
Time-Trends of Drug-Drug Interactions among Elderly Outpatients in the Piedmont Region (Italy): A Population-Based Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Setting
2.3. Evaluation of Drug-Drug Interactions
2.4. Statistical Analysis
3. Results
4. Discussion
Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Onder, G.; Pedone, C.; Landi, F.; Cesari, M.; Della Vedova, C.; Bernabei, R.; Gambassi, G. Adverse Drug Reactions as Cause of Hospital Admissions: Results from the Italian Group of Pharmacoepidemiology in the Elderly (GIFA). J. Am. Geriatr. Soc. 2002, 50, 1962–1968. [Google Scholar] [CrossRef] [PubMed]
- Sultana, J.; Cutroneo, P.; Trifirò, G. Clinical and Economic Burden of Adverse Drug Reactions. J. Pharmacol. Pharm. 2013, 4, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalil, H.; Huang, C. Adverse Drug Reactions in Primary Care: A Scoping Review. BMC Health Serv. Res. 2020, 20, 5. [Google Scholar] [CrossRef] [PubMed]
- Montastruc, J.; Lafaurie, M.; Canecaude, C.; Durrieu, G.; Sommet, A.; Montastruc, F.; Bagheri, H. Fatal Adverse Drug Reactions: A Worldwide Perspective in the World Health Organization Pharmacovigilance Database. Br. J. Clin. Pharmacol. 2021, 87, 4334–4340. [Google Scholar] [CrossRef] [PubMed]
- Violan, C.; Foguet-Boreu, Q.; Flores-Mateo, G.; Salisbury, C.; Blom, J.; Freitag, M.; Glynn, L.; Muth, C.; Valderas, J.M. Prevalence, Determinants and Patterns of Multimorbidity in Primary Care: A Systematic Review of Observational Studies. PLoS ONE 2014, 9, e102149. [Google Scholar] [CrossRef]
- Oscanoa, T.J.; Lizaraso, F.; Carvajal, A. Hospital Admissions Due to Adverse Drug Reactions in the Elderly. A Meta-Analysis. Eur. J. Clin. Pharmacol. 2017, 73, 759–770. [Google Scholar] [CrossRef]
- Insani, W.N.; Whittlesea, C.; Alwafi, H.; Man, K.K.C.; Chapman, S.; Wei, L. Prevalence of Adverse Drug Reactions in the Primary Care Setting: A Systematic Review and Meta-Analysis. PLoS ONE 2021, 16, e0252161. [Google Scholar] [CrossRef]
- Tragni, E.; Casula, M.; Pieri, V.; Favato, G.; Marcobelli, A.; Trotta, M.G.; Catapano, A.L. Prevalence of the Prescription of Potentially Interacting Drugs. PLoS ONE 2013, 8, e78827. [Google Scholar] [CrossRef]
- Mangoni, A.A.; Jackson, S.H.D. Age-Related Changes in Pharmacokinetics and Pharmacodynamics: Basic Principles and Practical Applications: Age-Related Changes in Pharmacokinetics and Pharmacodynamics. Br. J. Clin. Pharmacol. 2003, 57, 6–14. [Google Scholar] [CrossRef] [Green Version]
- OSMED 2020 Osservatorio Nazionale Sull’impiego Dei Medicinali. L’uso Dei Farmaci in Italia. Rapporto Nazionale 2020; Agenzia Italiana Del Farmaco: Roma, Italy, 2021. [Google Scholar]
- Pont, L.; Alhawassi, T.; Bajorek, B.; Krass, I. A Systematic Review of the Prevalence and Risk Factors for Adverse Drug Reactions in the Elderly in the Acute Care Setting. CIA 2014, 9, 2079. [Google Scholar] [CrossRef] [Green Version]
- Mallet, L.; Spinewine, A.; Huang, A. The Challenge of Managing Drug Interactions in Elderly People. Lancet 2007, 370, 185–191. [Google Scholar] [CrossRef]
- Delafuente, J.C. Understanding and Preventing Drug Interactions in Elderly Patients. Crit. Rev. Oncol. Hematol. 2003, 48, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Rogero-Blanco, E.; Del-Cura-González, I.; Aza-Pascual-Salcedo, M.; García de Blas González, F.; Terrón-Rodas, C.; Chimeno-Sánchez, S.; García-Domingo, E.; López-Rodríguez, J.A.; Group MULTIPAP. Drug Interactions Detected by a Computer-Assisted Prescription System in Primary Care Patients in Spain: MULTIPAP Study. Eur. J. Gen. Pract. 2021, 27, 90–96. [Google Scholar] [CrossRef]
- Santos, T.R.A.; Silveira, E.A.; Pereira, L.V.; Provin, M.P.; Lima, D.M.; Amaral, R.G. Potential Drug-Drug Interactions in Older Adults: A Population-Based Study: Potential Drug-Drug Interactions. Geriatr. Gerontol. Int. 2017, 17, 2336–2346. [Google Scholar] [CrossRef] [PubMed]
- Classen, D.C. Computerized Surveillance of Adverse Drug Events in Hospital Patients. JAMA 1991, 266, 2847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franceschi, M.; Scarcelli, C.; Niro, V.; Seripa, D.; Pazienza, A.M.; Pepe, G.; Colusso, A.M.; Pacilli, L.; Pilotto, A. Prevalence, Clinical Features and Avoidability of Adverse Drug Reactions as Cause of Admission to a Geriatric Unit: A Prospective Study of 1756 Patients. Drug Saf. 2008, 31, 545–556. [Google Scholar] [CrossRef]
- Raschi, E.; Piccinni, C.; Signoretta, V.; Lionello, L.; Bonezzi, S.; Delfino, M.; Di Candia, L.; Di Castri, L.; Pieraccini, F.; Carati, D.; et al. Clinically Important Drug-Drug Interactions in Poly-Treated Elderly Outpatients: A Campaign to Improve Appropriateness in General Practice: Clinically Important Drug-Drug Interactions in Poly-Treated Elderly Patients. Br. J. Clin. Pharmacol. 2015, 80, 1411–1420. [Google Scholar] [CrossRef] [Green Version]
- Franchi, C.; Tettamanti, M.; Pasina, L.; Djignefa, C.D.; Fortino, I.; Bortolotti, A.; Merlino, L.; Nobili, A. Changes in Drug Prescribing to Italian Community-Dwelling Elderly People: The EPIFARM–Elderly Project 2000–2010. Eur. J. Clin. Pharmacol. 2014, 70, 437–443. [Google Scholar] [CrossRef]
- Haider, S.I.; Johnell, K.; Thorslund, M.; Fastbom, J. Trends in Polypharmacy and Potential Drug-Drug Interactions across Educational Groups in Elderly Patients in Sweden for the Period 1992–2002. Int. J. Clin. Pharmacol. Ther. 2007, 45, 643–653. [Google Scholar] [CrossRef]
- Guthrie, B.; Makubate, B.; Hernandez-Santiago, V.; Dreischulte, T. The Rising Tide of Polypharmacy and Drug-Drug Interactions: Population Database Analysis 1995–2010. BMC Med. 2015, 13, 74. [Google Scholar] [CrossRef] [Green Version]
- Onder, G.; Bonassi, S.; Abbatecola, A.M.; Folino-Gallo, P.; Lapi, F.; Marchionni, N.; Pani, L.; Pecorelli, S.; Sancarlo, D.; Scuteri, A.; et al. High Prevalence of Poor Quality Drug Prescribing in Older Individuals: A Nationwide Report From the Italian Medicines Agency (AIFA). J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 430–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- FDA Drug Safety Communication. FDA Warns about Increased Risk of Ruptures or Tears in the Aorta Blood Vessel with Fluoroquinolone Antibiotics in Certain Patients. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-warns-about-increased-risk-ruptures-or-tears-aorta-blood-vessel-fluoroquinolone-antibiotics (accessed on 13 April 2022).
- EMA/795349/2018 Disabling and Potentially Permanent Side Effects Lead to Suspension or Restrictions of Quinolone and Fluoroquinolone Antibiotics. Available online: https://www.ema.europa.eu/en/news/disabling-potentially-permanent-side-effects-lead-suspension-restrictions-quinolone-fluoroquinolone (accessed on 13 April 2022).
- Sankar, A.; Swanson, K.M.; Zhou, J.; Jena, A.B.; Ross, J.S.; Shah, N.D.; Karaca-Mandic, P. Association of Fluoroquinolone Prescribing Rates With Black Box Warnings from the US Food and Drug Administration. JAMA Netw. Open 2021, 4, e2136662. [Google Scholar] [CrossRef] [PubMed]
- Fick, D.M.; Semla, T.P.; Steinman, M.; Beizer, J.; Brandt, M.; Dombrowski, R.; DuBeau, C.E.; Pezzullo, L.; Epplin, J.J.; Flanagan, N.; et al. American Geriatrics Society 2019 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults: 2019 AGS Beers Criteria® Update Expert Panel. J. Am. Geriatr Soc. 2019, 67, 674–694. [Google Scholar] [CrossRef]
- OSMED 2019 Osservatorio Nazionale Sull’impiego Dei Medicinali. L’uso Dei Farmaci Nella Popolazione Anziana in Italia. Rapporto Nazionale 2019; Agenzia Italiana Del Farmaco: Roma, Italy, 2021. [Google Scholar]
- Motola, D.; Vaccheri, A.; Silvani, M.C.; Poluzzi, E.; Bottoni, A.; De Ponti, F.; Montanaro, N. Pattern of NSAID Use in the Italian General Population: A Questionnaire-Based Survey. Eur. J. Clin. Pharmacol. 2004, 60, 731–738. [Google Scholar] [CrossRef]
- Conaghan, P.G. A Turbulent Decade for NSAIDs: Update on Current Concepts of Classification, Epidemiology, Comparative Efficacy, and Toxicity. Rheumatol. Int. 2012, 32, 1491–1502. [Google Scholar] [CrossRef] [Green Version]
- Wehling, M. Non-Steroidal Anti-Inflammatory Drug Use in Chronic Pain Conditions with Special Emphasis on the Elderly and Patients with Relevant Comorbidities: Management and Mitigation of Risks and Adverse Effects. Eur. J. Clin. Pharmacol. 2014, 70, 1159–1172. [Google Scholar] [CrossRef]
- Dreischulte, T.; Morales, D.R.; Bell, S.; Guthrie, B. Combined Use of Nonsteroidal Anti-Inflammatory Drugs with Diuretics and/or Renin–Angiotensin System Inhibitors in the Community Increases the Risk of Acute Kidney Injury. Kidney Int. 2015, 88, 396–403. [Google Scholar] [CrossRef]
- Wongrakpanich, S.; Wongrakpanich, A.; Melhado, K.; Rangaswami, J. A Comprehensive Review of Non-Steroidal Anti-Inflammatory Drug Use in The Elderly. Aging Dis. 2018, 9, 143. [Google Scholar] [CrossRef] [Green Version]
- Grodzinsky, A.; Arnold, S.V.; Jacob, D.; Draznin, B.; Kosiborod, M. The Impact of Cardiovascular Drugs on Glycemic Control: A Review. Endocr. Pract. 2017, 23, 363–371. [Google Scholar] [CrossRef] [Green Version]
- Hirst, J.A.; Farmer, A.J.; Feakins, B.G.; Aronson, J.K.; Stevens, R.J. Quantifying the Effects of Diuretics and β-Adrenoceptor Blockers on Glycaemic Control in Diabetes Mellitus—A Systematic Review and Meta-Analysis: Diuretics and β-Blockers on Glycaemic Control in Diabetes. Br. J. Clin. Pharmacol. 2015, 79, 733–743. [Google Scholar] [CrossRef] [Green Version]
- Juurlink, D.N.; Gomes, T.; Ko, D.T.; Szmitko, P.E.; Austin, P.C.; Tu, J.V.; Henry, D.A.; Kopp, A.; Mamdani, M.M. A Population-Based Study of the Drug Interaction between Proton Pump Inhibitors and Clopidogrel. CMAJ 2009, 180, 713–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agewall, S.; Cattaneo, M.; Collet, J.P.; Andreotti, F.; Lip, G.Y.H.; Verheugt, F.W.A.; Huber, K.; Grove, E.L.; Morais, J.; Husted, S.; et al. Expert Position Paper on the Use of Proton Pump Inhibitors in Patients with Cardiovascular Disease and Antithrombotic Therapy. Eur. Heart J. 2013, 34, 1708–1713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasina, L.; Nobili, A.; Tettamanti, M.; Salerno, F.; Corrao, S.; Marengoni, A.; Iorio, A.; Marcucci, M.; Mannucci, P.M. Prevalence and Appropriateness of Drug Prescriptions for Peptic Ulcer and Gastro-Esophageal Reflux Disease in a Cohort of Hospitalized Elderly. Eur. J. Inter. Med. 2011, 22, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Marengoni, A.; Pasina, L.; Concoreggi, C.; Martini, G.; Brognoli, F.; Nobili, A.; Onder, G.; Bettoni, D. Understanding Adverse Drug Reactions in Older Adults through Drug–Drug Interactions. Eur. J. Inter. Med. 2014, 25, 843–846. [Google Scholar] [CrossRef] [PubMed]
- Montano, N.; Costantino, G.; Casazza, G.; Sbrojavacca, R.; Lenti, M.V.; Falsetti, L.; Guzzo, A.; Majo, R.; Perticone, F.; Corazza, G.R. The Italian Society of Internal Medicine Choosing Wisely Campaign. Intern. Emerg. Med. 2016, 11, 1125–1130. [Google Scholar] [CrossRef] [PubMed]
- Stasi, E.; Michielan, A.; Morreale, G.C.; Tozzi, A.; Venezia, L.; Bortoluzzi, F.; Triossi, O.; Soncini, M.; Leandro, G.; Milazzo, G.; et al. Five Common Errors to Avoid in Clinical Practice: The Italian Association of Hospital Gastroenterologists and Endoscopists (AIGO) Choosing Wisely Campaign. Intern. Emerg. Med. 2019, 14, 301–308. [Google Scholar] [CrossRef]
- Savarino, V.; Dulbecco, P.; de Bortoli, N.; Ottonello, A.; Savarino, E. The Appropriate Use of Proton Pump Inhibitors (PPIs): Need for a Reappraisal. Eur. J. Inter. Med. 2017, 37, 19–24. [Google Scholar] [CrossRef]
- Carpenter, M.; Berry, H.; Pelletier, A.L. Clinically Relevant Drug-Drug Interactions in Primary Care. Am. Fam. Physician 2019, 99, 558–564. [Google Scholar]
- Swart, F.; Bianchi, G.; Lenzi, J.; Iommi, M.; Maestri, L.; Raschi, E.; Zoli, M.; Ponti, F.D.; Poluzzi, E. Risk of Hospitalization from Drug-Drug Interactions in the Elderly: Real-World Evidence in a Large Administrative Database. Aging 2020, 12, 19711–19739. [Google Scholar] [CrossRef]
- Salvi, V.; Barone-Adesi, F.; D’Ambrosio, V.; Albert, U.; Maina, G. High H1-Affinity Antidepressants and Risk of Metabolic Syndrome in Bipolar Disorder. Psychopharmacology 2016, 233, 49–56. [Google Scholar] [CrossRef]

{kind=link}
| Year | |||||||
|---|---|---|---|---|---|---|---|
| 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | |
| Subjects, N | 4,924,918 | 4,874,715 | 4,825,135 | 4,771,202 | 4,719,997 | 4,666,102 | 4,612,679 |
| Over 65, N (%) | 1,146,111 (23.27) | 1,160,271 (23.80) | 1,173,887 (24.33) | 1,180,494 (24.74) | 1,190,234 (25.22) | 1,196,981 (25.65) | 1,205,837 (26.14) |
| Polypharmacy, N (%) | 154,584 (13.49) | 162,809 (14.03) | 166,984 (14.22) | 173,534 (14.70) | 177,804 (14.94) | 179,669 (15.01) | 180,750 (14.99) |
| Males, N (%) | 491,701 (42.90) | 499,622 (43.06) | 507,160 (43.2) | 511,591 (43.34) | 517,580 (43.49) | 522,214 (43.63) | 527,763 (43.77) |
| Age, mean (SD) | 76.21 (7.97) | 76.29 (8.04) | 76.4 (8.11) | 76.5 (8.16) | 76.61 (8.22) | 76.7 (8.28) | 76.78 (8.34) |
| Age Class, N (%) | |||||||
| 65–69 years | 279,275 (24.37) | 286,799 (24.72) | 297,187 (25.32) | 291,655 (24.71) | 285,931 (24.02) | 279,039 (23.31) | 277,388 (23.00) |
| 70–74 years | 259,228 (22.62) | 250,269 (21.57) | 238,264 (20.30) | 244,551 (20.72) | 253,199 (21.27) | 263,515 (22.01) | 270,870 (22.46) |
| 75–79 years | 234,410 (20.45) | 241,058 (20.78) | 245,690 (20.93) | 245,772 (20.82) | 242,620 (20.38) | 235,066 (19.64) | 226,956 (18.82) |
| 80–84 years | 184,095 (16.06) | 185,598 (16.00) | 186,361 (15.88) | 186,833 (15.83) | 190,430 (16.00) | 197,028 (16.46) | 203,225 (16.85) |
| ≥85 years | 189,103 (16.50) | 196,547 (16.94) | 206,385 (17.58) | 211,683 (17.93) | 218,054 (18.32) | 222,333 (18.57) | 227,398 (18.86) |
| DDI | 2013 | 2019 | Percent Change (95% CI) |
|---|---|---|---|
| % | % | ||
| Antidiabetics—beta-blocking agents | 21.85 | 24.24 | 10.94 (9.57; 12.33) |
| Antidiabetics—fluoroquinolones | 10.91 | 5.97 | −45.25 (−46.5; −43.97) |
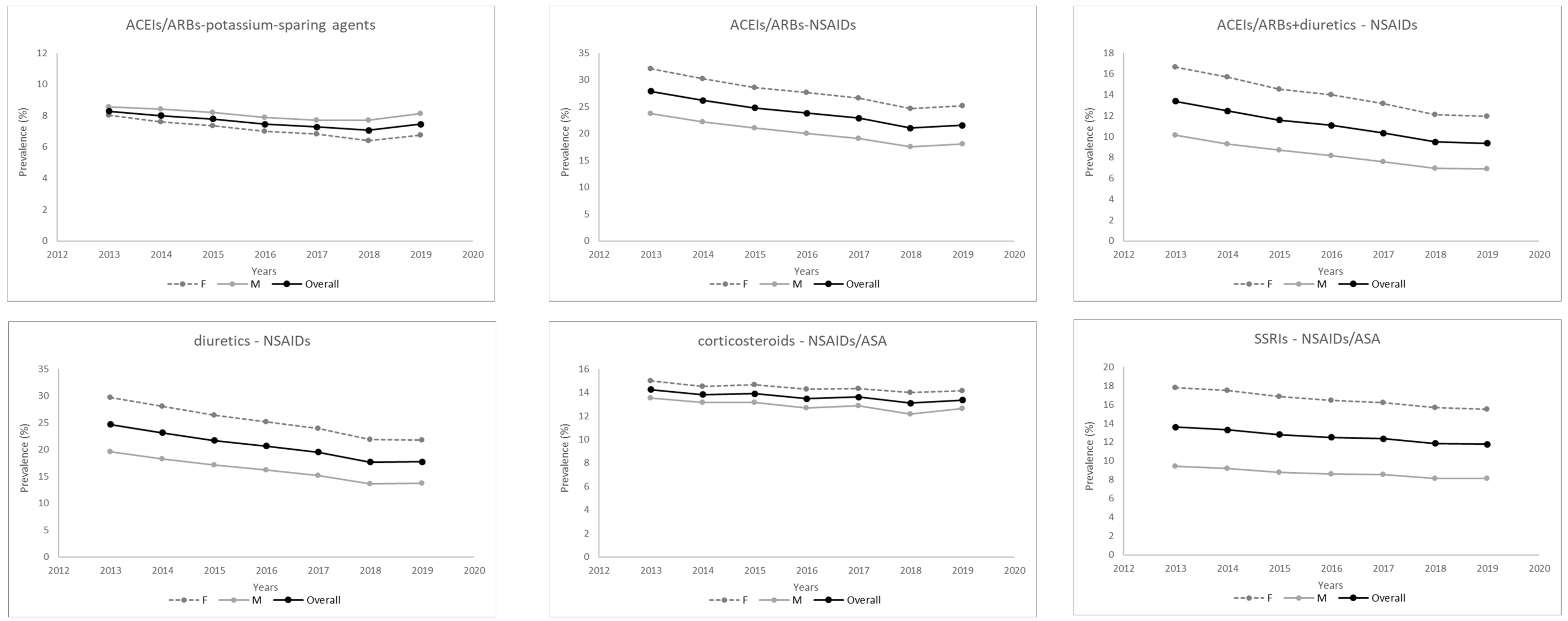
| ACEIs/ARBs—NSAIDs | 27.87 | 21.54 | −22.7 (−23.62; −21.77) |
| ACEIs/ARBs—potassium-sparing agents | 8.28 | 7.45 | −10.06 (−12.12; −7.95) |
| ACEIs/ARBs + diuretics—NSAIDs | 13.38 | 9.37 | −30.00 (−31.33; −28.65) |
| Diuretics—NSAIDs | 24.66 | 17.71 | −28.19 (−29.14; −27.24) |
| SSRIs—NSAIDs/ASA | 13.61 | 11.76 | −13.61 (−15.13; −12.05) |
| vitamin K antagonists—PPIs | 10.75 | 5.64 | −47.52 (−48.75; −46.26) |
| vitamin K antagonists—statins | 8.38 | 4.79 | −42.81 (−44.3; −41.29) |
| Clopidogrel—PPIs | 7.09 | 8.11 | 14.36 (11.67; 17.12) |
| Corticosteroids—NSAIDs/ASA | 14.24 | 13.36 | −6.14 (−7.72; −4.53) |
| 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | ||
|---|---|---|---|---|---|---|---|---|
| Age Group | % | % | % | % | % | % | % | |
| ACEIs/ARBs +potassium-sparing agents | 65–69 years | 6.67 | 6.26 | 6.21 | 6.12 | 6.12 | 6.35 | 6.46 |
| 70–74 years | 7.31 | 7.23 | 6.79 | 6.64 | 6.56 | 6.48 | 6.80 | |
| 75–79 years | 7.99 | 7.66 | 7.58 | 7.24 | 6.95 | 6.75 | 7.35 | |
| 80–84 years | 9.37 | 9.04 | 8.72 | 8.07 | 7.85 | 7.59 | 7.93 | |
| ≥85 years | 9.90 | 9.55 | 9.24 | 8.78 | 8.54 | 7.89 | 8.23 | |
| ACEIs/ARBs +Diuretics—NSAIDs | 65–69 years | 14.77 | 13.86 | 12.56 | 12.00 | 11.11 | 10.17 | 9.78 |
| 70–74 years | 14.81 | 14.13 | 13.19 | 12.62 | 11.72 | 10.59 | 10.42 | |
| 75–79 years | 14.87 | 13.34 | 12.91 | 12.01 | 11.41 | 10.22 | 10.30 | |
| 80–84 years | 12.63 | 12.07 | 11.09 | 10.77 | 10.28 | 9.56 | 9.36 | |
| ≥85 years | 9.25 | 8.72 | 8.02 | 8.08 | 7.24 | 7.03 | 7.07 | |
| ACEIs/ARBs + NSAIDs | 65–69 years | 30.80 | 29.32 | 27.52 | 26.21 | 25.23 | 23.56 | 24.14 |
| 70–74 years | 30.17 | 28.54 | 27.37 | 26.81 | 25.63 | 24.00 | 24.37 | |
| 75–79 years | 29.59 | 27.58 | 26.55 | 25.21 | 24.51 | 22.27 | 22.91 | |
| 80–84 years | 26.74 | 25.26 | 23.98 | 23.05 | 22.34 | 20.34 | 21.03 | |
| ≥85 years | 21.5 | 20.18 | 18.59 | 18.26 | 17.12 | 15.94 | 16.29 | |
| diuretics + NSAIDs | 65–69 years | 24.08 | 22.66 | 21.05 | 20.05 | 18.62 | 17.12 | 16.64 |
| 70–74 years | 24.73 | 23.39 | 22.10 | 21.18 | 19.93 | 18.29 | 18.18 | |
| 75–79 years | 25.65 | 23.50 | 22.57 | 21.19 | 20.25 | 18.15 | 18.57 | |
| 80–84 years | 25.00 | 23.75 | 22.22 | 21.02 | 19.98 | 18.03 | 18.22 | |
| ≥85 years | 23.23 | 21.85 | 20.08 | 19.42 | 18.35 | 16.59 | 16.37 | |
| corticosteroids + NSAIDs/ASA | 65–69 years | 13.79 | 14.24 | 14.05 | 13.84 | 14.32 | 13.97 | 14.29 |
| 70–74 years | 14.19 | 14.16 | 13.97 | 14.06 | 14.07 | 13.72 | 14.24 | |
| 75–79 years | 14.40 | 13.71 | 14.27 | 13.84 | 13.95 | 13.23 | 13.73 | |
| 80–84 years | 13.97 | 13.33 | 13.56 | 13.08 | 13.16 | 12.69 | 13.11 | |
| ≥85 years | 14.78 | 13.84 | 13.57 | 12.62 | 12.72 | 12.17 | 11.84 | |
| SSRIs + NSAIDs/ASA | 65–69 years | 11.54 | 11.22 | 10.73 | 10.66 | 10.42 | 10.08 | 10.15 |
| 70–74 years | 11.98 | 11.80 | 11.64 | 11.42 | 11.19 | 10.75 | 10.66 | |
| 75–79 years | 13.47 | 13.06 | 12.77 | 12.70 | 12.40 | 12.03 | 11.56 | |
| 80–84 years | 14.82 | 14.70 | 13.72 | 13.20 | 13.08 | 12.69 | 12.81 | |
| ≥85 years | 16.10 | 15.39 | 14.71 | 13.87 | 13.97 | 12.91 | 12.85 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galai, E.; Scotti, L.; Gilardetti, M.; Ucciero, A.; Ferrante, D.; Poluzzi, E.; Genazzani, A.A.; Barone-Adesi, F. Time-Trends of Drug-Drug Interactions among Elderly Outpatients in the Piedmont Region (Italy): A Population-Based Study. Int. J. Environ. Res. Public Health 2022, 19, 7353. https://doi.org/10.3390/ijerph19127353
Galai E, Scotti L, Gilardetti M, Ucciero A, Ferrante D, Poluzzi E, Genazzani AA, Barone-Adesi F. Time-Trends of Drug-Drug Interactions among Elderly Outpatients in the Piedmont Region (Italy): A Population-Based Study. International Journal of Environmental Research and Public Health. 2022; 19(12):7353. https://doi.org/10.3390/ijerph19127353
Chicago/Turabian StyleGalai, Elisabetta, Lorenza Scotti, Marco Gilardetti, Andrealuna Ucciero, Daniela Ferrante, Elisabetta Poluzzi, Armando A. Genazzani, and Francesco Barone-Adesi. 2022. "Time-Trends of Drug-Drug Interactions among Elderly Outpatients in the Piedmont Region (Italy): A Population-Based Study" International Journal of Environmental Research and Public Health 19, no. 12: 7353. https://doi.org/10.3390/ijerph19127353
APA StyleGalai, E., Scotti, L., Gilardetti, M., Ucciero, A., Ferrante, D., Poluzzi, E., Genazzani, A. A., & Barone-Adesi, F. (2022). Time-Trends of Drug-Drug Interactions among Elderly Outpatients in the Piedmont Region (Italy): A Population-Based Study. International Journal of Environmental Research and Public Health, 19(12), 7353. https://doi.org/10.3390/ijerph19127353