
Is Subjective Age Associated with Physical Fitness in Community-Dwelling Older Adults?


Abstract
1. Introduction
2. Materials and Methods
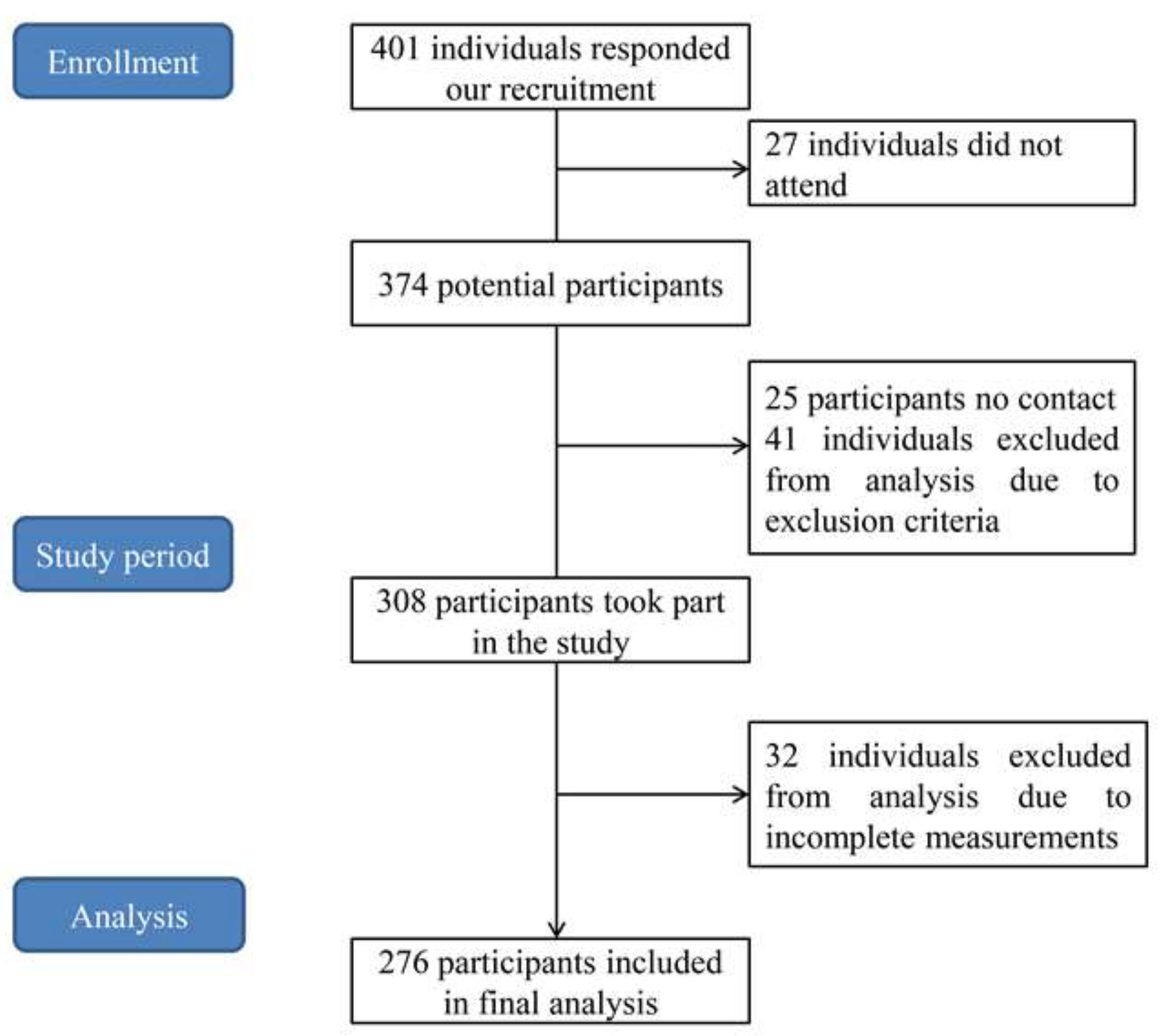
2.1. Participants
2.2. Procedures
2.3. Subjective Age Measurement
2.4. Physical Fitness Measurement
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Avila-Carvalho, L.; Klentrou, P.; Palomero, M.D.; Lebre, E. Anthropometric profiles and age at menarche in elite group rhythmic gymnasts according to their chronological age. Sci. Sport 2013, 28, 172–180. [Google Scholar] [CrossRef]
- Lentin, G.; Cumming, S.; Piscione, J.; Pezery, P.; Bouchouicha, M.; Gadea, J.; Raymond, J.J.; Duche, P.; Gavarry, O. A Comparison of an alternative weight-grading model against chronological age group model for the grouping of schoolboy male rugby players. Front. Physiol. 2021, 12, 670720. [Google Scholar] [CrossRef] [PubMed]
- Koolhaas, W.; van der Klink, J.J.L.; Groothoff, J.W.; Brouwer, S. Towards a sustainable healthy working life: Associations between chronological age, functional age and work outcomes. Eur. J. Public Health 2012, 22, 424–429. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zhao, X.G.; Huang, H.M.; Gu, Y.D. Age score for assessing motor function in Chinese community-dwelling older women. J. Women Aging 2022, 34, 170–180. [Google Scholar] [CrossRef]
- Zhao, X.G.; Huang, H.M.; Gu, Y.D.; Zhou, Z.X. Age score for assessing motor function in Chinese older men. J. Mens Health 2021, 17, 37–43. [Google Scholar]
- Deeg, D.J.H.; Timmermans, E.J.; Kok, A.A.L. Capturing subjective age, subjective life expectancy, and their links with older adults’ health: The Dutch Longitudinal Aging Study Amsterdam. J. Aging Health 2021, 33, 633–644. [Google Scholar] [CrossRef]
- Morris, E.P.; Zaheed, A.B.; Sharifian, N.; Sol, K.; Kraal, A.Z.; Zahodne, L.B. Subjective age, depressive symptoms, and cognitive functioning across five domains. J. Clin. Exp. Neuropsyc. 2021, 43, 310–323. [Google Scholar] [CrossRef]
- Bodner, E.; Shrira, A.; Hoffman, Y.; Bergman, Y.S. Day-to-day variability in subjective age and ageist attitudes and their association with depressive symptoms. J. Gerontol. B-Psychol. 2021, 76, 836–844. [Google Scholar] [CrossRef]
- Stephan, Y.; Sutin, A.R.; Bayard, S.; Terracciano, A. Subjective age and sleep in middle-aged and older adults. Psychol. Health 2017, 32, 1140–1151. [Google Scholar] [CrossRef]
- Shrira, A.; Palgi, Y.; Hoffman, Y.; Avidor, S.; Bodner, E.; Ben-Ezra, M.; Bensimon, M. Subjective age as a moderator in the reciprocal effects between posttraumatic stress disorder symptoms and self-rated physical functioning. Front. Psychol. 2018, 9, 1746. [Google Scholar] [CrossRef]
- Li, Y.X.; Liu, M.H.; Miyawaki, C.E.; Sun, X.C.; Hou, T.X.; Tang, S.Y.; Szanton, S.L. Bidirectional relationship between subjective age and frailty: A prospective cohort study. BMC Geriatr. 2021, 21, 395. [Google Scholar] [CrossRef] [PubMed]
- Stephan, Y.; Sutin, A.R.; Terracciano, A. Subjective age and mortality in three longitudinal samples. Psychosom. Med. 2018, 80, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Segel-Karpas, D.; Palgi, Y.; Shrira, A. The reciprocal relationship between depression and physical morbidity: The role of subjective age. Health Psychol. 2017, 36, 848–851. [Google Scholar] [CrossRef] [PubMed]
- Wettstein, M.; Spuling, S.M.; Cengia, A.; Nowossadeck, S. Feeling younger as a stress buffer: Subjective age moderates the effect of perceived stress on change in functional health. Psychol. Aging 2021, 36, 322–337. [Google Scholar] [CrossRef] [PubMed]
- Shao, J.J.; Zhang, L.; Xiao, L.X.; Li, X.Y.; Li, J.M. Subjective age and memory performance among older Chinese adults: A moderated mediation model. Int. J. Aging Hum. Dev. 2020, 91, 182–197. [Google Scholar] [CrossRef]
- Stephan, Y.; Sutin, A.R.; Wurm, S.; Terracciano, A. Subjective aging and incident cardiovascular disease. J. Gerontol. B-Psychol. 2021, 76, 910–919. [Google Scholar] [CrossRef]
- Rippon, I.; Steptoe, A. Is the relationship between subjective age, depressive symptoms and activities of daily living bidirectional? Soc. Sci. Med. 2018, 214, 41–48. [Google Scholar] [CrossRef]
- Daimiel, L.; Martinez-Gonzalez, M.A.; Corella, D.; Salas-Salvado, J.; Schroder, H.; Vioque, J.; Romaguera, D.; Martinez, J.A.; Warnberg, J.; Lopez-Miranda, J.; et al. Physical fitness and physical activity association with cognitive function and quality of life: Baseline cross-sectional analysis of the PREDIMED-Plus trial. Sci. Rep. 2020, 10, 3472. [Google Scholar] [CrossRef]
- Janssen, A.; Leahy, A.A.; Diallo, T.M.O.; Smith, J.J.; Kennedy, S.G.; Eather, N.; Mavilidi, M.F.; Wagemakers, A.; Babic, M.J.; Lubans, D.R. Cardiorespiratory fitness, muscular fitness and mental health in older adolescents: A multi-level cross-sectional analysis. Prev. Med. 2020, 132, 105985. [Google Scholar] [CrossRef]
- Hessert, M.J.; Gugliucci, M.R.; Pierce, H.R. Functional fitness: Maintaining or improving function for elders with chronic diseases. Fam. Med. 2005, 37, 472–476. [Google Scholar]
- Shen, B.; Bo, J.; Lu, X.Y. Profiles of health-related quality of life and their relationships with happiness, physical activity and physical fitness. Res. Q. Exerc. Sport 2020, 91, 260–269. [Google Scholar]
- Fogelholm, M. Physical activity, fitness and fatness: Relations to mortality, morbidity and disease risk factors. A systematic review. Obes. Rev. 2010, 11, 202–221. [Google Scholar] [CrossRef] [PubMed]
- Stephan, Y.; Sutin, A.R.; Terracciano, A. “Feeling younger, walking faster”: Subjective age and walking speed in older adults. Age 2015, 37, 86. [Google Scholar] [CrossRef] [PubMed]
- Stephan, Y.; Chalabaev, A.; Kotter-Grühn, D.; Jaconelli, A. “Feeling younger, being stronger”: An experimental study of subjective age and physical functioning among older adults. J. Gerontol. Ser. B Psychol. Sci. Soc. 2013, 68, 1–7. [Google Scholar] [CrossRef]
- Dietze-Hermosa, M.; Montalvo, S.; Gonzalez, M.P.; Dorgo, S. Physical fitness in older adults: Is there a relationship with the modified Functional Movement Screen™? J. Bodyw. Mov. Ther. 2021, 25, 28–34. [Google Scholar] [CrossRef]
- Lin, P.S.; Hsieh, C.C.; Cheng, H.S.; Tseng, T.J.; Su, S.C. Association between physical fitness and successful aging in Taiwanese older adults. PLoS ONE 2016, 11, e0150389. [Google Scholar] [CrossRef]
- Chan, D.C.; Lee, W.T.; Lo, D.H.; Leung, J.C.; Kwok, A.W.; Leung, P.C. Relationship between grip strength and bone mineral density in healthy Hong Kong adolescents. Osteoporos. Int. 2008, 19, 1485–1495. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, W.; Liu, T.; Zhang, D. Association of grip strength with risk of all-cause mortality, cardiovascular diseases, and cancer in community-dwelling populations: A meta-analysis of prospective cohort studies. J. Am. Med. Dir. Assoc. 2017, 18, e17–e551. [Google Scholar] [CrossRef]
- Shinohara, T.; Saida, K.; Miyata, K.; Usuda, S. The balance function is associated with frailty in community-dwelling older women. Int. J. Rehabil. Res. 2021, 44, 51–56. [Google Scholar] [CrossRef]
- Yu, R.; Tong, C.; Ho, F.; Woo, J. Effects of a multicomponent frailty prevention program in prefrail community-dwelling older persons: A randomized controlled trial. J. Am. Med. Dir. Assoc. 2020, 21, 294.e1–294.e10. [Google Scholar] [CrossRef]
- Parentoni, A.N.; Mendonça, V.A.; Dos Santos, K.D.; Sá, L.F.; Ferreira, F.O.; Gomes Pereira, D.A.; Lustosa, L.P. Gait speed as a predictor of respiratory muscle function, strength, and frailty syndrome in community-dwelling elderly people. J. Frailty Aging 2015, 4, 64–68. [Google Scholar] [CrossRef] [PubMed]
- De la Cámara, M.Á.; Higueras-Fresnillo, S.; Sadarangani, K.P.; Esteban-Cornejo, I.; Martinez-Gomez, D.; Veiga, Ó.L. Clinical and ambulatory gait speed in older adults: Associations with several physical, mental, and cognitive health outcomes. Phys. Ther. 2020, 100, 718–727. [Google Scholar] [CrossRef] [PubMed]
- Notthoff, N.; Drewelies, J.; Kazanecka, P.; Steinhagen-Thiessen, E.; Norman, K.; Düzel, S.; Daumer, M.; Lindenberger, U.; Demuth, I.; Gerstorf, D. Feeling older, walking slower-but only if someone’s watching. Subjective age is associated with walking speed in the laboratory, but not in real life. Eur. J. Ageing 2018, 15, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Zhong, Q.; Ji, J.; Ma, J.; Wu, H.; Gao, Y.; Ali, N.; Wang, T. Effects of aerobic dance on cognition in older adults with mild cognitive impairment: A systematic review and meta-analysis. J. Alzheimers Dis. 2020, 74, 679–690. [Google Scholar] [CrossRef] [PubMed]
- Maillot, P.; Perrot, A.; Hartley, A. Effects of interactive physical-activity video-game training on physical and cognitive function in older adults. Psychol. Aging 2012, 27, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Koh, Y.; Oh, Y.; Park, H.; Kim, W.; Park, E.C. The relationship between physical exercise and cognitive function in Korean middle aged and elderly adults without dementia. Int. J. Environ. Res. Public Health 2020, 17, 8821. [Google Scholar] [CrossRef] [PubMed]
- Engeseth, K.; Prestgaard, E.E.; Mariampillai, J.E.; Grundvold, I.; Liestol, K.; Kjeldsen, S.E.; Bodegard, J.; Erikssen, J.E.; Gjesdal, K.; Skretteberg, P.T. Physical fitness is a modifiable predictor of early cardiovascular death: A 35-year follow-up study of 2014 healthy middle-aged men. Eur. J. Prev. Cardiol. 2018, 25, 1655–1663. [Google Scholar] [CrossRef]
- Leirós-Rodríguez, R.; Romo-Pérez, V.; Pérez-Ribao, I.; García-Soidán, J.L. A comparison of three physical activity programs for health and fitness tested with older women: Benefits of aerobic activity, aqua fitness, and strength training. J. Women Aging 2019, 31, 419–431. [Google Scholar] [CrossRef]
- Mendonca, G.V.; Pezarat-Correia, P.; Vaz, J.R.; Silva, L.; Almeida, I.D.; Heffernan, K.S. Impact of exercise training on physiological measures of physical fitness in the elderly. Curr. Aging Sci. 2016, 9, 240–259. [Google Scholar] [CrossRef]
- Zhao, X.; Hu, F. Relationship between physical fitness, anthropometric measurement, and bone health in adult men. Clin. Nurs. Res. 2021, 1–9. [Google Scholar] [CrossRef]
- Zhao, X.; Hu, F. Effect of telling older adults their predictive physical fitness age on physical activity: A quasi-experimental study. Health Soc. Care Community 2022, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Denche-Zamorano, Á.; Mendoza-Muñoz, M.; Carlos-Vivas, J.; Muñoz-Bermejo, L.; Rojo-Ramos, J.; Pastor-Cisneros, R.; Giakoni-Ramírez, F.; Godoy-Cumillaf, A.; Barrios-Fernandez, S. A cross-sectional study on self-perceived health and physical activity level in the Spanish population. Int. J. Environ. Res. Public Health 2022, 19, 5656. [Google Scholar] [CrossRef] [PubMed]
- Kotter-Grühn, D.; Kornadt, A.E.; Stephan, Y. Looking beyond chronological age: Current knowledge and future directions in the study of subjective age. Gerontology 2016, 62, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Gilleard, C. Age, subjectivity and the concept of subjective age: A critique. J. Aging Stud. 2022, 60, 101001. [Google Scholar] [CrossRef] [PubMed]
- Wahl, H.W.; Drewelies, J.; Duezel, S.; Lachman, M.E.; Smith, J.; Eibich, P.; Steinhagen-Thiessen, E.; Demuth, I.; Lindenberger, U.; Wagner, G.G.; et al. Subjective age and attitudes toward own aging across two decades of historical time. Psychol. Aging 2022, 37, 413–429. [Google Scholar] [CrossRef]


{kind=link}
| Older Men | Older Women | Overall | |
|---|---|---|---|
| Numbers (n) | 94 | 182 | 276 |
| Chronological age (years) | 71.21 ± 5.04 | 70.71 ± 4.82 | 70.88 ± 4.89 |
| Subjective age (years) | 69.09 ± 7.77 | 69.85 ± 7.11 | 69.59 ± 7.33 |
| Age discrepancy (scores) | 0.03 ± 0.06 | 0.01 ± 0.05 | 0.02 ± 0.05 |
| Grip strength (kg) | 37.20 ± 5.68 | 24.24 ± 4.34 | 28.66 ± 7.82 |
| Balancing on one leg with eyes open (s) | 43.09 ± 20.12 | 43.08 ± 22.47 | 43.08 ± 21.66 |
| 30 s chair stand test (repetitions/30 s) | 20.91 ± 4.96 | 20.05 ± 5.44 | 20.35 ± 5.29 |
| 4 m habitual walk (s) | 2.96 ± 0.46 | 3.05 ± 1.16 | 3.02 ± 0.98 |
| 6 min walk test (m) | 605.50 ± 62.45 | 556.51 ± 84.65 | 573.19 ± 81.09 |
| ① Felt Younger Group | ② Felt the Same Group | ③ Felt Older Group | p Values ① vs. ② | p Values ① vs. ③ | p Values ② vs. ③ | |
|---|---|---|---|---|---|---|
| Older men | ||||||
| Grip strength (kg) | 39.98 ± 4.48 | 35.80 ± 5.61 | 33.83 ± 5.27 | 0.039 | <0.001 | 0.746 |
| Balancing on one leg with eyes open (s) | 50.73 ± 17.50 | 37.82 ± 21.08 | 34.27 ± 19.53 | 0.125 | <0.001 | 1.000 |
| 30 s chair stand test (repetitions/30 s) | 23.92 ± 4.22 | 20.09 ± 4.32 | 17.06 ± 2.98 | 0.010 | <0.001 | 0.071 |
| 4 m habitual walk (s) | 2.80 ± 0.40 | 3.27 ± 0.44 | 3.08 ± 0.47 | 0.005 | 0.013 | 0.675 |
| 6 min walk test (m) | 641.85 ± 37.53 | 598.27 ± 47.73 | 557.91 ± 61.95 | 0.028 | <0.001 | 0.059 |
| Older women | ||||||
| Grip strength (kg) | 26.79 ± 3.59 | 23.57 ± 3.89 | 22.42 ± 4.09 | <0.001 | <0.001 | 0.442 |
| Balancing on one leg with eyes open (s) | 56.37 ± 10.43 | 38.17 ± 24.65 | 34.14 ± 23.72 | <0.001 | <0.001 | 0.983 |
| 30 s chair stand test (repetitions/30 s) | 23.79 ± 4.93 | 17.94 ± 4.51 | 17.85 ± 4.46 | <0.001 | <0.001 | 1.000 |
| 4 m habitual walk (s) | 2.75 ± 0.41 | 3.12 ± 0.65 | 3.26 ± 1.61 | 0.374 | 0.020 | 1.000 |
| 6 min walk test (m) | 613.77 ± 44.67 | 548.85 ± 97.92 | 512.35 ± 76.58 | <0.001 | <0.001 | 0.040 |
| B | SE | Beta | t | p Values | |
|---|---|---|---|---|---|
| Older men | |||||
| (Constant) | −0.257 | 0.045 | - | −5.726 | <0.001 |
| Grip strength | 0.003 | 0.001 | 0.247 | 3.974 | <0.001 |
| Balancing on one leg with eyes open | 0.001 | 0.000 | 0.190 | 3.142 | 0.002 |
| 30-s chair stand test | 0.005 | 0.001 | 0.387 | 5.666 | <0.001 |
| 4-m habitual walk | −0.025 | 0.007 | −0.202 | −3.518 | 0.001 |
| 6-min walk test | 0.001 | 0.000 | 0.268 | 4.044 | <0.001 |
| R2 = 0.85, Adjusted R2 = 0.71, F = 46.35, p < 0.001 | |||||
| Older women | |||||
| (Constant) | −0.206 | 0.023 | - | -9.032 | <0.001 |
| Grip strength | 0.003 | 0.001 | 0.295 | 5.270 | <0.001 |
| Balancing on one leg with eyes open | 0.001 | 0.000 | 0.145 | 2.474 | 0.014 |
| 30-s chair stand test | 0.003 | 0.001 | 0.356 | 6.053 | <0.001 |
| 4-m habitual walk | −0.002 | 0.002 | −0.050 | −0.941 | 0.348 |
| 6-min walk test | 0.001 | 0.000 | 0.211 | 3.376 | 0.001 |
| R2 = 0.54, Adjusted R2 = 0.53, F = 41.16, p < 0.001 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.; Yu, J.; Zhao, X. Is Subjective Age Associated with Physical Fitness in Community-Dwelling Older Adults? Int. J. Environ. Res. Public Health 2022, 19, 6841. https://doi.org/10.3390/ijerph19116841
Wang J, Yu J, Zhao X. Is Subjective Age Associated with Physical Fitness in Community-Dwelling Older Adults? International Journal of Environmental Research and Public Health. 2022; 19(11):6841. https://doi.org/10.3390/ijerph19116841
Chicago/Turabian StyleWang, Jin, Jiabin Yu, and Xiaoguang Zhao. 2022. "Is Subjective Age Associated with Physical Fitness in Community-Dwelling Older Adults?" International Journal of Environmental Research and Public Health 19, no. 11: 6841. https://doi.org/10.3390/ijerph19116841
APA StyleWang, J., Yu, J., & Zhao, X. (2022). Is Subjective Age Associated with Physical Fitness in Community-Dwelling Older Adults? International Journal of Environmental Research and Public Health, 19(11), 6841. https://doi.org/10.3390/ijerph19116841