
Bone Metastases of Endometrial Carcinoma Treated by Surgery: A Report on 13 Patients and a Review of the Medical Literature

Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Follow Up
2.3. Data Collection
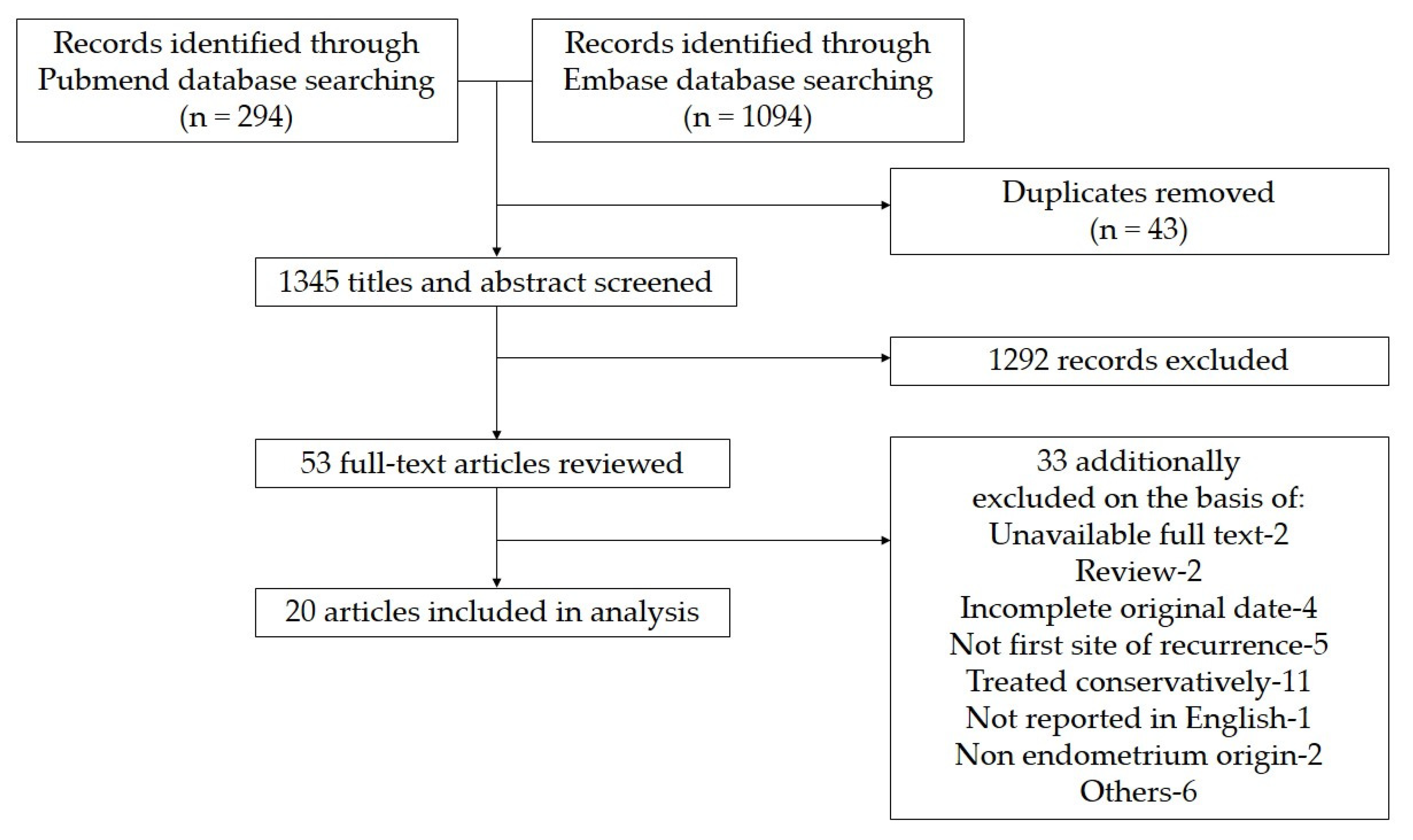
2.4. Literature Research
2.4.1. Search Strategy
2.4.2. Inclusion and Exclusion Criteria
2.4.3. Data Extraction and Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Characteristics of Bone Metastasis
3.3. Literature Review
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, J.; Zhang, L.; Jiang, W.; Zhang, R.; Zhang, B.; Silayiding, A.; Duan, X. MicroRNA-135a promotes proliferation, migration, invasion and induces chemoresistance of endometrial cancer cells. Eur. J. Obstet. Gynecol. Reprod. Biol. X 2020, 5, 100103. [Google Scholar] [CrossRef] [PubMed]
- Aalders, J.G.; Abeler, V.; Kolstad, P. Recurrent adenocarcinoma of the endometrium: A clinical and histopathological study of 379 patients. Gynecol. Oncol. 1984, 17, 85–103. [Google Scholar] [CrossRef]
- Fujimoto, T.; Nanjyo, H.; Fukuda, J.; Nakamura, A.; Mizunuma, H.; Yaegashi, N.; Sugiyama, T.; Kurachi, H.; Sato, A.; Tanaka, T. Endometrioid uterine cancer: Histopathological risk factors of local and distant recurrence. Gynecol. Oncol. 2009, 112, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Kaya, A.; Olmezoglu, A.; Eren, C.S.; Bayol, U.; Altay, T.; Karapinar, L.; Ozturk, H.; Oztekin, D.; Guvenli, Y.; Karadogan, I. Solitary bone metastasis in the tibia as a presenting sign of endometrial adenocarcinoma: A case report and the review of the literature. Clin. Exp. Metastasis 2007, 24, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Albareda, J.; Herrera, M.; Lopez Salva, A.; Garcia Donas, J.; Gonzalez, R. Sacral metastasis in a patient with endometrial cancer: Case report and review of the literature. Gynecol. Oncol. 2008, 111, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Jiang, G.Q.; Gao, Y.N.; Gao, M.; Zheng, H.; Yan, X.; Wang, W.; An, N.; Cao, K. Clinicopathological features and treatment of extremity bone metastasis in patients with endometrial carcinoma: A case report and review. Chin. Med. J. 2011, 124, 622–626. [Google Scholar]
- Hoshi, M.; Takada, J.; Ieguchi, M.; Takahashi, S.; Nakamura, H. Prognostic factors for patients with solitary bone metastasis. Int. J. Clin. Oncol. 2013, 18, 164–169. [Google Scholar] [CrossRef]
- Ravault, P.P.; Lejeune, E.; Bouvier, M.; Vauzelle, J.L.; Ricard, R.; Bochu, M.; Jeanneret, J. Isolated metastasis of the tarsal scaphoid bone in the course of cancer of the uterine body. Rev. Rhum. Mal. Osteo-Articul. 1967, 34, 650–654. [Google Scholar]
- Petru, E.; Malleier, M.; Lax, S.; Lahousen, M.; Ehall, R.; Pickel, H.; Winter, R. Solitary metastasis in the tarsus preceding the diagnosis of primary endometrial cancer. A case report. Eur. J. Gynaecol. Oncol. 1995, 16, 387–391. [Google Scholar]
- Clarke, S.J.; Smith, T.P. Metastatic endometrial carcinoma of the foot. A case report. J. Am. Podiatr. Med. Assoc. 1996, 86, 331–333. [Google Scholar] [CrossRef]
- Mustafa, M.S.; Al-Nuaim, L.; Inayat-Ur-Rahman, N. Scalp and cranial bone metastasis of endometrial carcinoma: A case report and literature review. Gynecol. Oncol. 2001, 81, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Neto, A.G.; Gupta, D.; Broaddus, R.; Malpica, A. Endometrial endometrioid adenocarcinoma in a premenopausal woman presenting with metastasis to bone: A case report and review of the literature. Int. J. Gynecol. Pathol. Off. J. Int. Soc. Gynecol. Pathol. 2002, 21, 281–284. [Google Scholar] [CrossRef] [PubMed]
- Arnold, J.; Charters, D.; Perrin, L. Prolonged survival time following initial presentation with bony metastasis in stage IVb endometrial carcinoma. Aust. N. Z. J. Obstet. Gynaecol. 2003, 43, 239–240. [Google Scholar] [CrossRef] [PubMed]
- Ali, Z.A.; Wimhurst, J.A.; Ali, A.A.; Tempest, M.E.; Edwards, D.J. Endometrial cancer metastasis presenting as a grossly swollen toe. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2003, 13, 909–911. [Google Scholar] [CrossRef]
- Haraguchi, S.; Hioki, M.; Hisayoshi, T.; Yamashita, K.; Koizumi, K.; Shimizu, K. Resection of sternal metastasis from endometrial carcinoma followed by reconstruction with sandwiched marlex and stainless steel mesh: Report of a case. Surg. Today 2006, 36, 184–186. [Google Scholar] [CrossRef]
- Uharcek, P.; Mlyncek, M.; Ravinger, J. Endometrial adenocarcinoma presenting with an osseous metastasis. Gynecol. Obstet. Investig. 2006, 61, 200–202. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.; Peng, Z.; Gao, Y. Bilateral femur metastasis in endometrial adenocarcinoma. Saudi Med. J. 2008, 29, 766–769. [Google Scholar]
- Pakos, E.E.; Gartzonikas, D.N.; Tsekeris, P.G.; Xenakis, T.A. Solitary tibial osteolytic lesion. Case Rep. Med. 2009, 2009, 352085. [Google Scholar] [CrossRef]
- Chan, V.; Lau, J.; Rubens, F.D.; Dennie, C.; Ruel, M. Malignant invasion of sternotomy incision after cardiac operation. Ann. Thorac. Surg. 2010, 89, 1295–1296. [Google Scholar] [CrossRef]
- Kehoe, S.M.; Zivanovic, O.; Ferguson, S.E.; Barakat, R.R.; Soslow, R.A. Clinicopathologic features of bone metastases and outcomes in patients with primary endometrial cancer. Gynecol. Oncol. 2010, 117, 229–233. [Google Scholar] [CrossRef]
- Vizzielli, G.; Fanfani, F.; Costantini, B.; Gallotta, V.; Scambia, G.; Fagotti, A. External hemipelvectomy as treatment for solitary coxofemoral metastasis from endometrial carcinoma: Case report and review of the literature. J. Obstet. Gynaecol. Res. 2012, 38, 892–898. [Google Scholar] [CrossRef] [PubMed]
- Uccella, S.; Morris, J.M.; Bakkum-Gamez, J.N.; Keeney, G.L.; Podratz, K.C.; Mariani, A. Bone metastases in endometrial cancer: Report on 19 patients and review of the medical literature. Gynecol. Oncol. 2013, 130, 474–482. [Google Scholar] [CrossRef] [PubMed]
- Myriokefalitaki, E.; D’Costa, D.; Smith, M.; Ahmed, A.S. Primary bone metastasis as initial presentation of endometrial cancer (stage IVb). Arch. Gynecol. Obstet. 2013, 288, 739–746. [Google Scholar] [CrossRef]
- Kimyon, G.; Karalok, A.; Basaran, D.; Ureyen, I.; Celik, M.; Tasci, T.; Tulunay, G.; Turan, T. Bone recurrence rarely seen in endometrial cancer and review of the literature. J. Obstet. Gynaecol. Res. 2016, 42, 602–611. [Google Scholar] [CrossRef] [PubMed]
- Makris, G.M.; Mene, J.; Battista, M.J.; Chrelias, G.; Sergentanis, T.N.; Psyrri, A.; Chrelias, C. Endometrial carcinoma with tibial bone metastasis: A case report and literature review. J. Obstet. Gynaecol. J. Inst. Obstet. Gynaecol. 2018, 38, 1039–1047. [Google Scholar] [CrossRef]
- Abdul-Karim, F.W.; Kida, M.; Wentz, W.B.; Carter, J.R.; Sorensen, K.; Macfee, M.; Zika, J.; Makley, J.T. Bone metastasis from gynecologic carcinomas: A clinicopathologic study. Gynecol. Oncol. 1990, 39, 108–114. [Google Scholar] [CrossRef]
- Yoon, A.; Choi, C.H.; Kim, T.H.; Choi, J.K.; Park, J.Y.; Lee, Y.Y.; Kim, T.J.; Lee, J.W.; Bae, D.S.; Kim, B.G. Bone metastasis in primary endometrial carcinoma: Features, outcomes, and predictors. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2014, 24, 107–112. [Google Scholar] [CrossRef]
- Takeshita, S.; Todo, Y.; Matsumiya, H.; Okamoto, K.; Yamashiro, K.; Kato, H. A prediction model of survival for patients with bone metastasis from uterine corpus cancer. Jpn. J. Clin. Oncol. 2016, 46, 973–978. [Google Scholar] [CrossRef]
- Cooper, J.K.; Wong, F.L.; Swenerton, K.D. Endometrial adenocarcinoma presenting as an isolated calcaneal metastasis. A rare entity with good prognosis. Cancer 1994, 73, 2779–2781. [Google Scholar] [CrossRef]
- Litton, G.J.; Ward, J.H.; Abbott, T.M.; Williams, H.J., Jr. Isolated calcaneal metastasis in a patient with endometrial adenocarcinoma. Cancer 1991, 67, 1979–1983. [Google Scholar] [CrossRef]
- Peterson, J.J. F-18 FDG-PET for detection of osseous metastatic disease and staging, restaging, and monitoring response to therapy of musculoskeletal tumors. Semin. Musculoskelet. Radiol. 2007, 11, 246–260. [Google Scholar] [CrossRef] [PubMed]
- Mariani, A.; Webb, M.J.; Keeney, G.L.; Calori, G.; Podratz, K.C. Hematogenous dissemination in corpus cancer. Gynecol. Oncol. 2001, 80, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Kandoth, C.; Schultz, N.; Cherniack, A.D.; Akbani, R.; Liu, Y.; Shen, H.; Robertson, A.G.; Pashtan, I.; Shen, R.; Benz, C.C.; et al. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [PubMed]
- Bosse, T.; Nout, R.A.; McAlpine, J.N.; McConechy, M.K.; Britton, H.; Hussein, Y.R.; Gonzalez, C.; Ganesan, R.; Steele, J.C.; Harrison, B.T.; et al. Molecular Classification of Grade 3 Endometrioid Endometrial Cancers Identifies Distinct Prognostic Subgroups. Am. J. Surg. Pathol. 2018, 42, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Cosgrove, C.M.; Tritchler, D.L.; Cohn, D.E.; Mutch, D.G.; Rush, C.M.; Lankes, H.A.; Creasman, W.T.; Miller, D.S.; Ramirez, N.C.; Geller, M.A.; et al. An NRG Oncology/GOG study of molecular classification for risk prediction in endometrioid endometrial cancer. Gynecol. Oncol. 2018, 148, 174–180. [Google Scholar] [CrossRef]
- Kommoss, S.; McConechy, M.K.; Kommoss, F.; Leung, S.; Bunz, A.; Magrill, J.; Britton, H.; Kommoss, F.; Grevenkamp, F.; Karnezis, A.; et al. Final validation of the ProMisE molecular classifier for endometrial carcinoma in a large population-based case series. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2018, 29, 1180–1188. [Google Scholar] [CrossRef]
- Talhouk, A.; McConechy, M.K.; Leung, S.; Li-Chang, H.H.; Kwon, J.S.; Melnyk, N.; Yang, W.; Senz, J.; Boyd, N.; Karnezis, A.N.; et al. A clinically applicable molecular-based classification for endometrial cancers. Br. J. Cancer 2015, 113, 299–310. [Google Scholar] [CrossRef]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2021, 31, 12–39. [Google Scholar] [CrossRef]
- Travaglino, A.; Raffone, A.; Stradella, C.; Esposito, R.; Moretta, P.; Gallo, C.; Orlandi, G.; Insabato, L.; Zullo, F. Impact of endometrial carcinoma histotype on the prognostic value of the TCGA molecular subgroups. Arch. Gynecol. Obstet. 2020, 301, 1355–1363. [Google Scholar] [CrossRef]
- Wortman, B.G.; Bosse, T.; Nout, R.A.; Lutgens, L.C.H.W.; van der Steen-Banasik, E.M.; Westerveld, H.; van den Berg, H.; Slot, A.; De Winter, K.A.J.; Verhoeven-Adema, K.W.; et al. Molecular-integrated risk profile to determine adjuvant radiotherapy in endometrial cancer: Evaluation of the pilot phase of the PORTEC-4a trial. Gynecol. Oncol. 2018, 151, 69–75. [Google Scholar] [CrossRef]
- Soumerai, T.E.; Donoghue, M.T.A.; Bandlamudi, C.; Srinivasan, P.; Chang, M.T.; Zamarin, D.; Cadoo, K.A.; Grisham, R.N.; O’Cearbhaill, R.E.; Tew, W.P.; et al. Clinical Utility of Prospective Molecular Characterization in Advanced Endometrial Cancer. Clin. Cancer Res. 2018, 24, 5939–5947. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.R.; Cooper, K.; Croce, S.; Djordevic, B.; Herrington, S.; Howitt, B.; Hui, P.; Ip, P.; Koebel, M.; Lax, S.; et al. International Society of Gynecological Pathologists (ISGyP) Endometrial Cancer Project: Guidelines From the Special Techniques and Ancillary Studies Group. Int. J. Gynecol. Pathol. Off. J. Int. Soc. Gynecol. Pathol. 2019, 38 (Suppl. 1), S114–S122. [Google Scholar] [CrossRef] [PubMed]
- Stelloo, E.; Nout, R.A.; Osse, E.M.; Jürgenliemk-Schulz, I.J.; Jobsen, J.J.; Lutgens, L.C.; van der Steen-Banasik, E.M.; Nijman, H.W.; Putter, H.; Bosse, T.; et al. Improved Risk Assessment by Integrating Molecular and Clinicopathological Factors in Early-stage Endometrial Cancer-Combined Analysis of the PORTEC Cohorts. Clin. Cancer Res. 2016, 22, 4215–4224. [Google Scholar] [CrossRef]
- He, D.; Wang, H.; Dong, Y.; Zhang, Y.; Zhao, J.; Lv, C.; Zheng, X.; Li, D.; Li, T. POLE mutation combined with microcystic, elongated and fragmented (MELF) pattern invasion in endometrial carcinomas might be associated with poor survival in Chinese women. Gynecol. Oncol. 2020, 159, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Loukovaara, M.; Pasanen, A.; Bützow, R. Mismatch repair protein and MLH1 methylation status as predictors of response to adjuvant therapy in endometrial cancer. Cancer Med. 2021, 10, 1034–1042. [Google Scholar] [CrossRef]
- Pasanen, A.; Loukovaara, M.; Bützow, R. Clinicopathological significance of deficient DNA mismatch repair and MLH1 promoter methylation in endometrioid endometrial carcinoma. Mod. Pathol. 2020, 33, 1443–1452. [Google Scholar] [CrossRef]
- Raffone, A.; Travaglino, A.; Raimondo, D.; Neola, D.; Maletta, M.; Santoro, A.; Insabato, L.; Casadio, P.; Fanfani, F.; Zannoni, G.F.; et al. Lymphovascular space invasion in endometrial carcinoma: A prognostic factor independent from molecular signature. Gynecol. Oncol. 2022, 165, 192–197. [Google Scholar] [CrossRef]
- Nguyen, M.L.; Lafargue, C.J.; Pua, T.L.; Tedjarati, S.S. Grade 1 endometrioid endometrial carcinoma presenting with pelvic bone metastasis: A case report and review of the literature. Case Rep. Obstet. Gynecol. 2013, 2013, 807205. [Google Scholar] [CrossRef]
- Rove, K.O.; Crawford, E.D. Evolution of treatment options for patients with CRPC and bone metastases: Bone-targeted agents that go beyond palliation of symptoms to improve overall survival. Oncology 2011, 25, 1362–1370, 1375–1381, 1387. [Google Scholar]
- Schöls, W.A.; Kock, H.C.; van Etten, F.H. Recurrent endometrial adenocarcinoma presenting as a solitary humeral metastasis. Gynecol. Oncol. 1995, 59, 148–150. [Google Scholar] [CrossRef]
- Fuller, A.F., Jr.; Scannell, J.G.; Wilkins, E.W., Jr. Pulmonary resection for metastases from gynecologic cancers: Massachusetts General Hospital experience, 1943–1982. Gynecol. Oncol. 1985, 22, 174–180. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA A Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.L.; Hsiao, S.M.; Lin, M.C.; Lin, H.H. Bone metastasis as the initial presentation in one case of ovarian cancer with two components of endometrioid adenocarcinoma and adenosarcoma. Taiwan. J. Obstet. Gynecol. 2009, 48, 298–301. [Google Scholar] [CrossRef]
- Zhang, M.; Sun, J. Bone metastasis from ovarian cancer. Clinical analysis of 26 cases. Saudi Med. J. 2013, 34, 1270–1273. [Google Scholar] [PubMed]
- Reed, E.; Zerbe, C.S.; Brawley, O.W.; Bicher, A.; Steinberg, S.M. Analysis of autopsy evaluations of ovarian cancer patients treated at the National Cancer Institute, 1972–1988. Am. J. Clin. Oncol. 2000, 23, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Sehouli, J.; Olschewski, J.; Schotters, V.; Fotopoulou, C.; Pietzner, K. Prognostic role of early versus late onset of bone metastasis in patients with carcinoma of the ovary, peritoneum and fallopian tube. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2013, 24, 3024–3028. [Google Scholar] [CrossRef]
- Friedlander, M.; Grogan, M. Guidelines for the treatment of recurrent and metastatic cervical cancer. Oncologist 2002, 7, 342–347. [Google Scholar] [CrossRef]
- Matsuyama, T.; Tsukamoto, N.; Imachi, M.; Nakano, H. Bone metastasis from cervix cancer. Gynecol. Oncol. 1989, 32, 72–75. [Google Scholar] [CrossRef]
- Makino, H.; Nishio, S.; Tsubamoto, H.; Shimada, M.; Nishikawa, R.; Kai, K.; Ito, K.; Mizuno, T.; Ushijima, K.; Morishige, K. Treatment and prognosis of bone metastasis from cervical cancer (KCOG-G1202s). J. Obstet. Gynaecol. Res. 2016, 42, 701–706. [Google Scholar] [CrossRef]
- Balachandran, V.P.; Gonen, M.; Smith, J.J.; DeMatteo, R.P. Nomograms in oncology: More than meets the eye. Lancet Oncol. 2015, 16, e173–e180. [Google Scholar] [CrossRef]
- Vargas, R.; Rauh-Hain, J.A.; Clemmer, J.; Clark, R.M.; Goodman, A.; Growdon, W.B.; Schorge, J.O.; Del Carmen, M.G.; Horowitz, N.S.; Boruta, D.M., 2nd. Tumor size, depth of invasion, and histologic grade as prognostic factors of lymph node involvement in endometrial cancer: A SEER analysis. Gynecol. Oncol. 2014, 133, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Dursun, P.; Gültekin, M.; Yüce, K.; Ayhan, A. Skeletal carcinomatosis in endometrial clear cell carcinoma at initial presentation: A case report. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2006, 16, 891–895. [Google Scholar] [CrossRef] [PubMed]
- Shigemitsu, A.; Furukawa, N.; Koike, N.; Kobayashi, H. Endometrial cancer diagnosed by the presence of bone metastasis and treated with zoledronic Acid: A case report and review of the literature. Case Rep. Oncol. 2010, 3, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Ji, T.; Eskander, R.; Wang, Y.; Sun, K.; Hoang, B.H.; Guo, W. Can surgical management of bone metastases improve quality of life among women with gynecologic cancer? World J. Surg. 2014, 12, 250. [Google Scholar] [CrossRef]


{kind=link}
| Pt. No. | Age (Years) | Histology, Grade, Stage | Symptoms at Presentation | CA-125 (u/mL) | Interval to Bone Met (Months) | No. of Bone Met | Side | Localization | Extraosseous Met | Palliative Surgical Resection | Adjuvant Therapy after Surgery | Status | Survival after Bone Met (Months) | VAS (Pre/Post-Operative) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 45 | ADK,G2,IV | pain | 84.62 | 9 | 1 | Median | T12 | Skin | Reconstruction | / | Dead | 1 | 7/3 |
| 2 | 54 | ADK,NA,NA | Pain | NA | 38 | 1 | Median | L2 | No | Reconstruction | / | Dead | 20 | 4/1 |
| 3 | 58 | Clear cell,G3,II | Pain | NA | 48 | 2 | L | Acetabulum, L1 | No | Reconstruction | / | Dead | 4 | 8/3 |
| 4 | 76 | ADK,NA,III | Pain | 242.6 | 10 | 1 | Median | L3 | Lung | Reconstruction | RT | Dead | 4 | 6/4 |
| 5 | 55 | ADK,NA,NA | Pain | 56.12 | 13 | 1 | R | Tibia | Lung | Reconstruction | / | Live | 47 | 6/2 |
| 6 | 65 | ADK,NA,NA | Pain | 22.06 | 144 | 2 | Bilateral | Ilium | No | Reconstruction | / | Dead | 16 | 4/1 |
| 7 | 74 | ADK,G2,I | Pain | 7.79 | 13 | 3 | R | Sacrum, ilium, L5 | No | Reconstruction | / | Live | 53 | 4/0 |
| 8 | 54 | ADK,G2,IV | Pain | 14.31 | At dx | 2 | L | Pubis, ischium | No | Reconstruction | RT + CHT + HT | Dead | 57 | 6/8 |
| 9 | 56 | ADK,G3,IV | Pain | 64.74 | At dx | 2 | R | Pubis, ischium | No | Reconstruction | RT + CHT | Live | 14 | 5/1 |
| 10 | 59 | ADK,G3,IV | Pain | 39.88 | At dx | 2 | L | Pubis, ischium | No | Reconstruction | CHT | Live | 12 | 3/1 |
| 11 | 63 | ADK,G1,I | Pain | NA | 5 | 3 | R | Acetabulum, pubis, ischium | Lung | Reconstruction | / | Live | 35 | 7/3 |
| 12 | 45 | ADK,G3,IV | Pain | 374.50 | At dx | 1 | R | Pubis | Abdomen | Reconstruction | CHT | Live | 18 | 7/2 |
| 13 | 72 | ADK,NA,NA | pain | 204.50 | 36 | 2 | R | Acetabulum, pubis | Lung | Reconstruction | / | Live | 4 | 6/1 |
| Author | Pt. No. | Age (Years) | Histology, Grade, Stage | Symptoms at Presentation | Interval to Bone Met (Months) | Localization | Extraosseous Met | Therapy | Status | Survival after Bone Met (Months) |
|---|---|---|---|---|---|---|---|---|---|---|
| Ravault et al. [8] | 1 | 61 | NA,NA,NA | Pain | 36 | R tarsus | No | Surgery, RT | Live | 7 |
| Petru et al. [9] | 2 | 61 | ADK,G1,IV | Pain, swelling | At dx | L tarsus | No | Surgery, CHT, HT | Live | 10 |
| Clarke and Smith [10] | 3 | 55 | ADK,NA,NA | Pain, swelling | 18 | R talus, calcaneus | Lung | Surgery, RT | Dead | 36 |
| Mustafa et al. [11] | 4 | 45 | ADK,G2,I | Infection | 36 | Cranium | Lung, pelvic sidewall | Surgery, HT | Dead | 6 |
| Neto at al. [12] | 5 | 39 | ADK,G2,IV | Pain, tumble | At dx | R ischium | No | Surgery, RT | Live | 36 |
| Arnold et al. [13] | 6 | 63 | ADK,G1,IV | Pain, leg weakness | At dx | T12 | No | Surgery, RT, HT | Live | 60 |
| Ali et al. [14] | 7 | 77 | ADK,G3,I | Throbbing, swelling | 24 | L 4th toe, distal phalanx | Lung | Surgery, HT | Live | 16 |
| Haraguchi et al. [15] | 8 | 87 | NA,NA,NA | Pain | 108 | Sternum | No | Surgery | Live | 60 |
| Uharcek et al. [16] | 9 | 67 | ADK,G1,IV | Pain, erythema, swelling | At dx | R foot | No | Surgery, CHT, HT | Live | 20 |
| Albareda et al. [5] | 10 | 62 | ADK,G1,I | None | 37 | Sacrum | No | Surgery, HT | Live | 26 |
| Qin et al. [17] | 11 | 48 | ADK,G3,II | Pain | 22 | R and L femur | No | Surgery, CHT, HT, RT | Live | 42 |
| Pakos et al. [18] | 12 | 62 | ADK,G3,II | Pain | 7 | R tibia | No | Surgery | Live | 27 |
| Chan et al. [19] | 13 | 62 | NA,NA,NA | Pain | 3 | Sternum | NA | Surgery | Dead | 18 |
| Kehoe et al. [20] | 14 | 58 | ADK,G3,I | Pain | 10 | L4, L5 | No | Surgery, RT, CHT | Live | 199 |
| Kehoe et al. [20] | 15 | 60 | Clear cell,G3,NA | Pain | 12 | Humerus, clavicle | No | Surgery, RT, CHT | Dead | 13 |
| Kehoe et al. [20] | 16 | 55 | ADK,G3,III | Pain | 9 | Rib | No | Surgery, RT | Dead | 26 |
| Kehoe et al. [20] | 17 | 55 | ADK,G3,IV | Pain | At dx | Ischium, acetabulum, femur | No | Surgery, RT | Dead | 10 |
| Jiang et al. [6] | 18 | 51 | ADK,G2,IV | Pain, swelling | At dx | L tibia, calcaneus, tarsus | Lung | Surgery, CHT, HT | Live | 56 |
| Vizzielli et al. [21] | 19 | 62 | ADK,G1,IV | Pain | At dx | Thigh, acetabulum, ischiopubic bone | Lung | Surgery, CHT | Live | 30 |
| Uccella et al. [22] | 20 | 65 | ADK,G2,IV | Pain | 19 | R sternum | No | Surgery, HT | Dead | 60 |
| Uccella et al. [22] | 21 | 65 | ADK,G2,NA | Lack of strength and sensation | 18 | T5 | No | Surgery, RT, HT | Dead | 9 |
| Myriokefalitaki et al. [23] | 22 | 57 | ADK,G2,IV | Pain | At dx | R femur | No | Surgery, RT | Live | 53 |
| Kimyon et al. [24] | 23 | 62 | ADK,G2,I | Pain | 2 | Tibia, femur | No | Surgery, RT, CHT | Live | 22 |
| Makris et al. [25] | 24 | 68 | ADK,G1,IV | Pain | At dx | R tibia | No | Surgery, RT, CHT | Live | 6 |
| Characteristics | Bone Metastases at Primary Recurrence of EC (n = 24) | Bone Metastases at the Diagnosis of EC (n = 13) | p-Value |
|---|---|---|---|
| Age, median (range), years | 62 (45, 87) | 57 (39, 68) | 0.119 |
| History | 0.513 | ||
| Endometrioid | 19 | 13 | |
| Nonendometrioid | 2 | 0 | |
| NA | 3 | 0 | |
| Grade | 0.396 | ||
| G1 | 2 | 5 | |
| G2 | 6 | 4 | |
| G3 | 7 | 4 | |
| NA | 9 | 0 | |
| No. of bone lesions | 0.985 | ||
| Single | 13 | 7 | |
| Multiple | 11 | 6 | |
| Concomitant extraosseous metastases | 0.708 | ||
| Yes | 8 | 3 | |
| No | 15 | 10 | |
| Solitary bone metastasis without extraosseous involvement | 0.501 | ||
| Yes | 8 | 6 | |
| No | 15 | 7 | |
| Metastases to the axial skeleton | 0.082 | ||
| Yes | 14 | 3 | |
| No | 10 | 10 | |
| Overall survival, median, months | 36.0 | 57.0 | 0.084 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.; Dai, Y.; Ji, T.; Guo, W.; Wang, Z.; Wang, J. Bone Metastases of Endometrial Carcinoma Treated by Surgery: A Report on 13 Patients and a Review of the Medical Literature. Int. J. Environ. Res. Public Health 2022, 19, 6823. https://doi.org/10.3390/ijerph19116823
Wang J, Dai Y, Ji T, Guo W, Wang Z, Wang J. Bone Metastases of Endometrial Carcinoma Treated by Surgery: A Report on 13 Patients and a Review of the Medical Literature. International Journal of Environmental Research and Public Health. 2022; 19(11):6823. https://doi.org/10.3390/ijerph19116823
Chicago/Turabian StyleWang, Jingyuan, Yibo Dai, Tao Ji, Wei Guo, Zhiqi Wang, and Jianliu Wang. 2022. "Bone Metastases of Endometrial Carcinoma Treated by Surgery: A Report on 13 Patients and a Review of the Medical Literature" International Journal of Environmental Research and Public Health 19, no. 11: 6823. https://doi.org/10.3390/ijerph19116823
APA StyleWang, J., Dai, Y., Ji, T., Guo, W., Wang, Z., & Wang, J. (2022). Bone Metastases of Endometrial Carcinoma Treated by Surgery: A Report on 13 Patients and a Review of the Medical Literature. International Journal of Environmental Research and Public Health, 19(11), 6823. https://doi.org/10.3390/ijerph19116823