et al. [31] | 2015 | United Kingdom | Fuel poverty | Cross-sectional | Social Residential buildings | Self-reported dampness and mould | No data | 671 households | Fuel poverty (linked to ineffective heating and ventilation practices) can increase indoor dampness and mould, regardless of the use of extractor fans. |
| Sharpe et al. [32] | 2016 | United Kingdom | Type of heating, glazing, insulation levels, energy efficiency ratings | Cross-sectional | Social Residential buildings | Self-reported allergenic mould | No data | 41 households | Energy efficiency improvement combined with increased ventilation flow rate reduced fungal contamination with Aspergillus/Penicillium mould species and Cladosporium spp. |
| Spertini et al. [33] | 2010 | Switzerland | Improved insulation, ventilation system with heat recovery and natural ventilation | One time measurement | Residential buildings | Self-reported house dust mites Der f 1 | Median 67 vs. 954 ng/g in mattresses and 20 vs. 174 ng/g in carpets | 289 households or 11 buildings | Buildings designed for low energy use with installation of mechanical ventilation reduced indoor relative air humidity as well as house dust mite allergen concentration both in mattresses and in carpets, as compared to control buildings. |
| Niculita-Hirzel et al. [34] | 2020 | Switzerland | Type of ventilation and energy consumption | One time measurement | Residential buildings | Fungal | Penicillium CFUs was lower | 149 households | Installation of mechanical ventilation in buildings reduced the infiltration of outdoor fungal particles, as compared to buildings with natural ventilation only. |
| Coombs et al. [35] | 2018 | United States | Green renovation with bathroom fans | Before-after | Residential buildings | Mould | 521,826 reads from green homes vs. 726,690 fungal reads from non-green homes | 52 households | The concentration of mould in air samples and door dust samples did not differ between green and non-green homes. However, green homes had a lower concentration of mould in bed samples. |
| Du et al. [29] | 2019 | Finland and Lithuania | Replacing windows and/or installation of heat recovery to the existing exhaust ventilation system | Intervention | Residential buildings | Airborne mould and bacterial | Fungal 0.6-log; Bacterial 0.6-log in gram-positive and 0.9-log in gram-negative bacterial (reduction in cells/m2) | 336 households or 65 buildings | In homes in Finland, energy efficiency retrofits with installation of mechanical ventilation reduced indoor concentrations of airborne mould and bacterial. |
| Wallner et al. [28] | 2015 | Austria | Mechanical ventilation and natural ventilation | Before-after | Residential buildings | Mould | 84% of rooms vs. 35% rooms | 123 households | Energy-efficient buildings with installation of mechanical ventilation reduced indoor mold spore concentration, as compared to conventional buildings without installation of mechanical ventilation. |
| Author | Year | Country | Energy Aspects | Type of Study | Type of Buildings | Measured Exposure | Changes of Measured Exposure | Number of Households or Buildings | Main Results |
|---|---|---|---|---|---|---|---|---|---|
| Derbez et al. [36] | 2018 | France | Installation of ventilation system or passive stack/hybrid ventilation | Before-after | Residential buildings | VOCs, aldehyde | Hexaldehyde: 37 vs. 17 µg/m3 in dwellings with/without flooring products | 72 households or 43 buildings | Low energy retrofit can increase the air concentration of alpha-pinene and hexaldehyde, possibly caused by the use of wood or wood-based products for the construction and insulation. |
| Du et al. [29] | 2019 | Finland and Lithuania | Replacing windows and/or installation of heat recovery to the existing exhaust ventilation system | Intervention | Residential buildings | BTEX and formaldehyde | Mean increase of 2.5 µg/m3 in BTEX | 336 households or 65 buildings | In homes in Finland, energy efficiency retrofits with existing mechanical ventilation increased indoor air concentrations of benzene, toluene, ethyl benzene and xylene (BTEX) but reduced indoor formaldehyde concentrations. |
| Leivo et al. [37] | 2018 | Finland and Lithuania | Installation of heat recovery to the existing exhaust ventilation system. Improved thermal insulation in wall, roof, windows or balconies | Intervention | Residential buildings | CO2 | Median: 775 vs. 956 PPM (1st); Median: 730 vs. 840 PPM (2nd) | 290 households or 66 buildings | In homes in Finland, energy efficiency retrofits with existing mechanical ventilation reduced CO2 concentration as compared to natural ventilation. In homes in Lithuania, improved insulation without installation of mechanical ventilation increased measured CO2 levels. |
| Coombs et al. [38] | 2016 | United States | Green renovation | Intervention | Residential buildings | Black carbon, formaldehyde | Black carbon averaging 682 vs. 2364 ng/m3; Formaldehyde 0.03 vs. 0.01 ppm | 42 households | Energy efficiency green renovation (linked to reduced ventilation) decreased indoor black carbon level in air from outdoor sources and increased indoor formaldehyde concentration. |
| Yang et al. [39] | 2020 | Switzerland | Thermal retrofit of roof, walls and floors, replacement of heating system, installation of mechanical ventilation system | One time measurement | Residential buildings | Aldehydes, VOCs | Formaldehyde 13 vs. 15; Toluene 16 vs. 26; Xylenes 1.4 vs. 5.8; Acrolein 0.4 vs. 0.6; D-limonene 7.9 vs. 11; Isobutane 3.4 vs. 10; Butane 8.8 vs. 2 (µg/m3) | 169 households | Energy efficiency thermal retrofit without installation of mechanical ventilation increased formaldehyde, aromatics, alkane, and levels of certain volatile organic compounds, as compared to new homes built with installed mechanical ventilation. |
| Verriele et al. [18] | 2016 | France | Controlled ventilation systems | Before-after | School buildings | CO2 | Peak Level 1000 ppm vs. 3800–5000 ppm | 10 school buildings | Low energy school buildings combined controlled mechanical ventilation systems and an adapted ventilation schedule can reduce CO2 levels. |
| Pigg et al. [27] | 2018 | United States | Weatherization services | Intervention | Residential buildings | CO | Peak Level 35 ppm vs. 13–20 ppm | 514 households | Energy efficiency weatherization services in homes without improved ventilation or ground covers can reduce exposure to CO. |
| Wallner et al. [28] | 2015 | Austria | Mechanical ventilation and natural ventilation | Before-after | Residential buildings | CO2, TVOC, aldehydes | CO2: 1360 vs. 1830 ppm and 1280 vs. 1740 ppm; TVOC: 300 vs. 560 µg/m3; aldehydes: 32 vs. 53 µg/m3 and 18 vs. 33 µg/m3 | 123 households | Energy efficient buildings with installation of mechanical ventilation reduced indoor concentrations of CO2, TVOC, aldehydes, and improved the measured indoor air quality in homes, as compared to conventional buildings without installation of mechanical ventilation. |
| Baumgartner et al. [40] | 2019 | China | Low-polluting semi gasifier cook stove with chimney, water heater and pelletized biomass fuel | Intervention | Residential buildings | PM2.5, black carbon | PM2.5 (46%), black carbon (55%) | 205 households | An energy intervention replacing low-polluting semi gasifier cook stove in rural buildings was associated with decreased exposures to PM2.5 and black carbon in winter but higher exposures to PM2.5 and black carbon in summer, as compared to untreated homes with traditional stoves. The negative effect could be caused by increased use of semi gasifier cook stove. |
| Author | Year | Country | Energy Aspects | Type of Study | Type of Buildings | Type of Health Variables | Number of Buildings | Number of Subjects | Main Results |
|---|---|---|---|---|---|---|---|---|---|
| Garland et al. [47] | 2013 | United States | Green buildings with LEED Credits | Intervention | Residential buildings | Self-reported asthma | 1 building | 18 children and adults | Green home buildings can reduce self-reported asthma symptoms. |
| Singh et al. [41] | 2010 | United States | Green buildings with LEED Credits | Longitudinal | Office buildings | Absenteeism due to self-reported asthma, respiratory allergies, depression and stress, and work productivity | 2 office buildings | 263 employees | Green office buildings can improve indoor environment quality and reduce absenteeism due to self-reported asthma, respiratory allergies, depression and stress, and moreover improve work productivity. |
| Breysse et al. [48] | 2011 | United States | Green efficiency renovation | Longitudinal | Residential buildings | Self-reported asthma, and non-asthma respiratory problems, overall health | 1 building | 80 children and adults | Among adults, green efficiency renovation in homes can reduce self-reported asthma. Green efficiency renovation in homes can improve self-reported overall health and reduce non-asthmatic respiratory symptoms in adults as well as in children. |
| Breysse et al. [49] | 2015 | United States | Green efficiency renovation | Intervention | Residential buildings | Self-reported mental and general physical health | 1 building | 612 older adults | Green efficiency renovation in homes can improve mental and general physical health. |
| Hedge et al. [44] | 2013 | United States | Green buildings with LEED Credits | Longitudinal | University buildings | Overall health, performance and work satisfaction | 2 university buildings | 44 employees | Green office buildings in a college campus improved health, performance and work satisfaction. |
| Hedge et al. [45] | 2014 | Canada | Green buildings with LEED Credits | Longitudinal | University buildings | Overall health, performance and study satisfaction | 3 university buildings | 319 employees | Green classrooms in an university campus improved health, performance and work satisfaction. |
| Gawande et al. [42] | 2020 | India | Green Office Buildings | cross-sectional | Office Buildings | SBS | 10 office buildings | 148 employees | No significant association between green buildings and sick building syndrome symptoms (SBS), compared with conventional buildings. |
| Author | Year | Country | Energy Aspects | Type of Study | Type of Buildings | Type of Health Variables | Number of Households | Number of Subjects | Main Results |
|---|---|---|---|---|---|---|---|---|---|
| Rudge et al. [50] | 2005 | United Kingdom | Fuel poverty | Longitudinal | Residential buildings | Winter respiratory disease | 220 households | 460 older adults | Fuel poverty in low-income homes can increase winter respiratory disease. |
| Webb et al. [51] | 2013 | United Kingdom | Fuel poverty | Cross-sectional | Residential buildings | Measured respiratory disease | 3763 households | 3763 older adults | Fuel poverty in low-income homes increase respiratory disease. |
| Sharpe et al. [52] | 2015 | United Kingdom | Type of heating, glazing, insulation, energy efficiency ratings | Cross-sectional | Social residential buildings | Doctor diagnosed asthma | 706 households | 944 adults | Energy efficiency improvement in social housing might increase current adult asthma. This may be due to increased exposure to physical, biological and chemical contaminants linked to inadequate heating, ventilation (fuel poverty behavior). |
| Poortinga et al. [53] | 2017 | United Kingdom | Loft insulation, cavity-wall insulation, external wall insulation | Repeated cross-sectional | Social residential buildings | General health, mental health, and social outcomes | Around 9200 households | 10,009 individuals | Energy efficiency improvements in social housing can improve respiratory symptoms. |
| Carlton et al. [54] | 2019 | United States | Home ventilation rate | Cross-sectional | Residential buildings | Respiratory symptoms | 216 households | 302 children and adults | High ventilation rates in low-income urban homes may increase chronic cough, asthma and asthma-like symptoms, probably caused by infiltration of outdoor air pollutants. |
| Howden-Chapman et al. [55] | 2011 | New Zealand | Improved insulation into existing houses; more effective heating in insulated houses | Intervention | Residential buildings | Respiratory symptoms | 1350 households; 409 households | 4407 children and adults; 409 children | Energy saving by using more effective heating in insulated low-income homes can improve health status and respiratory symptoms in children with asthma diagnosis. |
| Howden-Chapman et al. [56] | 2007 | New Zealand | Installation of a standard retrofit insulation package | Intervention | Residential buildings | Hospital admissions for respiratory conditions | 1350 households | 4407 children and adults | Energy saving by insulating existing houses in low-income communities can improve indoor environment and reduce hospital admissions for respiratory conditions. |
| Humphrey et al. [85] | 2020 | United States | Home ventilation rate | Cross-sectional | Residential buildings | Measured lung function | 187 households | 253 children and adults | High infiltration rate in low-income, urban, non-smoking homes can improve lung health. |
| Author | Year | Country | Energy Aspects | Type of Study | Type of Buildings | Type of Health Variables | Number of Households | Number of Subjects | Main Results |
|---|---|---|---|---|---|---|---|---|---|
| Thomson et al. [57] | 2017 | 32 European Countries | Fuel poverty | Cross-sectional | Residential buildings | General health and well-being | No data | 41,560 adults | Fuel poverty in low-income homes can reduce general health and emotional well-being. |
| Poortinga et al. [53] | 2017 | United Kingdom | Loft insulation, cavity-wall insulation, external wall insulation | Repeated cross-sectional | Social residential buildings | General health, mental health, and social outcomes | Around 9200 households | 10,009 individuals | Energy efficiency improvements in social housing can improve general health, mental health and social outcomes. However, installation of cavity wall insulation without installation of mechanical ventilation can reduce general health outcomes and social outcomes. |
| Ahrentzen et al. [58] | 2016 | United States | Insulation of roof and floor, improved thermal, air conditioner heating, cooling system, new ceiling fans, new windows | Intervention | Residential buildings | General health, emotional distress, sleep | 53 households | 57 older adults | Energy efficiency retrofits in low-income homes can improve general health, emotional distress, and sleep among the older adults. |
| Shortt et al. [59] | 2007 | United Kingdom | Installation of central heating systems or improved insulation | Intervention | Residential buildings | General health, well being | 100 households | 100 individuals | Energy efficiency intervention in fuel poverty homes can improve general health, well-being. |
| Howden-Chapman et al. [55] | 2011 | New Zealand | Improved insulation into existing houses; more effective heating in insulated houses | Intervention | Residential buildings | General health and well being | 1350 households; 409 households | 4407 children and adults; 409 children | Energy saving by improving insulation in low-income homes can improve general health and well-being and reduce hospitalization in children and adults. Energy saving by using more effective heating in insulated low-income homes can improve general health status in children. |
| Howden-Chapman et al. [56] | 2007 | New Zealand | Installation of a standard retrofit insulation package | Intervention | Residential buildings | General health and well being | 1350 households | 4407 children and adults | Energy saving by insulating existing houses in low-income communities can improve indoor environment so that improve self-reported health, wheezing, days off school and work. |
| Chapman et al. [60] | 2009 | New Zealand | Installation of a standard retrofit insulation package | Intervention | Residential buildings | General health, well being | 1350 households | 4407 children and adults | Energy saving by insulating existing houses in low-income communities can improve general health, as well as cost-benefit of general practitioner (GP) visits, hospitalizations, reduced time off work and school. |
| Grey et al. [61] | 2017 | United Kingdom | External wall insulation, central heating system, and installation of gas network | Intervention | Residential buildings | Well-being and psychosocial outcomes | 774 households | 776 individuals | Energy efficiency intervention in low-income homes can increase residential wellbeing and psychosocial-related health. |
| Poortinga et al. [62] | 2018 | United Kingdom | External wall insulation, photovoltaics, solar water heating, air source heat pumps, loft/rafter insulation | Intervention | Residential buildings | Well-being and psychosocial outcomes | 4968 households | 25,908 individuals | Energy efficiency intervention in low-income homes can improve well-being and psychosocial outcomes. |
| Pollard et al. [63] | 2019 | United Kingdom | Fuel poverty | Intervention | Residential buildings | Psychosocial outcomes | 22 households | 22 adults | Wearable telemetry (a thermometer with a low-temperature alarm) can raise awareness of the health effects of cold home among people living in fuel poverty (linked to psychosocial outcomes). |
| Author | Year | Country | Energy Aspects | Type of Study | Type of Buildings | Type of Health Variables | Number of Households | Number of Subjects | Main Results |
|---|---|---|---|---|---|---|---|---|---|
| Angelini et al. [64] | 2019 | United Kingdom | Winter fuel payment | Longitudinal | Residential buildings | Cold-related mortality, blood pressure, fibrinogen | 11,578 households | 18,813 adults | Low indoor air temperature in low-income homes can increase systolic and diastolic blood pressure and fibrinogen levels in blood samples (linked to cold-related mortality). |
| Sartini et al. [65] | 2018 | United Kingdom | Fuel poverty, types of home insulation and heating | Longitudinal | Residential buildings | Cold-related mortality | 1006 households | 1402 older men | Lack of insulation in low-income homes can increase cold-related mortality. |
| Peralta et al. [66] | 2017 | Spain | Energy efficient façade insulation retrofit | Longitudinal | Social residential buildings | Cold-related mortality | 2552 households | 2552 individuals | Energy efficient façade insulation retrofit in public housing can reduce cold-related mortality in women, but can increase cold-related total mortality in men. The health outcome for the gender difference is unclear. |
| Umishio et al. [67] | 2019 | Japan | Low insulation in cold homes | Cross-sectional | Residential buildings | Blood pressure | 1840 households | 2900 adults | Low indoor air temperature was higher associated with blood pressure and hypertension (linked to cold-related mortality). |
| López-Bueno et al. [68] | 2020 | Spain | Heating systems | Longitudinal | Residential buildings | Cold-related mortality | No data | No data | Districts with higher homes without a heating system had cold-related mortality. |
| Author | Year | Country | Energy Aspects | Type of Study | Type of Buildings | Type of Health Variables | Number of Buildings or Households | Number of Subjects | Main Results |
|---|---|---|---|---|---|---|---|---|---|
| Engvall et al. [69] | 2003 | Sweden | Type of ventilation and heating system, heat pumps, reconstruction and energy-saving measures | Cross-sectional | Residential buildings | Sick building syndrome (SBS) symptoms | 231 buildings | 3241 adults | In multi-family buildings, lack of a mechanical ventilation system and use of direct electric radiators were associated with increased prevalence of SBS-related symptoms. Major reconstruction and multiple sealing in multi-family buildings were associated with increased prevalence of SBS-related symptoms. |
| Smedje et al. [70] | 2017 | Sweden | Type of ventilation system and insulation level | Cross-sectional | Residential buildings | Sick building syndrome (SBS) symptoms | 605 buildings | 1160 adults | In single-family buildings, a lower U-value (higher insulation level) was associated with less SBS symptoms. |
| Norback et al. [71] | 2014 | Sweden | Type of ventilation and energy use for heating | Cross-sectional | Residential buildings | Doctor’s diagnosed asthma, allergy and self-reported pollen allergy, eczema | 472 buildings | 7554 adult | Multi-family buildings with balanced ventilation systems (supply/exhaust ventilation) had a higher prevalence of doctor diagnosed allergy, as compared to buildings with exhaust ventilation only. Buildings using more energy for heating were associated with less pollen allergy and eczema. |
| Wang et al. [72] | 2017 | Sweden | Type of ventilation and degree of insulation | Cross-sectional | Residential buildings | Doctors’ diagnosed asthma, self-reported asthma | 605 buildings | 1160 adults | Higher air exchange rate in the single-family residential homes was associated with less current asthma symptoms. |
| Sharpe et al. [73] | 2019 | United Kingdom | Energy efficiency ratings | Cross-sectional | Residential buildings | Asthma, chronic obstructive pulmonary disease, cardiovascular disease | No data | No data | Reduced home ventilation rates were associated with more asthma disease. Homes with more energy efficiency improvements may were associated with more admission rates for respiratory and cardiovascular diseases, possibly caused by reduced home ventilation flow rate. Energy efficiency measures can improve health outcomes, especially chronic respiratory illness. |
| Sobottka et al. [74] | 1996 | Germany | New windows and door, improved insulation and heating system | Cross-sectional | Residential buildings | Sick building syndrome (SBS) symptoms | 52 buildings | No data | Energy saving by installing new air tightness windows and door in homes was associated with more SBS-related health complaints. This may be due to fuel poverty behavior by not airing their flats sufficiently. |
| Bakke et al. [46] | 2008 | Norway | Lower air temperature | Cross-sectional | University buildings | Tear film stability, nasal patency | 4 university buildings | 173 employees | Lower air temperature in buildings at a university campus was associated with less tear film stability and more health problems. |
| Kennard et al. [75] | 2020 | United Kingdom | Space heating energy use | Cross-sectional | Residential buildings | Cold-mortality | 77,762 households | 77,762 adults | Higher thermal variety (linked to lower domestic demand temperatures) was associated with less morbidities related to cold-mortality. |
| Author | Year | Country | Energy Aspects | Type of Study | Type of Buildings | Type of Health Variables | Number of Buildings | Number of Subjects | Main Results |
|---|---|---|---|---|---|---|---|---|---|
| Wallner et al. [76] | 2017 | Austria | Mechanical ventilation and natural ventilation | Longitudinal | Residential buildings | General health and dry eye symptoms | 123 buildings | 575 children and adults | Energy efficient buildings combined with installation of mechanical ventilation can improve self-reported health but increase dry eye symptoms, as compared to conventional buildings with natural ventilation only. |
| Author | Year | Country | Energy Aspects | Type of Study | Type of Buildings | Type of Health Variables | Number of Buildings or Households | Number of Subjects | Main Results |
|---|---|---|---|---|---|---|---|---|---|
| Somerville et al. [77] | 2000 | United Kingdom | the installation of central heating systems | Intervention | Residential buildings | Respiratory symptoms | 59 households | 72 children with diagnosed asthma | Energy efficiency intervention in homes reduced respiratory symptoms, and reduced missed school days due to asthma in children with diagnosed asthma. |
| Barton et al. [78] | 2007 | United Kingdom | Central heating systems, ventilation, rewiring, insulation, and re-roofing | Intervention | Social residential buildings | Asthma, non-asthma-related respiratory disease | 119 households | 480 children and adults | Energy efficiency intervention in social housing reduced asthma symptoms, and non-asthmatic respiratory disease. |
| Osman et al. [79] | 2010 | United Kingdom | Central heating systems, installation of loft, under-floor and cavity wall insulation | Intervention | Residential buildings | Diagnosed chronic obstructive pulmonary disease (COPD) | 178 households | 178 older adults with COPD | Energy efficiency intervention in homes can improve respiratory health for elderly COPD patients. |
| Wilson et al. [80] | 2013 | United States | Insulation, heating equipment and ventilation improvements | Intervention | Residential buildings | Sinusitis, general health, satisfaction | 248 households | 323 children and adults | Energy efficiency retrofits work in homes can improve sinusitis, general health, satisfaction. |
| Haverinen-Shaughnessy et al. [81] | 2018 | Finland and Lithuania | Installation of heat recovery to the existing exhaust ventilation system. Improved thermal insulation in wall, roof, windows or balconies | Intervention | Residential buildings | Respiratory symptoms | 66 buildings | 283 individuals | Energy efficiency retrofits in homes can improve occupant satisfaction with daily noise nuisance, upper respiratory symptoms, and reduce absence from school or from work due to respiratory infections. |
| Wargocki et al. [43] | 2000 | Denmark | different ventilation rates | Intervention | Office building | Sick building syndrome (SBS) symptoms, work productivity | 1 office building | 30 female employees | Improved mechanical ventilation rate in office building improve SBS symptoms, work productivity, and perceived indoor air quality. |
| Engvall et al. [82] | 2005 | Sweden | different ventilation rates | Intervention | Residential buildings | General health | 1 building | 44 adults | Energy saving by reducing ventilation flow to below 0.5 ACH could impair perceived air quality but did not influence SBS. |
| Francisco et al. [83] | 2017 | United States | Weatherization services | Intervention | Residential buildings | General health | 72 households | 178 children and adults | Energy efficiency retrofits can improve self-reported health. |
| Umishio et al. [84] | 2020 | Japan | installation of outer walls, floor and/or roof insulation and replacement of windows | Intervention | Residential buildings | Blood pressure | 1009 households | 1685 adults | Energy efficiency insulation retrofitting in homes can reduce home blood pressure and reduce morning home systolic blood pressure of hypertensive patients. |
References
- Norbäck, D. An update on sick building syndrome. Curr. Opin. Allergy Clin. Immunol. 2009, 9, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Melikov, A.K. Advanced air distribution: Improving health and comfort while reducing energy use. Indoor Air 2016, 26, 112–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, K.R.; Frumkin, H.; Balakrishnan, K.; Butler, C.D.; Chafe, Z.A.; Fairlie, I.; Kinney, P.; Kjellstrom, T.; Mauzerall, D.L.; McKone, T.E.; et al. Energy and human health. Annu. Rev. Public Health 2013, 34, 159–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brennan, M.; O’Shea, P.M.; Mulkerrin, E.C. Preventative strategies and interventions to improve outcomes during heatwaves. Age Ageing 2020, 49, 729–732. [Google Scholar] [CrossRef]
- Willand, N.; Ridley, I.; Maller, C. Towards explaining the health impacts of residential energy efficiency interventions—A realist review. Part 1: Pathways. Soc. Sci. Med. 2015, 133, 191–201. [Google Scholar] [CrossRef]
- Barrett, B.; Charles, J.W.; Temte, J.L. Climate change, human health, and epidemiological transition. Prev. Med. 2015, 70, 69–75. [Google Scholar] [CrossRef] [Green Version]
- Wilkinson, P.; Smith, K.R.; Beevers, S.; Tonne, C.; Oreszczyn, T. Energy, energy efficiency, and the built environment. Lancet 2007, 370, 1175–1187. [Google Scholar] [CrossRef]
- Peat, J.K.; Dickerson, J.; Li, J. Effects of damp and mould in the home on respiratory health: A review of the literature. Allergy 1998, 53, 120–128. [Google Scholar] [CrossRef]
- Kolokotsa, D.; Santamouris, M. Review of the indoor environmental quality and energy consumption studies for low income households in Europe. Sci. Total Environ. 2015, 536, 316–330. [Google Scholar] [CrossRef]
- Carmichael, L.; Prestwood, E.; Marsh, R.; Ige, J.; Williams, B.; Pilkington, P.; Eaton, E.; Michalec, A. Healthy buildings for a healthy city: Is the public health evidence base informing current building policies? Sci. Total Environ. 2020, 719, 137146. [Google Scholar] [CrossRef]
- Houghton, A.; Castillo-Salgado, C. Associations between Green Building Design Strategies and Community Health Resilience to Extreme Heat Events: A Systematic Review of the Evidence. Int. J. Environ. Res. Public Health 2019, 16, 663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, J.G.; MacNaughton, P.; Laurent, J.G.; Flanigan, S.S.; Eitland, E.S.; Spengler, J.D. Green Buildings and Health. Curr. Environ. Health Rep. 2015, 2, 250–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cedeno-Laurent, J.G.; Williams, A.; MacNaughton, P.; Cao, X.; Eitland, E.; Spengler, J.; Allen, J. Building Evidence for Health: Green Buildings, Current Science, and Future Challenges. Annu. Rev. Public Health 2018, 39, 291–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liddell, C.; Morris, C. Fuel poverty and human health: A review of recent evidence. Energy Policy 2010, 38, 2987–2997. [Google Scholar] [CrossRef]
- Howieson, S.G.; Hogan, M. Multiple deprivation and excess winter deaths in Scotland. J. R. Soc. Promot. Health 2005, 125, 18–22. [Google Scholar] [CrossRef]
- Anderson, M.; Carmichael, C.; Murray, V.; Dengel, A.; Swainson, M. Defining indoor heat thresholds for health in the UK. Perspect. Public Health 2013, 133, 158–164. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Verriele, M.; Schoemaecker, C.; Hanoune, B.; Leclerc, N.; Germain, S.; Gaudion, V.; Locoge, N. The MERMAID study: Indoor and outdoor average pollutant concentrations in 10 low-energy school buildings in France. Indoor Air 2016, 26, 702–713. [Google Scholar] [CrossRef]
- Collignan, B.; Le Ponner, E.; Mandin, C. Relationships between indoor radon concentrations, thermal retrofit and dwelling characteristics. J. Environ. Radioact. 2016, 165, 124–130. [Google Scholar] [CrossRef]
- Symonds, P.; Rees, D.; Daraktchieva, Z.; McColl, N.; Bradley, J.; Hamilton, I.; Davies, M. Home energy efficiency and radon: An observational study. Indoor Air 2019, 29, 854–864. [Google Scholar] [CrossRef]
- Meyer, W. Impact of constructional energy-saving measures on radon levels indoors. Indoor Air 2019, 29, 680–685. [Google Scholar] [CrossRef] [PubMed]
- Pressyanov, D.; Dimitrov, D.; Dimitrova, I. Energy-efficient reconstructions and indoor radon: The impact assessed by CDs/DVDs. J. Environ. Radioact. 2015, 143, 76–79. [Google Scholar] [CrossRef] [PubMed]
- Vasilyev, A.; Yarmoshenko, I. Effect of energy-efficient measures in building construction on indoor radon in Russia. Radiat. Prot. Dosim. 2017, 174, 419–422. [Google Scholar] [CrossRef]
- Yarmoshenko, I.V.; Vasilyev, A.V.; Onishchenko, A.D.; Kiselev, S.M.; Zhukovsky, M.V. Indoor radon problem in energy efficient multi-storey buildings. Radiat. Prot. Dosim. 2014, 160, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Vasilyev, A.V.; Yarmoshenko, I.V.; Zhukovsky, M.V. Low air exchange rate causes high indoor radon concentration in energy-efficient buildings. Radiat. Prot. Dosim. 2015, 164, 601–605. [Google Scholar] [CrossRef]
- Burghele, B.D.; Botoș, M.; Beldean-Galea, S.; Cucoș, A.; Catalina, T.; Dicu, T.; Dobrei, G.; Florică, Ș.; Istrate, A.; Lupulescu, A.; et al. Comprehensive survey on radon mitigation and indoor air quality in energy efficient buildings from Romania. Sci. Total Environ. 2020, 751, 141858. [Google Scholar] [CrossRef]
- Pigg, S.; Cautley, D.; Francisco, P.W. Impacts of weatherization on indoor air quality: A field study of 514 homes. Indoor Air 2018, 28, 307–317. [Google Scholar] [CrossRef]
- Wallner, P.; Munoz, U.; Tappler, P.; Wanka, A.; Kundi, M.; Shelton, J.F.; Hutter, H.P. Indoor Environmental Quality in Mechanically Ventilated, Energy-Efficient Buildings vs. Conventional Buildings. Int. J. Environ. Res. Public Health 2015, 12, 14132–14147. [Google Scholar] [CrossRef]
- Du, L.; Leivo, V.; Prasauskas, T.; Taubel, M.; Martuzevicius, D.; Haverinen-Shaughnessy, U. Effects of energy retrofits on Indoor Air Quality in multifamily buildings. Indoor Air 2019, 29, 686–697. [Google Scholar] [CrossRef]
- Hirsch, T.; Hering, M.; Burkner, K.; Hirsch, D.; Leupold, W.; Kerkmann, M.L.; Kuhlisch, E.; Jatzwauk, L. House-dust-mite allergen concentrations (Der f 1) and mold spores in apartment bedrooms before and after installation of insulated windows and central heating systems. Allergy 2000, 55, 79–83. [Google Scholar] [CrossRef]
- Sharpe, R.A.; Thornton, C.R.; Nikolaou, V.; Osborne, N.J. Fuel poverty increases risk of mould contamination, regardless of adult risk perception & ventilation in social housing properties. Environ. Int. 2015, 79, 115–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharpe, R.A.; Cocq, K.L.; Nikolaou, V.; Osborne, N.J.; Thornton, C.R. Identifying risk factors for exposure to culturable allergenic moulds in energy efficient homes by using highly specific monoclonal antibodies. Environ. Res. 2016, 144, 32–42. [Google Scholar] [CrossRef] [Green Version]
- Spertini, F.; Berney, M.; Foradini, F.; Roulet, C.A. Major mite allergen Der f 1 concentration is reduced in buildings with improved energy performance. Allergy 2010, 65, 623–629. [Google Scholar] [CrossRef]
- Niculita-Hirzel, H.; Yang, S.; Hager Jörin, C.; Perret, V.; Licina, D.; Goyette Pernot, J. Fungal Contaminants in Energy Efficient Dwellings: Impact of Ventilation Type and Level of Urbanization. Int. J. Environ. Res. Public Health 2020, 17, 4936. [Google Scholar] [CrossRef]
- Coombs, K.; Taft, D.; Ward, D.V.; Green, B.J.; Chew, G.L.; Shamsaei, B.; Meller, J.; Indugula, R.; Reponen, T. Variability of indoor fungal microbiome of green and non-green low-income homes in Cincinnati, Ohio. Sci. Total Environ. 2018, 610–611, 212–218. [Google Scholar] [CrossRef]
- Derbez, M.; Wyart, G.; Le Ponner, E.; Ramalho, O.; Ribéron, J.; Mandin, C. Indoor air quality in energy-efficient dwellings: Levels and sources of pollutants. Indoor Air 2018, 28, 318–338. [Google Scholar] [CrossRef] [PubMed]
- Leivo, V.; Prasauskas, T.; Du, L.; Turunen, M.; Kiviste, M.; Aaltonen, A.; Martuzevicius, D.; Haverinen-Shaughnessy, U. Indoor thermal environment, air exchange rates, and carbon dioxide concentrations before and after energy retro fits in Finnish and Lithuanian multi-family buildings. Sci. Total Environ. 2018, 621, 398–406. [Google Scholar] [CrossRef]
- Coombs, K.C.; Chew, G.L.; Schaffer, C.; Ryan, P.H.; Brokamp, C.; Grinshpun, S.A.; Adamkiewicz, G.; Chillrud, S.; Hedman, C.; Colton, M.; et al. Indoor air quality in green-renovated vs. non-green low-income homes of children living in a temperate region of US (Ohio). Sci. Total Environ. 2016, 554–555, 178–185. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.; Perret, V.; Hager Jörin, C.; Niculita-Hirzel, H.; Goyette Pernot, J.; Licina, D. Volatile organic compounds in 169 energy-efficient dwellings in Switzerland. Indoor Air 2020, 30, 481–491. [Google Scholar] [CrossRef] [Green Version]
- Baumgartner, J.; Clark, S.; Carter, E.; Lai, A.; Zhang, Y.; Shan, M.; Schauer, J.J.; Yang, X. Effectiveness of a Household Energy Package in Improving Indoor Air Quality and Reducing Personal Exposures in Rural China. Environ. Sci. Technol. 2019, 53, 9306–9316. [Google Scholar] [CrossRef]
- Singh, A.; Syal, M.; Grady, S.C.; Korkmaz, S. Effects of green buildings on employee health and productivity. Am. J. Public Health 2010, 100, 1665–1668. [Google Scholar] [CrossRef] [PubMed]
- Gawande, S.; Tiwari, R.R.; Narayanan, P.; Bhadri, A. Indoor Air Quality and Sick Building Syndrome: Are Green Buildings Better than Conventional Buildings? Indian J. Occup. Environ. Med. 2020, 24, 30–32. [Google Scholar] [CrossRef]
- Wargocki, P.; Wyon, D.P.; Sundell, J.; Clausen, G.; Fanger, P.O. The effects of outdoor air supply rate in an office on perceived air quality, sick building syndrome (SBS) symptoms and productivity. Indoor Air 2000, 10, 222–236. [Google Scholar] [CrossRef] [PubMed]
- Hedge, A.; Dorsey, J.A. Green buildings need good ergonomics. Ergonomics 2013, 56, 492–506. [Google Scholar] [CrossRef] [PubMed]
- Hedge, A.; Miller, L.; Dorsey, J.A. Occupant comfort and health in green and conventional university buildings. Work 2014, 49, 363–372. [Google Scholar] [CrossRef]
- Bakke, J.V.; Norback, D.; Wieslander, G.; Hollund, B.E.; Florvaag, E.; Haugen, E.N.; Moen, B.E. Symptoms, complaints, ocular and nasal physiological signs in university staff in relation to indoor environment—temperature and gender interactions. Indoor Air 2008, 18, 131–143. [Google Scholar] [CrossRef] [PubMed]
- Garland, E.; Steenburgh, E.T.; Sanchez, S.H.; Geevarughese, A.; Bluestone, L.; Rothenberg, L.; Rialdi, A.; Foley, M. Impact of LEED-certified affordable housing on asthma in the South Bronx. Prog. Community Health Partnersh. Res. Educ. Act. 2013, 7, 29–37. [Google Scholar] [CrossRef]
- Breysse, J.; Jacobs, D.E.; Weber, W.; Dixon, S.; Kawecki, C.; Aceti, S.; Lopez, J. Health outcomes and green renovation of affordable housing. Public Health Rep. 2011, 126 (Suppl. 1), 64–75. [Google Scholar] [CrossRef] [Green Version]
- Breysse, J.; Dixon, S.L.; Jacobs, D.E.; Lopez, J.; Weber, W. Self-reported health outcomes associated with green-renovated public housing among primarily elderly residents. J. Public Health Manag. Pract. 2015, 21, 355–367. [Google Scholar] [CrossRef] [Green Version]
- Rudge, J.; Gilchrist, R. Excess winter morbidity among older people at risk of cold homes: A population-based study in a London borough. J. Public Health 2005, 27, 353–358. [Google Scholar] [CrossRef] [Green Version]
- Webb, E.; Blane, D.; de Vries, R. Housing and respiratory health at older ages. J. Epidemiol. Community Health 2013, 67, 280–285. [Google Scholar] [CrossRef]
- Sharpe, R.A.; Thornton, C.R.; Nikolaou, V.; Osborne, N.J. Higher energy efficient homes are associated with increased risk of doctor diagnosed asthma in a UK subpopulation. Environ. Int. 2015, 75, 234–244. [Google Scholar] [CrossRef]
- Poortinga, W.; Jones, N.; Lannon, S.; Jenkins, H. Social and health outcomes following upgrades to a national housing standard: A multilevel analysis of a five-wave repeated cross-sectional survey. BMC Public Health 2017, 17, 927. [Google Scholar] [CrossRef] [Green Version]
- Carlton, E.J.; Barton, K.; Shrestha, P.M.; Humphrey, J.; Newman, L.S.; Adgate, J.L.; Root, E.; Miller, S. Relationships between home ventilation rates and respiratory health in the Colorado Home Energy Efficiency and Respiratory Health (CHEER) study. Environ. Res. 2019, 169, 297–307. [Google Scholar] [CrossRef]
- Howden-Chapman, P.; Crane, J.; Chapman, R.; Fougere, G. Improving health and energy efficiency through community-based housing interventions. Int. J. Public Health 2011, 56, 583–588. [Google Scholar] [CrossRef]
- Howden-Chapman, P.; Matheson, A.; Crane, J.; Viggers, H.; Cunningham, M.; Blakely, T.; Cunningham, C.; Woodward, A.; Saville-Smith, K.; O’Dea, D.; et al. Effect of insulating existing houses on health inequality: Cluster randomised study in the community. BMJ 2007, 334, 460. [Google Scholar] [CrossRef] [Green Version]
- Thomson, H.; Snell, C.; Bouzarovski, S. Health, Well-Being and Energy Poverty in Europe: A Comparative Study of 32 European Countries. Int. J. Environ. Res. Public Health 2017, 14, 584. [Google Scholar] [CrossRef] [Green Version]
- Ahrentzen, S.; Erickson, J.; Fonseca, E. Thermal and health outcomes of energy efficiency retrofits of homes of older adults. Indoor Air 2016, 26, 582–593. [Google Scholar] [CrossRef]
- Shortt, N.; Rugkåsa, J. “The walls were so damp and cold” fuel poverty and ill health in Northern Ireland: Results from a housing intervention. Health Place 2007, 13, 99–110. [Google Scholar] [CrossRef]
- Chapman, R.; Howden-Chapman, P.; Viggers, H.; O’Dea, D.; Kennedy, M. Retrofitting houses with insulation: A cost-benefit analysis of a randomised community trial. J. Epidemiol. Community Health 2009, 63, 271–277. [Google Scholar] [CrossRef]
- Grey, C.N.; Jiang, S.; Nascimento, C.; Rodgers, S.E.; Johnson, R.; Lyons, R.A.; Poortinga, W. The short-term health and psychosocial impacts of domestic energy efficiency investments in low-income areas: A controlled before and after study. BMC Public Health 2017, 17, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poortinga, W.; Rodgers, S.E.; Lyons, R.A.; Anderson, P.; Tweed, C.; Grey, C.; Jiang, S.; Johnson, R.; Watkins, A.; Winfield, T.G. Public Health Research. In The Health Impacts of Energy Performance Investments in Low-Income Areas: A Mixed-Methods Approach; Public Health Research; NIHR Journals Library: Southampton, UK, 2018. [Google Scholar]
- Pollard, A.; Jones, T.; Sherratt, S.; Sharpe, R.A. Use of Simple Telemetry to Reduce the Health Impacts of Fuel Poverty and Living in Cold Homes. Int. J. Environ. Res. Public Health 2019, 16, 2853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angelini, V.; Daly, M.; Moro, M.; Navarro Paniagua, M.; Sidman, E.; Walker, I.; Weldon, M. Public Health Research. In The Effect of the Winter Fuel Payment on Household Temperature and Health: A Regression Discontinuity Design Study; Public Health Research; NIHR Journals Library: Southampton, UK, 2019. [Google Scholar]
- Sartini, C.; Tammes, P.; Hay, A.D.; Preston, I.; Lasserson, D.; Whincup, P.H.; Wannamethee, S.G.; Morris, R.W. Can we identify older people most vulnerable to living in cold homes during winter? Ann. Epidemiol. 2018, 28, 1–7.e3. [Google Scholar] [CrossRef] [PubMed]
- Peralta, A.; Camprubi, L.; Rodriguez-Sanz, M.; Basagana, X.; Borrell, C.; Mari-Dell’Olmo, M. Impact of energy efficiency interventions in public housing buildings on cold-related mortality: A case-crossover analysis. Int. J. Epidemiol. 2017, 46, 1192–1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Umishio, W.; Ikaga, T.; Kario, K.; Fujino, Y.; Hoshi, T.; Ando, S.; Suzuki, M.; Yoshimura, T.; Yoshino, H.; Murakami, S. Cross-Sectional Analysis of the Relationship Between Home Blood Pressure and Indoor Temperature in Winter: A Nationwide Smart Wellness Housing Survey in Japan. Hypertension 2019, 74, 756–766. [Google Scholar] [CrossRef]
- López-Bueno, J.A.; Linares, C.; Sánchez-Guevara, C.; Martinez, G.S.; Mirón, I.J.; Núñez-Peiró, M.; Valero, I.; Díaz, J. The effect of cold waves on daily mortality in districts in Madrid considering sociodemographic variables. Sci. Total Environ. 2020, 749, 142364. [Google Scholar] [CrossRef]
- Engvall, K.; Norrby, C.; Norback, D. Ocular, nasal, dermal and respiratory symptoms in relation to heating, ventilation, energy conservation, and reconstruction of older multi-family houses. Indoor Air 2003, 13, 206–211. [Google Scholar] [CrossRef]
- Smedje, G.; Wang, J.; Norback, D.; Nilsson, H.; Engvall, K. SBS symptoms in relation to dampness and ventilation in inspected single-family houses in Sweden. Int. Arch. Occup. Environ. Health 2017, 90, 703–711. [Google Scholar] [CrossRef] [Green Version]
- Norback, D.; Lampa, E.; Engvall, K. Asthma, allergy and eczema among adults in multifamily houses in Stockholm (3-HE study)--associations with building characteristics, home environment and energy use for heating. PLoS ONE 2014, 9, e112960. [Google Scholar] [CrossRef]
- Wang, J.; Engvall, K.; Smedje, G.; Nilsson, H.; Norback, D. Current wheeze, asthma, respiratory infections, and rhinitis among adults in relation to inspection data and indoor measurements in single-family houses in Sweden-The BETSI study. Indoor Air 2017, 27, 725–736. [Google Scholar] [CrossRef]
- Sharpe, R.A.; Machray, K.E.; Fleming, L.E.; Taylor, T.; Henley, W.; Chenore, T.; Hutchcroft, I.; Taylor, J.; Heaviside, C.; Wheeler, B.W. Household energy efficiency and health: Area-level analysis of hospital admissions in England. Environ. Int. 2019, 133, 105164. [Google Scholar] [CrossRef]
- Sobottka, A.; Thriene, B. Sanitation programmes for living spaces and health risks involved. Toxicol. Lett. 1996, 88, 365–368. [Google Scholar] [CrossRef]
- Kennard, H.R.; Huebner, G.M.; Shipworth, D.; Oreszczyn, T. The associations between thermal variety and health: Implications for space heating energy use. PLoS ONE 2020, 15, e0236116. [Google Scholar] [CrossRef] [PubMed]
- Wallner, P.; Tappler, P.; Munoz, U.; Damberger, B.; Wanka, A.; Kundi, M.; Hutter, H.P. Health and Wellbeing of Occupants in Highly Energy Efficient Buildings: A Field Study. Int. J. Environ. Res. Public Health 2017, 14, 314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Somerville, M.; Mackenzie, I.; Owen, P.; Miles, D. Housing and health: Does installing heating in their homes improve the health of children with asthma? Public Health 2000, 114, 434–439. [Google Scholar] [CrossRef]
- Barton, A.; Basham, M.; Foy, C.; Buckingham, K.; Somerville, M.; Torbay Healthy Housing, G. The Watcombe Housing Study: The short term effect of improving housing conditions on the health of residents. J. Epidemiol. Community Health 2007, 61, 771–777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osman, L.M.; Ayres, J.G.; Garden, C.; Reglitz, K.; Lyon, J.; Douglas, J.G. A randomised trial of home energy efficiency improvement in the homes of elderly COPD patients. Eur. Respir. J. 2010, 35, 303–309. [Google Scholar] [CrossRef] [Green Version]
- Wilson, J.; Dixon, S.L.; Jacobs, D.E.; Breysse, J.; Akoto, J.; Tohn, E.; Isaacson, M.; Evens, A.; Hernandez, Y. Watts-to-Wellbeing: Does residential energy conservation improve health? Energy Effic. 2013, 7, 151–160. [Google Scholar] [CrossRef]
- Haverinen-Shaughnessy, U.; Pekkonen, M.; Leivo, V.; Prasauskas, T.; Turunen, M.; Kiviste, M.; Aaltonen, A.; Martuzevicius, D. Occupant satisfaction with indoor environmental quality and health after energy retrofits of multi-family buildings: Results from INSULAtE-project. Int. J. Hyg. Environ. Health 2018, 221, 921–928. [Google Scholar] [CrossRef]
- Engvall, K.; Wickman, P.; Norback, D. Sick building syndrome and perceived indoor environment in relation to energy saving by reduced ventilation flow during heating season: A 1 year intervention study in dwellings. Indoor Air 2005, 15, 120–126. [Google Scholar] [CrossRef]
- Francisco, P.W.; Jacobs, D.E.; Targos, L.; Dixon, S.L.; Breysse, J.; Rose, W.; Cali, S. Ventilation, indoor air quality, and health in homes undergoing weatherization. Indoor Air 2017, 27, 463–477. [Google Scholar] [CrossRef] [PubMed]
- Umishio, W.; Ikaga, T.; Kario, K.; Fujino, Y.; Hoshi, T.; Ando, S.; Suzuki, M.; Yoshimura, T.; Yoshino, H.; Murakami, S. Intervention study of the effect of insulation retrofitting on home blood pressure in winter: A nationwide Smart Wellness Housing survey. J. Hypertens. 2020, 38, 2510–2518. [Google Scholar] [CrossRef] [PubMed]
- Humphrey, J.L.; Barton, K.E.; Man Shrestha, P.; Carlton, E.J.; Newman, L.S.; Dowling Root, E.; Adgate, J.L.; Miller, S.L. Air infiltration in low-income, urban homes and its relationship to lung function. J. Expo. Sci. Environ. Epidemiol. 2020, 30, 262–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, E.S.; Egger, S.; Hughes, S.; Weber, M.; Steinberg, J.; Rahman, B.; Worth, H.; Ruano-Ravina, A.; Rawstorne, P.; Yu, X.Q. Systematic review and meta-analysis of residential radon and lung cancer in never-smokers. Eur. Respir. Rev. 2021, 30, 200230. [Google Scholar] [CrossRef]
- Ilomets, S.; Kalamees, T. Evaluation of the criticality of thermal bridges. J. Build. Pathol. Rehabil. 2016, 1, 11. [Google Scholar] [CrossRef]
- Bolden, A.L.; Kwiatkowski, C.F.; Colborn, T. New Look at BTEX: Are Ambient Levels a Problem? Environ. Sci. Technol. 2015, 49, 5261–5276. [Google Scholar] [CrossRef]
| No. | References | Country | Pollutant Groups | Improved Ventilation | Thermal Retrofit | Draught Proofing | Green Retrofits | Fuel Poverty | Energy Carrier |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Collignan et al. 2016 [19] | France | Radon | ||||||
| 2 | Symonds et al. 2019 [20] | United Kingdom | Radon | ↑ | |||||
| 3 | Meyer et al. 2019 [21] | Germany | Radon | ↑ | ↑ | ||||
| 4 | Pressyanov et al. 2015 [22] | Bulgaria | Radon | ↑ | ↑ | ||||
| 5 | Vasilyev et al. 2017 [23] | Russia | Radon | ↑ | |||||
| 6 | Yarmoshenko et al. 2014 [24] | Russia | Radon | ↑ | |||||
| 7 | Vasilyev et al. 2015 [25] | Russia | Radon | ↑ | |||||
| 8 | Burghele et al. 2020 [26] | Romania | Radon | ↓ | |||||
| 9 | Pigg et al. 2018 [27] | United States | Radon 1, Chemicals 3 | ↓ | ↑1, ↓3 | ↑1, ↓3 | |||
| 10 | Wallner et al. 2015 [28] | Austria | Radon 1, Biological agents 2, Chemicals 3 | ↓1, ↓2, ↓3 | |||||
| 11 | Du et al. 2019 [29] | Finland Lithuania | Radon 1, Biological agents 2, Chemicals3 | ↓2, ↑↓3 | ↑1 | ||||
| 12 | Hirsch et al. 2020 [30] | Germany | biological agents | ↑ | |||||
| 13 | Sharpe et al. 2015 [31] | United Kingdom | biological agents | ↑ | |||||
| 14 | Sharpe et al. 2016 [32] | United Kingdom | biological agents | ↓ | |||||
| 15 | Spertini et al. 2010 [33] | Switzerland | biological agents | ↓ | |||||
| 16 | Niculita-Hirzel et al. 2000 [34] | Switzerland | biological agents | ↓ | |||||
| 17 | Coombs et al. 2018 [35] | United States | biological agents | 0 | |||||
| 18 | Derbez et al. 2018 [36] | France | Chemicals | ↑ | |||||
| 19 | Leivo et al. 2018 [37] | Finland Lithuania | Chemicals | ↓ | ↑ | ||||
| 20 | Coombs et al. 2016 [38] | United States | Chemicals | ↑↓ | |||||
| 21 | Yang et al. 2020 [39] | Switzerland | Chemicals | ↑ | |||||
| 22 | Verriele et al. 2016 [18] | France | Chemicals | ↓ | |||||
| 23 | Baumgartner et al. 2019 [40] | China | Chemicals | ↑↓ |
| No. | Reference | Thematic Group | Respiratory Health | General Health | Mental Health | Performance | Satisfaction | Cold-Related Mortality | SBS Symptoms | |
|---|---|---|---|---|---|---|---|---|---|---|
| Asthma | Other Respiratory Illnesses | |||||||||
| 1 | Garland et al. 2013 [47] | Green Buildings | + | |||||||
| 2 | Singh et al. 2010 [41] | Green Buildings | + | + | + | + | ||||
| 3 | Breysse et al. 2011 [48] | Green Buildings | + | + | + | |||||
| 4 | Breysse et al. 2015 [49] | Green Buildings | + | + | ||||||
| 5 | Hedge et al. 2013 [44] | Green Buildings | + | + | + | |||||
| 6 | Hedge et al. 2014 [45] | Green Buildings | + | + | + | |||||
| 7 | Gawande et al. 2020 [42] | Green Buildings | 0 | |||||||
| 8 | Rudge et al. 2005 [50] | Fuel Poverty | # | |||||||
| 9 | Webb et al. 2013 [51] | Fuel Poverty | # | |||||||
| 10 | Sharpe et al. 2015 [52] | Fuel Poverty | # | |||||||
| 11 | Poortinga et al. 2017 [53] | Fuel Poverty | + | +/− | + | +/− | ||||
| 12 | Carlton et al. 2019 [54] | Fuel Poverty | − | − | ||||||
| 13 | Howden-Chapman et al. 2011 [55] | Fuel Poverty | + | + | + | |||||
| 14 | Howden-Chapman et al. 2007 [56] | Fuel Poverty | + | + | ||||||
| 15 | Humphrey et al. 2020 [54] | Fuel Poverty | + | |||||||
| 16 | Thomson et al. 2017 [57] | Fuel Poverty | # | # | ||||||
| 17 | Ahrentzen et al. 2016 [58] | Fuel Poverty | + | + | ||||||
| 18 | Shortt et al. 2007 [59] | Fuel Poverty | + | + | ||||||
| 19 | Chapman et al. 2009 [60] | Fuel Poverty | + | |||||||
| 20 | Grey et al. 2017 [61] | Fuel Poverty | + | + | ||||||
| 21 | Poortinga et al. 2018 [62] | Fuel Poverty | + | + | ||||||
| 22 | Pollard et al. 2019 [63] | Fuel Poverty | # | |||||||
| 23 | Angelini et al. 2019 [64] | Fuel Poverty | # | |||||||
| 24 | Sartini et al. 2018 [65] | Fuel Poverty | + | |||||||
| 25 | Peralta et al. 2017 [66] | Fuel Poverty | +/− | |||||||
| 26 | Umishio et al. 2019 [67] | Fuel Poverty | # | |||||||
| 27 | López-Bueno et al. 2020 [68] | Fuel Poverty | + | |||||||
| 28 | Engvall et al. 2003 [69] | Cross sectional | − | |||||||
| 29 | Smedje et al. 2017 [70] | Cross sectional | + | |||||||
| 30 | Norback et al. 2014 [71] | Cross sectional | +/− | |||||||
| 31 | Wang et al. 2017 [72] | Cross sectional | + | |||||||
| 32 | Sharpe et al. 2019 [73] | Cross sectional | + | |||||||
| 33 | Sobottka et al. 1996 [74] | Cross sectional | − | |||||||
| 34 | Bakke et al. 2008 [46] | Cross sectional | # | |||||||
| 35 | Kennard et al. 2020 [75] | Cross sectional | # | |||||||
| 36 | Wallner et al. 2017 [76] | Longitudinal | + | |||||||
| 37 | Somerville et al. 2000 [77] | Intervention | + | + | ||||||
| 38 | Barton et al. 2007 [78] | Intervention | + | + | ||||||
| 39 | Osman et al. 2010 [79] | Intervention | + | |||||||
| 40 | Wilson et al. 2013 [80] | Intervention | + | + | + | |||||
| 41 | Haverinen-Shaughnessy et al. 2018 [81] | Intervention | + | + | ||||||
| 42 | Wargocki et al. 2000 [43] | Intervention | + | + | ||||||
| 43 | Engvall et al. 2005 [82] | Intervention | 0 | |||||||
| 44 | Francisco et al. 2017 [83] | Intervention | + | |||||||
| 45 | Umishio et al. 2020 [84] | Intervention | + | |||||||
| No. | References | Energy Efficiency Improvements (at Least Two Measures) | Green Buildings | More Effective Heating | Thermal Insulation | Draught Proofing | Higher Ventilation Rate | Installation of Mechanical Ventilation |
|---|---|---|---|---|---|---|---|---|
| 1 | Garland et al. 2013 [47] | + | ||||||
| 2 | Singh et al. 2010 [41] | + | ||||||
| 3 | Breysse et al. 2011 [48] | + | ||||||
| 4 | Breysse et al. 2015 [49] | + | ||||||
| 5 | Hedge et al. 2013 [44] | + | ||||||
| 6 | Hedge et al. 2014 [45] | + | ||||||
| 7 | Gawande et al. 2020 [42] | + | ||||||
| 8 | Poortinga et al. 2017 [61] | + | − | |||||
| 9 | Carlton et al. 2019 [54] | − | ||||||
| 10 | Howden-Chapman et al. 2011 [55] | + | + | |||||
| 11 | Howden-Chapman et al. 2007 [56] | + | ||||||
| 12 | Humphrey et al. 2020 [85] | + | ||||||
| 13 | Ahrentzen et al. 2016 [58] | + | ||||||
| 14 | Shortt et al. 2007 [59] | + | + | |||||
| 15 | Chapman et al. 2009 [60] | + | ||||||
| 16 | Grey et al. 2017 [61] | + | ||||||
| 17 | Poortinga et al. 2018 [62] | + | ||||||
| 18 | Sartini et al. 2018 [65] | + | ||||||
| 19 | Peralta et al. 2017 [66] | +/− | ||||||
| 20 | López-Bueno et al. 2020 [68] | + | ||||||
| 21 | Engvall et al. 2003 [69] | + | − | + | ||||
| 22 | Smedje et al. 2017 [70] | + | ||||||
| 23 | Norback et al. 2014 [71] | + | ||||||
| 24 | Wang et al. 2017 [72] | + | ||||||
| 25 | Sharpe et al. 2019 [63] | − | ||||||
| 26 | Sobottka et al. 1996 [74] | − | ||||||
| 27 | Wallner et al. 2017 [76] | + | ||||||
| 28 | Somerville et al. 2000 [77] | + | ||||||
| 29 | Barton et al. 2007 [78] | + | ||||||
| 30 | Osman et al. 2010 [79] | + | ||||||
| 31 | Wilson et al. 2013 [80] | + | ||||||
| 32 | Haverinen-Shaughnessy et al. 2018 [81] | + | ||||||
| 33 | Wargocki et al. 2000 [43] | + | ||||||
| 34 | Engvall et al. 2005 [82] | + | ||||||
| 35 | Francisco et al. 2017 [83] | + | ||||||
| 36 | Umishio et al. 2020 [84] | + | ||||||
| Positive associations (+) | 8 | 7 | 6 | 9 | 4 | 1 | ||
| Negative associations (−) | 1 | 3 | 1 | |||||
| Mixed results (+/−) | 1 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.; Wang, J.; Norbäck, D. A Systematic Review of Associations between Energy Use, Fuel Poverty, Energy Efficiency Improvements and Health. Int. J. Environ. Res. Public Health 2022, 19, 7393. https://doi.org/10.3390/ijerph19127393
Wang C, Wang J, Norbäck D. A Systematic Review of Associations between Energy Use, Fuel Poverty, Energy Efficiency Improvements and Health. International Journal of Environmental Research and Public Health. 2022; 19(12):7393. https://doi.org/10.3390/ijerph19127393
Chicago/Turabian StyleWang, Chengju, Juan Wang, and Dan Norbäck. 2022. "A Systematic Review of Associations between Energy Use, Fuel Poverty, Energy Efficiency Improvements and Health" International Journal of Environmental Research and Public Health 19, no. 12: 7393. https://doi.org/10.3390/ijerph19127393
APA StyleWang, C., Wang, J., & Norbäck, D. (2022). A Systematic Review of Associations between Energy Use, Fuel Poverty, Energy Efficiency Improvements and Health. International Journal of Environmental Research and Public Health, 19(12), 7393. https://doi.org/10.3390/ijerph19127393