
Engaging U.S. Adults with Serious Mental Illness in Participatory Design Research Exercises


Abstract
:1. Introduction
2. Background
2.1. Mental Illness and Serious Mental Illness in the U.S.
2.2. The Clubhouse Model of Psychosocial Rehabilitation
2.3. Mental and Behavioral Health and the Built Environment
2.3.1. Mental and Behavioral Health Facility Design
2.3.2. Clubhouse Facility Design
“Space emphasizes the importance of creating a dignified, attractive environment where important work is carried out.
- 1. What are Clubhouse members’ needs, preferences, and priorities relating to the design of a future Clubhouse facility?
- 2. Are participatory design research exercises a potentially meaningful and effective mechanism by which to engage Clubhouse members in the design process?
3. Methods
3.1. Research Design
3.2. Project Location and Context
3.3. Participants
3.4. Procedures
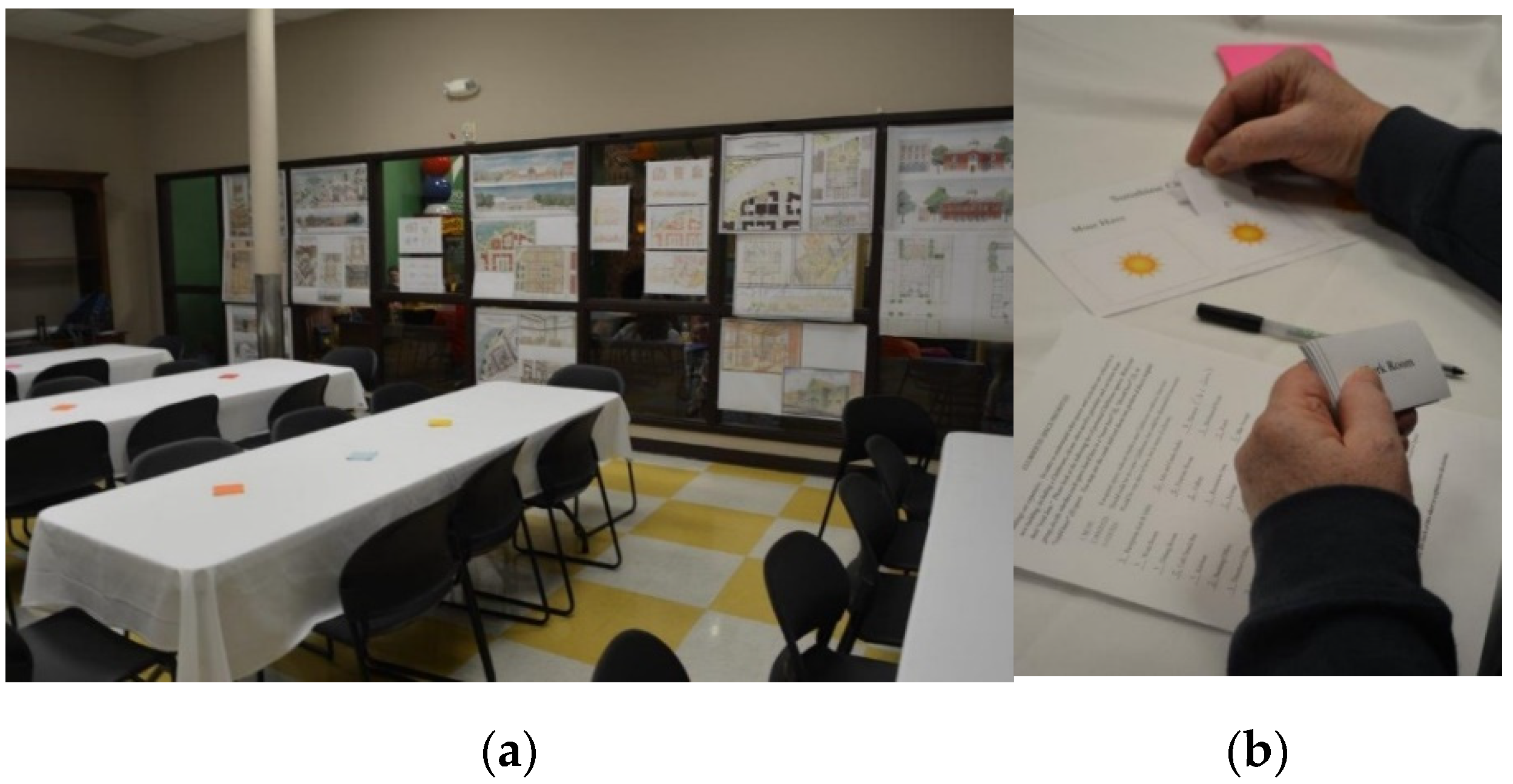
3.4.1. Participatory Exercise Development
- Must: A required space, without which a new Clubhouse could not function.
- Should: Needed in a new Clubhouse, but could be eliminated if necessary.
- Could: Would be very nice to have, but is more of a luxury.
3.4.2. Data Collection
3.4.3. Analysis
4. Results
4.1. Participant and Former Clubhouse Characteristics
4.1.1. Participant Characteristics
4.1.2. Former Clubhouse Use and Characteristics
4.2. Research Question 1: Member Needs, Preferences, and Priorities
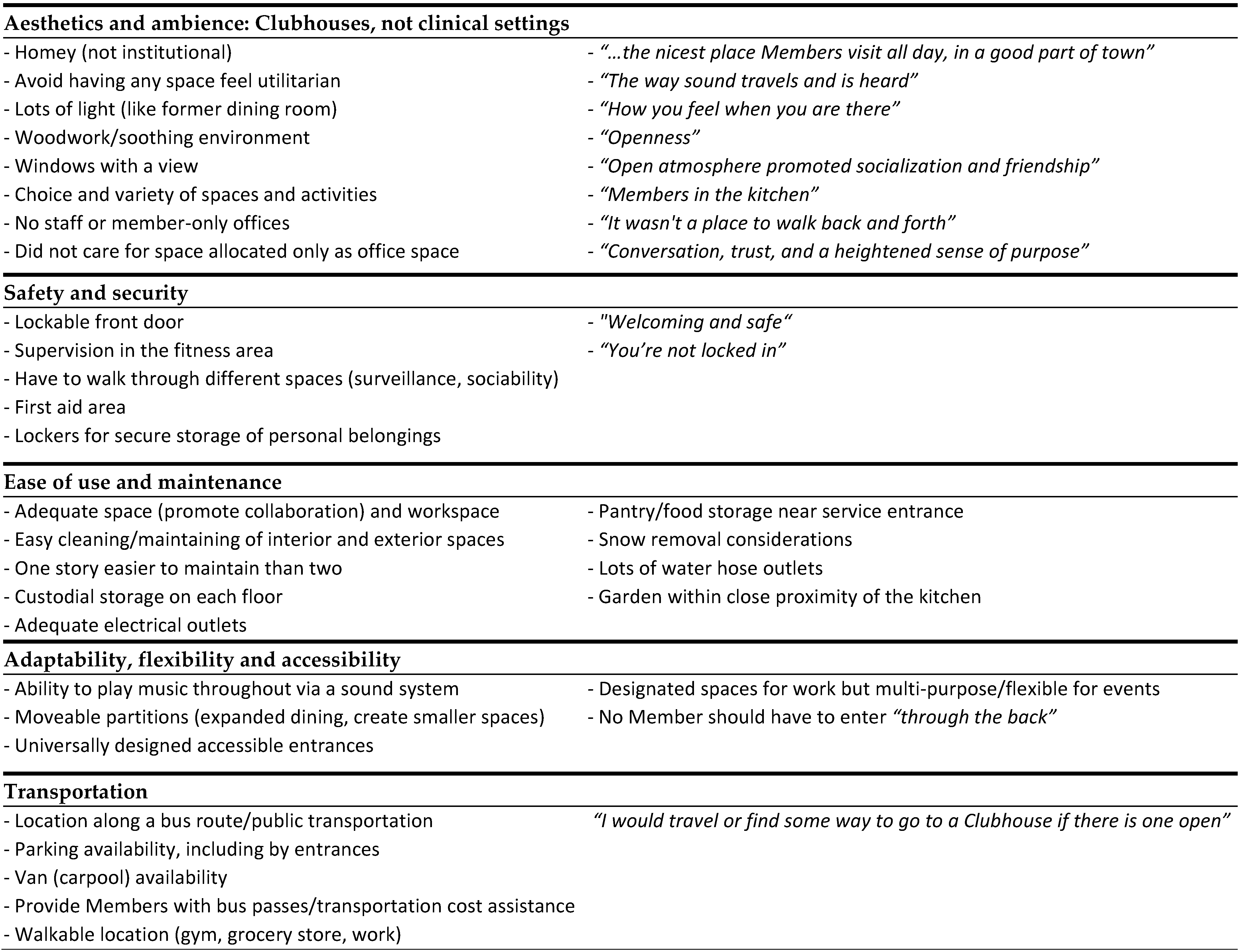
4.2.1. Aesthetics and Ambience: Clubhouses, Not Clinical Settings
- “The way sound travels and is heard”
- “How you feel when you are there”
- “It wasn’t a place to walk back and forth”
- “Conversation, trust, and a heightened sense of purpose”
- “Knowing that I was making a difference”
- “Helping others: It kept me out of my own head.”
- “I took on a role of trust both with the staff and the members”
4.2.2. Safety and Security
4.2.3. Ease of Use and Maintenance
4.2.4. Adaptability, Flexibility, and Accessibility
4.2.5. Transportation
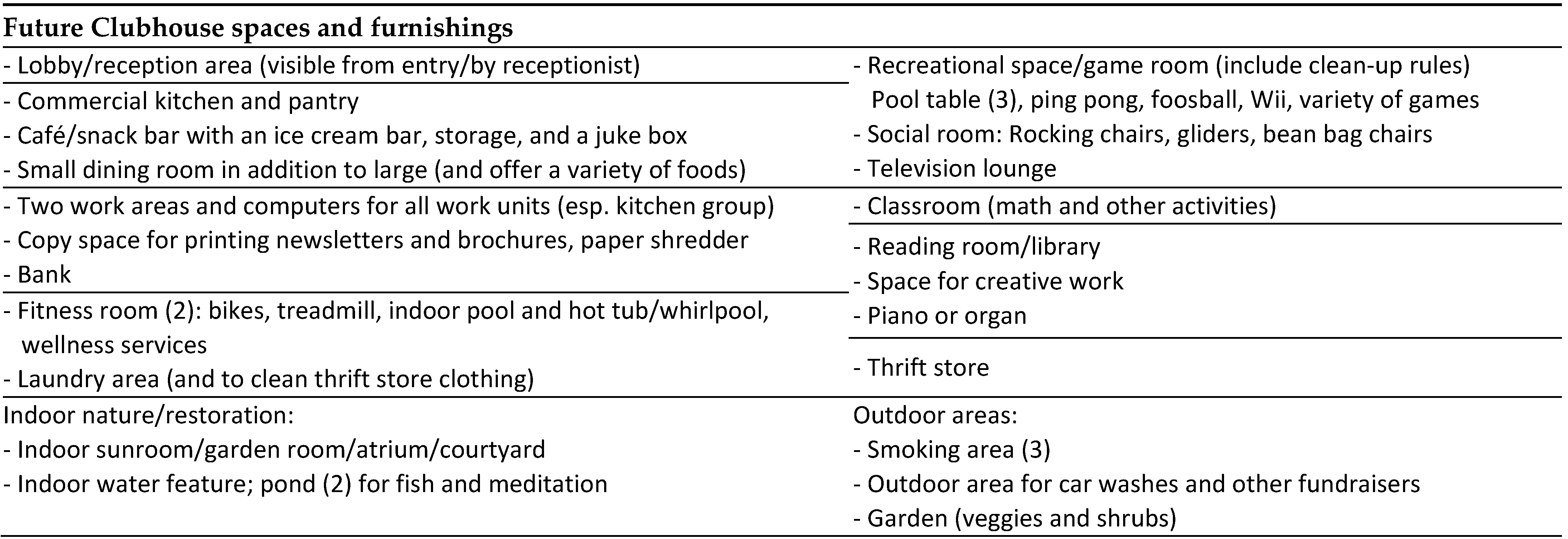
4.2.6. Future Clubhouse Spaces and Furnishings
4.2.7. Clubhouse Space Priorities
4.3. Research Question 2: Participatory Design Research Exercise Potential
“Everyone was so engaged in the activities that it truly was a Clubhouse Model event. I don’t think there was a single person who didn’t feel like they weren’t contributing to help with the design of the new Clubhouse…”
4.3.1. Questionnaire
4.3.2. Design Project Feedback
4.3.3. Space Prioritization
4.3.4. Ideal Clubhouse Drawings
4.3.5. Research Team Reflections
- Learn about and practice communicating clearly and respectfully with people of varying cognitive and physical abilities, especially when providing instructions, answering questions, and offering assistance with exercises (e.g., offering to write comments on sticky notes when members could not).
- Inquire about and practice using appropriate language (e.g., members, not patients).
- Identify opportunities to interact with the population. Student research assistants said they would have felt more confident during the session with prior experience.
- Arrange for participant transportation, food, and any other needs during the session.
- Refer to and adapt existing participatory design research exercises and best practices.
- Develop work-oriented exercises that can easily be completed in a fixed time period.
- Create and test more exercises than needed.
- Include members and staff in exercise development, testing, and administration (and ideally data entry and analysis). Familiar faces were also helpful to attendees who initially preferred not to communicate with strangers.
- Allow for some redundancy in data collection across exercises to improve reliability. Member control over engagement means allowing missing responses. Vary task types and required levels of interaction with peers, staff, and the research team.
- Begin with a short, simple, and engaging exercise. Conduct longer or (minimally) complex exercises that generate important data early but not first in the session.
- Test exercises from instructions through data entry and analysis, then revise and repeat. Confirm that responses align with data collection goals.
- Create detailed supply lists, timelines, and procedures for set-up, exercise administration, and clean-up so team focus remains on the exercises and supporting participants during the session. Visit the space in advance and address any anticipated challenges.
- Practice, practice, practice. Rehearse all exercises, revise exercises and procedures, and repeat. Assign tasks to each research team member, with “back-up” as needed.
- Wear friendly name tags and appropriate clothing.
- Stick to the schedule, but be flexible. Prioritize member needs and experiences.
- Ask participants about their work to subtly confirm exercise instructions were clear.
- Briefly check in with research team members during and in-between exercises.
- Emphasize Member expertise and the value of their input to inform the design process.
5. Discussion
5.1. Limitations
5.2. Future Directions
6. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McKay, C.; Nugent, K.L.; Johnsen, M.; Eaton, W.W.; Lidz, C.W. A systematic review of evidence for the Clubhouse Model of psychosocial rehabilitation. Adm. Policy Ment. Health Ment. Health Serv. Res. 2018, 45, 28–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clubhouse International. International Standards for Clubhouse Programs; Clubhouse International: New York, NY, USA, 2020; pp. 1–4. Available online: https://Clubhouse-intl.org/wp-content/uploads/2020/12/standards_2020_eng.pdf (accessed on 12 January 2022).
- Wallerstein, N.; Duran, B. The conceptual, historical and practice roots of community based participatory research and related participatory traditions. In Community-Based Participatory Research for Health; Minkler, M., Wallerstein, N., Eds.; Jossey-Bass: San Francisco, CA, USA, 2003; pp. 27–51. [Google Scholar]
- Fossey, E.; Harvey, C.; McDermott, F. Housing and support narratives of people experiencing mental health isues: Making my place, my home front. Psychiatry 2020, 10, 939. [Google Scholar]
- Substance Abuse and Mental Health Services Administration. Key Substance Use and Mental Health Indicators in the United States: Results from the 2020 National Survey on Drug Use and Health; HHS Publication No. PEP21-07-01-003, NSDUH Series H-56; Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2021. Available online: https://www.samhsa.gov/data/ (accessed on 14 January 2022).
- National Alliance on Mental Illness. Mental Health by the Numbers. Available online: https://www.nami.org/mhstats (accessed on 26 February 2022).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Wang, P.S.; Berglund, P.A.; Olfson, M.; Kessler, R.C. Delays in initial treatment contact after first onset of a mental disorder. Health Serv. Res. 2004, 39, 393–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [Green Version]
- National Council for Behavioral Health. The Psychiatric Shortage: Causes and Solutions; National Council for Behavioral Health, Medical Director Institute: Washington, DC, USA, 2018; Available online: https://www.thenationalcouncil.org/wp-content/uploads/2022/02/Revised-Final-Access-Paper.pdf (accessed on 10 January 2022).
- Health Resources & Services Administration. Shortage Areas. Available online: https://data.hrsa.gov/topics/health-workforce/shortage-areas (accessed on 26 February 2022).
- Steadman, H.J.; Osher, F.C.; Robbins, P.C.; Case, B.; Samuels, S. Prevalence of serious mental illness among jail inmates. Psychiatr. Serv. 2009, 60, 761–765. [Google Scholar] [CrossRef]
- Bronson, J.; Berzofsky, M. Steadman; U.S. Department of Justice: Office of Justice Programs: Washington, DC, USA, 2017. Available online: https://bjs.ojp.gov/content/pub/pdf/imhprpji1112.pdf (accessed on 10 January 2022).
- Diehl, S.; Douglas, D.; Honberg, R. Road to Recovery: Employment and Mental Illness; NAMI, the National Alliance on Mental Illness: Arlington, VA, USA, 2014; Available online: https://www.nami.org/Support-Education/Publications-Reports/Public-Policy-Reports/RoadtoRecovery.pdf (accessed on 10 January 2022).
- Caton, C.L.; Dominguez, B.; Schanzer, B.; Hasin, D.S.; Shrout, P.E.; Felix, A.; McQuistion, H.; Opler, L.A.; Hsu, E. Risk factors for long-term homelessness: Findings from a longitudinal study of first-time homeless single adults. Am. J. Public Health 2005, 95, 1753–1759. [Google Scholar] [CrossRef]
- Kertesz, S.G.; Larson, M.J.; Horton, N.J.; Winter, M.; Saitz, R.; Samet, J.H. Homeless chronicity and health-related quality of life trajectories among adults with addictions. Med. Care 2005, 43, 574–585. [Google Scholar] [CrossRef]
- Padgett, D.K.; Gulcur, L.; Tsemberis, S. Housing First services for people who are homeless with co-occurring serious mental illness and substance abuse. Res. Soc. Work. Pract. 2006, 16, 74–83. [Google Scholar] [CrossRef]
- Henry, M.; Watt, R.; Rosenthal, L.; Shivji, A.; Abt Associates. The 2016 Annual Homeless Assessment Report (AHAR) to Congress November 2016 PART 1: Point-in-Time Estimates of Homelessness; U.S. Department of Housing and Urban Development: Washington, DC, USA, 2016. [Google Scholar]
- Centers for Disease Control. Suicide Rising across the US: More than a Mental Health Concern; Centers for Disease Control, National Center for Injury Prevention and Control: Atlanta, GA, USA, 2018. Available online: https://www.cdc.gov/vitalsigns/pdf/vs-0618-suicide-H.pdf (accessed on 11 January 2022).
- Isometsä, E.T. Psychological autopsy studies—A review. Eur. Psychiatry 2001, 16, 379–385. [Google Scholar] [CrossRef]
- Anderson, S. We Are Not Alone: Fountain House & the Development of Clubhouse Culture; Fountain House Inc.: New York, NY, USA, 1999. [Google Scholar]
- Beard, J.H.; Propst, R.N.; Malamud, T.J. The Fountain House Model of Psychatric Rehabilitation. Psychosoc. Rehabil. J. 1982, 5, 47–53. [Google Scholar]
- Herman, S.E.; Onaga, E.; Pernice-Duca, F.M.; Oh, S.; Ferguson, C. Sense of community in Clubhouse programs: Member and staff concepts. Am. J. Community Psychol. 2005, 36, 343–356. [Google Scholar] [CrossRef]
- Pernice-Duca, F.M. The structure and quality of social network support among mental health consumers of Clubhouse programs. J. Community Psychol. 2008, 36, 929–946. [Google Scholar] [CrossRef]
- Pernice-Duca, F.M. Staff and member perceptions of the Clubhouse environment. Adm. Policy Ment. Health 2010, 37, 345–356. [Google Scholar] [CrossRef]
- Macias, C.; Jackson, R.; Schroeder, C.; Wang, Q. What is a Clubhouse? Report on the ICCD 1996 Survey of USA Clubhouses. Community Ment. Health J. 1999, 35, 181–190. [Google Scholar] [CrossRef]
- Mowbray, C.T.; Lewandowski, L.; Holter, M.C.; Bybee, D. The Clubhouse as an empowering setting. Health Soc. Work. 2006, 31, 167–179. [Google Scholar] [CrossRef]
- Malamud, T.J.; McCrory, D. Transitional employment and psycho-social rehabilitation. In Vocational Rehabilitation of Persons with Prolonged Psychiatric Disorders; Cardiello, J.A., Bell, M.D., Eds.; Johns Hopkins University Press: Baltimore, MD, USA, 1988; pp. 150–162. [Google Scholar]
- Jackson, R.L. The Clubhouse Model: Empowering Applications of Theory to Generalist Practice, 1st ed.; Wadsworth: Belmont, CA, USA, 2001. [Google Scholar]
- Waters, B. The work unit: The heart of the Clubhouse. Psychosoc. Rehabil. J. 1992, 16, 41–48. [Google Scholar] [CrossRef]
- Doyle, A.; Lanoil, J.; Dudek, K.J. Fountain House: Creating Community in Mental Health Practice; Columbia University Press: New York, NY, USA, 2013. [Google Scholar]
- Propst, R.N. Stages in realizing the international diffusion of a single way of working: The Clubhouse Model. New Dir. Ment. Health Serv. 1997, 74, 53–66. [Google Scholar] [CrossRef]
- Mertz, M.A.; Harvey, R.B. Career development theory as a framework for assessment and planning in Clubhouse-based transitional employment programs for people with psychiatric disabilities. Work. A J. Prev. Assess. Rehabil. 1998, 10, 219–233. [Google Scholar]
- Owens, P.L.; Mutter, R.; Stocks, C. Mental Health and Substance Abuse-Related Emergency Department Visits among Adults, 2007; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2010. Available online: https://www.hcup-us.ahrq.gov/reports/statbriefs/sb92.pdf (accessed on 11 January 2022).
- Kessler, R.C.; Heeringa, S.; Lakoma, M.D.; Petukhova, M.; Rupp, A.E.; Schoenbaum, M.; Zaslavsky, A.M. Individual and societal effects of mental disorders on earnings in the United States: Results from the national comorbidity survey replication. Am. J. Psychiatry 2008, 165, 703–711. [Google Scholar] [CrossRef]
- Johnson, J.; Hickey, S. Arrests and incarcerations after psychosocial program involvement: Clubhouse vs. Jailhouse. Psychiatr. Rehabil. J. 1999, 23, 66–69. [Google Scholar] [CrossRef]
- McKay, C.E.; Yates, B.T.; Johnsen, M. Costs of Clubhouses: An international perspective. Adm. Policy Ment. Health Ment. Health Serv. Res. 2007, 34, 62. [Google Scholar] [CrossRef] [PubMed]
- Cowell, A.J.; Pollio, D.E.; North, C.S.; Stewart, A.M.; McCabe, M.M.; Anderson, D.W. Deriving service costs for a Clubhouse psychosocial rehabilitation program. Adm. Policy Ment. Health Ment. Health Serv. Res. 2003, 30, 323–340. [Google Scholar] [CrossRef] [PubMed]
- Moos, R. Evaluating Treatment Environments: The Quality of Psychiatric and Substance Abuse Programs, 2nd ed.; Transaction Publishers: New Brunswick, NJ, USA, 1997. [Google Scholar]
- Moos, R. Evaluating Treatment Environments: A Social Ecological Approach; Wiley: New York, NY, USA, 1974. [Google Scholar]
- Liddicoat, S.; Badcock, P.; Killackey, E. Principles for designing the built environment of mental health services. Lancet Psychiatry 2020, 7, 915–920. [Google Scholar] [CrossRef]
- Shepley, M.M.; Watson, A.; Pitts, F.; Garrity, A.; Spelman, E.; Kelkar, J.; Fronsman, A. Mental and behavioral health environments: Critical considerations for facility design. Gen. Hosp. Psychiatry 2016, 42, 15–21. [Google Scholar] [CrossRef]
- Shepley, M.M.; Sachs, N.A. Design Attributes for Improved Mental and Behavioral Health. In Architecture and Health: Guiding Principles for Practice; Routledge: New York, NY, USA, 2019; pp. 75–97. [Google Scholar]
- Shepley, M.M.; Pasha, S. Design for Mental and Behavioral Health; Routledge: Abingdon, UK, 2017. [Google Scholar]
- Aljunaidy, M.M.; Adi, M.N. Architecture and Mental Disorders: A Systematic Study of Peer-Reviewed Literature. Herd-Health Env. Res. Des. J. 2021, 14, 320–330. [Google Scholar] [CrossRef]
- Evans, G.W. The built environment and mental health. J. Urban Health Bull. N. Y. Acad. Med. 2003, 80, 536–555. [Google Scholar] [CrossRef]
- Evans, G.W.; Wells, N.M.; Hoi-Yan, E.C.; Saltzman, H. Housing quality and mental health. J. Consult. Clin. Psychol. 2000, 68, 526–530. [Google Scholar] [CrossRef]
- Ulrich, R.; Zimring, C.; Zhu, X.; DuBose, J.; Seo, H.; Choi, Y.; Quan, X.; Joseph, A. A review of the research literature on evidence-based healthcare design. Health Environ. Res. Des. J. 2008, 1, 61–125. [Google Scholar] [CrossRef]
- Wells, N.M.; Rollings, K.A. The natural environment: Influences on human health and function. In The Oxford Handbook of Environmental and Conservation Psychology; Clayton, S., Ed.; Oxford University Press: Oxford, UK, 2012; pp. 509–523. [Google Scholar]
- Long, C.G.; Langford, V.; Clay, R.; Craig, L.; Hollin, C.R. Architectural change and the effects on the perceptions of the ward environment in a medium secure unit for women. Br. J. Forensic Pract. 2011, 13, 205–212. [Google Scholar] [CrossRef]
- Golembiewski, J. Lost in space: The place of the architectural milieu in the aetiology and treatment of schizophrenia. Facilities 2013, 31, 427–448. [Google Scholar] [CrossRef] [Green Version]
- Rollings, K.A.; Bollo, C.S. Permanent supportive housing design characteristics associated with the mental health of formerly homeless adults in the U.S. and Canada: An integrative review. Int. J. Environ. Res. Public Health 2021, 18, 9588. [Google Scholar] [CrossRef]
- Shepley, M.M.; Pasha, S.; Ferguson, P.; Huffcut, J.C.; Kiyokawa, G.; Martere, J. Design Research and Behavioral Health Facilities; The Center for Health Design: Concord, CA, USA, 2013; pp. 1–81. Available online: https://www.healthdesign.org/system/files/chd428_researchreport_behavioralhealth_1013-_final_0.pdf (accessed on 26 February 2022).
- Shepley, M.M.; Watson, A.; Pitts, F.; Garrity, A.; Spelman, E.; Fronsman, A.; Kelkar, J. Mental and behavioral health settings: Importance & effectiveness of environmental qualities & features as perceived by staff. J. Environ. Psychol. 2017, 50, 37–50. [Google Scholar]
- Connellan, K.; Gaardboe, M.; Riggs, D.; Due, C.; Reinschmidt, A.; Mustillo, L. Stressed spaces: Mental health and architecture. Health Environ. Res. Des. J. 2013, 6, 127–168. [Google Scholar] [CrossRef]
- Friesinger, J.G.; Topor, A.; Boe, T.D.; Larsen, I.B. Studies regarding supported housing and the built environment for people with mental health problems: A mixed-methods literature review. Health Place 2019, 57, 44–53. [Google Scholar] [CrossRef]
- Marcheschi, E.; Johansson, M.; Brunt, D.; Laike, T. Physical-environment qualities of supported-housing facilities for people with severe mental illness. J. Archit. Plan. Res. 2014, 31, 128–142. [Google Scholar]
- Cook, J.A.; Razzano, L. Discriminant function analysis of competitive employment outcomes in a transitional employment program for persons with severe mental illness. J. Vocat. Rehabil. 1995, 5, 127–139. [Google Scholar] [CrossRef]
- Macias, C.; Propst, R.; Rodican, C.; Boyd, J. Strategic planning for ICCD Clubhouse implementation: Development of the Clubhouse Research and Evaluation Screening Survey (CRESS). Ment. Health Serv. Res. 2001, 3, 155–167. [Google Scholar] [CrossRef]
- Kemmis, S.; McTaggart, R. Participatory action research. In Strategies of Qualitative Inquiry; Denzin, N.K., Lincoln, Y.S., Eds.; Sage: Thousand Oaks, CA, USA, 2003; pp. 336–398. [Google Scholar]
- Duerk, D.P. Architectural Programming: Information Management for Design; Van Nostrand Reinhold Company: Hoboken, NJ, USA, 1993. [Google Scholar]
- Jackson, L. The relationship of urban design to human health and condition. Landsc. Urban Plan. 2002, 64, 191–200. [Google Scholar] [CrossRef]
- Jackson, R.J.; Kochtitzky, C. Creating a Healthy Environment: The Impact of the Built Environment on Public Health; Sprawl Watch Clearinghouse: Washington, DC, USA, 2010; Available online: http://www.sprawlwatch.org/health.pdf (accessed on 28 February 2022).
- Erfani, K. Post-Occupancy Evaluation of Fountain House: A Study on an Alternative Healthcare Facility. Master’s Thesis, Cornell University, Ithaca, NY, USA, 2017. [Google Scholar]
- Shepley, M.; Watson, A.; Pitts, F.; Garrity, A.; Spelman, E.; Fronsman, A.; Kelkar, J. Mental and Behavioral Health Environments: Measurement of Building Performance; The Center for Health Design: Concord, CA, USA, 2016; pp. 1–118. Available online: https://www.healthdesign.org/knowledge-repository/mental-and-behavioral-health-environments-measurement-building-performance (accessed on 26 February 2022).
- Schweitzer, M.; Gilpin, L.; Frampton, S. Healing spaces: Elements of environmental design that make an impact on health. J. Altern. Complem. Med. 2004, 10, S71–S83. [Google Scholar] [CrossRef] [Green Version]
- Abdelaal, M.S.; Soebarto, V. Biophilia and Salutogenesis as restorative design approaches in healthcare architecture. Archit. Sci. Rev. 2019, 62, 195–205. [Google Scholar] [CrossRef]
- Tsai, J.; Rosenheck, R.A. Racial differences among supported housing clients in outcomes and therapeutic relationships. Psychiatr. Q. 2012, 83, 103–112. [Google Scholar] [CrossRef]
- Adame, A.L.; Perry, C.; Pierce, E. Community and Housing First: A qualitative analysis of USA residents’ perspectives. Health Soc. Care Community 2020, 28, 1292–1300. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Must = 1 (1–1.5) | Should = 2 (1.6–2.5) | Could = 3 (2.6–3) | |||
|---|---|---|---|---|---|
| Space | Average | Space | Average | Space | Average |
| Meeting room | 1.0 | Classroom | 1.6 | Balcony | 2.6 |
| Smoking area | “ | Dining room | “ | Bike storage | “ |
| Reception desk/lobby | 1.2 | Lockers | “ | Gallery | “ |
| Kitchen | “ | Stairs | “ | Audio-visual | 2.8 |
| Copy center | “ | Café/snack bar | 1.8 | Member housing | 3.0 |
| Restrooms | “ | Covered outdoor space | “ | Visitor lodging | “ |
| Parking | “ | Custodial storage | “ | ||
| Work room | 1.4 | Delivery area | “ | ||
| Computer room | “ | Porch | “ | ||
| Admin. Office | “ | Donation storage | 2.0 | ||
| Director’s office | “ | Exercise room | “ | ||
| Elevator | “ | Garage/storage shed | “ | ||
| Laundry/mudroom | “ | Garden | “ | ||
| Library/reading room | “ | ||||
| Mechanical room | “ | ||||
| Recreation area | “ | ||||
| Retail space | “ | ||||
| Drop-off area | 2.2 | ||||
| Arts and crafts studio | 2.4 | ||||
| Banking office | “ | ||||
| Employment office | “ | ||||
| Fitting room | “ | ||||
| Lounge | “ | ||||
| (Any) outdoor space | “ | ||||
| Observed Benefits According to: | Selected Comments |
|---|---|
| Clubhouse Members Contributed to design process All engaged at some level Felt included | “Educational and entertaining” “Atmosphere of excitement” “When can we do this again?” “When will this be built?” |
| Clubhouse Working Group | |
| Informative and identified priorities Inclusion of Members in design Treated Members with dignity | “We wanted to make sure a new building supported our needs, we just didn’t realize how much that support can depend on our space and location.” |
| Architecture Students | |
| Information available Importance of user input Motivation to design well | “I would completely change my design” “What… architects don’t always talk to users?!” “We did so little but it mattered so much” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rollings, K.A. Engaging U.S. Adults with Serious Mental Illness in Participatory Design Research Exercises. Int. J. Environ. Res. Public Health 2022, 19, 6743. https://doi.org/10.3390/ijerph19116743
Rollings KA. Engaging U.S. Adults with Serious Mental Illness in Participatory Design Research Exercises. International Journal of Environmental Research and Public Health. 2022; 19(11):6743. https://doi.org/10.3390/ijerph19116743
Chicago/Turabian StyleRollings, Kimberly A. 2022. "Engaging U.S. Adults with Serious Mental Illness in Participatory Design Research Exercises" International Journal of Environmental Research and Public Health 19, no. 11: 6743. https://doi.org/10.3390/ijerph19116743
APA StyleRollings, K. A. (2022). Engaging U.S. Adults with Serious Mental Illness in Participatory Design Research Exercises. International Journal of Environmental Research and Public Health, 19(11), 6743. https://doi.org/10.3390/ijerph19116743