
Effect of Ankle Weights as a Frailty Prevention Strategy in the Community-Dwelling Elderly: A Preliminary Report

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Sites, and Participants
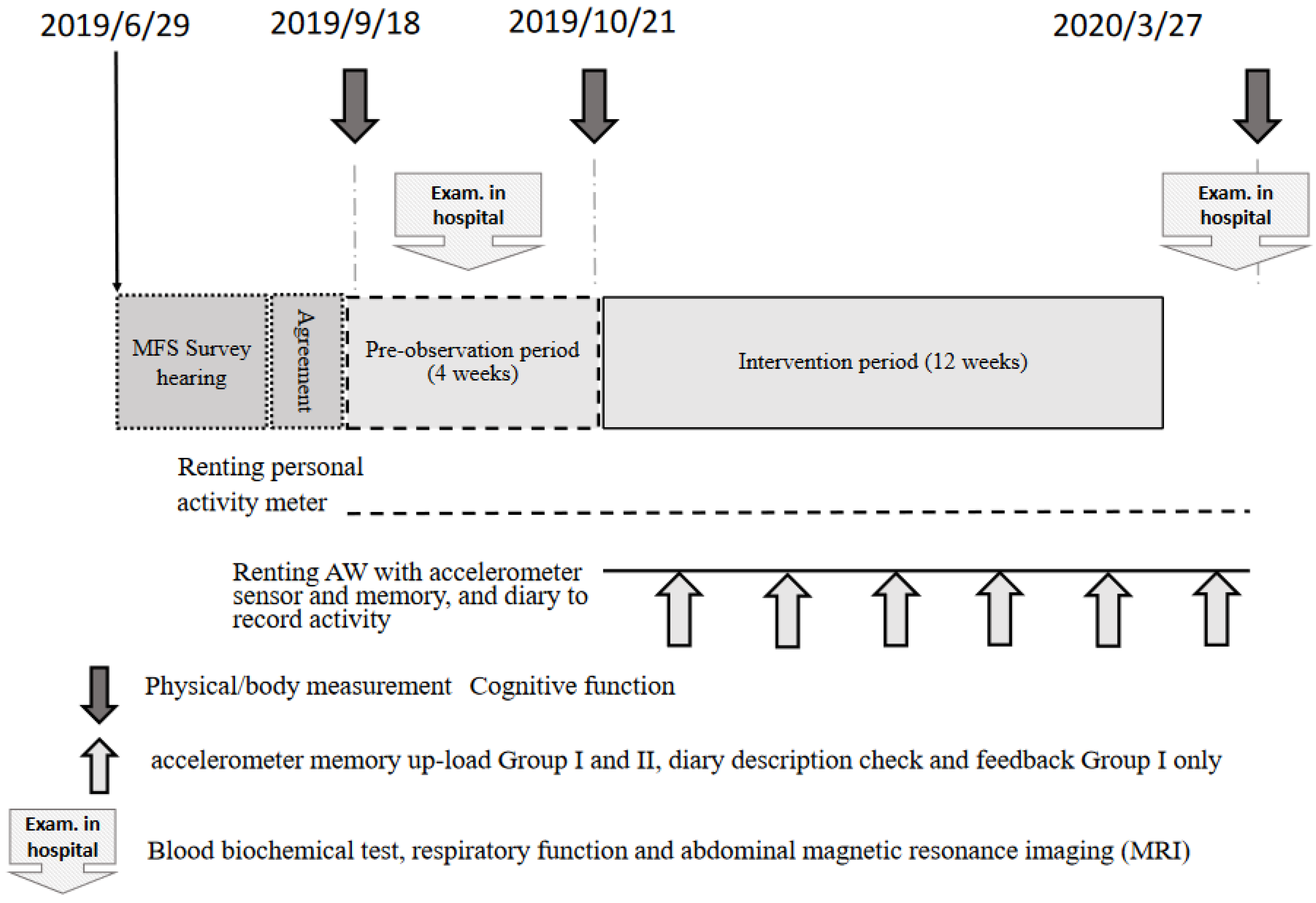
2.2. Schedule and Recording Daily Activity
2.3. Lifestyle Questionnaire Survey
2.4. Muscle Measurements
2.5. Balance and Mobility Tests
2.6. Statistical Analysis
3. Results
3.1. Background Overview and Adverse Events during the Intervention
3.2. Changes in Body Composition before and after Intervention
3.3. Anthropometry
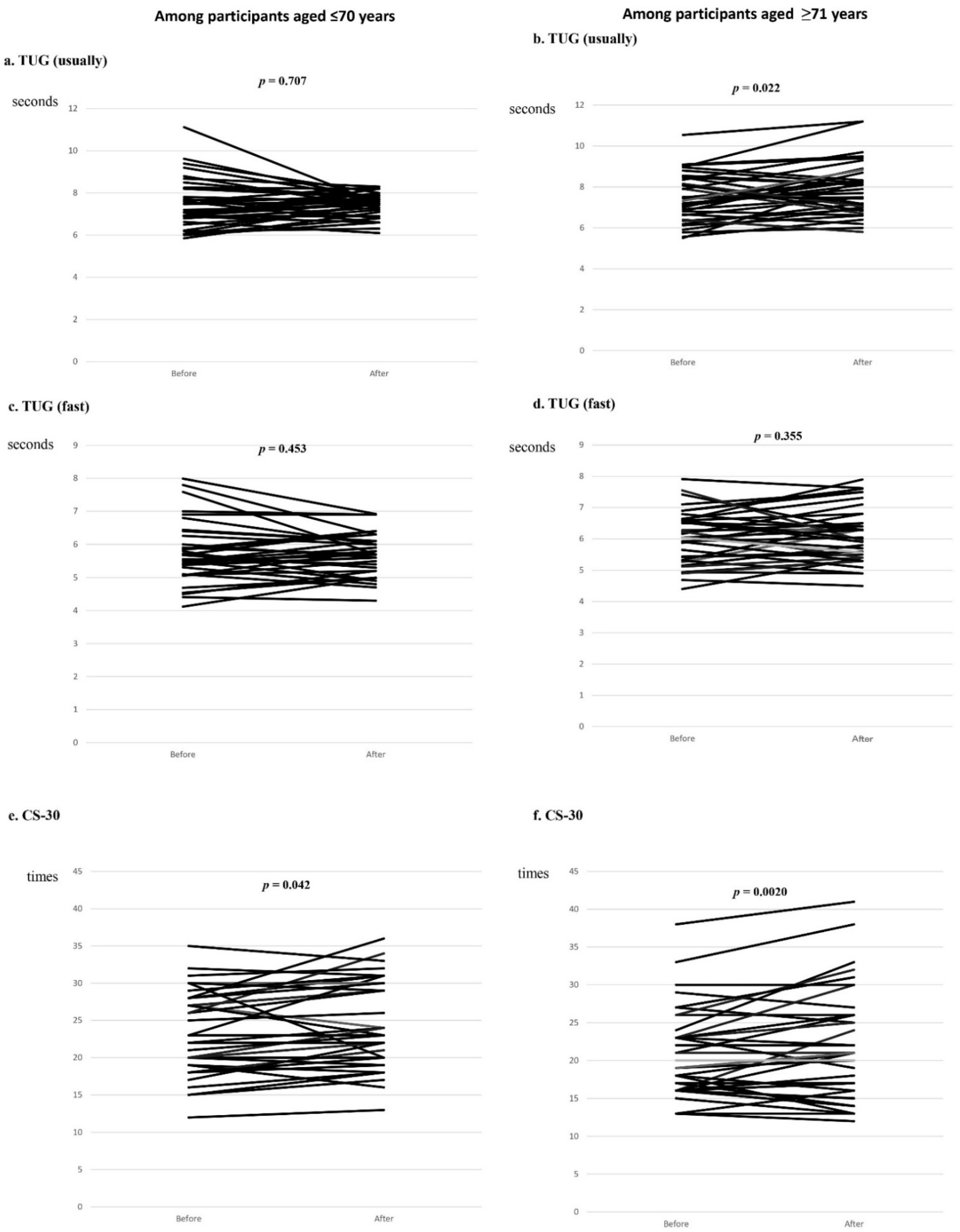
3.4. Performance
3.5. Standing Position Balance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sherrington, C.; Fairhall, N.; Wallbank, G.; Tiedemann, A.; Michaleff, Z.A.; Howard, K.; Clemson, L.; Hopewell, S.; Lamb, S. Exercise for preventing falls in older people living in the community: An abridged Cochrane systematic review. Br. J. Sports Med. 2019, 54, 885–891. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.; Min, L.; Xu, N.; Huang, L.; Li, X. The Effect of Exercise Intervention on Reducing the Fall Risk in Older Adults: A Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2021, 18, 12562. [Google Scholar] [CrossRef] [PubMed]
- Chittrakul, J.; Siviroj, P.; Sungkarat, S.; Sapbamrer, R. Multi-System Physical Exercise Intervention for Fall Prevention and Quality of Life in Pre-Frail Older Adults: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 3102. [Google Scholar] [CrossRef] [PubMed]
- Binder, E.F.; Schechtman, K.B.; Ehsani, A.A.; Steger-May, K.; Brown, M.; Sinacore, D.R.; Yarasheski, K.E.; Holloszy, J.O. Effects of exercise training on frailty in community-dwelling older adults: Results of a randomized, controlled trial. J. Am. Geriatr. Soc. 2002, 50, 1921–1928. [Google Scholar] [CrossRef]
- Bernabei, R.; Landi, F.; Calvani, R.; Cesari, M.; Del Signore, S.; Anker, S.D.; Bejuit, R.; Bordes, P.; Cherubini, A.; Cruz-Jentoft, A.J.; et al. Multicomponent intervention to prevent mobility disability in frail older adults: Randomised controlled trial (SPRINTT project). BMJ 2022, 377, e068788. [Google Scholar] [CrossRef]
- Van Gameren, M.; Bossen, D.; Bosmans, J.E.; Visser, B.; Frazer, S.W.T.; Pijnappels, M. The (cost-) effectiveness of an implemented fall prevention intervention on falls and fall-related injuries among community-dwelling older adults with an increased risk of falls: Protocol for the in balance randomized controlled trial. BMC Geriatr. 2021, 21, 381. [Google Scholar] [CrossRef]
- Mendoza-Ruvalcaba, N.M.; Gutierrez-Herrera, R.; Lopez, C.; Hesse, H.; Soto-Anari, M.; Ramos-Henderson, M.; Cardenas-Valverde, J.C.; Camargo, L.; Caldichoury, N.; Herrera-Pino, J.; et al. Impact of quarantine due to COVID-19 pandemic on health and lifestyle conditions in older adults from Centro American countries. PLoS ONE 2022, 17, e0264087. [Google Scholar] [CrossRef]
- Gao, Z.; Lee, J.E.; McDonough, D.J.; Albers, C. Virtual Reality Exercise as a Coping Strategy for Health and Wellness Promotion in Older Adults during the COVID-19 Pandemic. J. Clin. Med. 2020, 9, 1986. [Google Scholar] [CrossRef]
- Graves, J.E.; Martin, A.D.; Miltenberger, L.A.; Pollock, M.L. Physiological responses to walking with hand weights, wrist weights, and ankle weights. Med. Sci. Sports Exerc. 1988, 20, 265–271. [Google Scholar] [CrossRef]
- Barnett, S.L.; Bagley, A.M.; Skinner, H.B. Ankle weight effect on gait: Orthotic implications. Orthopedics 1993, 16, 1127–1131. [Google Scholar] [CrossRef]
- Zhang, Q.; Liu, Y.; Li, D.; Jia, Y.; Zhang, W.; Chen, B.; Wan, Z. Exercise intervention for the risk of falls in older adults: A protocol for systematic review and meta-analysis. Medicine 2021, 100, e24548. [Google Scholar] [CrossRef] [PubMed]
- Balachandran, A.T.; Steele, J.; Angielczyk, D.; Belio, M.; Schoenfeld, B.J.; Quiles, N.; Askin, N.; Abou-Setta, A.M. Comparison of Power Training vs Traditional Strength Training on Physical Function in Older Adults: A Systematic Review and Meta-analysis. JAMA Netw. Open 2022, 5, e2211623. [Google Scholar] [CrossRef] [PubMed]
- Hoshi, M.; Hozawa, A.; Kuriyama, S.; Nakaya, N.; Ohmori-Matsuda, K.; Sone, T.; Kakizaki, M.; Niu, K.; Fujita, K.; Ueki, S.; et al. The predictive power of physical function assessed by questionnaire and physical performance measures for subsequent disability. Aging Clin. Exp. Res. 2012, 24, 345–353. [Google Scholar] [CrossRef] [PubMed]
- McLester, C.N.; Nickerson, B.S.; Kliszczewicz, B.M.; McLester, J.R. Reliability and agreement of various InBody body composition analyzers as compared with dual-energy X-ray absorptiometry in healthy men and women. J. Clin. Densitom. 2020, 23, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Sugiura, Y.; Tanimoto, Y.; Watanabe, M.; Tsuda, Y.; Kimura, M.; Kusabiraki, T.; Kono, K. Handgrip strength as a predictor of higher-level competence decline among community-dwelling Japanese elderly in an urban area during a 4-year follow-up. Arch. Gerontol. Geriatr. 2013, 57, 319–324. [Google Scholar] [CrossRef]
- Yamagata, M.; Ikezoe, T.; Kamiya, M.; Masaki, M.; Ichihashi, N. Correlation between movement complexity during static standing and balance function in institutionalized older adults. Clin. Interv. Aging 2017, 12, 499–503. [Google Scholar] [CrossRef]
- Vainshelboim, B.; Kramer, M.R.; Myers, J.; Unterman, A.; Izhakian, S.; Oliveira, J. 8-Foot-Up-and-Go Test is associated with hospitalizations and mortality in idiopathic pulmonary fibrosis: A prospective pilot study. Lung 2019, 197, 81–88. [Google Scholar] [CrossRef]
- Jones, C.J.; Rikli, R.E.; Beam, W.C. A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res. Q. Exerc. Sport 1999, 70, 113–119. [Google Scholar] [CrossRef]
- Nara, M.; Sugie, M.; Takahashi, T.; Koyama, T.; Sengoku, R.; Fujiwara, Y.; Obuchi, S.; Harada, K.; Kyo, S.; Ito, H. Japanese version of the Montreal Cognitive Assessment cut-off score to clarify improvement of mild cognitive impairment after exercise training in community-dwelling older adults. Geriatr. Gerontol. Int. 2018, 18, 833–838. [Google Scholar] [CrossRef]
- Weening-Dijksterhuis, E.; de Greef, M.H.; Scherder, E.J.; Slaets, J.P.; van der Schans, C.P. Frail institutionalized older persons: A comprehensive review on physical exercise, physical fitness, activities of daily living, and quality-of-life. Am. J. Phys. Med. Rehabil. 2011, 90, 156–168. [Google Scholar] [CrossRef] [PubMed]
- Daniels, R.; van Rossum, E.; de Witte, L.; Kempen, G.I.; van den Heuvel, W. Interventions to prevent disability in frail community-dwelling elderly: A systematic review. BMC Health Serv. Res. 2008, 8, 278. [Google Scholar] [CrossRef]
- Cameron, I.D.; Fairhall, N.; Langron, C.; Lockwood, K.; Monaghan, N.; Aggar, C.; Sherrington, C.; Lord, S.R.; Kurrle, S.E. A multifactorial interdisciplinary intervention reduces frailty in older people: Randomized trial. BMC Med. 2013, 11, 65. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.W.; Lee, S.K.; Park, J.S.; Ahn, S.H.; Lee, K.J.; Lee, S.J. The effects of ankle weight loading on the walking factors of adults without symptoms. J. Exerc. Rehabil. 2017, 13, 425–429. [Google Scholar] [CrossRef] [PubMed]
- Jette, A.M.; Lachman, M.; Giorgetti, M.M.; Assmann, S.F.; Harris, B.A.; Levenson, C.; Wernick, M.; Krebs, D. Exercise—it’s never too late: The strong-for-life program. Am. J. Public Health 1999, 89, 66–72. [Google Scholar] [CrossRef]
- Sevick, M.A.; Bradham, D.D.; Muender, M.; Chen, G.J.; Enarson, C.; Dailey, M.; Ettinger, W.H., Jr. Cost-effectiveness of aerobic and resistance exercise in seniors with knee osteoarthritis. Med. Sci. Sports Exerc. 2000, 32, 1534–1540. [Google Scholar] [CrossRef]
- Buchner, D.M.; Cress, M.E.; de Lateur, B.J.; Esselman, P.C.; Margherita, A.J.; Price, R.; Wagner, E.H. The effect of strength and endurance training on gait, balance, fall risk, and health services use in community-living older adults. J. Gerontol. A Biol. Sci. Med. Sci. 1997, 52, M218–M224. [Google Scholar] [CrossRef]
- Skelton, D.A.; Young, A.; Greig, C.A.; Malbut, K.E. Effects of resistance training on strength, power, and selected functional abilities of women aged 75 and older. J. Am. Geriatr. Soc. 1995, 43, 1081–1087. [Google Scholar] [CrossRef]
- Latham, N.K.; Anderson, C.S.; Lee, A.; Bennett, D.A.; Moseley, A.; Cameron, I.D.; Fitness Collaborative Group. A randomized, controlled trial of quadriceps resistance exercise and vitamin D in frail older people: The Frailty Interventions Trial in Elderly Subjects (FITNESS). J. Am. Geriatr. Soc. 2003, 51, 291–299. [Google Scholar] [CrossRef]
- Lustosa, L.P.; Silva, J.P.; Coelho, F.M.; Pereira, D.S.; Parentoni, A.N.; Pereira, L.S. Impact of resistance exercise program on functional capacity and muscular strength of knee extensor in pre-frail community-dwelling older women: A randomized crossover trial. Rev. Bras. Fisioter. 2011, 15, 318–324. [Google Scholar] [CrossRef]
- Chou, C.H.; Hwang, C.L.; Wu, Y.T. Effect of exercise on physical function, daily living activities, and quality of life in the frail older adults: A meta-analysis. Arch. Phys. Med. Rehabil. 2012, 93, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Narouei, S.; Akatsu, H.; Watanabe, K. Regional neuromuscular regulation within rectus femoris muscle following three-month limb-loaded walking in older adults. Sports Med. Health Sci. 2022, 4, 38–43. [Google Scholar] [CrossRef]
- Woollacott, M.H.; Shumway-Cook, A.; Nashner, L.M. Aging and posture control: Changes in sensory organization and muscular coordination. Int. J. Aging Hum. Dev. 1986, 23, 97–114. [Google Scholar] [CrossRef] [PubMed]
- Horak, F.B. Clinical measurement of postural control in adults. Phys. Ther. 1987, 67, 1881–1885. [Google Scholar] [CrossRef]
- Gine-Garriga, M.; Roque-Figuls, M.; Coll-Planas, L.; Sitja-Rabert, M.; Salva, A. Physical exercise interventions for improving performance-based measures of physical function in community-dwelling, frail older adults: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2014, 95, 753–769.e3. [Google Scholar] [CrossRef]
- Ganz, D.A.; Latham, N.K. Prevention of falls in community-dwelling older adults. N. Engl. J. Med. 2020, 382, 734–743. [Google Scholar] [CrossRef]
- Raja Adnan, R.N.E.; Mat Din, H.; Ashari, A.; Minhat, H.S. Effectiveness of a community-based muscle strengthening exercise program to increase muscle strength among pre-frail older persons in Malaysia: A pilot study. Front. Public Health 2021, 9, 610184. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| N = 73 | |
|---|---|
| Demographics | |
| Age, years, median (IQR) | 71 (66–76) |
| age > 70, n (%) | 37 (50.7) |
| Men, n (%) | 18 (24.7) |
| Living conditions | |
| Living with family, n (%) | 58 (79.5) |
| Employment status | |
| Employee | 3 (4.1) |
| Self-employed person | 2 (2.7) |
| Homemaker | 27 (37.0) |
| Retiree | 25 (34.2) |
| Part-time job | 11 (15.1) |
| Other | 4 (5.5) |
| Lifestyle factors | |
| Smoking history, n (%) | 6 (8.2) |
| Alcohol consumption, n (%) | 27 (37.0) |
| Problems with sleep, n (%) | 35 (47.9) |
| Clinical factors | |
| One or more underlying diseases, n (%) (n = 71) | 46 (63.0) |
| Experience of hospitalization, n (%) | 31 (42.5) |
| Taking prescription medication, n (%) (n = 72) | 48 (65.8) |
| Age, ≤70 Years N = 36 | Age, >70 Years N = 37 | |||||
|---|---|---|---|---|---|---|
| Parameters | Before | After | p-Value | Before | After | p-Value |
| BMI | 23.0 (3.4) | 23.0 (3.3) | 0.908 | 22.1 (2.3) | 22.2 (2.3) | 0.318 |
| Body fat % | 29.3 (8.3) | 28.9 (8.1) | 0.220 | 28.2 (7.0) | 28.1 (7.2) | 0.941 |
| Muscle mass | 38.8 (7.4) | 39.1 (7.8) | 0.176 | 36.0 (7.5) | 36.1 (7.2) | 0.698 |
| Skeletal muscle mass | 22.2 (4.6) | 22.4 (4.9) | 0.104 | 20.4 (4.6) | 20.5 (4.5) | 0.490 |
| Right arm muscle mass | 2.0 (0.6) | 2.0 (0.5) | 0.722 | 1.8 (0.6) | 1.8 (0.6) | 0.075 |
| Left arm muscle mass | 2.0 (0.6) | 2.0 (0.5) | 0.865 | 1.8 (0.5) | 1.8 (0.5) | 0.097 |
| Trunk muscle mass | 18.0 (3.6) | 18.0 (3.3) | 0.985 | 16.6 (3.4) | 16.7 (3.4) | 0.065 |
| Right leg muscle mass | 6.4 (1.5) | 6.6 (1.7) | 0.287 | 5.8 (1.5) | 5.8 (1.5) | 0.738 |
| Left leg muscle mass | 6.4 (1.5) | 6.5 (1.7) | 0.310 | 5.8 (1.5) | 5.8 (1.4) | 0.596 |
| SMI (n = 22) | 6.5 (0.9) | 6.4 (0.9) | * 0.045 | 6.3 (1.0) | 6.2 (0.9) | * 0.024 |
| Age, ≤70 Years N = 36 | Age, >70 Years N = 37 | |||||
|---|---|---|---|---|---|---|
| Parameters | Before | After | p-Value | Before | After | p-Value |
| Anthropometry | ||||||
| Calf circumference | ||||||
| Right | 39.2 (8.2) | 40.1 (7.9) | 0.551 | 33.5 (3.0) | 33.8 (2.9) | * 0.023 |
| Left | 35.1 (2.6) | 35.0 (3.1) | 0.494 | 33.6 (3.0) | 33.9 (3.1) | * 0.031 |
| Blood pressure (mmHg/mean of right and left arm) | ||||||
| Systolic | 133.3 (23.3) | 133.2 (23.0) | 0.986 | 130.1 (18.5) | 131.8 (13.0) | 0.626 |
| Diastolic | 78.4 (16.9) | 76.8 (16.3) | 0.309 | 69.6 (10.8) | 70.1 (10.4) | 0.474 |
| Heart rate(beat/minutes) | ||||||
| Right | 82.0 (13.5) | 81.0 (10.8) | 0.524 | 76.8 (9.6) | 76.1 (9.0) | 0.635 |
| Performance assessment | ||||||
| Tongue pressure | 39.2 (8.2) | 40.1 (7.9) | 0.199 | 35.6 (8.9) | 37.3 (1.4) | 0.106 |
| Grip strength (mean of right and left arms) | ||||||
| Right arm (kg) | 30.0 (8.1) | 30.2 (7.3) | 0.818 | 25.4 (6.7) | 25.4 (6.9) | 0.928 |
| Left arm (kg) | 27.2 (6.8) | 27.5 (6.6) | 0.637 | 25.4 (6.9) | 23.3 (6.0) | 0.099 |
| OLST total 120, n (%) | 21 (58.3) | 20 (55.6) | 1.000 | 11 (29.7) | 13 (35.1) | 0.804 |
| 3.0 m walking (second) | 1.7 (0.2) | 1.6 (0.2) | * 0.012 | 1.7 (0.3) | 1.7 (0.3) | 0.225 |
| TUG (usual) (second) | 7.5 (1.2) | 7.4 (1.2) | 0.707 | 7.5 (1.2) | 7.8 (1.3) | (0.022) |
| TUG (fast) (second) | 5.7 (0.9) | 5.7 (0.6) | 0.453 | 6.3 (0.8) | 6.1 (0.9) | 0.355 |
| CS-30 (times) | 23.4 (5.6) | 24.7 (5.9) | 0.042 | 21.0 (5.9) | 22.4 (7.3) | * 0.020 |
| MOCA-J (points) | 28.0 (2.1) | 28.1 (1.9) | 0.782 | 26.0 (3.0) | 26.1 (3.1) | 0.772 |
| ≤26 points n (%) | 32 (88.9) | 32 (88.9) | 1.000 | 24 (64.9) | 25 (67.6) | 1.000 |
| Balance in standing position | ||||||
| Eyes open | ||||||
| Area (cm2) | 4.48 (1.94) | 4.88 (2.67) | 0.502 | 4.29 (2.69) | 4.03 (2.16) | 0.451 |
| Speed (cm/s) | 1.76 (0.47) | 1.80 (0.47) | 0.655 | 1.73 (0.48) | 1.82 (0.68) | 0.186 |
| Density (1/cm) | 27.14 (11.02) | 27.76 (13.42) | 0.820 | 29.0 (11.37) | 30.26 (9.85) | 0.401 |
| Center left and right (cm) | 0.05 (0.52) | −0.10 (0.66) | 0.177 | −0.13 (0.90) | −0.04 (0.63) | 0.639 |
| Center front and rear (cm) | −0.56 (1.69) | −0.13 (0.90) | * 0.012 | −0.13 (0.63) | −0.23 (1.20) | 0.706 |
| Berg Balance Scale score | 1.33 (0.49) | 1.27 (0.49) | 0.762 | 1.33 (0.80) | 1.35 (0.49) | 0.889 |
| Short area (cm2) | 10.53 (4.58) | 11.79 (6.06) | 0.351 | 10.49 (7.27) | 9.03 (5.72) | 0.086 |
| Rms value area (cm2) | 2.39 (1.58) | 2.35 (1.36) | 0.923 | 2.00 (5.73) | 1.84 (1.08) | 0.482 |
| Total track length (cm) | 100.29 (36.83) | 108.03 (29.24) | 0.168 | 103.56 (28.57) | 108.93 (40.63) | 0.195 |
| Eyes closed | ||||||
| Area (cm2) | 5.81(2.87) | 5.28 (2.20) | 0.177 | 5.23 (3.43) | 5.34 (3.38) | 0.823 |
| Speed (cm/s) | 2.52 (0.95) | 2.30 (0.73) | 0.148 | 2.50 (1.25) | 2.52 (1.18) | 0.778 |
| Congestion (1/cm) | 30.48 (12.93) | 29.68 (12.48) | 0.652 | 32.55 (11.59) | 32.23 (11.65) | 0.870 |
| Center left and right (cm) | 0.09 (0.65) | −0.16 (1.78) | * 0.039 | −0.12 (0.67) | −0.10 (0.77) | 0.935 |
| Center front and rear (cm) | −0.08 (1.78) | −0.82 (1.00) | * 0.021 | 0.24 (1.61) | 0.11 (1.26) | 0.650 |
| Berg Balance Scale score | 14.58 (7.59) | 13.05 (5.09) | 0.298 | 12.97 (8.91) | 11.76 (6.78) | 0.264 |
| Short area (cm2) | 2.45 (1.17) | 2.25 (0.96) | 0.118 | 2.20 (1.40) | 2.20 (1.26) | 0.950 |
| Rms value area (cm2) | 151.23 (56.81) | 138.17 (43.83) | 0.151 | 149.71 (75.30) | 151.51 (70.53) | 0.773 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akatsu, H.; Manabe, T.; Kawade, Y.; Masaki, Y.; Hoshino, S.; Jo, T.; Kobayashi, S.; Hayakawa, T.; Ohara, H. Effect of Ankle Weights as a Frailty Prevention Strategy in the Community-Dwelling Elderly: A Preliminary Report. Int. J. Environ. Res. Public Health 2022, 19, 7350. https://doi.org/10.3390/ijerph19127350
Akatsu H, Manabe T, Kawade Y, Masaki Y, Hoshino S, Jo T, Kobayashi S, Hayakawa T, Ohara H. Effect of Ankle Weights as a Frailty Prevention Strategy in the Community-Dwelling Elderly: A Preliminary Report. International Journal of Environmental Research and Public Health. 2022; 19(12):7350. https://doi.org/10.3390/ijerph19127350
Chicago/Turabian StyleAkatsu, Hiroyasu, Toshie Manabe, Yoshihiro Kawade, Yoshiyuki Masaki, Shigeru Hoshino, Takashi Jo, Shinya Kobayashi, Tomihiro Hayakawa, and Hirotaka Ohara. 2022. "Effect of Ankle Weights as a Frailty Prevention Strategy in the Community-Dwelling Elderly: A Preliminary Report" International Journal of Environmental Research and Public Health 19, no. 12: 7350. https://doi.org/10.3390/ijerph19127350
APA StyleAkatsu, H., Manabe, T., Kawade, Y., Masaki, Y., Hoshino, S., Jo, T., Kobayashi, S., Hayakawa, T., & Ohara, H. (2022). Effect of Ankle Weights as a Frailty Prevention Strategy in the Community-Dwelling Elderly: A Preliminary Report. International Journal of Environmental Research and Public Health, 19(12), 7350. https://doi.org/10.3390/ijerph19127350