
Differences in Unfavorable Lifestyle Changes during the COVID-19 Pandemic between People with and without Disabilities in Finland: Psychological Distress as a Mediator


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data and Design
2.2. Measures
2.2.1. Disability
2.2.2. Outcome Variables
2.2.3. Potential Meditator
2.2.4. Demographic Covariates
2.2.5. Data Analyses
3. Results
3.1. Lifestyle Differences between People with and without Disabilities
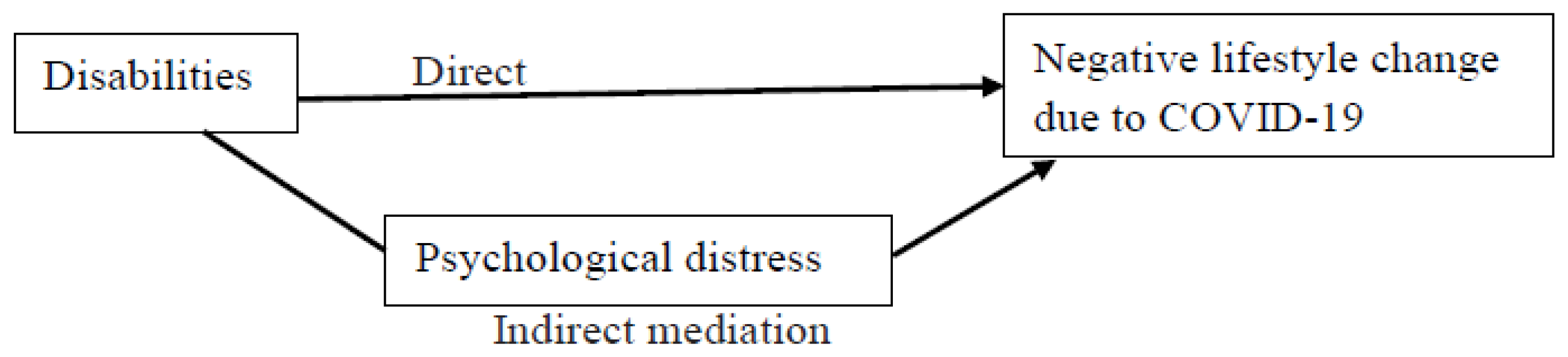
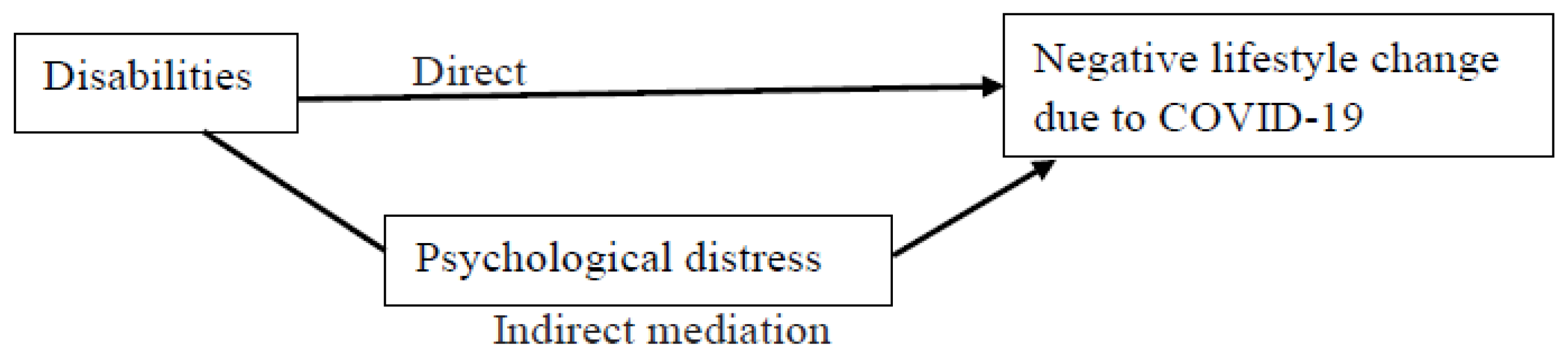
3.2. Psychological Distress as a Mediator
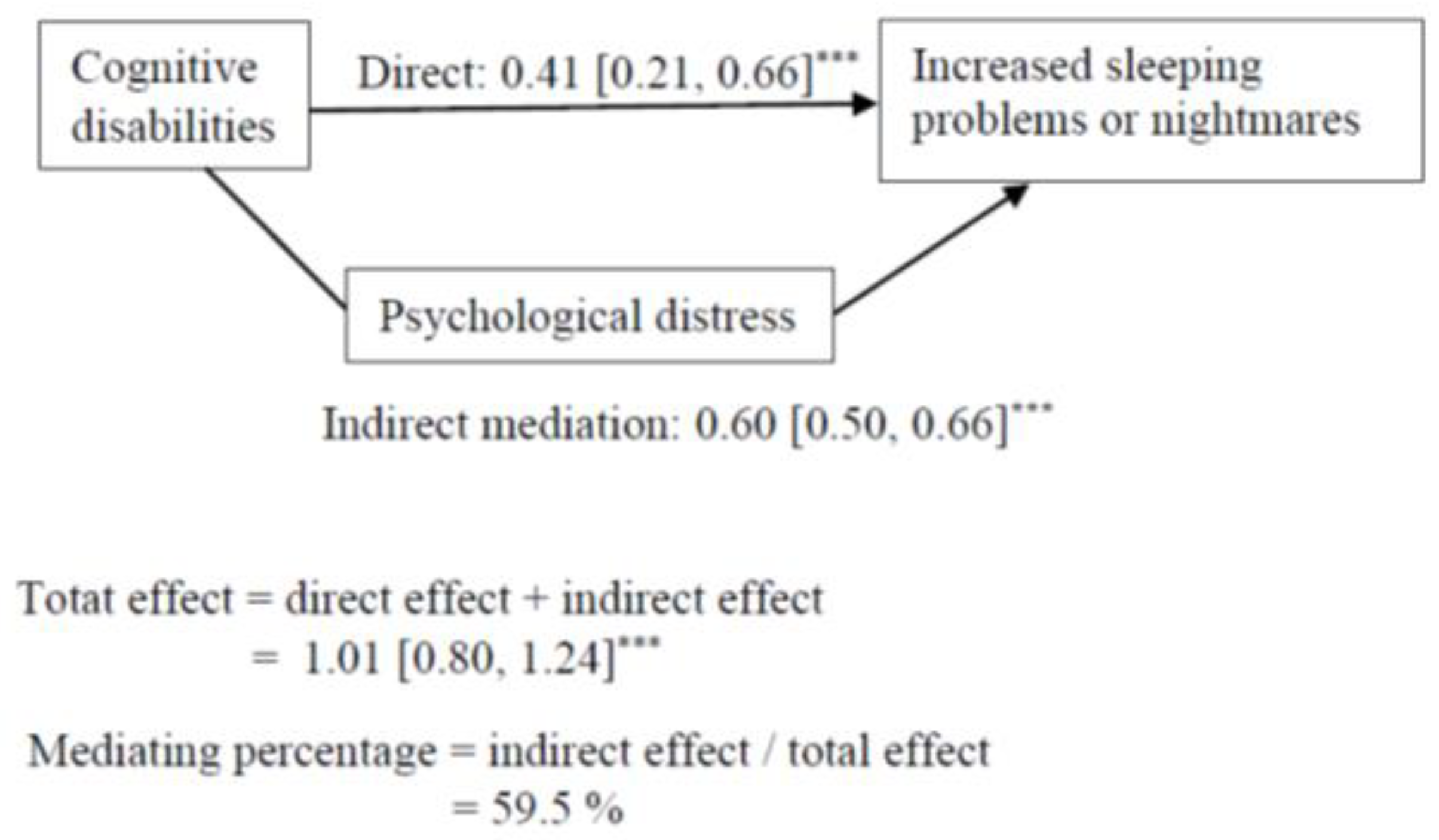
3.2.1. Increased Sleeping Problems or Nightmares
3.2.2. Decreased Daily Exercise
3.2.3. Decreased Vegetable Consumption
3.2.4. Increased Snacking
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Increased Sleeping Problems or Nightmares | Decreased Daily Exercise | |||
| Disabilities | OR [95% CI] | % [95% CI] | OR [95% CI] | % [95% CI] |
| Any disabilities a | ||||
| No | ref. | 10.6 [9.9, 11.3] | ref. | 24.3 [23.4, 25.3] |
| Yes | 2.82 *** [2.45, 3.25] | 25.0 [22.8, 27.3] | 1.50 *** [1.34, 1.68] | 32.5 [30.3, 34.8] |
| Cognitive disabilities | ||||
| No | ref. | 11.3 [10.6, 12.0] | ref. | 24.9 [24.0, 25.8] |
| Yes | 3.08 *** [2.54, 3.73] | 28.2 [24.6, 31.9] | 1.40 *** [1.18, 1.66] | 31.7 [28.2, 35.2] |
| Vision disabilities | ||||
| No | ref. | 11.9 [11.3, 12.6] | ref. | 25.2 [24.3, 26.1] |
| Yes | 3.23 *** [2.40, 4.35] | 30.5 [24.3, 36.6] | 1.28 [0.97, 1.69] | 30.2 [24.5, 36.0] |
| Hearing disabilities | ||||
| No | ref. | 11.9 [11.2, 12.6] | ref. | 25.3 [24.4, 26.2] |
| Yes | 3.02 *** [2.31, 3.94] | 29.0 [23.7, 34.3] | 1.15 [0.90, 1.47] | 28.0 [23.2, 32.9] |
| Mobility disabilities | ||||
| No | ref. | 11.4 [10.7, 12.1] | ref. | 24.5 [23.5, 25.4] |
| Yes | 2.79 *** [2.38, 3.28] | 26.4 [23.6, 29.2] | 1.97 *** [1.73, 2.24] | 38.9 [36.1, 41.7] |
| Decreased vegetable consumption | Increased snacking b | |||
| Disabilities | OR [95% CI] | % [95% CI] | OR [95% CI] | % [95% CI] |
| Any disabilities | ||||
| No | ref. | 4.7 [4.2, 5.1] | ref. | 25.5 [24.4, 26.6] |
| Yes | 1.85 *** [1.50, 2.28] | 8.4 [7.0, 9.7] | 1.46 *** [1.24, 1.73] | 33.4 [29.9, 36.9] |
| Cognitive disabilities | ||||
| No | ref. | 4.9 [4.4, 5.4] | ref. | 25.6 [24.6, 26.7] |
| Yes | 2.00 *** [1.51, 2.64] | 9.3 [7.1, 11.5] | 1.81 *** [1.44, 2.28] | 38.4 [33.1, 43.7] |
| Vision disabilities | ||||
| No | ref. | 5.1 [4.6, 5.5] | ref. | 26.1 [25.1, 27.1] |
| Yes | 1.84 ** [1.20, 2.81] | 8.9 [5.6, 12.3] | 1.40 [0.96, 2.05] | 33.1 [24.7, 41.4] |
| Hearing disabilities | ||||
| No | ref. | 5.0 [4.5, 5,5] | ref. | 26.1 [25.1, 27.2] |
| Yes | 2.24 *** [1.59, 3.16] | 10.6 [7.5, 13.7] | 1.25 [0.84, 1.86] | 30.7 [22.2, 39.1] |
| Mobility disabilities | ||||
| No | ref. | 4.9 [4.5, 5.4] | ref. | 26.1 [25.1, 27.2] |
| Yes | 1.77 *** [1.41, 2.22] | 8.4 [6.8, 10.0] | 1.15 [0.90, 1.48] | 28.9 [23.9, 33.9] |
References
- Finnish Government. Restrictions during the Coronavirus Epidemic. 2022. Available online: https://valtioneuvosto.fi/en/information-on-coronavirus/current-restrictions (accessed on 21 April 2022).
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. 2022. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/ (accessed on 21 April 2022).
- Lund, E.M.; Forber-Pratt, A.J.; Wilson, C.; Mona, L.R. The COVID-19 pandemic, stress, and trauma in the disability community: A call to action. Rehabil. Psychol. 2020, 65, 313–322. [Google Scholar] [CrossRef] [PubMed]
- United Nations. United Nations Policy Brief: A Disability-Inclusive Response to COVID-19. 2021. Available online: https://unsdg.un.org/sites/default/files/2020-05/Policy-Brief-A-Disability-Inclusive-Response-to-COVID-19.pdf (accessed on 21 April 2022).
- Littlejohn, J.; Venneri, A.; Marsden, A.; Plack, C.J. Self-reported hearing difficulties are associated with loneliness, depression and cognitive dysfunction during the COVID-19 pandemic. Int. J. Audiol. 2022, 61, 97–101. [Google Scholar] [CrossRef]
- Necho, M.; Birkie, M.; Gelaye, H.; Beyene, A.; Belete, A.; Tsehay, M. Depression, anxiety symptoms, Insomnia, and coping during the COVID-19 pandemic period among individuals living with disabilities in Ethiopia. PLoS ONE 2020, 15, e0244530. [Google Scholar] [CrossRef]
- Okoro, C.A.; Strine, T.W.; McKnight-Eily, L.; Verlenden, J.; Hollis, N.T.D. Indicators of poor mental health and stressors during the COVID-19 pandemic, by disability status: A cross-sectional analysis. Disabil. Health J. 2021, 14, 101110. [Google Scholar] [CrossRef]
- Steptoe, A.; Di Gessa, G. Mental health and social interactions of older people with physical disabilities in England during the COVID-19 pandemic: A longitudinal cohort study. Lancet Public Health 2021, 6, e365–e373. [Google Scholar] [CrossRef]
- Ting, D.S.J.; Krause, S.; Said, D.G.; Dua, H.S. Psychosocial impact of COVID-19 pandemic lockdown on people living with eye diseases in the UK. Eye 2021, 35, 2064–2066. [Google Scholar] [CrossRef] [PubMed]
- Kuper, H.; Banks, L.M.; Bright, T.; Dave, C.; Shakespeare, T. Disability-inclusive COVID-19 response: What it is, why it is important and what we can learn from the United Kingdom’s response. Wellcome Open Res. 2020, 5. [Google Scholar] [CrossRef]
- Bentzen, M.; Brurok, B.; Roeleveld, K.; Hoff, M.; Jahnsen, R.; Wouda, M.F.; Baumgart, J.K. Changes in physical activity and basic psychological needs related to mental health among people with physical disability during the COVID-19 pandemic in Norway. Disabil. Health J. 2021, 14, 101126. [Google Scholar] [CrossRef]
- Yang, Y.; Xiao, Y.; Liu, Y.; Li, Q.; Shan, C.; Chang, S.; Jen, P.H.-S. Mental health and psychological impact on students with or without hearing loss during the recurrence of the COVID-19 pandemic in China. Int. J. Environ. Res. Public Health 2021, 18, 1421. [Google Scholar] [CrossRef] [PubMed]
- Holm, M.E.; Sainio, P.; Parikka, S.; Koskinen, S. The Effects of the COVID-19 pandemic on the psychosocial well-being of people with disabilities. Disabil. Health 2022, 15, 101224. [Google Scholar] [CrossRef] [PubMed]
- Beck, F.; Léger, D.; Fressard, L.; Peretti-Watel, P.; Verger, P.; The Coconel Group. COVID-19 health crisis and lockdown associated with high level of sleep complaints and hypnotic uptake at the population level. J. Sleep Res. 2021, 30, e13119. [Google Scholar] [CrossRef] [PubMed]
- Cellini, N.; Canale, N.; Mioni, G.; Costa, S. Changes in sleep pattern, sense of time, and digital media use during COVID-19 lockdown in Italy. J. Sleep Res. 2020, 29, e13074. [Google Scholar] [CrossRef]
- Mandelkorn, U.; Genzer, S.; Choshen-Hillel, S.; Reiter, J.; Meira e Cruz, M.; Hochner, H.; Kheirandish-Gozal, L.; Gozal, D.; Gileles-Hillel, A. Escalation of sleep disturbances amid the COVID-19 pandemic: A cross-sectional international study. J. Clin. Sleep Med. 2021, 17, 45–53. [Google Scholar] [CrossRef]
- Rawat, D.; Dixit, V.; Gulati, S.; Gulati, S.; Gulati, A. Impact of COVID-19 outbreak on lifestyle behaviour: A review of studies published in India. Diabetes Metab. Syndr. 2021, 15, 331–336. [Google Scholar] [CrossRef]
- Castañeda-Babarro, A.; Arbillaga-Etxarri, A.; Gutiérrez-Santamaría, B.; Coca, A. Physical activity change during COVID-19 confinement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef]
- Maugeri, G.; Castrogiovanni, P.; Battaglia, G.; Pippi, R.; D’Agata, V.; Palma, A.; Di Rosa, M.; Musumeci, G. The impact of physical activity on psychological health during COVID-19 pandemic in Italy. Heliyon 2020, 6, e04315. [Google Scholar] [CrossRef]
- Robinson, E.; Gillespie, S.; Jones, A. Weight-related lifestyle behaviours and the COVID-19 crisis: An online survey study of UK adults during social lockdown. Obes. Sci. Pract. 2020, 6, 735–740. [Google Scholar] [CrossRef]
- López-Bueno, R.; Calatayud, J.; Casaña, J.; Casajús, J.A.; Smith, L.; Tully, M.A.; Andersen, L.L.; López-Sánchez, G.F. COVID 19 confinement and health risk behaviors in Spain. Front. Psychol. 2020, 11, 1426. [Google Scholar] [CrossRef]
- Aghababa, A.; Sani, S.H.Z.; Rohani, H.; Nabilpour, M.; Badicu, G.; Fathirezaie, Z.; Brand, S. No evidence of systematic change of physical activity patterns before and during the COVID-19 pandemic and related mood states among Iranian adults attending team sports activities. Front. Psychol. 2021, 12, 641895. [Google Scholar] [CrossRef]
- Albrecht, J.N.; Werner, H.; Rieger, N.; Widmer, N.; Janisch, D.; Huber, R.; Jenni, O.G. Association between homeschooling and adolescent sleep duration and health during COVID-19 Pandemic high school closures. JAMA Netw. Open 2022, 5, e2142100. [Google Scholar] [CrossRef]
- Poelman, M.P.; Gillebaart, M.; Schlinkert, C.; Dijkstra, S.C.; Derksen, E.; Mensink, F.; Hermans, R.C.J.; Aardening, P.; de Ridder, D.; de Vet, E. Eating behavior and food purchases during the COVID-19 lockdown: A cross-sectional study among adults in the Netherlands. Appetite 2021, 157, 105002. [Google Scholar] [CrossRef]
- Yang, G.-Y.; Lin, X.-L.; Fang, A.-P.; Zhu, H.-L. Eating habits and lifestyles during the initial stage of the COVID-19 lockdown in China: A cross-sectional study. Nutrients 2021, 13, 970. [Google Scholar] [CrossRef]
- Bakaloudi, D.R.; Jeyakumar, D.T.; Jayawardena, R.; Chourdakis, M. The impact of COVID-19 lockdown on snacking habits, fast-food and alcohol consumption: A systematic review of the evidence. Clin. Nutr. 2021. Online ahead of print. [Google Scholar] [CrossRef]
- Dixon-Ibarra, A.; Horner-Johnson, W. Disability status as an antecedent to chronic conditions: National health interview survey, 2006–2012. Prev. Chronic Dis. 2014, 11, 130251. [Google Scholar] [CrossRef] [Green Version]
- Sabariego, C.; Oberhauser, C.; Posarac, A.; Bickenbach, J.; Kostanjsek, N.; Chatterji, S.; Officer, A.; Coenen, M.; Chhan, L.; Cieza, A. Measuring disability: Comparing the impact of two data collection approaches on disability rates. Int. J. Environ. Res. Public Health 2015, 12, 10329–10351. [Google Scholar] [CrossRef] [Green Version]
- Carroll, D.D.; Courtney-Long, E.A.; Stevens, A.C.; Sloan, M.L.; Lullo, C.; Visser, S.N.; Fox, M.H.; Armour, B.S.; Campbell, V.A.; Brown, D.R.; et al. Vital signs: Disability and physical activity—United States, 2009–2012. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 407–413. [Google Scholar]
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.L.; Alley, S.J.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, anxiety and stress during COVID-19: Associations with changes in physical activity, sleep, tobacco and alcohol use in Australian adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef]
- Puccinelli, P.J.; da Costa, T.S.; Seffrin, A.; de Lira, C.A.B.; Vancini, R.L.; Nikolaidis, P.T.; Knechtle, B.; Rosemann, T.; Hill, L.; Andrade, M.S. Reduced level of physical activity during COVID-19 pandemic is associated with depression and anxiety levels: An internet-based survey. BMC Public Health 2021, 21, 425. [Google Scholar] [CrossRef]
- Chee, M.J.; Koziel Ly, N.K.; Anisman, H.; Matheson, K. Piece of Cake: Coping with COVID-19. Nutrients 2020, 12, 3803. [Google Scholar] [CrossRef]
- Landaeta-Díaz, L.; González-Medina, G.; Agüero, S.D. Anxiety, anhedonia and food consumption during the COVID-19 quarantine in Chile. Appetite 2021, 164, 105259. [Google Scholar] [CrossRef]
- Okoro, C.A.; Strine, T.W.; Balluz, L.S.; Crews, J.E.; Dhingra, S.; Berry, J.T.; Mokdad, A.H. Serious psychological distress among adults with and without disabilities. Int. J. Public Health 2009, 54, S52–S60. [Google Scholar] [CrossRef]
- Rotarou, E.S.; Sakellariou, D. Depressive symptoms in people with disabilities; secondary analysis of cross-sectional data from the United Kingdom and Greece. Disabil. Health J. 2018, 11, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Cree, R.A.; Okoro, C.A.; Zack, M.M.; Carbone, E. Frequent mental distress among adults, by disability status, disability type, and selected characteristics—United States, 2018. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1238–1243. [Google Scholar] [CrossRef] [PubMed]
- Temple, J.B.; Kelaher, M. Is disability exclusion associated with psychological distress? Australian evidence from a national cross-sectional survey. BMJ Open 2018, 8, e020829. [Google Scholar] [CrossRef] [Green Version]
- Emerson, E.; Fortune, N.; Llewellyn, G.; Stancliffe, R. Loneliness, social support, social isolation and wellbeing among working age adults with and without disability: Cross sectional study. Disabil. Health J. 2021, 14, 100965. [Google Scholar] [CrossRef]
- Banks, L.M.; Kuper, H.; Polack, S. Correction: Poverty and disability in low- and middle-income countries: A systematic review. PLoS ONE 2018, 13, e0204881. [Google Scholar] [CrossRef]
- Bright, T.; Wallace, S.; Kuper, H.A. A systematic review of access to rehabilitation for people with disabilities in low- and middle-income countries. Int. J. Environ. Res. Public Health 2018, 15, 2165. [Google Scholar] [CrossRef] [Green Version]
- Kavanagh, A.; Hatton, C.; Stancliffe, R.J.; Aitken, Z.; King, T.; Hastings, R.; Totsika, V.; Llewellyn, G.; Emerson, E. Health and healthcare for people with disabilities in the UK during the COVID-19 pandemic. Disabil. Health J. 2021, 15, 101171. [Google Scholar] [CrossRef]
- Lunsky, Y. The impact of stress and social support on the mental health of individuals with intellectual disabilities. Salud Pública Mex. 2008, 2, 151–153. [Google Scholar] [CrossRef] [Green Version]
- Luca, A.; Luca, M.; Calandra, C. Sleep disorders and depression: Brief review of the literature, case report, and nonpharmacologic interventions for depression. Clin. Interv. Aging 2013, 8, 1033–1039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geiker, N.R.W.; Astrup, A.; Hjorth, M.F.; Sjodin, A.; Pijls, L.; Markus, C.R. Does stress influence sleep patterns, food intake, weight gain, abdominal obesity and weight loss interventions and vice versa? Obes. Rev. 2018, 19, 81–97. [Google Scholar] [CrossRef]
- Marashi, M.Y.; Nicholson, E.; Ogrodnik, M.; Fenesi, B.; Heisz, J.J. A mental health paradox: Mental health was both a motivator and barrier to physical activity during the COVID-19 pandemic. PLoS ONE 2021, 16, e0239244. [Google Scholar] [CrossRef]
- Pentala-Nikulainen, O.; Koskela, T.; Parikka, S.; Aalto, A.-M.; Muuri, A. Alueelliset Erot Aikuisväestön Palvelukokemuksissa ja Hyvinvoinnissa: FinSote 2018. 2018. Available online: https://www.julkari.fi/handle/10024/136438 (accessed on 21 April 2022).
- Härkänen, T.; Kaikkonen, R.; Virtala, E.; Koskinen, S. Inverse probability weighting and doubly robust methods in correcting the effects of non-response in the reimbursed medication and self-reported turnout estimates in the ATH survey. BMC Public Health 2014, 14, 1150. [Google Scholar] [CrossRef]
- Seaman, S.R.; White, I.R. Review of inverse probability weighting for dealing with missing data. Stat. Methods Med. Res. 2013, 22, 278–295. [Google Scholar] [CrossRef]
- Washington Group. Washington Group on Disability Statistics. 2020. Available online: https://www.washingtongroup-disability.com/question-sets/wg-short-set-on-functioning-wg-ss (accessed on 21 April 2022).
- Cuijpers, P.; Smits, N.; Donker, T.; ten Have, M.; de Graaf, R. Screening for mood and anxiety disorders with the five-item, the three-item, and the two-item mental health inventory. Psychiatry Res. 2009, 168, 250–255. [Google Scholar] [CrossRef]
- Kelly, M.J.; Dunstan, F.D.; Lloyd, K.; Fone, D.L. Evaluating cutpoints for the MHI-5 and MCS using the GHQ-12: A comparison of five different methods. BMC Psychiatry 2008, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.; Yi, F.; Xu, Z.; Tian, X. Do living arrangements matter?—Evidence from eating behaviors of the elderly in rural China. J. Econ. Ageing 2021, 19, 100307. [Google Scholar] [CrossRef]
- Kreuter, F.; Valliant, R. A survey on survey statistics: What is done and can be done in Stata. Stata J. 2007, 7, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Williams, R. Using the margins command to estimate and interpret adjusted predictions and marginal effects. Stata J. 2012, 12, 308–331. [Google Scholar] [CrossRef] [Green Version]
- Kohler, U.; Karlson, K.B.; Holm, A. Comparing coefficients of nested nonlinear probability models. Stata J. 2011, 11, 420–438. [Google Scholar] [CrossRef] [Green Version]
- Karlson, K.B.; Holm, A.; Breen, R. Comparing regression coefficients between models using logit and probit: A new method. Sociol. Methodol. 2012, 42, 286–313. [Google Scholar] [CrossRef]
- Smith, E.K.; Lacy, M.G.; Mayer, A. Performance simulations for categorical mediation: Analyzing KHB estimates of mediation in ordinal regression models. Stata J. 2019, 19, 913–930. [Google Scholar] [CrossRef]
- Deng, Y.; Li, X.; Liu, L.; Chui, W.H. Suicide attempts and perceived social support among Chinese drug users: The mediating role of self-esteem and depression. Int. J. Environ. Res. Public Health 2021, 18, 208. [Google Scholar] [CrossRef]
- Stubbs, B.; Koyanagi, A.; Schuch, F.B.; Firth, J.; Rosenbaum, S.; Veronese, N.; Solmi, M.; Mugisha, J.; Vancampfort, D. Physical activity and depression: A large cross-sectional, population-based study across 36 low- and middle-income countries. Acta Psychiatr. Scand. 2016, 134, 546–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinne, S.; Patrick, D.L.; Doyle, D.L. Prevalence of secondary conditions among people with disabilities. Am. J. Public Health 2004, 94, 443–445. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, R.A.P.C. Sleep disturbances and mild cognitive impairment: A review. Sleep Sci. 2015, 8, 36–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clarke, N.A.; Hoare, D.J.; Killan, E.C. Evidence for an association between hearing impairment and disrupted sleep: Scoping Review. Am. J. Audiol. 2019, 28, 1015–1024. [Google Scholar] [CrossRef] [Green Version]
- Seixas, A.; Ramos, A.R.; Gordon-Strachan, G.M.; Fonseca, V.A.; Zizi, F.; Jean-Louis, G. Relationship between visual impairment, insomnia, anxiety/depressive symptoms among Russian immigrants. J. Sleep Med. Disord. 2014, 1, 1009. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Jesus, T.S.; Bhattacharjya, S.; Papadimitriou, C.; Bogdanova, Y.; Bentley, J.; Arango-Lasprilla, J.C.; Kamalakannan, S.; The Refugee Empowerment Task Force, International Networking Group of the American Congress of Rehabilitation Medicine. Lockdown related disparities experienced by people with disabilities during the first wave of the COVID-19 pandemic: Scoping review with thematic analysis. Int. J. Environ. Res. Public Health 2021, 18, 6178. [Google Scholar] [CrossRef] [PubMed]
- McGuire, B.E.; Daly, P.; Smyth, F. Lifestyle and health behaviours of adults with an intellectual disability. J. Intellect. Disabil. Res. 2007, 51, 497–510. [Google Scholar] [CrossRef]
- McClure, K.S.; Halpern, J.; Wolper, P.A.; Donahue, J.J. Emotion regulation and intellectual disability. J. Dev. Disabil. 2009, 15, 38–44. [Google Scholar]
- Berger, N.; Robine, J.M.; Ojima, T.; Madans, J.; Van Oyen, H. Harmonising summary measures of population health using global survey instruments. J. Epidemiol. Community Health 2016, 70, 1039–1044. [Google Scholar] [CrossRef] [Green Version]
- Elovanio, M.; Hakulinen, C.; Pulkki-Råback, L.; Aalto, A.-M.; Virtanen, M.; Partonen, T.; Suvisaari, J. General health questionnaire (GHQ-12), Beck depression inventory (BDI-6), and Mental Health Index (MHI-5): Psychometric and predictive properties in a Finnish population-based sample. Psychiatry Res. 2020, 289, 112973. [Google Scholar] [CrossRef]
- Mäntyselkä, P.; Kautiainen, H.; Miettola, J. Beliefs and attitudes towards lifestyle change and risks in primary care—A community based study. BMC Public Health 2019, 19, 1049. [Google Scholar] [CrossRef] [Green Version]
- Viertio, S.; Kiviruusu, O.; Piirtola, M.; Kaprio, J.; Korhonen, T.; Marttunen, M.; Suvisaari, J. Factors contributing to psychological distress in the working population, with a special reference to gender difference. BMC Public Health 2021, 21. [Google Scholar] [CrossRef] [PubMed]
- Lake, S.; MacHale, R. Mindfulness Matters: A pilot study of a Mindfulness-Based Stress Reduction group for adults with intellectual disabilities. Br. J. Learn. Disabil. 2021. Online ahead of print. [Google Scholar] [CrossRef]
- Mactavish, J.; Iwasaki, Y. Exploring perspectives of individuals with disabilities on stress-coping. J. Rehabil. 2005, 71, 20–31. [Google Scholar]
| No Disabilities | Any Disabilities a | Cognitive Disabilities | Vision Disabilities | Hearing Disabilities | Mobility Disabilities | |
|---|---|---|---|---|---|---|
| Total, n | 17,733 | 4134 | 1773 | 663 | 884 | 2580 |
| Total | 86.8 [86.2, 87.3] | 13.2 [12.7, 13.8] | 6.3 [5.9, 6.8] | 2.3 [2.1, 2.6] | 2.7 [2.4, 2.9] | 7.0 [6.6, 7.3] |
| Females | 52.7 [51.6, 53.7] | 51.4 [49.2, 53.7] | 47.5 [44.0, 51.0] | 46.5 [41.0, 52.1] | 44.1 [39.5, 48.7] | 58.0 [55.3, 60.7] |
| Age | ||||||
| 20–54 | 58.9 [58.0, 59.8] | 27.0 [24.4, 29.6] | 36.2 [32.2, 40.2] | 34.1 [27.7, 40.5] | 24.3 [18.8, 29.8] | 12.0 [9.3, 14.7] |
| 55–74 | 32.3 [31.4, 33.1] | 35.3 [33.2, 37.4] | 30.1 [27.1, 33.0] | 31.5 [26.6, 36.4] | 29.0 [25.0, 33.0] | 36.3 [33.7, 38.9] |
| 75 or over | 8.9 [8.5, 9.2] | 37.7 [35.8, 39.6] | 33.7 [31.0, 36.4] | 34.3 [29.9, 38.8] | 46.6 [42.1, 51.2] | 51.7 [49.0, 54.4] |
| Living alone | 28.4 [27.4, 29.4] | 45.8 [43.5, 48.0] | 45.8 [42.2, 49.4] | 47.5 [41.6, 53.4] | 45.4 [40.5, 50.2] | 49.4 [46.7, 52.1] |
| Education level | ||||||
| Low | 39.6 [38.6, 40.7] | 54.1 [51.8, 56.5] | 55.0 [51.3, 58.6] | 65.4 [59.9, 70.9] | 56.0 [51.1, 60.9] | 53.1 [50.3, 55.8] |
| Medium | 33.7 [32.8, 34.7] | 29.3 [27.2, 31.4] | 29.6 [26.3, 33.0] | 24.4 [19.4, 29.4] | 26.6 [22.4, 30.8] | 30.1 [27.6, 32.6] |
| High | 26.6 [25.7, 27.5] | 16.5 [14.9, 18.1] | 15.4 [12.9, 17.9] | 10.2 [7.3, 13.1] | 17.4 [13.8, 21.0] | 16.8 [14.9, 18.7] |
| Increased Sleeping Problems or Nightmares | Decreased Daily Exercise | |||
| Disabilities | OR[95% CI] | % [95% CI] | OR[95% CI] | % [95% CI] |
| Any disabilities a | ||||
| No | ref. | 10.7 [10.0, 11.4] | ref. | 24.0 [23.0, 24.9] |
| Yes | 2.45 *** [2.06, 2.91] | 22.4 [19.7, 25.0] | 1.80 *** [1.57, 2.05] | 35.8 [33.0, 38.5] |
| Cognitive disabilities | ||||
| No | ref. | 11.3 [10.6, 12.0] | ref. | 24.8 [23.9, 25.7] |
| Yes | 2.73 *** [2.19, 3.40] | 25.3 [21.4, 29.2] | 1.56 *** [1.30, 1.88] | 33.7 [29.8, 37.6] |
| Vision disabilities | ||||
| No | ref. | 11.9 [11.2, 12.6] | ref. | 25.1 [24.2, 26.1] |
| Yes | 2.74 *** [1.95, 3.84] | 26.4 [20.1, 32.6] | 1.37 [0.99, 1.89] | 31.2 [25.0, 37.5] |
| Hearing disabilities | ||||
| No | ref. | 11.8 [11.2, 12.5] | ref. | 25.2 [24.3, 26.1] |
| Yes | 2.52 *** [1.85, 3.45] | 24.8 [19.2, 30.4] | 1.19 [0.90, 1.58] | 28.6 [23.0, 34.1] |
| Mobility disabilities | ||||
| No | ref. | 11.5 [10.8, 12.2] | ref. | 24.2 [23.3, 25.1] |
| Yes | 2.04 *** [1.68, 2.49] | 20.8 [17.7, 23.9] | 2.52 *** [2.18, 2.93] | 43.9 [40.5, 47.4] |
| Decreased vegetable consumption | Increased snacking b | |||
| Disabilities | OR[95% CI] | % [95% CI] | OR[95% CI] | % [95% CI] |
| Any disabilities | ||||
| No | ref. | 4.6 [4.2, 5.1] | ref. | 25.6 [24.5, 26.7] |
| Yes | 2.05 *** [1.60, 2.63] | 9.0 [7.2, 10.9] | 1.71 *** [1.42, 2.05] | 36.5 [32.6., 40.3] |
| Cognitive disabilities | ||||
| No | ref. | 4.9 [4.4, 5.4] | ref. | 25.9 [24.8, 26.9] |
| Yes | 1.99 *** [1.45, 2.72] | 9.2 [6.7, 11.7] | 1.95 *** [1.52, 2.50] | 39.8 [34.3, 45.4] |
| Vision disabilities | ||||
| No | ref. | 5.1 [4.6, 5.5] | ref. | 26.3 [25.3, 27.4] |
| Yes | 1.80 * [1.12, 2.89] | 8.7 [5.0, 12.4] | 1.47 [0.95, 2.26] | 34.0 [24.8, 43.3] |
| Hearing disabilities | ||||
| No | ref. | 5.0 [4.5, 5.5] | ref. | 26.3 [25.3, 27.4] |
| Yes | 2.36 *** [1.60, 3.47] | 10.9 [7.3, 14.6] | 1.37 [0.86, 2.17] | 32.6 [23.0, 42.2] |
| Mobility disabilities | ||||
| No | ref. | 4.9 [4.4, 5.4] | ref. | 26.2 [25.2, 27.3] |
| Yes | 1.94 *** [1.48, 2.55] | 9.1 [6.9, 11.2] | 1.39 [1.00, 1.86] | 33.1 [27.0, 39.2] |
| OR [95% CI] | % [95% CI] | |
|---|---|---|
| Any disabilities a | ||
| No | ref. | 18.6 [17.7, 19.4] |
| Yes | 4.98 *** [4.36, 5.68] | 51.1 [48.4, 53.9] |
| Cognitive disabilities | ||
| No | ref. | 20.0 [19.1, 20.8] |
| Yes | 6.46 *** [5.46, 7.63] | 59.9 [56.2, 63.5] |
| Vision disabilities | ||
| No | ref. | 21.7 [20.8, 22.5] |
| Yes | 3.85 *** [2.96, 4.99] | 50.3 [44.1, 56.5] |
| Hearing disabilities | ||
| No | ref. | 21.5 [20.7, 22.4] |
| Yes | 4.54 *** [3.67, 5.62] | 54.0 [49.0, 59.0] |
| Mobility disabilities | ||
| No | ref. | 20.9 [20.1, 21.8] |
| Yes | 3.14 *** [2.70, 3.65] | 44.2 [40.8, 47.6] |
| Any Disabilities a | Cognitive Disabilities | Vision Disabilities | Hearing Disabilities | Mobility Disabilities | |
|---|---|---|---|---|---|
| Mediation Models | B [95% CI] | B [95% CI] | B [95% CI] | B [95% CI] | B [95% CI] |
| Disabilities → Increased sleeping problems or nightmares | |||||
| Direct path | 0.44 *** [0.26, 0.62] | 0.41 *** [0.21, 0.66] | 0.64 *** [0.28, 1.00] | 0.54 ** [0.21, 0.87] | 0.43 *** [0.22, 0.64] |
| Indirect path through MHI-5 | 0.44 *** [0.38, 0.51] | 0.60 *** [0.50, 0.66] | 0.44 *** [0.33, 0.55] | 0.48 *** [0.39, 0.57] | 0.31 *** [0.25, 0.37] |
| Total | 0.89 *** [0.71, 1.06] | 1.01 *** [80, 1.24] | 1.08 *** [0.73, 1.44] | 1.02 ** [0.69, 1.35] | 0.74 *** [0.53, 0.95] |
| Mediating percentage b, % | 49.2 | 59.5 | 40.8 | 47.0 | 41.7 |
| Disabilities → Decreased daily exercise | ns | ns | |||
| Direct path | 0.48 *** [0.34, 0.62] | 0.31 ** [0.11, 0.51] | 0.85 *** [0.70, 1.01] | ||
| Indirect path through MHI-5 | 0.11 *** [0.08, 0.15] | 0.17 *** [0.11, 0.22] | 0.08 *** [0.06, 0.11] | ||
| Total | 0.60 *** [0.46, 0.73] | 0.48 *** [0.28, 0.67] | 0.94 *** [0.79, 1.09] | ||
| Mediating percentage, % | 19.2 | 34.8 | 9.0 | ||
| Disabilities → Decreased vegetable consumption | |||||
| Direct path | 0.45 *** [0.18, 0.72] | 0.37 * [0.03, 0.72] | 0.34 [−0.14, 0.83] | 0.66 *** [0.24, 1.08] | 0.43 *** [0.14, 0.71] |
| Indirect path through MHI-5 | 0.22 *** [0.15, 0.30] | 0.30 *** [0.20, 0.40] | 0.24 *** [0.15, 0.32] | 0.24 *** [0.16, 0.32] | 0.16 *** [0.11, 0.22] |
| Total | 0.67 *** [0.42, 0.93] | 0.68 *** [0.35, 1.00] | 0.58 * [0.10, 1.07] | 0.90 *** [0.49, 1.30] | 0.59 *** [0.30, 0.87] |
| Mediating percentage, % | 32.7 | 44.7 | 39.9 | 26.4 | 27.6 |
| Disabilities → Increased snacking c | ns | ns | ns | ||
| Direct path | 0.30 ** [0.11, 0.50] | 0.38 ** [0.12, 0.65] | |||
| Indirect mediation path through MHI-5 | 0.22 *** [0.16, 0.27] | 0.28 *** [0.21, 0.35] | |||
| Total | 0.52 *** [0.33, 0.71] | 0.66 *** [0.40, 0.92] | |||
| Mediating percentage, % | 41.5 | 42.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holm, M.E.; Sainio, P.; Suvisaari, J.; Sääksjärvi, K.; Jääskeläinen, T.; Parikka, S.; Koskinen, S. Differences in Unfavorable Lifestyle Changes during the COVID-19 Pandemic between People with and without Disabilities in Finland: Psychological Distress as a Mediator. Int. J. Environ. Res. Public Health 2022, 19, 6971. https://doi.org/10.3390/ijerph19126971
Holm ME, Sainio P, Suvisaari J, Sääksjärvi K, Jääskeläinen T, Parikka S, Koskinen S. Differences in Unfavorable Lifestyle Changes during the COVID-19 Pandemic between People with and without Disabilities in Finland: Psychological Distress as a Mediator. International Journal of Environmental Research and Public Health. 2022; 19(12):6971. https://doi.org/10.3390/ijerph19126971
Chicago/Turabian StyleHolm, Marja Eliisa, Päivi Sainio, Jaana Suvisaari, Katri Sääksjärvi, Tuija Jääskeläinen, Suvi Parikka, and Seppo Koskinen. 2022. "Differences in Unfavorable Lifestyle Changes during the COVID-19 Pandemic between People with and without Disabilities in Finland: Psychological Distress as a Mediator" International Journal of Environmental Research and Public Health 19, no. 12: 6971. https://doi.org/10.3390/ijerph19126971
APA StyleHolm, M. E., Sainio, P., Suvisaari, J., Sääksjärvi, K., Jääskeläinen, T., Parikka, S., & Koskinen, S. (2022). Differences in Unfavorable Lifestyle Changes during the COVID-19 Pandemic between People with and without Disabilities in Finland: Psychological Distress as a Mediator. International Journal of Environmental Research and Public Health, 19(12), 6971. https://doi.org/10.3390/ijerph19126971