
Mediating Factors Explaining the Associations between Solid Fuel Use and Self-Rated Health among Chinese Adults 65 Years and Older: A Structural Equation Modeling Approach



Abstract
:1. Introduction
2. Materials and Methods
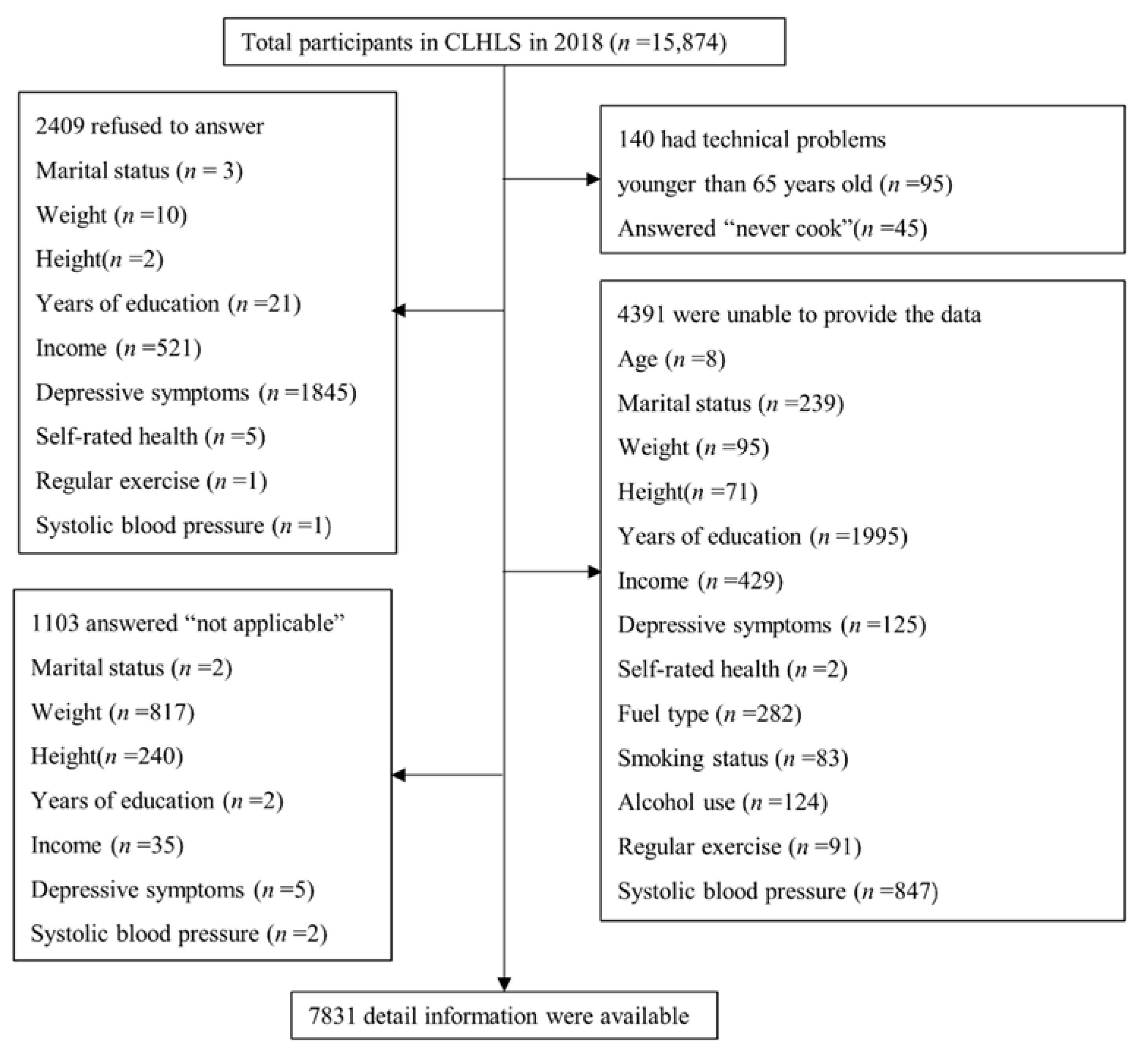
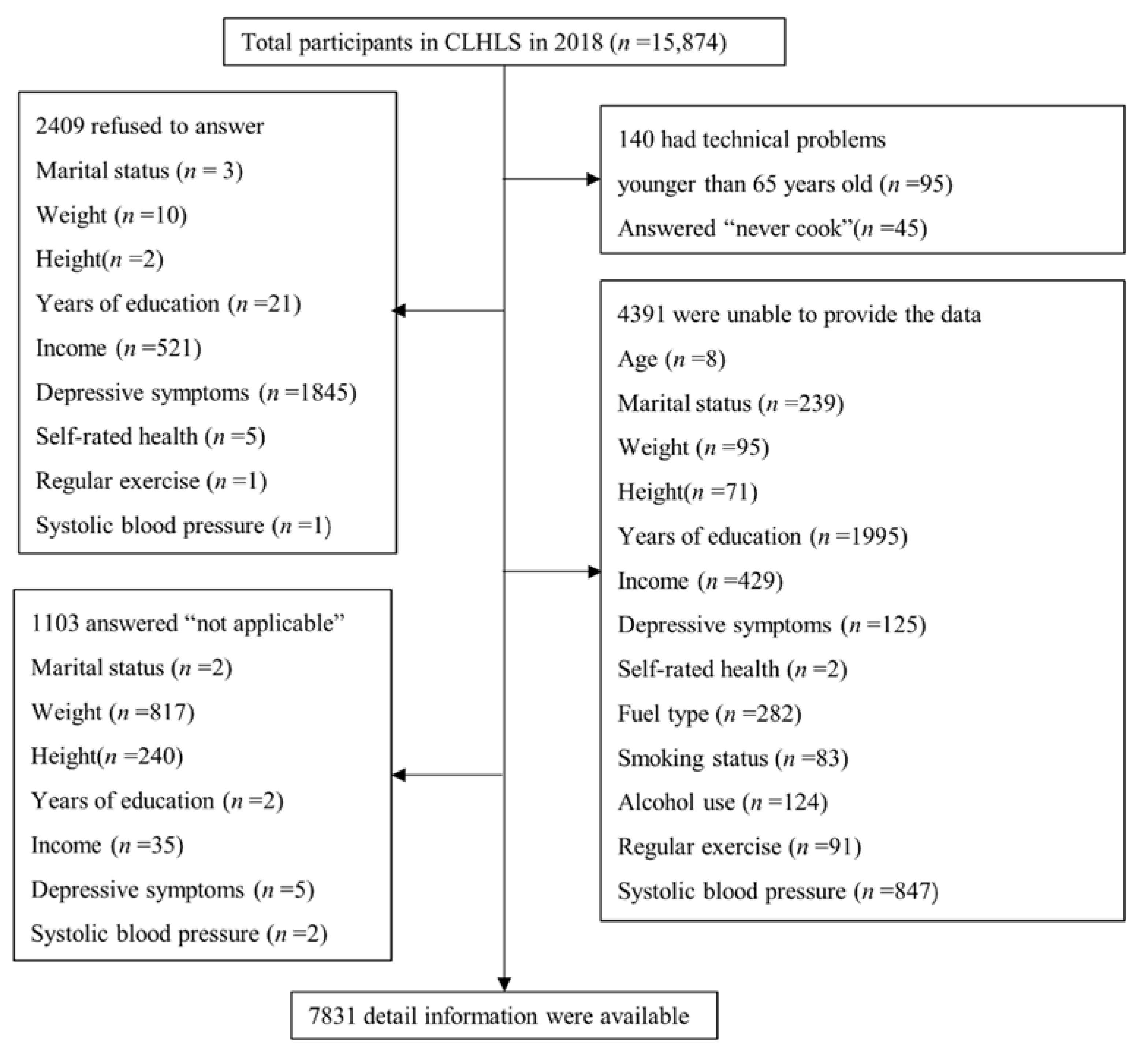
2.1. Setting and Participants
2.2. Outcome Variables
2.3. Exposure Variables
2.4. Mediators
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. Basic Characteristics of the Participants
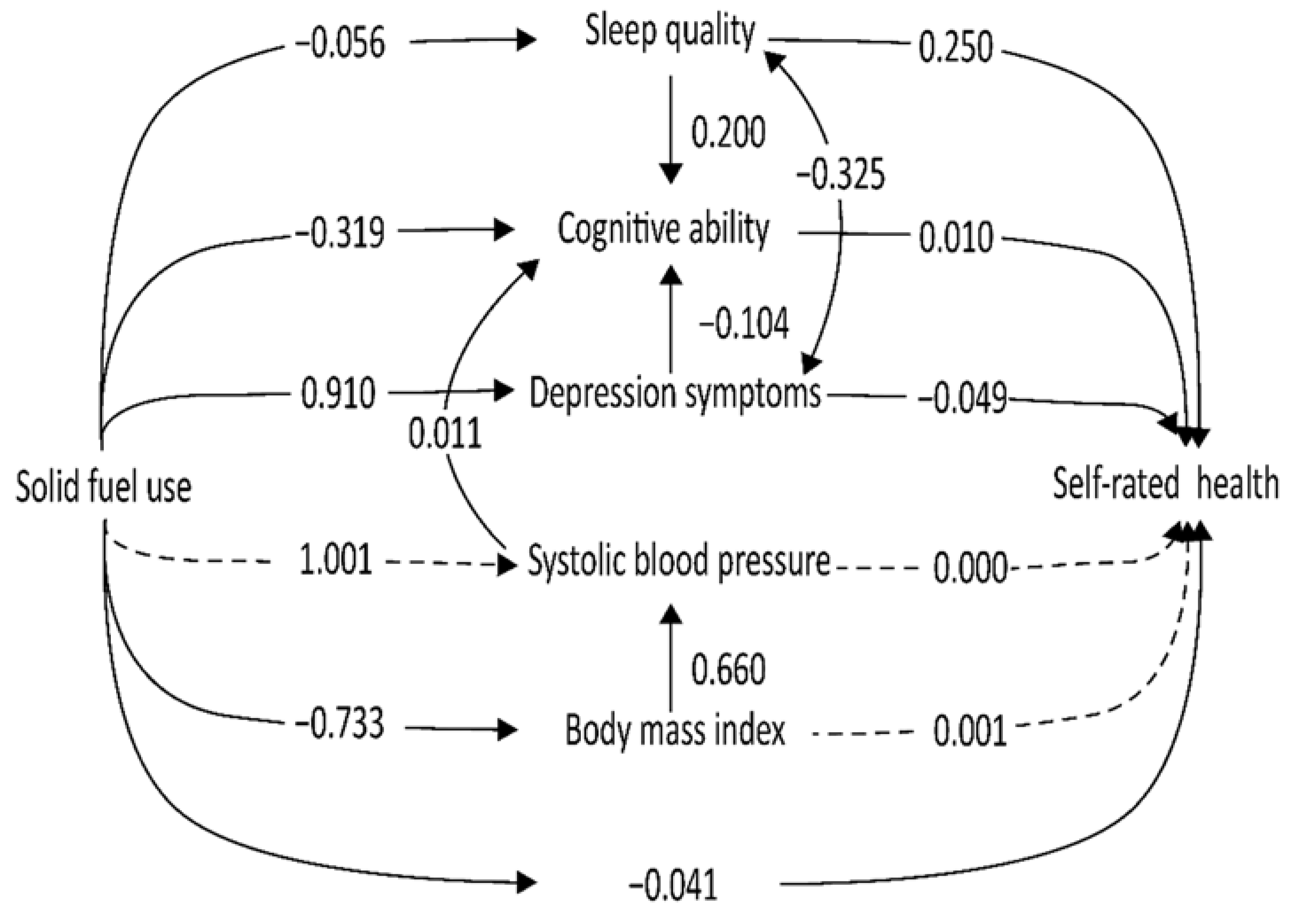
3.2. Structural Equation Model
4. Discussion
4.1. Main Findings
4.2. Available Evidence on the Association of Solid Fuel with Self-Rated Health
4.3. Depression Was the Strongest Mediator of the Relationship between Solid Fuel Use and Self-Rated Health
4.4. Cognition as the Protective Factor Linking Systolic Blood Pressure to Self-Rated Health
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Bureau of Statistics of the People’s Republic of China Interpretation of the Seventh National Census Communiqué. Available online: http://www.stats.gov.cn/tjsj/sjjd/202105/t20210512_1817336.html (accessed on 17 November 2021).
- Tang, X.; Liao, H. Energy poverty and solid fuels use in rural China: Analysis based on national population census. Energy Sustain. Dev. 2014, 23, 122–129. [Google Scholar] [CrossRef]
- Wang, L.; Xiang, Z.; Stevanovic, S.; Ristovski, Z.; Salimi, F.; Gao, J.; Wang, H.; Li, L. Role of Chinese cooking emissions on ambient air quality and human health. Sci. Total Environ. 2017, 589, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Zhai, D.; Kuang, M.; Xia, Y. Indoor air pollution and frailty: A cross-sectional and follow-up study among older Chinese adults. Environ. Res. 2021, 204, 112006. [Google Scholar] [CrossRef]
- Shao, J.; Ge, T.; Liu, Y.; Zhao, Z.; Xia, Y. Longitudinal associations between household solid fuel use and depression in middle-aged and older Chinese population: A cohort study. Ecotoxicol. Env. Saf. 2021, 209, 111833. [Google Scholar] [CrossRef] [PubMed]
- Balidemaj, F.; Isaxon, C.; Abera, A.; Malmqvist, E. Indoor Air Pollution Exposure of Women in Adama, Ethiopia, and Assessment of Disease Burden Attributable to Risk Factor. Int. J. Env. Res. Public Health 2021, 18, 9859. [Google Scholar] [CrossRef]
- Yu, H. Solid Fuel-Related Indoor Air Pollution And Poor Sleep Quality In Adults Aged 45 Years And Older; A National Longitudinal Study in China. Master‘s Thesis, Yale, New Haven, CT, USA, January 2020. [Google Scholar]
- Luo, Y.; Zhong, Y.; Pang, L.; Zhao, Y.; Liang, R.; Zheng, X. The effects of indoor air pollution from solid fuel use on cognitive function among middle-aged and older population in China. Sci. Total Environ. 2021, 754, 142460. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Gao, Q.; Yang, D.; Hua, H.; Wang, N.; Ou, F.; Liu, R.; Wu, B.; Liu, Y. Association between biomass fuel use and risk of hypertension among Chinese older people: A cohort study. Environ. Int. 2020, 138, 105620. [Google Scholar] [CrossRef]
- Lin, L.; Wang, H.H.; Liu, Y.; Lu, C.; Chen, W.; Guo, V.Y. Indoor solid fuel use for heating and cooking with blood pressure and hypertension: A cross-sectional study among middle-aged and older adults in China. Indoor Air 2021, 31, 2158–2166. [Google Scholar] [CrossRef]
- Pan, M.; Gu, J.; Li, R.; Chen, H.; Liu, X.; Tu, R.; Chen, R.; Yu, S.; Mao, Z.; Huo, W.; et al. Independent and combined associations of solid-fuel use and smoking with obesity among rural Chinese adults. Environ. Sci. Pollut. Res. Int. 2021, 28, 33613–33622. [Google Scholar] [CrossRef]
- Deng, Y.; Gao, Q.; Yang, T.; Wu, B.; Liu, Y.; Liu, R. Indoor solid fuel use and incident arthritis among middle-aged and older adults in rural China: A nationwide population-based cohort study. Sci. Total Environ. 2021, 772, 145395. [Google Scholar] [CrossRef]
- Dutta, A.; Mukherjee, B.; Das, D.; Banerjee, A.; Ray, M.R. Hypertension with elevated levels of oxidized low-density lipoprotein and anticardiolipin antibody in the circulation of premenopausal Indian women chronically exposed to biomass smoke during cooking. Indoor Air 2011, 21, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Yu, Q.; Zuo, G. Relationship of indoor solid fuel use for cooking with blood pressure and hypertension among the elderly in China. Environ. Sci. Pollut. Res. 2022, 2022, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Wang, J.; Shen, Z.; Huang, Y.; Zhang, Y.; Niu, X.; Cao, J.; Zhang, Q.; Xu, H.; Zhang, N.; et al. Volatile organic compounds from residential solid fuel burning in Guanzhong Plain, China: Source-related profiles and risks. Chemosphere 2019, 221, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Idler, E.L.; Benyamini, Y. Self-rated health and mortality: A review of twenty-seven community studies. J. Health Soc. Behav. 1997, 38, 21–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jylha, M. What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Soc. Sci. Med. 2009, 69, 307–316. [Google Scholar] [CrossRef]
- Chen, F.; Yang, Y.; Liu, G. Social Change and Socioeconomic Disparities in Health over the Life Course in China: A Cohort Analysis. Am. Sociol. Rev. 2010, 75, 126–150. [Google Scholar] [CrossRef]
- Yi, Z.; Vaupel, J.W. Functional Capacity and Self-Evaluation of Health and Life of Oldest Old in China. J. Soc. Issues 2002, 58, 733–748. [Google Scholar] [CrossRef]
- Zeng, Y.; Feng, Q.; Hesketh, T.; Christensen, K.; Vaupel, J.W. Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in China: A cohort study. Lancet 2017, 389, 1619–1629. [Google Scholar] [CrossRef]
- Lv, X.; Li, W.; Ma, Y.; Chen, H.; Zeng, Y.; Yu, X.; Hofman, A.; Wang, H. Cognitive decline and mortality among community-dwelling Chinese older people. BMC Med. 2019, 17, 63. [Google Scholar] [CrossRef] [Green Version]
- Andresen, E.M.; Malmgren, J.A.; Carter, W.B.; Patrick, D.L. Screening for Depression in Well Older Adults: Evaluation of a Short Form of the CES-D. Am. J. Prev. Med. 1994, 10, 77–84. [Google Scholar] [CrossRef]
- Cheng, S.; Chan, A. The Center for Epidemiologic Studies Depression Scale in older Chinese: Thresholds for long and short forms. Int. J. Geriatr. Psychiatry 2010, 20, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Idler, E.; Cartwright, K. What Do We Rate When We Rate Our Health? Decomposing Age-related Contributions to Self-rated Health. J. Health Soc. Behav. 2018, 59, 74–93. [Google Scholar] [CrossRef] [PubMed]
- Engberg, I.; Segerstedt, J.; Waller, G.; Wennberg, P.; Eliasson, M. Fatigue in the general population- associations to age, sex, socioeconomic status, physical activity, sitting time and self-rated health: The northern Sweden MONICA study 2014. BMC Public Health 2017, 17, 654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer, O.L.; Castro-Schilo, L.; Aguilar-Gaxiola, S. Determinants of mental health and self-rated health: A model of socioeconomic status, neighborhood safety, and physical activity. Am. J. Public Health 2014, 104, 1734–1741. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Porritt, J.M.; Sufi, F.; Barlow, A.; Baker, S.R. The role of illness beliefs and coping in the adjustment to dentine hypersensitivity. J. Clin. Periodontol. 2014, 41, 60–69. [Google Scholar] [CrossRef]
- Li, C.; Zhou, Y.; Ding, L. Effects of long-term household air pollution exposure from solid fuel use on depression: Evidence from national longitudinal surveys from 2011 to 2018. Environ. Pollut. 2021, 283, 117350. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, X.; Yan, Z. Depression in the house: The effects of household air pollution from solid fuel use among the middle-aged and older population in China. Sci. Total Environ. 2020, 703, 134706. [Google Scholar] [CrossRef]
- Yu, H.; Luo, J.; Chen, K.; Pollitt, K.J.G.; Liew, Z. Solid fuels use for cooking and sleep health in adults aged 45 years and older in China. Sci. Rep. 2021, 11, 13304. [Google Scholar] [CrossRef]
- Chen, C.; Liu, G.G.; Sun, Y.; Gu, D.; Zhang, H.; Yang, H.; Lu, L.; Zhao, Y.; Yao, Y. Association between household fuel use and sleep quality in the oldest-old: Evidence from a propensity-score matched case-control study in Hainan, China. Environ. Res. 2020, 191, 110229. [Google Scholar] [CrossRef]
- Siddharthan, T.; Grigsby, M.R.; Goodman, D.; Chowdhury, M.; Rubinstein, A.; Irazola, V.; Gutierrez, L.; Miranda, J.J.; Bernabe-Ortiz, A.; Alam, D.; et al. Association between Household Air Pollution Exposure and Chronic Obstructive Pulmonary Disease Outcomes in 13 Low- and Middle-Income Country Settings. Am. J. Respir. Crit. Care Med. 2018, 197, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Block, M.L.; Calderón-Garciduenas, L. Air pollution: Mechanisms of neuroinflammation and CNS disease. Trends Neurosci. 2009, 32, 506–516. [Google Scholar] [CrossRef] [Green Version]
- Cao, L.; Zhao, Z.; Ji, C.; Xia, Y. Association between solid fuel use and cognitive impairment: A cross-sectional and follow-up study in a middle-aged and older Chinese population. Environ. Int. 2021, 146, 106251. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Y.; Yang, F.-A.; Lai, W. The impact of indoor air pollution on health outcomes and cognitive abilities: Empirical evidence from China. Popul. Environ. 2019, 40, 388–410. [Google Scholar] [CrossRef]
- Kaplan, G.A.; Goldberg, D.E.; Everson, S.A.; Cohen, R.D.; Salonen, R.; Tuomilehto, J.; Salonen, J. Perceived Health Status and Morbidity and Mortality: Evidence from the Kuopio Ischaemic Heart Disease Risk Factor Study. Int. J. Epidemiol. 1996, 25, 259–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balakrishnan, K.; Ramaswamy, P.; Sambandam, S.; Thangavel, G.; Ghosh, S.; Johnson, P.; Mukhopadhyay, K.; Venugopal, V.; Thanasekaraan, V. Air pollution from household solid fuel combustion in India: An overview of exposure and health related information to inform health research priorities. Glob. Health Action 2011, 4, 1–9. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variables | All (n = 7831) | Solid Fuel (n = 2317) | Clean Fuel (n = 5514) | p-Value |
|---|---|---|---|---|
| Age (years, mean, SD) | 82.70 (11.28) | 82.75 (11.22) | 82.68 (11.31) | 0.783 |
| Sex (n, %) | 0.024 | |||
| Male | 3682 (47.02) | 1044 (45.06) | 2638 (47.84) | |
| Female | 4149 (52.98) | 1273 (54.94) | 2876 (52.16) | |
| Marital status (n, %) | 0.024 | |||
| Not married | 3997 (51.04) | 1137 (49.07) | 2860 (51.87) | |
| Married | 3834 (48.96) | 1180 (50.93) | 2654 (48.13) | |
| Community Location (n, %) | <0.001 | |||
| Urban | 4383 (55.97) | 907 (39.15) | 3476 (63.04) | |
| Rural | 3448 (44.03) | 1410 (60.85) | 2038 (36.96) | |
| Education (n, %) | 3407 (43.51) | 1272 (54.90) | 2135 (38.72) | <0.001 |
| 0 | 2451 (31.30) | 421 (18.17) | 2030 (36.82) | |
| 1–6 | 1973 (25.19) | 624 (26.93) | 1349 (24.46) | |
| 7– | <0.001 | |||
| Income (n, %) | 2105 (26.88) | 1055 (45.53) | 1050 (19.04) | |
| 0–10,000 | 2633 (33.62) | 884 (38.15) | 1749 (31.72) | |
| 10,000–50,000 | 3093 (39.05) | 378 (16.31) | 2715 (49.24) | |
| ≥50,000 | ||||
| Smoking status (n, %) | <0.001 | |||
| Not current | 6503 (83.04) | 1871 (80.75) | 4632 (84.00) | |
| Current | 1328 (16.96) | 446 (19.25) | 882 (16.00) | |
| Alcohol use (n, %) | 0.049 | |||
| Not current | 6581 (84.04) | 1918 (82.78) | 4663 (84.57) | |
| Current | 1250 (15.96) | 399 (17.22) | 851 (15.43) | |
| Regular exercise (n, %) | <0.001 | |||
| Not current | 4957 (63.30) | 1759 (75.92) | 3198 (58.00) | |
| Current | 2874 (36.70) | 558 (24.08) | 2316 (42.00) | |
| Sleep quality (n, %) | <0.001 | |||
| Very poor | 160 (2.04) | 47 (2.03) | 113 (2.05) | |
| Poor | 926 (11.82) | 301 (12.99) | 625 (11.33) | |
| Moderate | 2471 (31.55) | 801 (34.57) | 1670 (30.29) | |
| Good | 2939 (37.53) | 854 (36.86) | 2085 (37.81) | |
| Very good | 1335 (17.05) | 314 (13.55) | 1021 (18.52) | |
| Cognitive abilities (mean, SD) | 20.44 (4.93) | 19.90 (5.29) | 20.67 (4.75) | <0.001 |
| Depression symptoms (mean, SD) | 22.87 (5.38) | 24.05 (5.44) | 22.37 (5.28) | <0.001 |
| SBP 1 (mmHg, mean, SD) | 139.50 (20.82) | 141.07 (21.56) | 138.84 (20.46) | <0.001 |
| BMI (kg/m2, mean, SD) | 22.67 (4.36) | 22.02 (3.92) | 22.94 (4.50) | <0.001 |
| Self-rated health (n, %) | <0.001 | |||
| Very poor | 63 (0.80) | 27 (1.17) | 36 (0.65) | |
| Poor | 857 (10.94) | 299 (12.90) | 558 (10.12) | |
| Fair | 2969 (37.91) | 949 (40.96) | 2020 (36.63) | |
| Good | 2892 (36.93) | 813 (35.09) | 2079 (37.70) | |
| Very good | 1050 (13.41) | 229 (9.88) | 821 (14.89) |
| Pathways | β 1 | SE | p-Value |
|---|---|---|---|
| Direct effects | |||
| Solid fuel→sleep quality | −0.056 | 0.026 | 0.030 |
| Solid fuel→cognitive abilities | −0.319 | 0.111 | 0.004 |
| Solid fuel→depression symptoms | 0.910 | 0.138 | <0.001 |
| Solid fuel→ systolic blood pressure | 1.001 | 0.556 | 0.068 |
| Solid fuel→body mass index | −0.733 | 0.111 | <0.001 |
| Solid fuel→self-rated health | −0.041 | 0.020 | 0.037 |
| Sleep quality→self-rated health | 0.250 | 0.009 | <0.001 |
| Cognitive abilities→self-rated health | 0.010 | 0.002 | <0.001 |
| Depression symptoms→self-rated health | −0.049 | 0.002 | <0.001 |
| Systolic blood pressure→self-rated health | 0.000 | 0.000 | 0.876 |
| Body mass index→self-rated health | 0.001 | 0.002 | 0.599 |
| Indirect effects | |||
| Solid fuel→sleep quality→self-rated health | −0.013 | 0.006 | 0.030 |
| Solid fuel→cognitive symptoms→self-rated health | −0.003 | 0.001 | 0.011 |
| Solid fuel→depression symptoms→self-rated health | −0.045 | 0.007 | <0.001 |
| Solid fuel→systolic blood pressure→self-rated health | 0.000 | 0.000 | 0.0877 |
| Solid fuel→body mass index→self-rated health | −0.001 | 0.002 | 0.600 |
| Total effects | |||
| Solid fuel→self-rated health | −0.107 | 0.022 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, Q.; Cheng, Y.; Li, W.; Zuo, G. Mediating Factors Explaining the Associations between Solid Fuel Use and Self-Rated Health among Chinese Adults 65 Years and Older: A Structural Equation Modeling Approach. Int. J. Environ. Res. Public Health 2022, 19, 6904. https://doi.org/10.3390/ijerph19116904
Yu Q, Cheng Y, Li W, Zuo G. Mediating Factors Explaining the Associations between Solid Fuel Use and Self-Rated Health among Chinese Adults 65 Years and Older: A Structural Equation Modeling Approach. International Journal of Environmental Research and Public Health. 2022; 19(11):6904. https://doi.org/10.3390/ijerph19116904
Chicago/Turabian StyleYu, Qiutong, Yuqing Cheng, Wei Li, and Genyong Zuo. 2022. "Mediating Factors Explaining the Associations between Solid Fuel Use and Self-Rated Health among Chinese Adults 65 Years and Older: A Structural Equation Modeling Approach" International Journal of Environmental Research and Public Health 19, no. 11: 6904. https://doi.org/10.3390/ijerph19116904
APA StyleYu, Q., Cheng, Y., Li, W., & Zuo, G. (2022). Mediating Factors Explaining the Associations between Solid Fuel Use and Self-Rated Health among Chinese Adults 65 Years and Older: A Structural Equation Modeling Approach. International Journal of Environmental Research and Public Health, 19(11), 6904. https://doi.org/10.3390/ijerph19116904