
Positive Effect of Air Purifier Intervention on Baroreflex Sensitivity and Biomarkers of Oxidative Stress in Patients with Coronary Artery Disease: A Randomized Crossover Intervention Trial

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
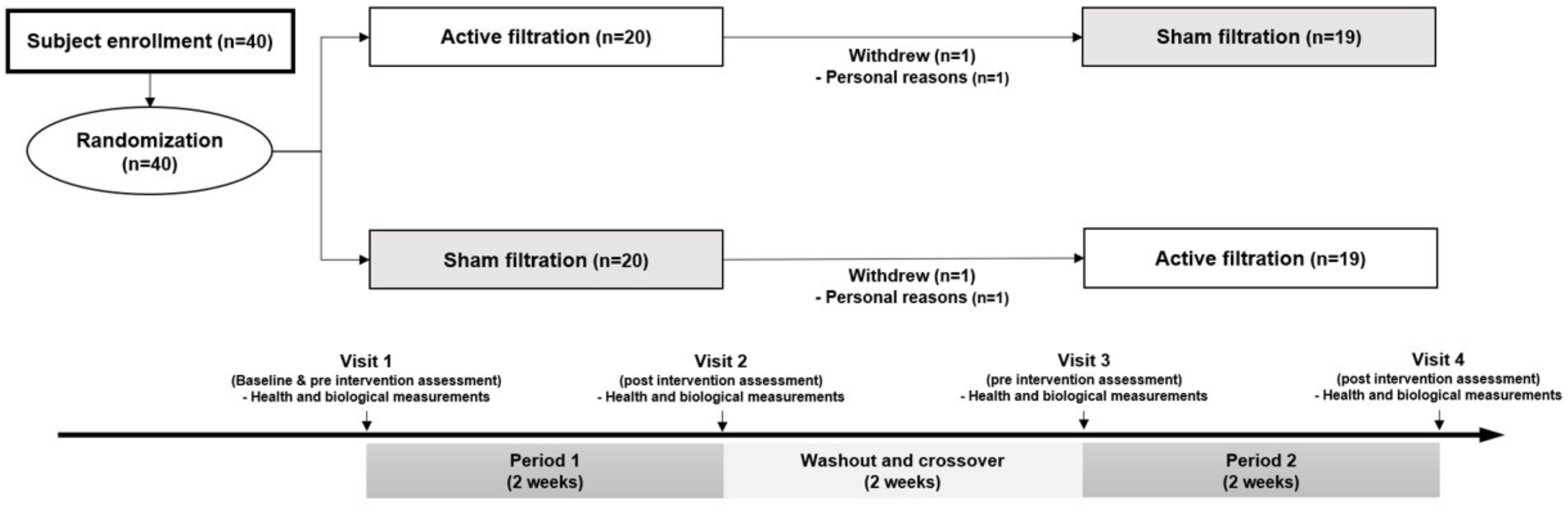
2.2. Study Design
2.3. Indoor and Outdoor Particulate Matter Assessments
2.4. Health Measurements
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Burnett, R.T.; Pope, C.A., III; Ezzati, M.; Olives, C.; Lim, S.S.; Mehta, S.; Shin, H.H.; Singh, G.; Hubbell, B.; Brauer, M.; et al. An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ. Health Perspect. 2014, 122, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Lu, F.; Xu, D.; Cheng, Y.; Dong, S.; Guo, C.; Jiang, X.; Zheng, X. Systematic review and meta-analysis of the adverse health effects of ambient PM2.5 and PM10 pollution in the Chinese population. Environ. Res. 2015, 136, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., III; Dockery, D.W. Health effects of fine particulate air pollution: Lines that connect. J. Air Waste Manag. Assoc. 2006, 56, 709–742. [Google Scholar] [CrossRef] [PubMed]
- Al-Kindi, S.G.; Brook, R.D.; Biswal, S.; Rajagopalan, S. Environmental determinants of cardiovascular disease: Lessons learned from air pollution. Nat. Rev. Cardiol. 2020, 17, 656–672. [Google Scholar] [CrossRef]
- Hamanaka, R.B.; Mutlu, G.M. Particulate matter air pollution: Effects on the cardiovascular system. Front. Endocrinol. 2018, 9, 680. [Google Scholar] [CrossRef] [Green Version]
- Burnett, R.; Chen, H.; Szyszkowicz, M.; Fann, N.; Hubbell, B.; Pope, C.A., III; Apte, J.S.; Brauer, M.; Cohen, A.; Weichenthal, S.; et al. Global estimates of mortality associated with long-term exposure to outdoor fine particulate matter. Proc. Natl. Acad. Sci. USA 2018, 115, 9592–9597. [Google Scholar] [CrossRef] [Green Version]
- Dominici, F.; Peng, R.D.; Zeger, S.L.; White, R.H.; Samet, J.M. Particulate air pollution and mortality in the United States: Did the risks change from 1987 to 2000? Am. J. Epidemiol. 2007, 166, 880–888. [Google Scholar] [CrossRef]
- Yorifuji, T.; Kashima, S.; Doi, H. Fine-particulate Air Pollution from Diesel Emission Control and Mortality Rates in Tokyo: A Quasi-experimental Study. Epidemiology 2016, 27, 769–778. [Google Scholar] [CrossRef]
- Brauner, E.V.; Forchhammer, L.; Moller, P.; Barregard, L.; Gunnarsen, L.; Afshari, A.; Wåhlin, P.; Glasius, M.; Dragsted, L.O.; Basu, S.; et al. Indoor particles affect vascular function in the aged: An air filtration-based intervention study. Am. J. Respir. Crit. Care Med. 2008, 177, 419–425. [Google Scholar] [CrossRef]
- Allen, R.W.; Carlsten, C.; Karlen, B.; Leckie, S.; van Eeden, S.; Vedal, S.; Wong, I.; Brauer, M. An air filter intervention study of endothelial function among healthy adults in a woodsmoke-impacted community. Am. J. Respir. Crit. Care Med. 2011, 183, 1222–1230. [Google Scholar] [CrossRef]
- Shao, D.; Du, Y.; Liu, S.; Brunekreef, B.; Meliefste, K.; Zhao, Q.; Chen, J.; Song, X.; Wang, M.; Wang, J.; et al. Cardiorespiratory responses of air filtration: A randomized crossover intervention trial in seniors living in Beijing: Beijing Indoor Air Purifier Study, BIAPSY. Sci. Total Environ. 2017, 603–604, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Zhao, A.; Chen, H.; Zhao, Z.; Cai, J.; Wang, C.; Yang, C.; Li, H.; Xu, X.; Ha, S.; et al. Cardiopulmonary benefits of reducing indoor particles of outdoor origin: A randomized, double-blind crossover trial of air purifiers. J. Am. Coll. Cardiol. 2015, 65, 2279–2287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morishita, M.; Adar, S.D.; D’Souza, J.; Ziemba, R.A.; Bard, R.L.; Spino, C.; Brook, R.D. Effect of Portable Air Filtration Systems on Personal Exposure to Fine Particulate Matter and Blood Pressure Among Residents in a Low-Income Senior Facility: A Randomized Clinical Trial. JAMA Intern. Med. 2018, 178, 1350–1357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chun, K.J.; Yim, H.R.; Park, J.; Park, S.J.; Park, K.M.; On, Y.K.; Kim, J.S. Role of Baroreflex Sensitivity in Predicting Tilt Training Response in Patients with Neurally Mediated Syncope. Yonsei Med. J. 2016, 57, 313–320. [Google Scholar] [CrossRef]
- Low, P.A. Testing the autonomic nervous system. Semin. Neurol. 2003, 23, 407–421. [Google Scholar] [CrossRef]
- Novak, P. Quantitative autonomic testing. J. Vis. Exp. 2011, e2502. [Google Scholar] [CrossRef] [Green Version]
- Deanfield, J.E.; Halcox, J.P.; Rabelink, T.J. Endothelial function and dysfunction: Testing and clinical relevance. Circulation 2007, 115, 1285–1295. [Google Scholar] [CrossRef]
- Fu, P.; Guo, X.; Cheung, F.M.H.; Yung, K.K.L. The association between PM2.5 exposure and neurological disorders: A systematic review and meta-analysis. Sci. Total Environ. 2019, 655, 1240–1248. [Google Scholar] [CrossRef]
- Krewski, D.; Jerrett, M.; Burnett, R.T.; Ma, R.; Hughes, E.; Shi, Y.; Turner, M.C.; Pope, C.A., III; Thurston, G.; Calle, E.E.; et al. Extended Follow-Up and Spatial Analysis of the American Cancer Society Study Linking Particulate Air Pollution and Mortality; Health Effects Institute: Boston, MA, USA, 2009. [Google Scholar]
- Crouse, D.L.; Peters, P.A.; van Donkelaar, A.; Goldberg, M.S.; Villeneuve, P.J.; Brion, O.; Khan, S.; Atari, D.O.; Jerrett, M.; Pope, C.A., III; et al. Risk of nonaccidental and cardiovascular mortality in relation to long-term exposure to low concentrations of fine particulate matter: A Canadian national-level cohort study. Environ. Health Perspect. 2012, 120, 708–714. [Google Scholar] [CrossRef]
- Mustafic, H.; Jabre, P.; Caussin, C.; Murad, M.H.; Escolano, S.; Tafflet, M.; Périer, M.-C.; Marijon, E.; Vernerey, D.; Empana, J.-P.; et al. Main air pollutants and myocardial infarction: A systematic review and meta-analysis. JAMA 2012, 307, 713–721. [Google Scholar] [CrossRef]
- Nagayoshi, Y.; Kawano, H.; Hokamaki, J.; Miyamoto, S.; Kojima, S.; Shimomura, H.; Tsujita, K.; Sakamoto, T.; Yoshimura, M.; Ogawa, H. Urinary 8-hydroxy-2′-deoxyguanosine levels increase after reperfusion in acute myocardial infarction and may predict subsequent cardiac events. Am. J. Cardiol. 2005, 95, 514–517. [Google Scholar] [CrossRef] [PubMed]
- Mizukoshi, G.; Katsura, K.; Katayama, Y. Urinary 8-hydroxy-2′-deoxyguanosine and serum S100beta in acute cardioembolic stroke patients. Neurol. Res. 2005, 27, 644–646. [Google Scholar] [CrossRef] [PubMed]
- Brea, D.; Roquer, J.; Serena, J.; Segura, T.; Castillo, J.; Artico, S. Oxidative stress markers are associated to vascular recurrence in non-cardioembolic stroke patients non-treated with statins. BMC Neurol. 2012, 12, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chuang, H.C.; Ho, K.F.; Lin, L.Y.; Chang, T.Y.; Hong, G.B.; Ma, C.M.; Liu, I.-J.; Chuang, K.-J. Long-term indoor air conditioner filtration and cardiovascular health: A randomized crossover intervention study. Environ. Int. 2017, 106, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Martin, B.L.; Thompson, L.C.; Kim, Y.H.; King, C.; Snow, S.; Schladweiler, M.; Haykal-Coates, N.; George, I.; Gilmour, M.I.; Kodavanti, U.P.; et al. Peat smoke inhalation alters blood pressure, baroreflex sensitivity, and cardiac arrhythmia risk in rats. J. Toxicol. Environ. Health Part A 2020, 83, 748–763. [Google Scholar] [CrossRef] [PubMed]
- Carll, A.P.; Crespo, S.M.; Filho, M.S.; Zati, D.H.; Coull, B.A.; Diaz, E.A.; Raimundo, R.D.; Jaeger, T.N.G.; Ricci-Vitor, A.L.; Papapostolou, V.; et al. Inhaled ambient-level traffic-derived particulates decrease cardiac vagal influence and baroreflexes and increase arrhythmia in a rat model of metabolic syndrome. Part. Fibre Toxicol. 2017, 14, 16. [Google Scholar] [CrossRef]
- La Rovere, M.T.; Bigger, J.T., Jr.; Marcus, F.I.; Mortara, A.; Schwartz, P.J. Baroreflex sensitivity and heart-rate variability in prediction of total cardiac mortality after myocardial infarction. Lancet 1998, 351, 478–484. [Google Scholar] [CrossRef]
- McDonald, E.; Cook, D.; Newman, T.; Griffith, L.; Cox, G.; Guyatt, G. Effect of air filtration systems on asthma: A systematic review of randomized trials. Chest 2002, 122, 1535–1542. [Google Scholar] [CrossRef]

{kind=link}
| Variable | Mean ± STD or N (%) | |
|---|---|---|
| Number | 38 | |
| Age | yrs | 65.8 ± 6.4 |
| Sex | Male:female | 8:30 |
| Height | cm | 165.1 ± 7.9 |
| Weight | kg | 69.1 ± 8.7 |
| BMI | kg/m2 | 25.4 ± 3.1 |
| Clinical diagnosis | STEMI | 17 (44.7) |
| NSTEMI | 6 (15.8) | |
| Unstable angina | 15 (39.5) | |
| Number of of prior PCI | 1 | 34 (89.5) |
| 2 | 4 (10.5) | |
| Underlying disease | Hypertension | 13 (34.2) |
| Diabetes | 13 (34.2) | |
| Dyslipidemia | 10 (26.3) | |
| HF | 2 (5.3) | |
| TIA | 1 (2.6) | |
| Antianginal medication | Beta blocker | 26 (68.4) |
| ACEI/ARB | 20 (52.6) | |
| Nitrate | 7 (18.4) | |
| Smoking status | Current smokers | 8 (21.1) |
| Secondary smokers | 13 (34.2) | |
| Intervention | p-Value | |||
|---|---|---|---|---|
| Sham Filtration | Active Filtration | |||
| PM10, µg/m3 | Indoors | 27.4 ± 18.2 | 18.6 ± 10.6 | <0.001 |
| Outdoors | 40.2 ± 7.9 | 43.3 ± 9.9 | 0.032 | |
| PM2.5, µg/m3 | Indoors | 18.6 ± 14.9 | 12.3 ± 8.0 | <0.001 |
| Outdoors | 23.4 ± 5.5 | 26.0 ± 7.2 | 0.007 | |
| Sham Filtration | Active Filtration | |||||
|---|---|---|---|---|---|---|
| Pre | Post | p-Value | Pre | Post | p-Value | |
| Blood pressure | ||||||
| SBP (mmHg) | 125.50 (2.10) | 121.70 (2.19) | 0.091 | 126.40 (1.90) | 121.90 (2.31) | 0.065 |
| DBP (mmHg) | 73.96 (1.26) | 73.98 (1.52) | 0.984 | 74.27 (1.36) | 73.90 (1.61) | 0.815 |
| HR (beats/min) | 63.30 (1.95) | 63.86 (2.10) | 0.590 | 63.36 (1.89) | 64.79 (1.93) | 0.266 |
| Autonomic nerve function | ||||||
| xBRS (ms/mmHg) | 7.33 (0.88) | 8.02 (0.81) | 0.248 | 7.96 (0.70) | 9.52 (0.74) | 0.028 |
| Inflammation and oxidative stress markers | ||||||
| CRP (mg/dL) | 0.52 (0.07) | 0.51 (0.10) | 0.469 | 0.59 (0.10) | 0.68 (0.18) | 0.132 |
| IL-6 (pg/mL) | 2.65 (0.27) | 2.57 (0.28) | 0.738 | 2.51 (0.27) | 3.01 (0.44) | 0.118 |
| BNP (pg/mL) | 30.07 (4.37) | 31.55 (5.45) | 0.616 | 24.25 (3.95) | 25.55 (4.80) | 0.518 |
| 8-OHdG (µg/g creatinine) | 7.63 (0.76) | 8.58 (0.68) | 0.016 | 7.59 (0.64) | 7.15 (0.83) | 0.431 |
| Outcomes | Intervention (Active vs. Sham) | Indoor PM2.5 Level (One Percent Increase) | ||||
|---|---|---|---|---|---|---|
| Percent, % | 95% CI | p-Value | Percent, % | 95% CI | p-Value | |
| Blood pressure | ||||||
| SBP (mmHg) | −0.71 | −4.17, 2.87 | 0.736 | −1.25 | −6.38, 3.87 | 0.622 |
| DBP (mmHg) | −0.32 | −3.86, 3.34 | 0.880 | −2.51 | −7.97, 2.95 | 0.356 |
| HR (beats/min) | 0.50 | −3.91, 5.10 | 0.853 | −3.38 | −8.59, 1.83 | 0.196 |
| Autonomic nerve function | ||||||
| xBRS (ms/mmHg) | 14.44 | −2.67, 34.57 | 0.168 | −19.94 | −39.29, −0.59 | 0.044 |
| Inflammation and oxidative stress markers | ||||||
| CRP (mg/dL) | 17.36 | −15.68, 63.36 | 0.418 | −8.60 | −54.01, 36.82 | 0.703 |
| IL-6 (pg/mL) | −5.61 | −21.00, 12.77 | 0.587 | 20.10 | −1.40, 41.59 | 0.066 |
| BNP (pg/mL) | 18.82 | −1.91, 43.91 | 0.138 | −1.15 | −29.71, 27.40 | 0.935 |
| 8-OHdG (µg/g creatinine) | −15.56 | −25.38, −4.45 | 0.027 | 3.35 | −13.69, 20.40 | 0.692 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eom, S.-Y.; Kim, A.; Lee, J.-H.; Kim, S.M.; Lee, S.-Y.; Hwang, K.-K.; Lim, H.-J.; Cho, M.-C.; Kim, Y.-D.; Bae, J.-W.; et al. Positive Effect of Air Purifier Intervention on Baroreflex Sensitivity and Biomarkers of Oxidative Stress in Patients with Coronary Artery Disease: A Randomized Crossover Intervention Trial. Int. J. Environ. Res. Public Health 2022, 19, 7078. https://doi.org/10.3390/ijerph19127078
Eom S-Y, Kim A, Lee J-H, Kim SM, Lee S-Y, Hwang K-K, Lim H-J, Cho M-C, Kim Y-D, Bae J-W, et al. Positive Effect of Air Purifier Intervention on Baroreflex Sensitivity and Biomarkers of Oxidative Stress in Patients with Coronary Artery Disease: A Randomized Crossover Intervention Trial. International Journal of Environmental Research and Public Health. 2022; 19(12):7078. https://doi.org/10.3390/ijerph19127078
Chicago/Turabian StyleEom, Sang-Yong, Aryun Kim, Ju-Hee Lee, Sang Min Kim, Sang-Yeub Lee, Kyung-Kuk Hwang, Hyun-Joung Lim, Myeong-Chan Cho, Yong-Dae Kim, Jang-Whan Bae, and et al. 2022. "Positive Effect of Air Purifier Intervention on Baroreflex Sensitivity and Biomarkers of Oxidative Stress in Patients with Coronary Artery Disease: A Randomized Crossover Intervention Trial" International Journal of Environmental Research and Public Health 19, no. 12: 7078. https://doi.org/10.3390/ijerph19127078
APA StyleEom, S.-Y., Kim, A., Lee, J.-H., Kim, S. M., Lee, S.-Y., Hwang, K.-K., Lim, H.-J., Cho, M.-C., Kim, Y.-D., Bae, J.-W., Kim, J. H., & Lee, D.-I. (2022). Positive Effect of Air Purifier Intervention on Baroreflex Sensitivity and Biomarkers of Oxidative Stress in Patients with Coronary Artery Disease: A Randomized Crossover Intervention Trial. International Journal of Environmental Research and Public Health, 19(12), 7078. https://doi.org/10.3390/ijerph19127078