
Usability Evaluation and Classification of mHealth Applications for Type 2 Diabetes Mellitus Using MARS and ID3 Algorithm


 ,
,  and
and
Abstract
:1. Introduction
- Evaluating the usability of mHealth applications for T2DM and ranking the applications using MARS methodology.
- Choosing the best mHealth applications for T2DM using the ID3 decision making algorithm.
2. Proposed Methodology
2.1. Alternatives Used for the Study
- It can track blood sugar, insulin, weight, blood pressure, A1C, and other trends, as well as record blood glucose, medicine, and meals all in one entry;
- Adds notes to entries for future reference and automatically track walks and other aerobic exercises;
- It offers real-time blood sugar monitoring as a straightforward and convenient way to control diabetes;
- It provides expert advice and help.
- It assists in presenting detailed information to the user. It provides good, remote diabetes management;
- It presents the material in a statistical format (such as a bar chart) to aid comprehension;
- It can recognize trends and look for any pre-defined recurring issues as well as the causes of their occurrence;
- It has an insulin bolus calculator that calculates insulin based on dietary information.
- It may record blood glucose, medicine details, and meals all in one entry, as well as track blood sugar, insulin, weight, blood pressure, A1C, and other trends;
- It has a customizable logging screen that can record data from a Bluetooth-enabled blood glucose meter and analyze the trend to give you a rapid summary of your blood glucose levels;
- It has a superior search capability for documenting meals and activities, which makes diabetes management easier;
- Reminders and recommendations on blood pressure, diabetes, food, exercise, foot, eyes, kidneys, and cardiovascular risks are available;
- It is capable of providing the highest level of data protection, as required by the general data protection rule (GDPR);
- Users can get important medical data from the app and export it as a PDF report or an Excel file.
- It may record blood glucose, medicine details, and meals all in one entry, as well as track blood sugar, insulin, weight, blood pressure, A1C, and other trends;
- All blood glucose readings are instantly saved on the app’s blood sugar diary and may be evaluated using simple graphs;
- It uses color coding to show high, low, and normal blood sugar levels;
- It syncs with the fitness tracker so you can track your steps and see how many calories you burned in a day right on the app. It works with Google Fit, Apple Health Kit, Fit Bit, and other popular fitness trackers to provide a unified view of health and activity data.
- It measures blood glucose at various levels throughout the day (for example, at breakfast, lunch, and dinner) to help patients maintain efficient blood sugar control;
- Among other things, it can monitor blood pressure, weight, and HbA1c levels;
- It allows the user to filter the history by event type/tag, which is useful for keeping track of things such as exercise reactions and food preferences.
- It conveniently logs blood glucose readings and allows users to add notes, pick medications, eat foods, and attach images;
- It keeps track of blood pressure measurements and allows you to enter systolic, diastolic, and pulse readings to monitor how you are doing with blood pressure control;
- It can keep track of weight changes and one can enter the weight and body fat, set goals, and easily see the progress made;
- It has a dashboard that gives a quick analysis of the recent blood sugar history in table and graph formats. One can see whether the readings are within range, the movement of the readings, and can even chart differences between before-meal and after-meal readings;
- It has a diary that allows the user to easily review past blood sugar records. One can quickly see what factors contributed to a high or low reading;
- It can keep track of the A1C history and allows the data entered on the app to be exported as a PDF Report or Excel file.
- It organizes blood sugar information in a way that beginner users may understand using a unique color-coding technique;
- It sends out automatic alerts when repeated highs or lows occur, allowing the user to take appropriate action;
- It sets a daily goal for the logging of steps, carbs, and activities;
- It reminds the user when it is time to take a blood sugar test and when to take insulin.
- It keeps track of blood glucose levels and blood pressure readings so one can monitor how one is doing with blood pressure control;
- It can keep track of weight changes, and one can enter the weight and body fat, set goals, and easily see the progress made;
- It can aid in the comparison of physical activity and weight-checking findings entered in various sessions;
- It can give patients specific advice on how to effectively handle a problem;
- It reminds patients when to take medicine and about other self-care activities, as well as predicts their condition based on data entered into the system.
- It keeps track of the blood glucose levels, blood pressure, activity, BMI, and more with ease;
- It can assist with weight management and HbA1c levels;
- It can aid in the management of Type 1, Type 2, and gestational diabetes by providing motivating patterns and feedback;
- It can be used to keep track of medications and data can be exported as a PDF report or an Excel spreadsheet.
- It allows the user to easily track blood pressure, activity, BMI, blood glucose levels, and more;
- It enables the monitoring and management of blood sugar levels with the blood sugar monitor;
- It allows one to discover the top diabetic risk factors and how to manage them if you have diabetes;
- It provides reminders and recommendations on how to manage the blood pressure, glucose, nutrition, activity, foot, eyes, kidneys, and cardiovascular risks;
- It uses motivational trends and feedback to help manage Type 1, Type 2, and gestational diabetes;
- It provides diabetes analysis on a daily, weekly, monthly, and annual basis;
- It allows the user to backup diabetic data safely;
- Over 100 devices can be connected to track the activity, weight reduction, BMI, blood pressure, blood sugar, and other metrics. With the addition of other devices, one will be able to take control of their diabetes quickly.
- It enables users to add notes, choose medications, eat foods, and upload photographs to their blood glucose readings;
- It can keep track of weight changes and allows users to enter their weight and body fat percentage, set goals, and track their progress;
- It can also track blood pressure and HbA1c levels, among other things;
- It establishes a daily goal for tracking steps, carbohydrates, and activities;
- It allows users to get important medical information and export data as a PDF report or an Excel spreadsheet from the app.
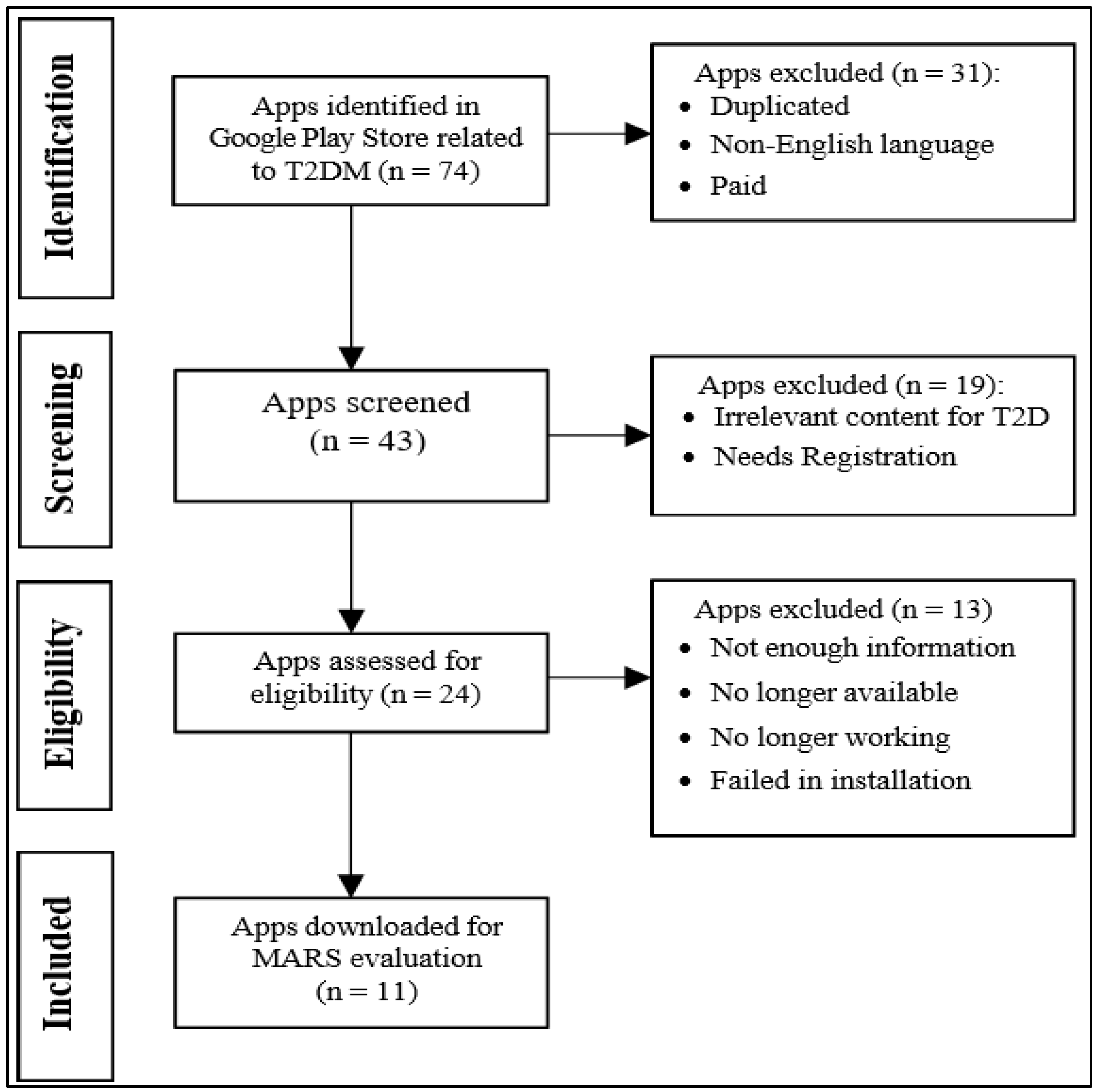
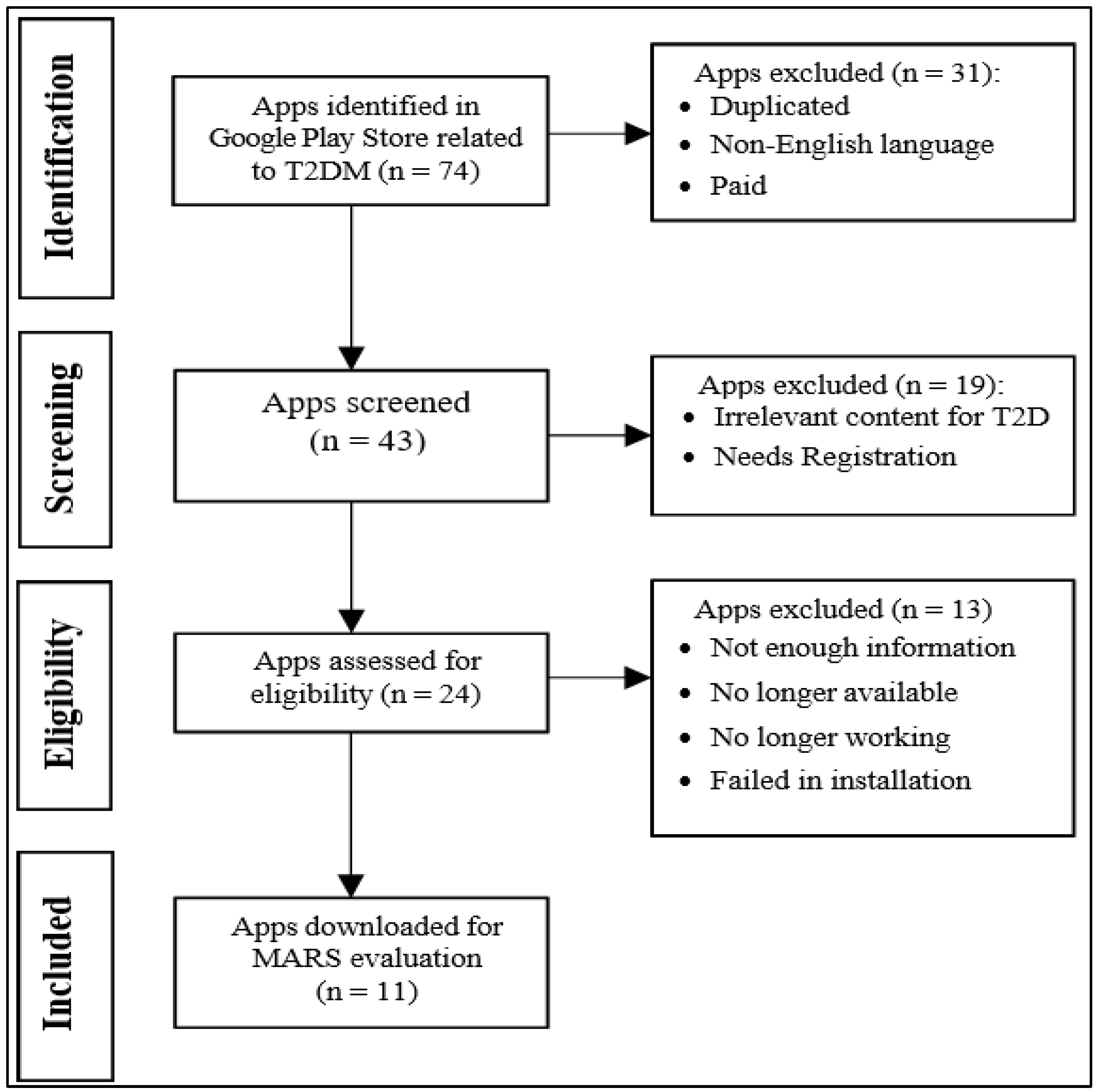
2.2. PRISMA for Search Strategy and Inclusion and Exclusion Criteria
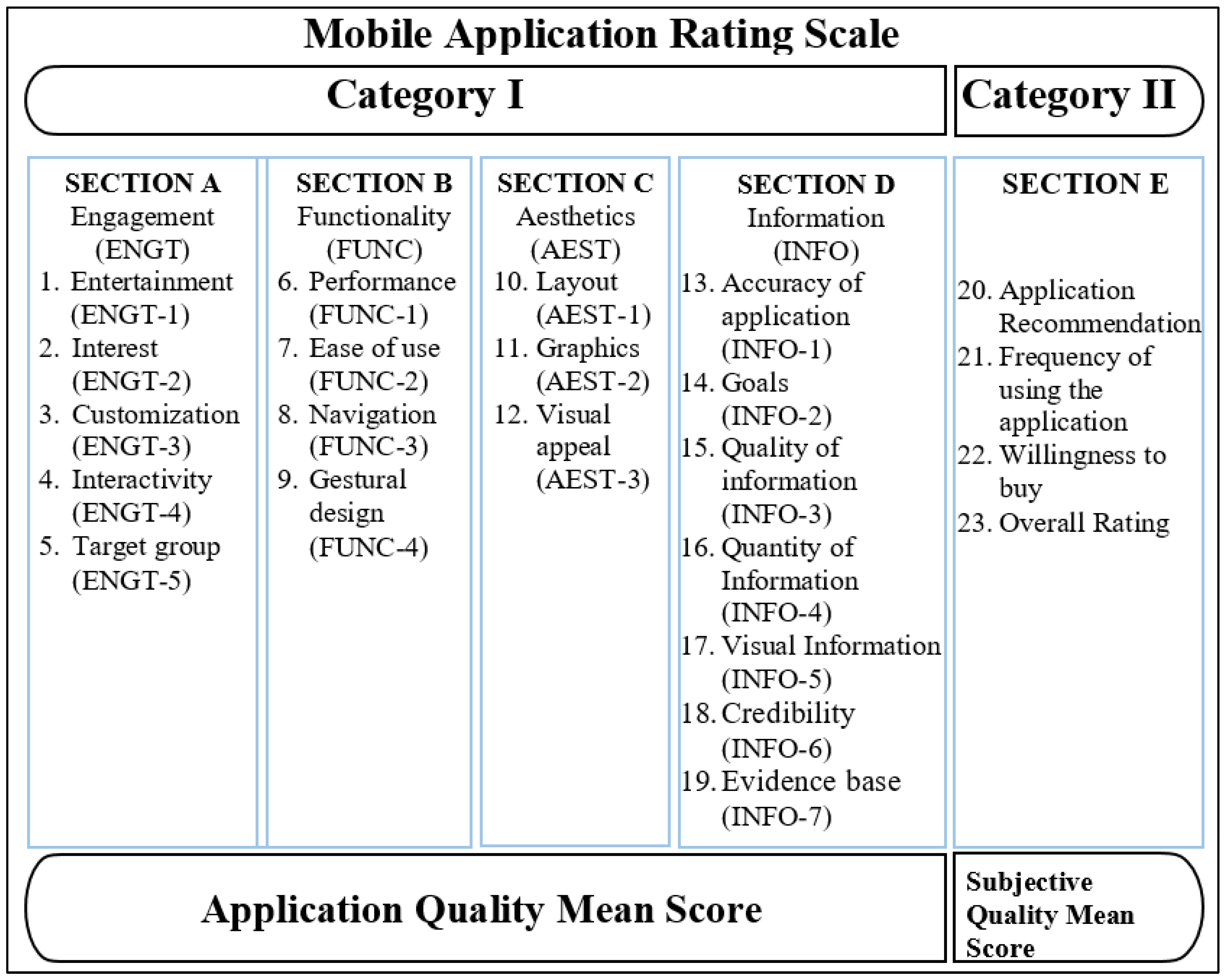
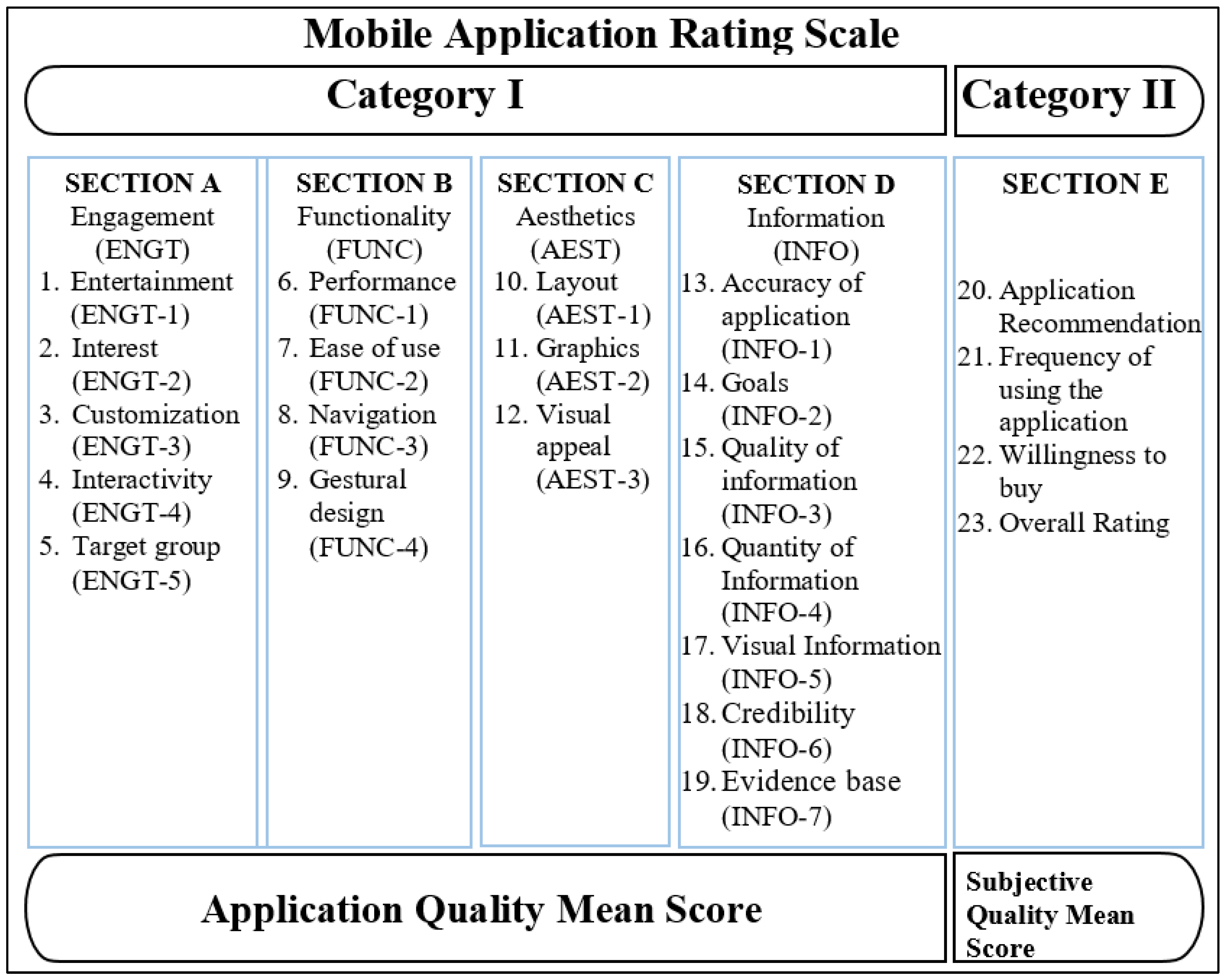
2.3. Mobile App Rating Scale (MARS)
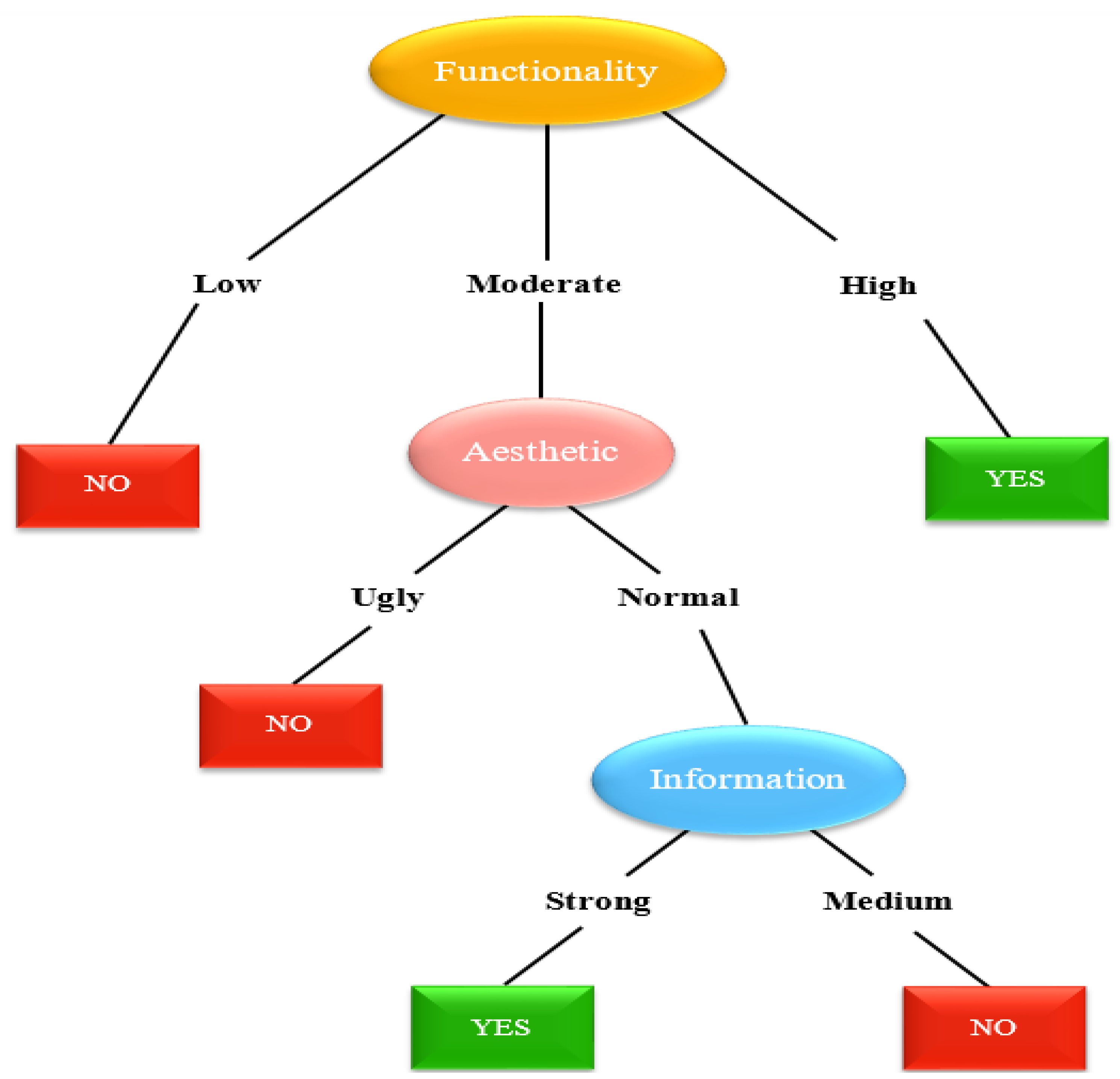
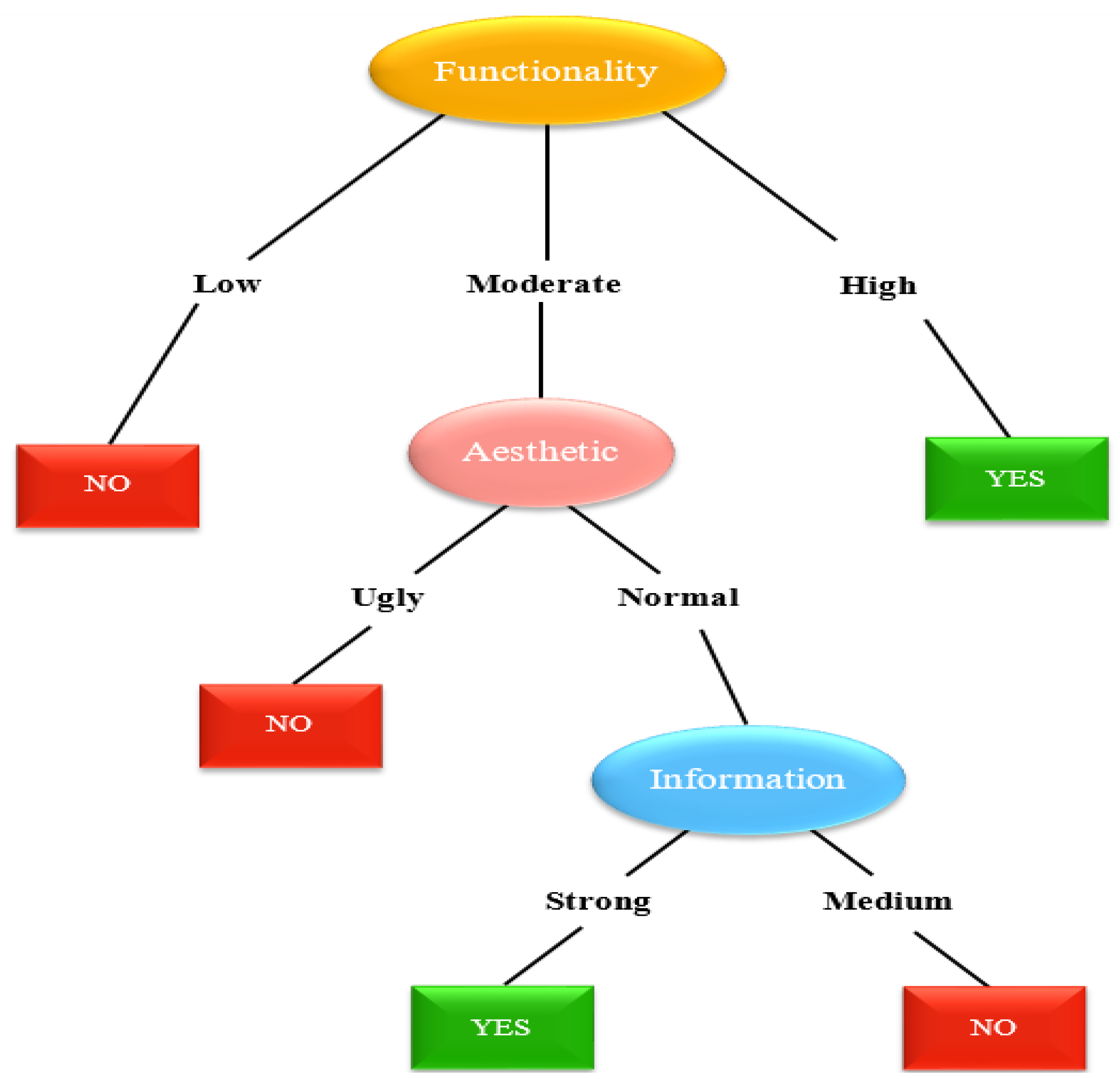
2.4. Decision Tree Classifier
2.5. ID3 Algorithm
- Determine each feature’s Information Gain.
- Divide dataset S into subsets utilizing the attribute that has the highest Information Gain, assuming that not all rows correspond with the similar class.
- Create a decision tree node with the feature that gives you the highest information.
- If all corresponds to the similar class, create the present node with a leaf node that has the class as its label.
- Continue until the decision tree is completely filled with leaf nodes or until you run out of attributes.
3. Literature Review
3.1. Review Works on MARS
3.2. Review Works on ID3 Algorithm
4. Implementation of MARS and ID3 Algorithm
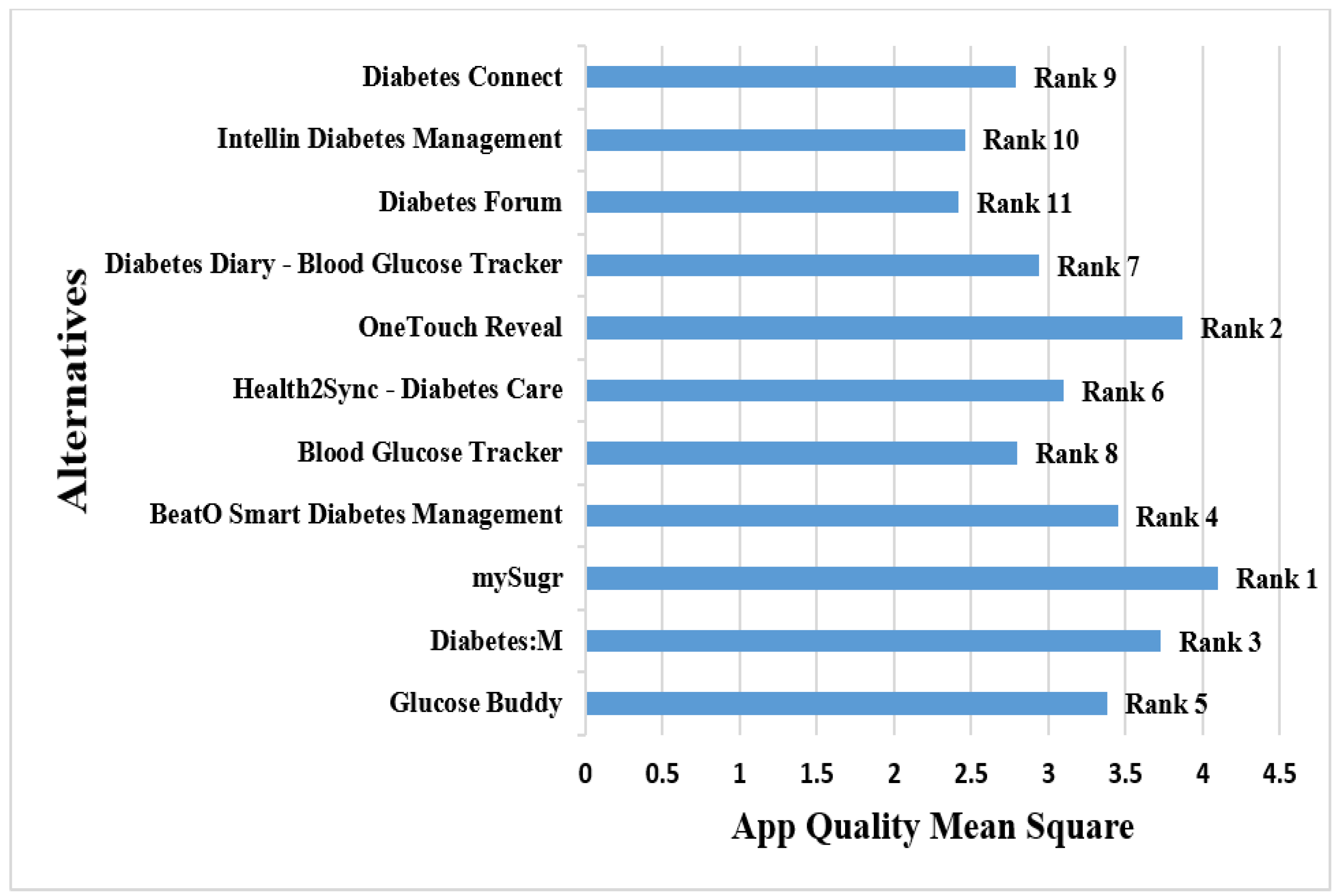
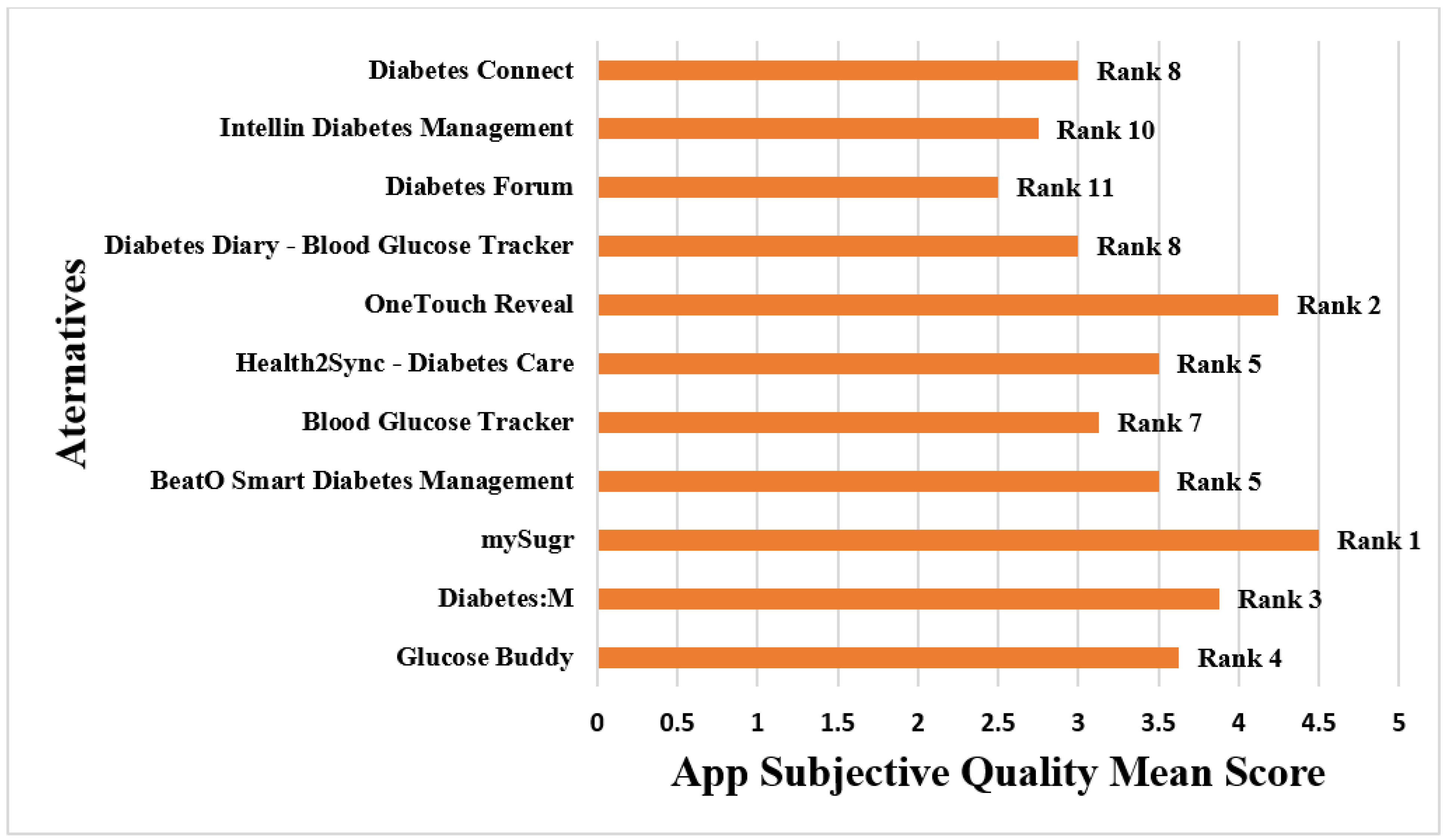
4.1. Ranking of mHealth Applications Based on Usability Using MARS
4.1.1. Search Strategy and Inclusion and Exclusion Criteria
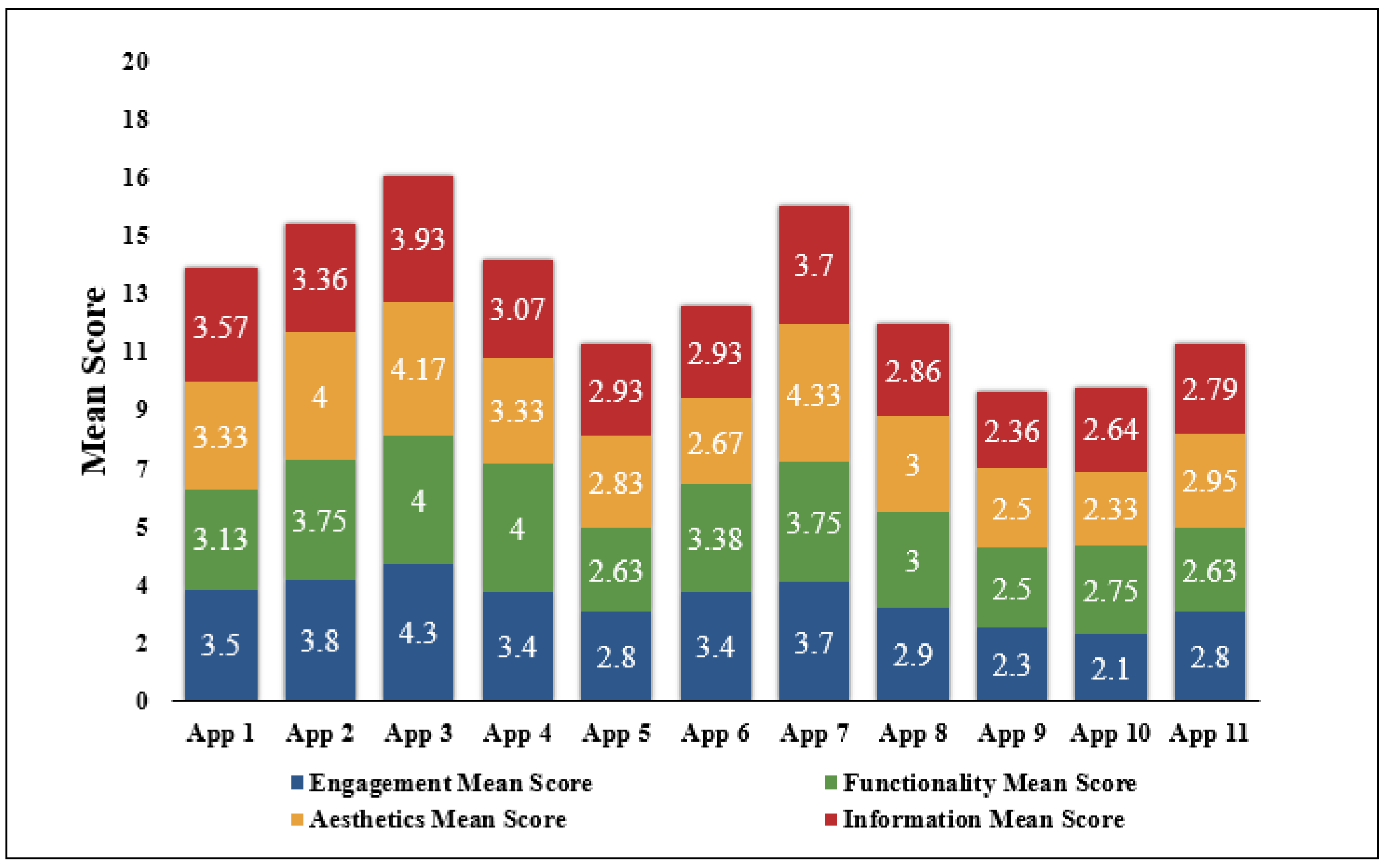
4.1.2. Quality Assessment of the Applications Using MARS
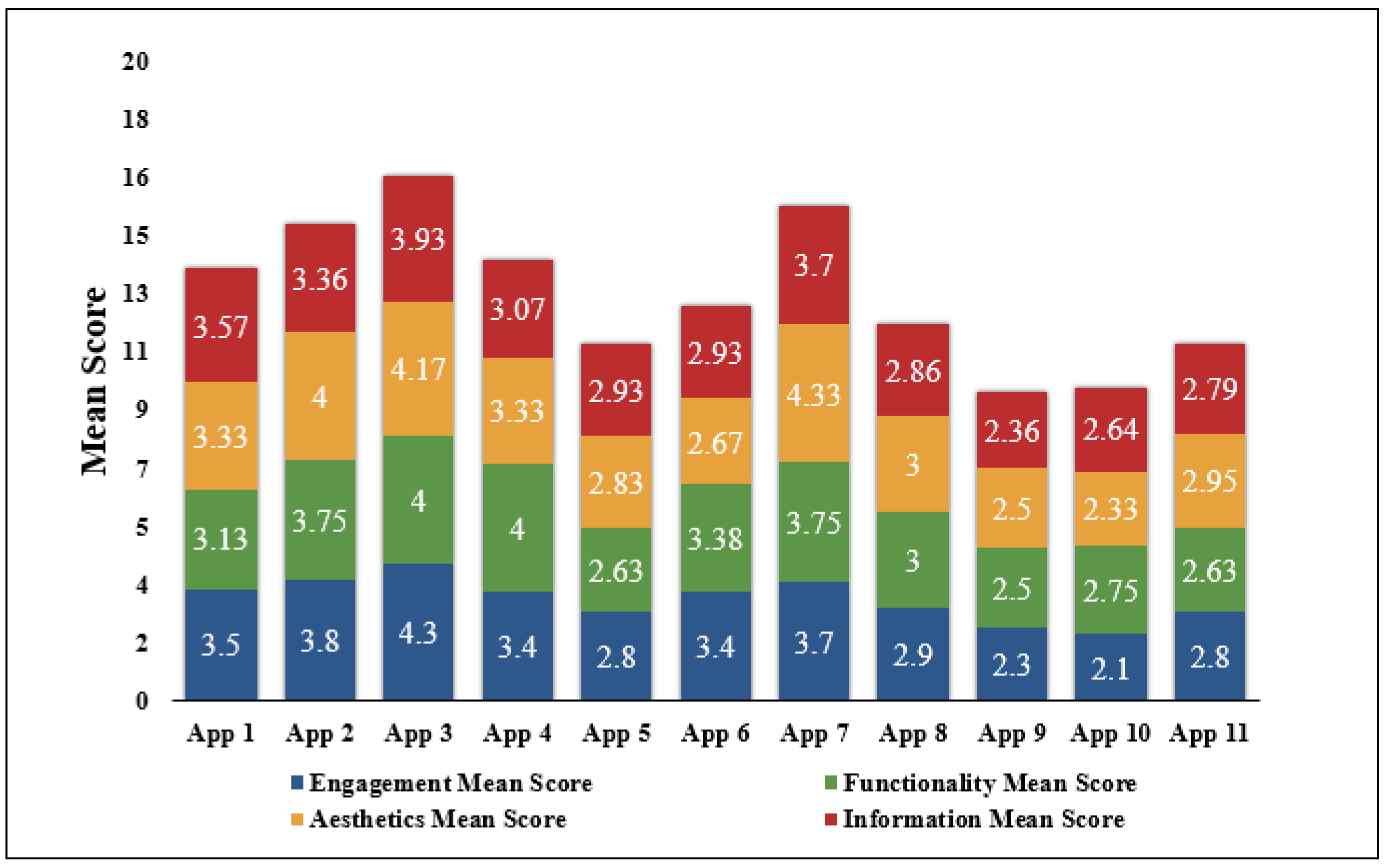
4.1.3. Data Analysis
4.2. Selection of mHealth Applications Based on Usability Using ID3 Algorithm
Feature Selection
- 1.
- Determination of the Entropy and Information Gain for the first attribute—Engagement
- 2.
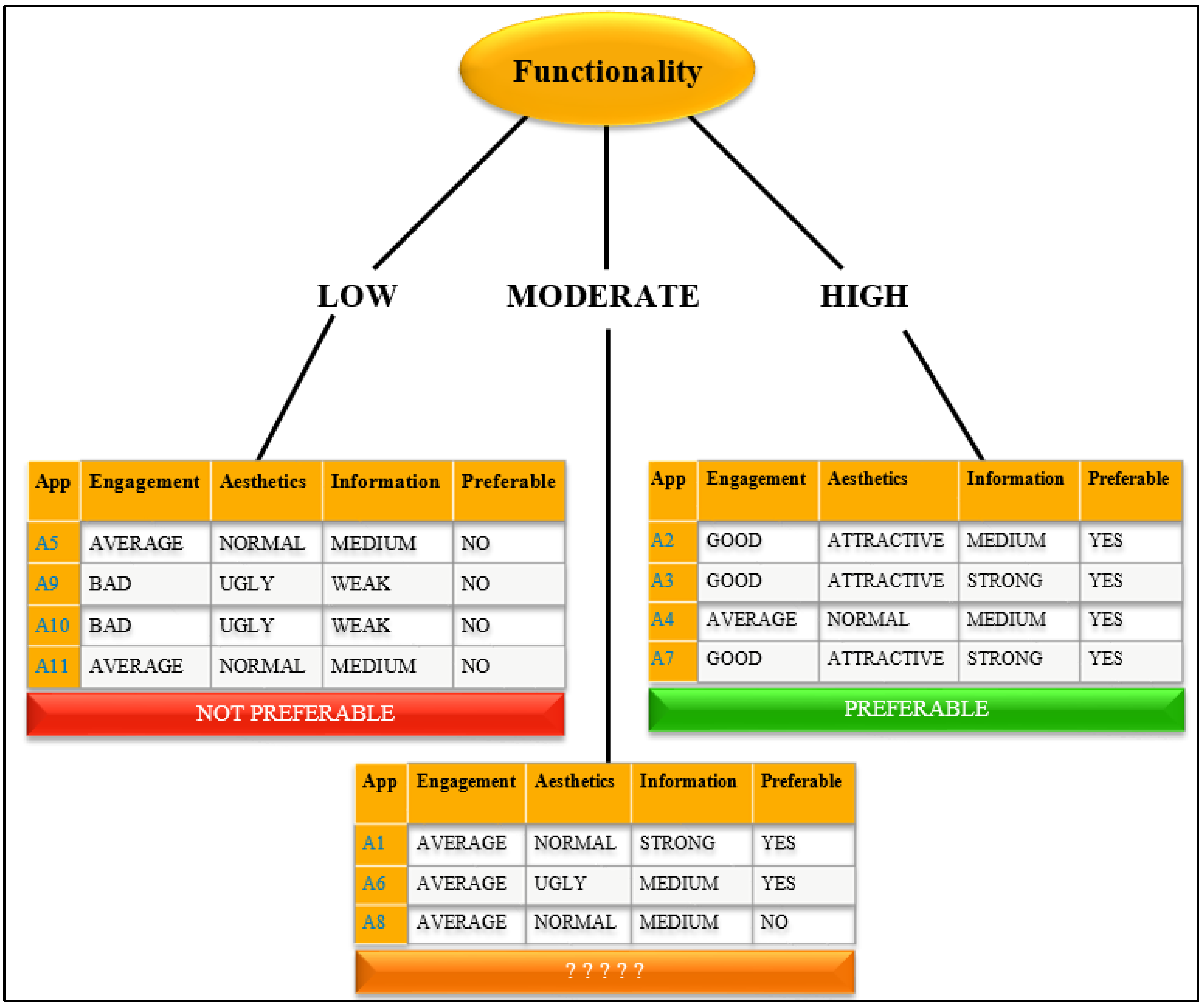
- Determination of the Entropy and Information Gain for the second attribute—Functionality
5. Results
5.1. Systematic Search and Screening
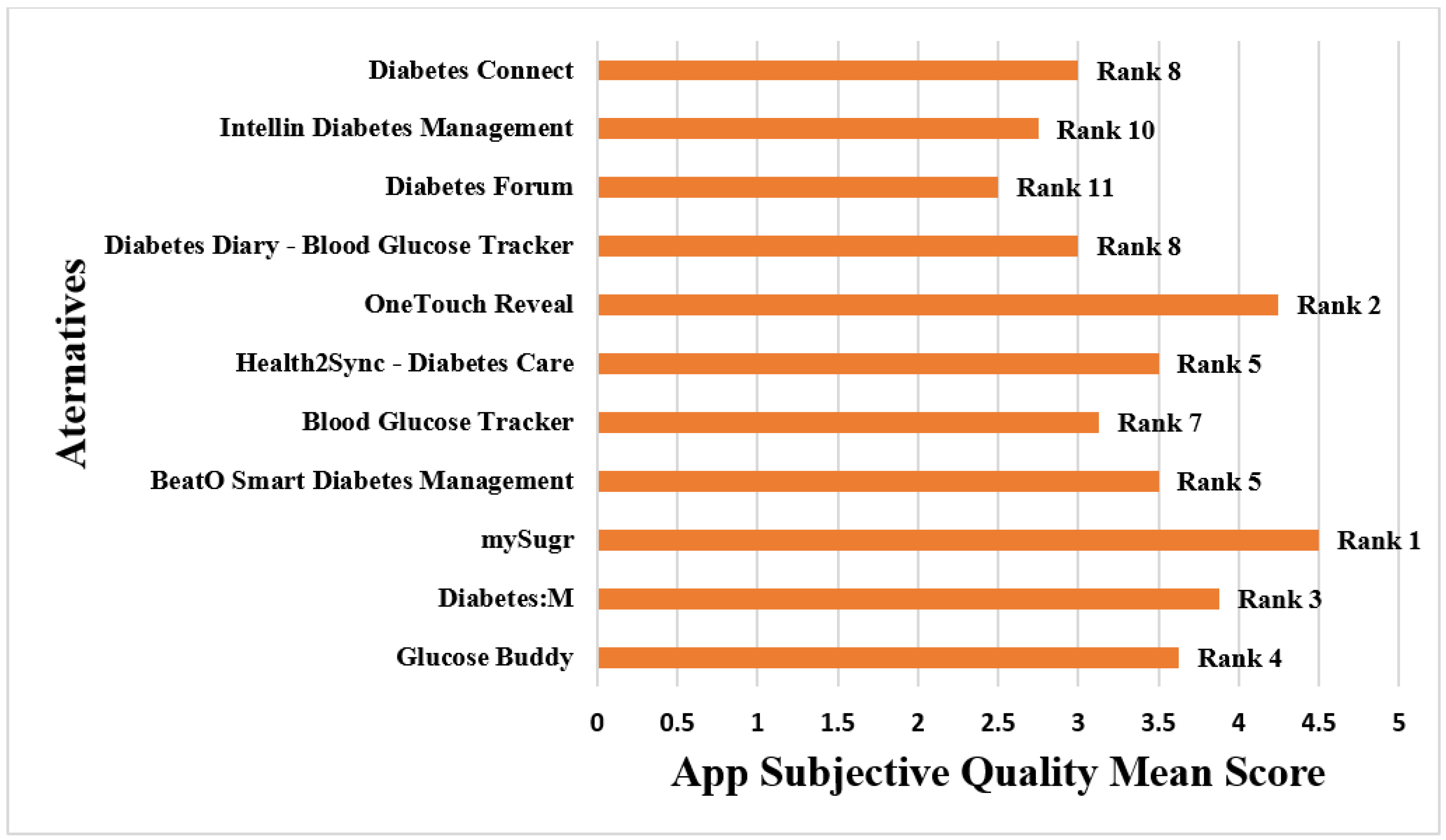
5.2. Results Based on MARS Rating
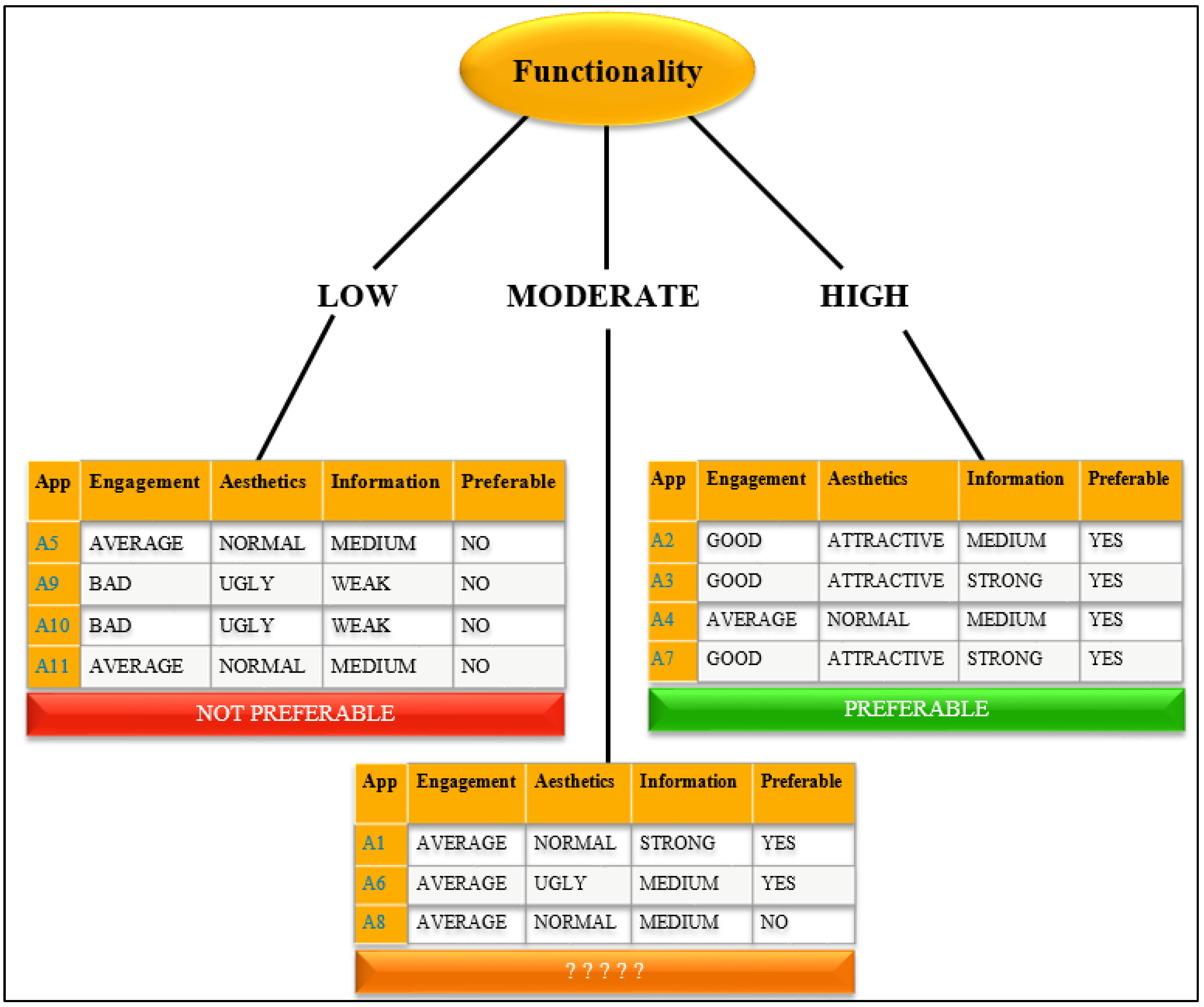
5.3. Results Based on ID3 Algorithm
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jusoh, S. A survey on trend, opportunities and challenges of mHealthapplications. Int. J. Interact. Mob. Technol. 2017, 11, 73–85. [Google Scholar] [CrossRef] [Green Version]
- Klasnja, P.; Pratt, W. Managing health with mobile technology. Interactions 2014, 21, 66–69. [Google Scholar] [CrossRef]
- Sittig, S.; Wang, J.; Iyengar, S.; Myneni, S.; Franklin, A. Incorporating Behavioral Trigger 478 Messages Into a Mobile Health App for Chronic Disease Management: Randomized Clinical Feasibility Trial in Diabetes. JMIR Mhealth Uhealth 2020, 8, e15927. [Google Scholar] [CrossRef] [Green Version]
- Kay, M.; Santos, J.; Takane, M.; World Health Organization. mHealth: New Horizons for Health Through Mobile Technologies. 2011. Available online: https://www.who.int/ehealth/mhealth_summit.pdf (accessed on 23 January 2020).
- Kitsiou, S.; Paré, G.; Jaana, M.; Gerber, B. Effectiveness of mHealth interventions for patients with diabetes: An overview of systematic reviews. PLoS ONE 2017, 12, e0173160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eng, D.S.; Lee, J.M. The promise and peril of mobile health applications for diabetes and endocrinology. Pediatric Diabetes 2013, 14, 231–238. [Google Scholar] [CrossRef] [Green Version]
- Milne-Ives, M.; Lam, C.; De Cock, C.; Van Velthoven, M.H.; Meinert, E. Mobile Applications for Health Behavior Change in Physical Activity, Diet, Drug and Alcohol Use, and Mental Health: Systematic Review. JMIR MhealthUhealth 2020, 8, e17046. [Google Scholar] [CrossRef] [PubMed]
- Grainger, R.; Townsley, H.; White, B.; Langlotz, T.; Taylor, W.J. Applications for People With Rheumatoid Arthritis to Monitor Their Disease Activity: A Review of Applications for Best Practice and Quality. JMIR Mhealth Uhealth 2017, 5, e7. [Google Scholar] [CrossRef] [Green Version]
- Subhi, Y.; Bube, S.H.; Bojsen, S.R.; Thomsen, A.S.S.; Konge, L. Expert involvement and adherence to medical evidence in medical mobile phone applications: A systematic review. JMIR Mhealth Uhealth 2015, 3, e79. [Google Scholar] [CrossRef]
- Stoyanov, S.R.; Hides, L.; Kavanagh, D.J.; Zelenko, O.; Tjondronegoro, D.; Mani, M. Mobile app rating scale: A new tool for assessing the quality of health mobile applications. JMIR MHealth UHealth 2015, 3, e3422. [Google Scholar] [CrossRef] [Green Version]
- Kalhori, S.R.N.; Hemmat, M.; Noori, T.; Heydarian, S.; Katigari, M.R. Quality Evaluation of English Mobile Applications for Gestational Diabetes: App Review using Mobile Application Rating Scale (MARS). Curr. Diabetes Rev. 2020, 17, 161–168. [Google Scholar] [CrossRef]
- Verma, A. Study and Evaluation of Classification Algorithms in Data Mining. Int. Res. J. Eng. Technol. 2018, 5, 1–11. [Google Scholar]
- Hutton, B.; Catalá-López, F.; Moher, D. La extensión de la declaración PRISMA para revisions sistemáticas que incorporan metaanálisis en red: PRISMA-NMA. Med. Clin. 2016, 147, 262–266. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoyanov, S.R.; Hides, L.; Kavanagh, D.J.; Wilson, H. Development and Validation of the User Version of the Mobile Application Rating Scale (uMARS). JMIR MhealthUhealth 2016, 4, e72. [Google Scholar] [CrossRef] [Green Version]
- Shrivastava, A.; Choudhary, V. Comparison between ID3 andC4.5 in Contrast to IDS SurbhiHardikar. VSRD-IJCSIT 2012, 2, 659–667. [Google Scholar]
- Han, J.; Kamber, M. Data Mining Concepts and Techniques, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2012. [Google Scholar] [CrossRef]
- Decision Trees: ID3 Algorithm Explained. 2020. Available online: https://towardsdatascience.com/decision-trees-for-classification-id3-algorithm-explained-89df76e72df1 (accessed on 11 December 2021).
- Quinlan, J.R. Induction of Decision Trees. Mach. Learn. 1986, 1, 81–106. [Google Scholar] [CrossRef] [Green Version]
- Gong, E.; Zhang, Z.; Jin, X.; Liu, Y.; Zhong, L.; Wu, Y.; Zhong, X.; Yan, L.L.; Oldenburg, B. Quality, functionality, and features of Chinese mobile applications for diabetes self-management: Systematic search and evaluation of mobile applications. JMIR MHealth UHealth 2020, 8, e14836. [Google Scholar] [CrossRef]
- Stec, M.A.; Arbour, M.W.; Hines, H.F. Client-Centered Mobile Health Care Applications: Using the Mobile Application Rating Scale Instrument for Evidence-Based Evaluation. J. Midwifery Women’s Health 2019, 3, 324–329. [Google Scholar] [CrossRef]
- Escriche-Escuder, A.; De-Torres, I.; Roldán-Jiménez, C.; Martín-Martín, J.; Muro-Culebras, A.; González-Sánchez, M.; Ruiz-Muñoz, M.; Mayoral-Cleries, F.; Biró, A.; Tang, W.; et al. Assessment of the quality of mobile applications (Applications) for management of low back pain using the mobile app rating scale (mars). Int. J. Environ. Res. Public Health 2020, 17, 9209. [Google Scholar] [CrossRef]
- Bardus, M.; van Beurden, S.B.; Smith, J.R.; Abraham, C. A review and content analysis of engagement, functionality, aesthetics, information quality, and change techniques in the most popular commercial applications for weight management. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 3–9. [Google Scholar] [CrossRef] [Green Version]
- Salazar, A.; de Sola, H.; Failde, I.; Moral-Munoz, J.A. Measuring the quality of mobile applications for the management of pain: Systematic search and evaluation using the mobile app rating scale. JMIR MHealth UHealth 2018, 6, e10718. [Google Scholar] [CrossRef]
- Salehinejad, S.; NiakanKalhori, S.R.; HajesmaeelGohari, S.; Bahaadinbeigy, K.; Fatehi, F. A review and content analysis of national applications for COVID-19 management using Mobile Application Rating Scale (MARS). Inform. Health Soc. Care 2021, 46, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Knitza, J.; Tascilar, K.; Messner, E.M.; Meyer, M.; Vossen, D.; Pulla, A.; Bosch, P.; Kittler, J.; Kleyer, A.; Sewerin, P.; et al. German mobile applications in rheumatology: Review and analysis using the mobile application rating scale (MARS). JMIR MHealth UHealth 2019, 7, e14991. [Google Scholar] [CrossRef]
- Sullivan, R.K.; Marsh, S.; Halvarsson, J.; Holdsworth, M.; Waterlander, W.; Poelman, M.P.; Salmond, J.A.; Christian, H.; Koh, L.S.C.; Cade, J.E.; et al. Smartphone applications for measuring human health and climate change co-benefits: A comparison and quality rating of available applications. JMIR MHealth UHealth 2016, 4, e5931. [Google Scholar] [CrossRef]
- Santo, K.; Richtering, S.S.; Chalmers, J.; Thiagalingam, A.; Chow, C.K.; Redfern, J. Mobile phone applications to improve medication adherence: A systematic stepwise process to identify high-quality applications. JMIR MHealth UHealth 2016, 4, e6742. [Google Scholar] [CrossRef] [PubMed]
- Creber, R.M.M.; Maurer, M.S.; Reading, M.; Hiraldo, G.; Hickey, K.T.; Iribarren, S. Review and analysis of existing mobile phone applications to support heart failure symptom monitoring and self-care management using the mobile application rating scale (MARS). JMIR MHealth UHealth 2016, 4, e5882. [Google Scholar] [CrossRef]
- Larco, A.; Enriquez, F.; Lujan-Mora, S. Review and evaluation of special education iOSapplications using MARS. In Proceedings of the EDUNINE 2018—2nd IEEE World Engineering Education Conference: The Role of Professional Associations in Contemporaneous Engineer Careers, Buenos Aires, Argentina, 11–14 March 2018. [Google Scholar] [CrossRef]
- Moseley, I.; Roy, A.; Deluty, A.; Brewer, J.A. Evaluating the Quality of Smartphone Applications for Overeating, Stress, and Craving-Related Eating Using the Mobile Application Rating Scale. Curr. Addict. Rep. 2020, 7, 260–267. [Google Scholar] [CrossRef]
- Kale, A.; Auti, N. Automated Menu Planning Algorithm for Children: Food Recommendation by Dietary Management System using ID3 for Indian Food Database. In Procedia Computer Science; Elsevier: Amsterdam, The Netherlands, 2015; Volume 50, pp. 197–202. [Google Scholar]
- Aalagadda, V.; Latha, I.M. Identifying Dropout Students using ID3 Decision Tree Algorithm. Int. J. Sci. Res. Dev. 2019, 7, 1203–1206. [Google Scholar]
- Prasanthi, L.S.; Kumar, R.K. ID3 and Its Applications in Generation of Decision Trees across Various Domains-Survey. Int. J. Comput. Sci. Inf. Technol. 2015, 6, 5353–5357. [Google Scholar]
- Adhatrao, K.; Gaykar, A.; Dhawan, A.; Jha, R.; Honrao, V. Predicting Students’ Performance Using ID3 and C4.5 Classification Algorithms. arXiv 2013, arXiv:1310.2071. [Google Scholar] [CrossRef]
- Zhang, H.; Zhou, R. The analysis and optimization of decision tree based on ID3 algorithm. In Proceedings of the 2017 9th International Conference On Modelling, Identification and Control, ICMIC 2017, Kunming, China, 10–12 July 2017. [Google Scholar] [CrossRef]
- Hazra, S.; Technologies, I.; Sanyal, S. Recruitment Prediction Using Id3 Decision Tree. Int. J. Adv. Eng. Res. Dev. 2016, 3. [Google Scholar] [CrossRef]
- Gupta, K.; Roy, S.; Poonia, R.C.; Nayak, S.R.; Kumar, R.; Alzahrani, K.J.; Alnfiai, M.M.; Al-Wesabi, F.N. Evaluating the Usability of mHealth Applications on Type 2 Diabetes Mellitus Using Various MCDM Methods. Healthcare 2022, 10, 4. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.; Roy, S.; Poonia, R.C.; Kumar, R.; Alzahrani, K.J.; Altameem, A.; Saudagar, A.K.J. Multi-Criteria Usability Evaluation of mHealth Applications on Type 2 Diabetes Mellitus Using Two Hybrid MCDM Models: CODAS-FAHP and MOORA-FAHP. Appl. Sci. 2022, 12, 9. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Application No. | Application Name |
|---|---|
| App 1 | Glucose Buddy |
| App 2 | Diabetes:M |
| App 3 | mySugr |
| App 4 | BeatO Smart Diabetes Management |
| App 5 | Blood Glucose Tracker |
| App 6 | Health2Sync-Diabetes Care |
| App 7 | OneTouch Reveal |
| App 8 | Diabetes Diary-Blood Glucose Tracker |
| App 9 | Diabetes Forum |
| App 10 | Intellin Diabetes Management |
| App 11 | Diabetes Connect |
| Application Name | Attributes | Sub-Attributes | Reviewer 1 | Reviewer 2 | Mean | Standard Deviation | Application Quality Score |
|---|---|---|---|---|---|---|---|
| App 1 (Glucose Buddy) | ENGT | ENGT-1 | 4 | 3 | 3.5 | 0.53 | 3.38 |
| ENGT-2 | 4 | 3 | |||||
| ENGT-3 | 3 | 4 | |||||
| ENGT-4 | 3 | 4 | |||||
| ENGT-5 | 4 | 3 | |||||
| FUNT | FUNT-1 | 3 | 3 | 3.13 | 0.64 | ||
| FUNT-2 | 3 | 4 | |||||
| FUNT-3 | 4 | 3 | |||||
| FUNT-4 | 2 | 3 | |||||
| AEST | AEST-1 | 4 | 4 | 3.33 | 0.82 | ||
| AEST-2 | 4 | 2 | |||||
| AEST-3 | 3 | 3 | |||||
| INFN | INFN-1 | 3 | 4 | 3.57 | 0.76 | ||
| INFN-2 | 4 | 3 | |||||
| INFN-3 | 3 | 4 | |||||
| INFN-4 | 4 | 5 | |||||
| INFN-5 | 4 | 3 | |||||
| INFN-6 | 3 | 2 | |||||
| INFN-7 | 4 | 4 | |||||
| App 2 (Diabetes:M) | ENGT | ENGT-1 | 4 | 4 | 3.8 | 0.63 | 3.73 |
| ENGT-2 | 3 | 3 | |||||
| ENGT-3 | 4 | 4 | |||||
| ENGT-4 | 4 | 3 | |||||
| ENGT-5 | 5 | 4 | |||||
| FUNT | FUNT-1 | 4 | 3 | 3.75 | 0.71 | ||
| FUNT-2 | 5 | 4 | |||||
| FUNT-3 | 4 | 3 | |||||
| FUNT-4 | 3 | 4 | |||||
| AEST | AEST-1 | 4 | 4 | 4.0 | 0.63 | ||
| AEST-2 | 4 | 5 | |||||
| AEST-3 | 3 | 4 | |||||
| INFN | INFN-1 | 3 | 5 | 3.36 | 0.74 | ||
| INFN-2 | 4 | 3 | |||||
| INFN-3 | 3 | 3 | |||||
| INFN-4 | 3 | 4 | |||||
| INFN-5 | 4 | 3 | |||||
| INFN-6 | 3 | 4 | |||||
| INFN-7 | 2 | 3 | |||||
| App 3 (mySugr) | ENGT | ENGT-1 | 4 | 5 | 4.3 | 0.67 | 4.1 |
| ENGT-2 | 5 | 4 | |||||
| ENGT-3 | 4 | 4 | |||||
| ENGT-4 | 5 | 3 | |||||
| ENGT-5 | 5 | 4 | |||||
| FUNT | FUNT-1 | 4 | 4 | 4 | 0.76 | ||
| FUNT-2 | 5 | 3 | |||||
| FUNT-3 | 4 | 4 | |||||
| FUNT-4 | 5 | 3 | |||||
| AEST | AEST-1 | 4 | 4 | 4.17 | 0.41 | ||
| AEST-2 | 5 | 4 | |||||
| AEST-3 | 4 | 4 | |||||
| INFN | INFN-1 | 5 | 5 | 3.93 | 0.73 | ||
| INFN-2 | 5 | 4 | |||||
| INFN-3 | 4 | 4 | |||||
| INFN-4 | 4 | 3 | |||||
| INFN-5 | 4 | 4 | |||||
| INFN-6 | 3 | 3 | |||||
| INFN-7 | 3 | 4 | |||||
| App 4 (BeatO Smart Diabetes Management) | ENGT | ENGT-1 | 4 | 3 | 3.4 | 0.7 | 3.45 |
| ENGT-2 | 3 | 3 | |||||
| ENGT-3 | 4 | 4 | |||||
| ENGT-4 | 2 | 4 | |||||
| ENGT-5 | 3 | 4 | |||||
| FUNT | FUNT-1 | 4 | 4 | 4 | 0.53 | ||
| FUNT-2 | 3 | 4 | |||||
| FUNT-3 | 4 | 4 | |||||
| FUNT-4 | 5 | 4 | |||||
| AEST | AEST-1 | 4 | 3 | 3.33 | 0.52 | ||
| AEST-2 | 4 | 3 | |||||
| AEST-3 | 3 | 3 | |||||
| INFN | INFN-1 | 4 | 3 | 3.07 | 0.73 | ||
| INFN-2 | 3 | 4 | |||||
| INFN-3 | 3 | 4 | |||||
| INFN-4 | 3 | 3 | |||||
| INFN-5 | 2 | 3 | |||||
| INFN-6 | 2 | 2 | |||||
| INFN-7 | 3 | 4 | |||||
| App 5 (Blood Glucose Tracker) | ENGT | ENGT-1 | 2 | 3 | 2.8 | 0.42 | 2.8 |
| ENGT-2 | 3 | 2 | |||||
| ENGT-3 | 3 | 3 | |||||
| ENGT-4 | 3 | 3 | |||||
| ENGT-5 | 3 | 3 | |||||
| FUNT | FUNT-1 | 3 | 2 | 2.63 | 0.74 | ||
| FUNT-2 | 3 | 4 | |||||
| FUNT-3 | 2 | 2 | |||||
| FUNT-4 | 3 | 2 | |||||
| AEST | AEST-1 | 3 | 3 | 2.83 | 0.41 | ||
| AEST-2 | 3 | 2 | |||||
| AEST-3 | 3 | 3 | |||||
| INFN | INFN-1 | 3 | 2 | 2.93 | 0.62 | ||
| INFN-2 | 3 | 3 | |||||
| INFN-3 | 4 | 3 | |||||
| INFN-4 | 3 | 4 | |||||
| INFN-5 | 3 | 2 | |||||
| INFN-6 | 2 | 3 | |||||
| INFN-7 | 3 | 3 | |||||
| App 6 (Health2Sync-Diabetes Care) | ENGT | ENGT-1 | 4 | 5 | 3.4 | 0.84 | 3.1 |
| ENGT-2 | 4 | 3 | |||||
| ENGT-3 | 2 | 3 | |||||
| ENGT-4 | 3 | 4 | |||||
| ENGT-5 | 3 | 3 | |||||
| FUNT | FUNT-1 | 3 | 4 | 3.38 | 0.74 | ||
| FUNT-2 | 4 | 3 | |||||
| FUNT-3 | 3 | 4 | |||||
| FUNT-4 | 2 | 4 | |||||
| AEST | AEST-1 | 3 | 3 | 2.67 | 0.52 | ||
| AEST-2 | 2 | 2 | |||||
| AEST-3 | 3 | 3 | |||||
| INFN | INFN-1 | 2 | 3 | 2.93 | 0.73 | ||
| INFN-2 | 3 | 3 | |||||
| INFN-3 | 3 | 4 | |||||
| INFN-4 | 3 | 4 | |||||
| INFN-5 | 2 | 4 | |||||
| INFN-6 | 2 | 3 | |||||
| INFN-7 | 2 | 3 | |||||
| App 7 (OneTouch Reveal) | ENGT | ENGT-1 | 4 | 4 | 3.7 | 0.82 | 3.87 |
| ENGT-2 | 5 | 5 | |||||
| ENGT-3 | 4 | 3 | |||||
| ENGT-4 | 3 | 3 | |||||
| ENGT-5 | 3 | 3 | |||||
| FUNT | FUNT-1 | 4 | 5 | 3.75 | 0.71 | ||
| FUNT-2 | 4 | 3 | |||||
| FUNT-3 | 3 | 4 | |||||
| FUNT-4 | 3 | 4 | |||||
| AEST | AEST-1 | 4 | 5 | 4.33 | 0.82 | ||
| AEST-2 | 5 | 4 | |||||
| AEST-3 | 3 | 5 | |||||
| INFN | INFN-1 | 3 | 4 | 3.7 | 0.61 | ||
| INFN-2 | 3 | 5 | |||||
| INFN-3 | 4 | 4 | |||||
| INFN-4 | 3 | 4 | |||||
| INFN-5 | 4 | 3 | |||||
| INFN-6 | 3 | 4 | |||||
| INFN-7 | 4 | 4 | |||||
| App 8 (Diabetes Diary-Blood Glucose Tracker) | ENGT | ENGT-1 | 3 | 4 | 2.9 | 0.74 | 2.94 |
| ENGT-2 | 3 | 2 | |||||
| ENGT-3 | 3 | 2 | |||||
| ENGT-4 | 3 | 3 | |||||
| ENGT-5 | 4 | 2 | |||||
| FUNT | FUNT-1 | 3 | 3 | 3 | 0.53 | ||
| FUNT-2 | 3 | 4 | |||||
| FUNT-3 | 3 | 3 | |||||
| FUNT-4 | 2 | 3 | |||||
| AEST | AEST-1 | 2 | 3 | 3 | 0.63 | ||
| AEST-2 | 3 | 4 | |||||
| AEST-3 | 3 | 3 | |||||
| INFN | INFN-1 | 4 | 3 | 2.86 | 0.66 | ||
| INFN-2 | 4 | 3 | |||||
| INFN-3 | 3 | 3 | |||||
| INFN-4 | 2 | 3 | |||||
| INFN-5 | 3 | 3 | |||||
| INFN-6 | 2 | 2 | |||||
| INFN-7 | 2 | 3 | |||||
| App 9 (Diabetes Forum) | ENGT | ENGT-1 | 2 | 3 | 2.3 | 0.67 | 2.42 |
| ENGT-2 | 3 | 3 | |||||
| ENGT-3 | 2 | 2 | |||||
| ENGT-4 | 2 | 1 | |||||
| ENGT-5 | 2 | 3 | |||||
| FUNT | FUNT-1 | 2 | 3 | 2.5 | 0.53 | ||
| FUNT-2 | 2 | 2 | |||||
| FUNT-3 | 3 | 2 | |||||
| FUNT-4 | 3 | 3 | |||||
| AEST | AEST-1 | 2 | 3 | 2.5 | 0.55 | ||
| AEST-2 | 3 | 2 | |||||
| AEST-3 | 2 | 3 | |||||
| INFN | INFN-1 | 3 | 2 | 2.36 | 0.63 | ||
| INFN-2 | 2 | 3 | |||||
| INFN-3 | 3 | 3 | |||||
| INFN-4 | 2 | 3 | |||||
| INFN-5 | 3 | 2 | |||||
| INFN-6 | 2 | 1 | |||||
| INFN-7 | 2 | 2 | |||||
| App 10 (Intellin Diabetes Management) | ENGT | ENGT-1 | 2 | 3 | 2.1 | 0.57 | 2.46 |
| ENGT-2 | 2 | 2 | |||||
| ENGT-3 | 1 | 2 | |||||
| ENGT-4 | 3 | 2 | |||||
| ENGT-5 | 2 | 2 | |||||
| FUNT | FUNT-1 | 3 | 3 | 2.75 | 0.46 | ||
| FUNT-2 | 2 | 3 | |||||
| FUNT-3 | 3 | 2 | |||||
| FUNT-4 | 3 | 3 | |||||
| AEST | AEST-1 | 2 | 3 | 2.33 | 0.52 | ||
| AEST-2 | 2 | 2 | |||||
| AEST-3 | 2 | 3 | |||||
| INFN | INFN-1 | 3 | 2 | 2.64 | 0.5 | ||
| INFN-2 | 3 | 2 | |||||
| INFN-3 | 3 | 3 | |||||
| INFN-4 | 2 | 3 | |||||
| INFN-5 | 3 | 2 | |||||
| INFN-6 | 3 | 2 | |||||
| INFN-7 | 3 | 3 | |||||
| App 11 (Diabetes Connect) | ENGT | ENGT-1 | 3 | 2 | 2.8 | 0.63 | 2.79 |
| ENGT-2 | 3 | 4 | |||||
| ENGT-3 | 2 | 3 | |||||
| ENGT-4 | 2 | 3 | |||||
| ENGT-5 | 3 | 3 | |||||
| FUNT | FUNT-1 | 2 | 3 | 2.63 | 0.52 | ||
| FUNT-2 | 3 | 3 | |||||
| FUNT-3 | 2 | 3 | |||||
| FUNT-4 | 3 | 2 | |||||
| AEST | AEST-1 | 3 | 4 | 2.95 | 0.52 | ||
| AEST-2 | 3 | 4 | |||||
| AEST-3 | 3 | 3 | |||||
| INFN | INFN-1 | 3 | 2 | 2.79 | 0.7 | ||
| INFN-2 | 3 | 3 | |||||
| INFN-3 | 2 | 2 | |||||
| INFN-4 | 3 | 4 | |||||
| INFN-5 | 3 | 4 | |||||
| INFN-6 | 2 | 3 | |||||
| INFN-7 | 2 | 3 |
| Application Name | Parameters | Reviewer 1 | Reviewer 2 | Mean Score |
|---|---|---|---|---|
| App 1 (Glucose Buddy) | App Recommendation | 3 | 5 | 3.63 |
| Frequency of using the app | 4 | 4 | ||
| Willingness to buy | 4 | 3 | ||
| Overall Rating | 3 | 3 | ||
| App 2 (Diabetes:M) | App Recommendation | 3 | 4 | 3.88 |
| Frequency of using the app | 4 | 4 | ||
| Willingness to buy | 4 | 3 | ||
| Overall Rating | 5 | 4 | ||
| App 3 (mySugr) | App Recommendation | 4 | 5 | 4.5 |
| Frequency of using the app | 5 | 4 | ||
| Willingness to buy | 4 | 5 | ||
| Overall Rating | 4 | 5 | ||
| App 4 (BeatO Smart Diabetes Management) | App Recommendation | 4 | 3 | 3.5 |
| Frequency of using the app | 4 | 3 | ||
| Willingness to buy | 4 | 3 | ||
| Overall Rating | 4 | 3 | ||
| App 5 (Blood Glucose Tracker) | App Recommendation | 3 | 3 | 3.13 |
| Frequency of using the app | 3 | 3 | ||
| Willingness to buy | 3 | 4 | ||
| Overall Rating | 3 | 3 | ||
| App 6 (Health2Sync-Diabetes Care) | App Recommendation | 3 | 4 | 3.5 |
| Frequency of using the app | 3 | 4 | ||
| Willingness to buy | 4 | 3 | ||
| Overall Rating | 3 | 4 | ||
| App 7 (OneTouch Reveal) | App Recommendation | 4 | 5 | 4.25 |
| Frequency of using the app | 5 | 4 | ||
| Willingness to buy | 4 | 4 | ||
| Overall Rating | 4 | 4 | ||
| App 8 (Diabetes Diary-Blood Glucose Tracker) | App Recommendation | 3 | 4 | 3 |
| Frequency of using the app | 3 | 4 | ||
| Willingness to buy | 2 | 3 | ||
| Overall Rating | 3 | 2 | ||
| App 9 (Diabetes Forum) | App Recommendation | 2 | 3 | 2.5 |
| Frequency of using the app | 3 | 2 | ||
| Willingness to buy | 2 | 4 | ||
| Overall Rating | 2 | 2 | ||
| App 10 (Intellin Diabetes Management) | App Recommendation | 4 | 3 | 2.75 |
| Frequency of using the app | 2 | 3 | ||
| Willingness to buy | 3 | 2 | ||
| Overall Rating | 3 | 2 | ||
| App 11 (Diabetes Connect) | App Recommendation | 3 | 3 | 3 |
| Frequency of using the app | 4 | 3 | ||
| Willingness to buy | 3 | 2 | ||
| Overall Rating | 3 | 3 |
| Attributes | Values | Mean Score Range |
|---|---|---|
| Engagement (ENGT) | Bad | ≤2.75 |
| Average | >2.75 & ≤3.5 | |
| Good | >3.5 | |
| Functionality (FUNT) | Low | ≤2.75 |
| Moderate | >2.75 & ≤3.5 | |
| High | >3.5 | |
| Aesthetics (AEST) | Ugly | ≤2.75 |
| Normal | >2.75 & ≤3.5 | |
| Attractive | >3.5 | |
| Information (INFN) | Weak | ≤2.75 |
| Medium | >2.75 & ≤3.5 | |
| Strong | >3.5 |
| Application | Engagement | Functionality | Aesthetics | Information | Application Selection |
|---|---|---|---|---|---|
| A1 | Average | Moderate | Normal | Strong | YES |
| A2 | Good | High | Attractive | Medium | YES |
| A3 | Good | High | Attractive | Strong | YES |
| A4 | Average | High | Normal | Medium | YES |
| A5 | Average | Low | Normal | Medium | NO |
| A6 | Average | Moderate | Ugly | Medium | YES |
| A7 | Good | High | Attractive | Strong | YES |
| A8 | Average | Moderate | Normal | Medium | NO |
| A9 | Bad | Low | Ugly | Weak | NO |
| A10 | Bad | Low | Ugly | Weak | NO |
| A11 | Average | Low | Normal | Medium | NO |
| App 1 | App 2 | App 3 | App 4 | App 5 | App 6 | App 7 | App 8 | App 9 | App 10 | App 11 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ratings in Google Play Store | 4.4 | 4.3 | 4.3 | 4.2 | 4.5 | 4.7 | 3.8 | 4.5 | 4.4 | 3.9 | 4.2 |
| Number of users | 14,540 | 21,475 | 63,207 | 19,050 | 19,233 | 13,050 | 29,436 | 2101 | 888 | 555 | 4768 |
| Engagement | 3.5 | 3.8 | 4.3 | 3.4 | 2.8 | 3.4 | 3.7 | 2.9 | 2.3 | 2.1 | 2.8 |
| Functionality | 3.13 | 3.75 | 4 | 4 | 2.63 | 3.38 | 3.75 | 3 | 2.5 | 2.75 | 2.63 |
| Aesthetics | 3.33 | 4 | 4.17 | 3.33 | 2.83 | 2.67 | 4.33 | 3 | 2.5 | 2.33 | 2.95 |
| Information | 3.57 | 3.36 | 3.93 | 3.07 | 2.93 | 2.93 | 3.7 | 2.86 | 2.36 | 2.64 | 2.79 |
| App Subjective Quality Mean Score | 3.63 | 3.88 | 4.5 | 3.5 | 3.13 | 3.5 | 4.25 | 3 | 2.5 | 2.75 | 3 |
| App Quality Mean Score | 3.38 | 3.73 | 4.1 | 3.45 | 2.8 | 3.1 | 3.87 | 2.94 | 2.42 | 2.46 | 2.79 |
| Ratings in Google Play Store | Number of Users | Engagement | Functionality | Aesthetics | Information | Application Subjective Quality Mean Score | Application Quality Mean Square | |
|---|---|---|---|---|---|---|---|---|
| Ratings in Google Play Store | 1 | |||||||
| Number of users | −0.097 | 1 | ||||||
| Engagement | 0.05 | 0.83 | 1 | |||||
| Functionality | −0.18 | 0.72 | 0.87 | 1 | ||||
| Aesthetics | −0.33 | 0.78 | 0.88 | 0.79 | 1 | |||
| Information | −0.21 | 0.84 | 0.91 | 0.76 | 0.90 | 1 | ||
| Application Subjective Quality Mean Score | −0.18 | 0.88 | 0.96 | 0.86 | 0.91 | 0.96 | 1 | |
| Application Quality Mean Square | −0.17 | 0.84 | 0.97 | 0.91 | 0.95 | 0.94 | 0.98 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gupta, K.; Roy, S.; Altameem, A.; Kumar, R.; Saudagar, A.K.J.; Poonia, R.C. Usability Evaluation and Classification of mHealth Applications for Type 2 Diabetes Mellitus Using MARS and ID3 Algorithm. Int. J. Environ. Res. Public Health 2022, 19, 6999. https://doi.org/10.3390/ijerph19126999
Gupta K, Roy S, Altameem A, Kumar R, Saudagar AKJ, Poonia RC. Usability Evaluation and Classification of mHealth Applications for Type 2 Diabetes Mellitus Using MARS and ID3 Algorithm. International Journal of Environmental Research and Public Health. 2022; 19(12):6999. https://doi.org/10.3390/ijerph19126999
Chicago/Turabian StyleGupta, Kamaldeep, Sharmistha Roy, Ayman Altameem, Raghvendra Kumar, Abdul Khader Jilani Saudagar, and Ramesh Chandra Poonia. 2022. "Usability Evaluation and Classification of mHealth Applications for Type 2 Diabetes Mellitus Using MARS and ID3 Algorithm" International Journal of Environmental Research and Public Health 19, no. 12: 6999. https://doi.org/10.3390/ijerph19126999
APA StyleGupta, K., Roy, S., Altameem, A., Kumar, R., Saudagar, A. K. J., & Poonia, R. C. (2022). Usability Evaluation and Classification of mHealth Applications for Type 2 Diabetes Mellitus Using MARS and ID3 Algorithm. International Journal of Environmental Research and Public Health, 19(12), 6999. https://doi.org/10.3390/ijerph19126999