
Association between Selected Screening Tests and Knee Alignment in Single-Leg Tasks among Young Football Players




Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Ethical Approval
2.3. Procedures
2.3.1. Anthropometric Characteristics
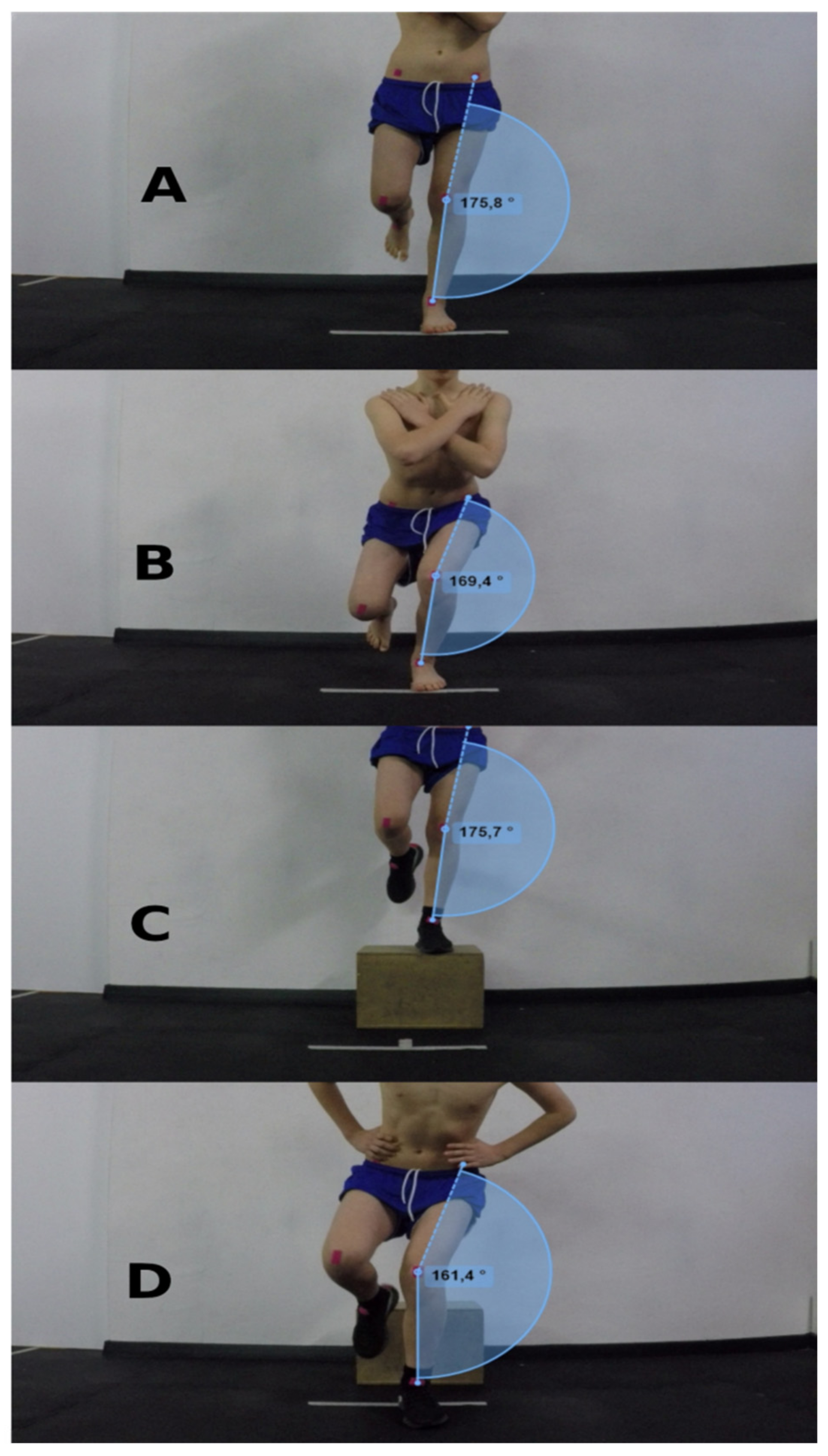
2.3.2. Single-Leg Squat and Single-Leg Landing
SLS
SLL
2.3.3. Two-Dimensional Video Assessment
2.3.4. Range of Motion
WBLT
PSLR
The Sit and Reach Test
Passive Hip ER and IR ROM
2.3.5. Dynamic Balance
2.3.6. Jump Performance
CMJ
SLHD
2.4. Statistical Analysis
3. Results
3.1. Physical Characteristics
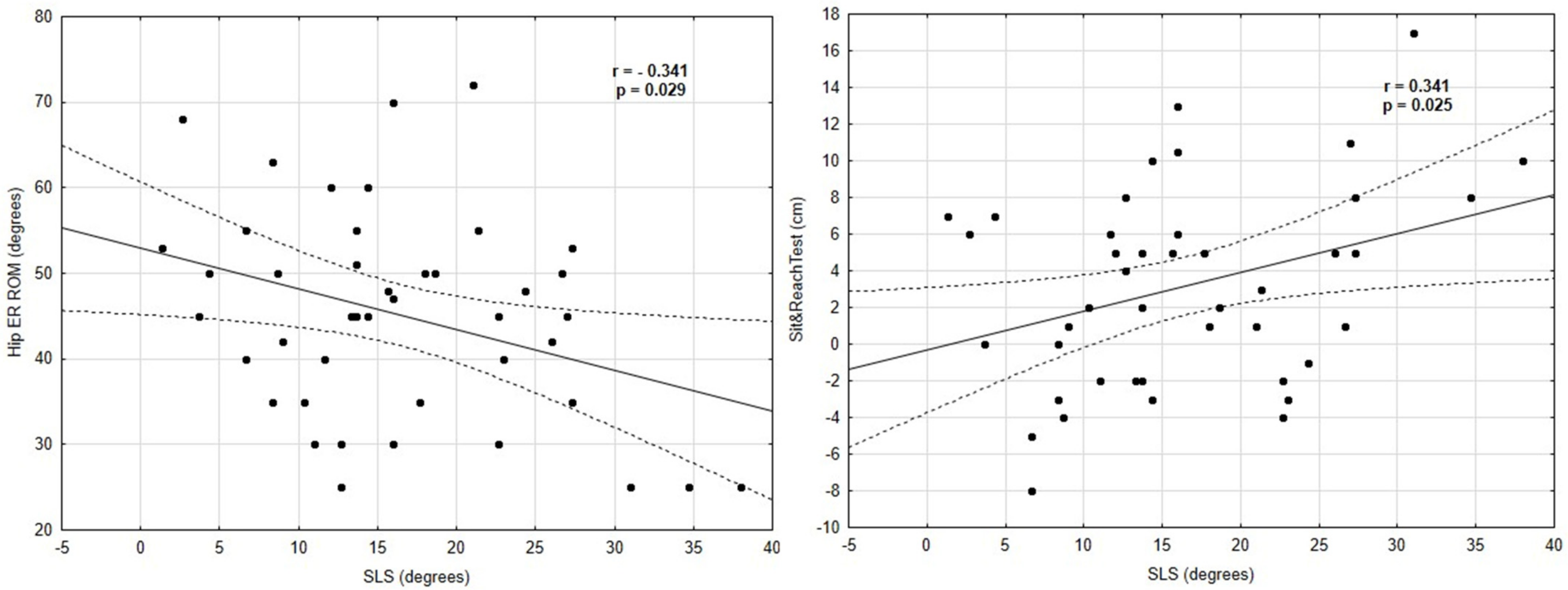
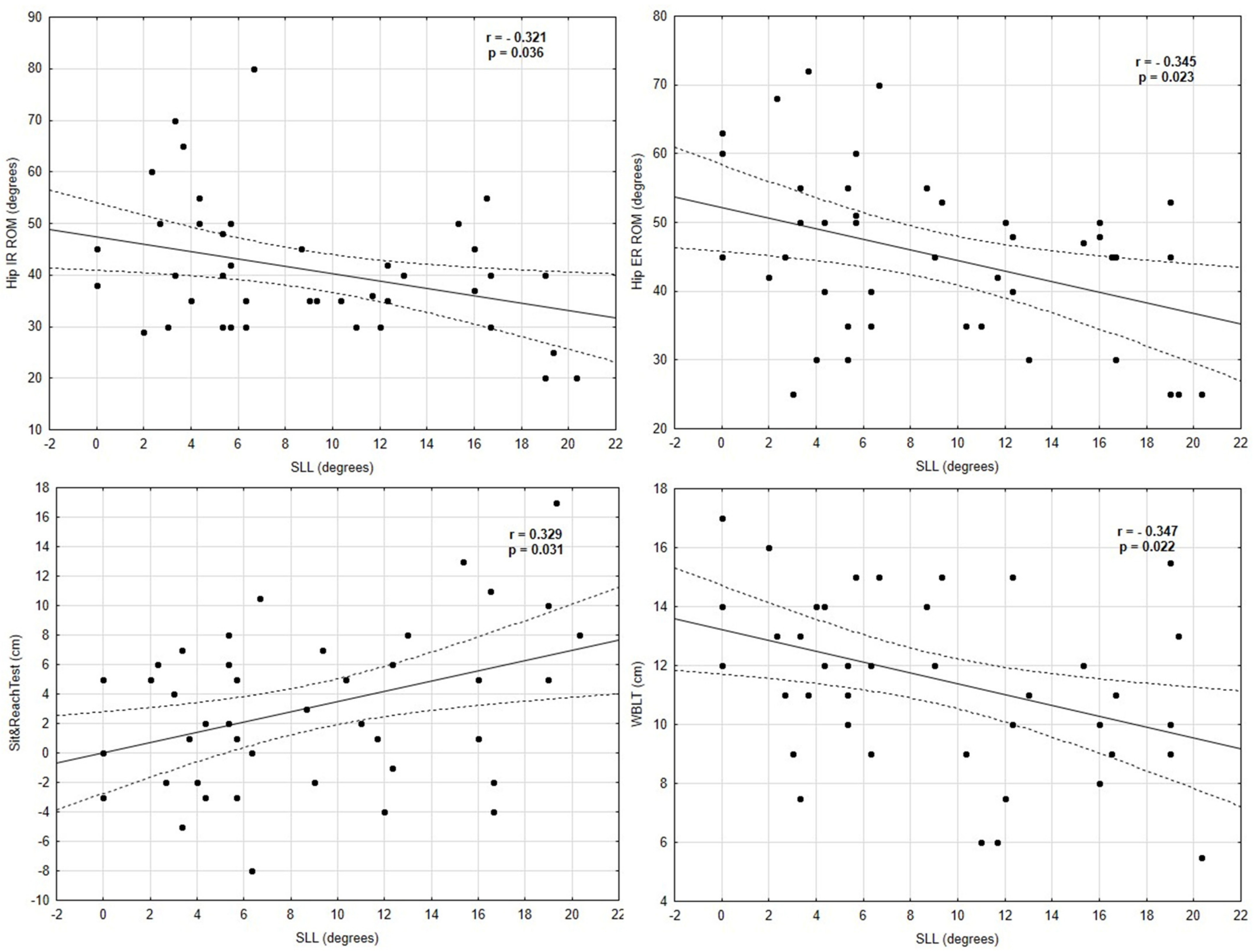
3.2. Correlation between Variables and Knee Valgus Angle
3.3. Predictor Variables for Knee Valgus Angles
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Faude, O.; Rößler, R.; Junge, A. Football Injuries in Children and Adolescent Players: Are There Clues for Prevention? Sport. Med. 2013, 43, 819–837. [Google Scholar] [CrossRef] [PubMed]
- Read, P.J.; Oliver, J.L.; De Ste Croix, M.B.A.; Myer, G.D.; Lloyd, R.S. Assessment of Injury Risk Factors in Male Youth Soccer Players. Strength Cond. J. 2016, 38, 12–21. [Google Scholar] [CrossRef]
- Gomes Neto, M.; Conceição, C.S.; De Lima Brasileiro, A.J.A.; De Sousa, C.S.; Carvalho, V.O.; De Jesus, F.L.A. Effects of the FIFA 11 Training Program on Injury Prevention and Performance in Football Players: A Systematic Review and Meta-Analysis. Clin. Rehabil. 2017, 31, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, C.; Echegoyen, S.; Aoyama, T. The Effects of ‘Prevent Injury and Enhance Performance Program’ in a Female Soccer Team. J. Sports Med. Phys. Fit. 2018, 58, 659–663. [Google Scholar] [CrossRef] [PubMed]
- Bram, J.T.; Magee, L.C.; Mehta, N.N.; Patel, N.M.; Ganley, T.J. Anterior Cruciate Ligament Injury Incidence in Adolescent Athletes: A Systematic Review and Meta-Analysis. Am. J. Sports Med. 2021, 49, 1962–1972. [Google Scholar] [CrossRef]
- Beck, N.A.; Lawrence, J.T.R.; Nordin, J.D.; DeFor, T.A.; Tompkins, M. ACL Tears in School-Aged Children and Adolescents over 20 Years. Pediatrics 2017, 139, e20161877. [Google Scholar] [CrossRef]
- Werner, B.C.; Yang, S.; Looney, A.M.; Gwathmey, F.W. Trends in Pediatric and Adolescent Anterior Cruciate Ligament Injury and Reconstruction. J. Pediatric Orthop. 2015, 36, 447–452. [Google Scholar] [CrossRef]
- Waldén, M.; Hägglund, M.; Magnusson, H.; Ekstrand, J. ACL Injuries in Men’s Professional Football: A 15-Year Prospective Study on Time Trends and Return-to-Play Rates Reveals Only 65% of Players Still Play at the Top Level 3 Years after ACL Rupture. Br. J. Sports Med. 2016, 50, 744–750. [Google Scholar] [CrossRef]
- Wilczyński, B.; Zorena, K.; Ślęzak, D. Dynamic Knee Valgus in Single-Leg Movement Tasks. Potentially Modifiable Factors and Exercise Training Options. a Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 8208. [Google Scholar] [CrossRef]
- Hewett, T.E.; Torg, J.S.; Boden, B.P. Video Analysis of Trunk and Knee Motion during Non-Contact Anterior Cruciate Ligament Injury in Female Athletes: Lateral Trunk and Knee Abduction Motion Are Combined Components of the Injury Mechanism. Br. J. Sports Med. 2009, 43, 417–422. [Google Scholar] [CrossRef]
- Barber-Westin, S.D.; Noyes, F.R. Effect of Fatigue Protocols on Lower Limb Neuromuscular Function and Implications for Anterior Cruciate Ligament Injury Prevention Training: A Systematic Review. Am. J. Sports Med. 2017, 45, 3388–3396. [Google Scholar] [CrossRef] [PubMed]
- Souza, R.B.; Powers, C.M. Differences in Hip Kinematics, Muscle Strength, and Muscle Activation between Subjects with and without Patellofemoral Pain. J. Orthop. Sports Phys. Ther. 2009, 39, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Waldén, M.; Krosshaug, T.; Bjørneboe, J.; Andersen, T.E.; Faul, O.; Hägglund, M. Three Distinct Mechanisms Predominate in Noncontact Anterior Cruciate Ligament Injuries in Male Professional Football Players: A Systematic Video Analysis of 39 Cases. Br. J. Sports Med. 2015, 49, 1452–1460. [Google Scholar] [CrossRef] [PubMed]
- Grassi, A.; Smiley, S.P.; Roberti di Sarsina, T.; Signorelli, C.; Marcheggiani Muccioli, G.M.; Bondi, A.; Romagnoli, M.; Agostini, A.; Zaffagnini, S. Mechanisms and Situations of Anterior Cruciate Ligament Injuries in Professional Male Soccer Players: A YouTube-Based Video Analysis. Eur. J. Orthop. Surg. Traumatol. 2017, 27, 967–981. [Google Scholar] [CrossRef] [PubMed]
- Räisänen, A.M.; Pasanen, K.; Krosshaug, T.; Vasankari, T.; Kannus, P.; Heinonen, A.; Kujala, U.M.; Avela, J.; Perttunen, J.; Parkkari, J. Association between Frontal Plane Knee Control and Lower Extremity Injuries: A Prospective Study on Young Team Sport Athletes. BMJ Open Sport Exerc. Med. 2018, 4, e000311. [Google Scholar] [CrossRef]
- McLean, S.G.; Walker, K.; Ford, K.R.; Myer, G.D.; Hewett, T.E.; Van Den Bogert, A.J. Evaluation of a Two Dimensional Analysis Method as a Screening and Evaluation Tool for Anterior Cruciate Ligament Injury. Br. J. Sports Med. 2005, 39, 355–362. [Google Scholar] [CrossRef]
- Willson, J.D.; Ireland, M.L.; Davis, I. Core Strenght and Lower Extremity Alignment during Single Leg Squats. Med. Sci. Sports Exerc. 2006, 38, 945–952. [Google Scholar] [CrossRef]
- Schurr, S.A.; Marshall, A.N.; Resch, J.E.; Saliba, S.A. Two-Dimensional Video Analysis Is Comparable to 3D Motion Capture in Lower Extremity Movement Assessment. Int. J. Sports Phys. Ther. 2017, 12, 163–172. [Google Scholar]
- Werner, D.M.; Di Stasi, S.; Lewis, C.L.; Barrios, J.A. Test-Retest Reliability and Minimum Detectable Change for Various Frontal Plane Projection Angles during Dynamic Tasks. Phys. Ther. Sport 2019, 40, 169–176. [Google Scholar] [CrossRef]
- Gabbe, B.J.; Bennell, K.L.; Wajswelner, H.; Finch, C.F. Reliability of Common Lower Extremity Musculoskeletal Screening Tests. Phys. Ther. Sport 2004, 5, 90–97. [Google Scholar] [CrossRef]
- Biencourt, N.F.N.; Ocarino, J.M.; Mendonça, L.D.; Hewe, T.E.; Fonseca, S.T. Foot and Hip Contributions to High Frontal Plane Knee Projection Angle in Athletes: A Classification and Regression Tree Approach. J. Orthop. Sports Phys. Ther. 2012, 42, 996–1004. [Google Scholar] [CrossRef] [PubMed]
- Hogg, J.A.; Schmitz, R.J.; Nguyen, A.D.; Shultz, S.J. Passive Hip Range-of-Motion Values across Sex and Sport. J. Athl. Train. 2018, 53, 560–567. [Google Scholar] [CrossRef] [PubMed]
- Hogg, J.A.; Schmitz, R.J.; Shultz, S.J. The Influence of Hip Structure on Functional Valgus Collapse During a Single-Leg Forward Landing in Females. J. Appl. Biomech. 2019, 35, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Lima, Y.L.; Ferreira, V.M.L.M.; de Paula Lima, P.O.; Bezerra, M.A.; de Oliveira, R.R.; Almeida, G.P.L. The Association of Ankle Dorsiflexion and Dynamic Knee Valgus: A Systematic Review and Meta-Analysis. Phys. Ther. Sport 2018, 29, 61–69. [Google Scholar] [CrossRef]
- Wyndow, N.; De Jong, A.; Rial, K.; Tucker, K.; Collins, N.; Vicenzino, B.; Russell, T.; Crossley, K. The Relationship of Foot and Ankle Mobility to the Frontal Plane Projection Angle in Asymptomatic Adults. J. Foot Ankle Res. 2016, 9, 3. [Google Scholar] [CrossRef]
- Nakagawa, T.H.; Petersen, R.S. Relationship of Hip and Ankle Range of Motion, Trunk Muscle Endurance with Knee Valgus and Dynamic Balance in Males. Phys. Ther. Sport 2018, 34, 174–179. [Google Scholar] [CrossRef]
- Nilstad, A.; Krosshaug, T.; Mok, K.M.; Bahr, R.; Andersen, T.E. Association between Anatomical Characteristics, Knee Laxity, Muscle Strength, and Peak Knee Valgus during Vertical Drop-Jump Landings. J. Orthop. Sports Phys. Ther. 2015, 45, 998–1005. [Google Scholar] [CrossRef]
- Hartley, E.M.; Hoch, M.C.; Boling, M.C. Y-Balance Test Performance and BMI Are Associated with Ankle Sprain Injury in Collegiate Male Athletes. J. Sci. Med. Sport 2018, 21, 676–680. [Google Scholar] [CrossRef]
- Smith, C.A.; Chimera, N.J.; Warren, M. Association of Y Balance Test Reach Asymmetry and Injury in Division I Athletes. Med. Sci. Sports Exerc. 2015, 47, 136–141. [Google Scholar] [CrossRef]
- Boey, D.; Lee, M.J. The Relationship between Y-Balance Test Scores and Knee Moments During Single-Leg Jump-Landing in Netball. Int. J. Sports Phys. Ther. 2020, 15, 722–731. [Google Scholar] [CrossRef]
- Wilczyński, B.; Hinca, J.; Ślęzak, D.; Zorena, K. The Relationship between Dynamic Balance and Jumping Tests among Adolescent Amateur Rugby Players. A Preliminary Study. Int. J. Environ. Res. Public Health 2021, 18, 312. [Google Scholar] [CrossRef] [PubMed]
- Muehlbauer, T.; Gollhofer, A.; Granacher, U. Associations between Measures of Balance and Lower-Extremity Muscle Strength/Power in Healthy Individuals Across the Lifespan: A Systematic Review and Meta-Analysis. Sport. Med. 2015, 45, 1671–1692. [Google Scholar] [CrossRef] [PubMed]
- Earl, J.E.; Hertel, J. Lower-Extremity Muscle Activation during the Star Excursion Balance Tests. J. Sport Rehabil. 2001, 10, 93–104. [Google Scholar] [CrossRef]
- Ellenberger, L.; Oberle, F.; Lorenzetti, S.; Frey, W.O.; Snedeker, J.G.; Spörri, J. Dynamic Knee Valgus in Competitive Alpine Skiers: Observation from Youth to Elite and Influence of Biological Maturation. Scand. J. Med. Sci. Sport. 2020, 30, 1212–1220. [Google Scholar] [CrossRef]
- Mirwald, R.L.; Baxter-Jones, A.D.G.; Bailey, D.A.; Beunen, G.P. An Assessment of Maturity from Anthropometric Measurements. Med. Sci. Sports Exerc. 2002, 34, 689–694. [Google Scholar] [CrossRef]
- Gwynne, C.R.; Curran, S.A. Quantifying Frontal Plane Knee Motion during Single Limb Squats: Reliability and Validity of 2-Dimensional Measures. Int. J. Sports Phys. Ther. 2014, 9, 898–906. [Google Scholar]
- Munro, A.; Herrington, L.; Comfort, P. The Relationship between 2-Dimensional Knee-Valgus Angles during Single-Leg Squat, Single-Leg-Land, and Drop-Jump Screening Tests. J. Sport Rehabil. 2017, 26, 72–77. [Google Scholar] [CrossRef]
- Herrington, L.; Alenezi, F.; Alzhrani, M.; Alrayani, H.; Jones, R. The Reliability and Criterion Validity of 2D Video Assessment of Single Leg Squat and Hop Landing. J. Electromyogr. Kinesiol. 2017, 34, 80–85. [Google Scholar] [CrossRef]
- Wilczyński, B.; Wąż, P.; Zorena, K. Impact of Three Strengthening Exercises on Dynamic Knee Valgus and Balance with Poor Knee Control among Young Football Players: A Randomized Controlled Trial. Healthcare 2021, 9, 558. [Google Scholar] [CrossRef]
- Balsalobre-Fernández, C.; Tejero-González, C.M.; Del Campo-Vecino, J.; Bavaresco, N. The Concurrent Validity and Reliability of a Low-Cost, High-Speed Camera-Based Method for Measuring the Flight Time of Vertical Jumps. J. Strength Cond. Res. 2014, 28, 528–533. [Google Scholar] [CrossRef]
- Puig, A.; Escalona, C.; Padullés, J.; Busquets, A.; Padullés, X.; Marcos, D. Validity and Reliability of the Kinovea Program in Obtaining Angles and Distances Using Coordinates in 4 Perspectives. PLoS ONE 2019, 14, e0216448. [Google Scholar] [CrossRef]
- Manning, C.; Hudson, Z. Comparison of Hip Joint Range of Motion in Professional Youth and Senior Team Footballers with Age-Matched Controls: An Indication of Early Degenerative Change? Phys. Ther. Sport 2009, 10, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Hoch, M.C.; Staton, G.S.; McKeon, P.O. Dorsiflexion Range of Motion Significantly Influences Dynamic Balance. J. Sci. Med. Sport 2011, 14, 90–92. [Google Scholar] [CrossRef]
- Powden, C.J.; Hoch, J.M.; Hoch, M.C. Reliability and Minimal Detectable Change of the Weight-Bearing Lunge Test: A Systematic Review. Man. Ther. 2015, 20, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Kendall, F.P.; Mccreary, E.K. Muscles, Testing and Function, 3rd ed.; Williams & Wilkins: Philadelphia, PA, USA, 1975; p. 1968. [Google Scholar]
- De Lucena, G.L.; Dos Santos Gomes, C.; Oliveira Guerra, R. Prevalence and Associated Factors of Osgood-Schlatter Syndrome in a Population-Based Sample of Brazilian Adolescents. Am. J. Sports Med. 2011, 39, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Stiffler, M.R.; Sanfilippo, J.L.; Brooks, M.A.; Heiderscheit, B.C. Star Excursion Balance Test Performance Varies by Sport in Healthy Division I Collegiate Athletes. J. Orthop. Sport. Phys. Ther. 2015, 45, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Picot, B.; Terrier, R.; Forestier, N.; Fourchet, F.; McKeon, P.O. The Star Excursion Balance Test: An Update Review and Practical Guidelines. Int. J. Athl. Ther. Train. 2021, 26, 285–293. [Google Scholar] [CrossRef]
- Castagna, C.; Castellini, E. Vertical jump performance in Italian male and female national team soccer players. J. Strength Cond. Res. 2013, 27, 1156–1161. [Google Scholar] [CrossRef]
- Gheller, R.G.; Dal Pupo, J.; Ache-Dias, J.; Detanico, D.; Padulo, J.; dos Santos, S.G. Effect of Different Knee Starting Angles on Intersegmental Coordination and Performance in Vertical Jumps. Hum. Mov. Sci. 2015, 42, 71–80. [Google Scholar] [CrossRef]
- Markovic, G.; Dizdar, D.; Jukic, I.; Cardinale, M. Reliability and Factorial Validity of Squat and Countermovement Jump Tests. J. Strength Cond. Res. 2004, 18, 551–555. [Google Scholar]
- Kockum, B.; Heijne, A.I.L.M. Hop Performance and Leg Muscle Power in Athletes: Reliability of a Test Battery. Phys. Ther. Sport 2015, 16, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Peat, J.; Barton, B.; Elliott, E. Statistics Workbook for Evidence-Based Health Care; John Wiley & Sons: Hoboken, NJ, USA, 2009. [Google Scholar]
- Flores-León, A.F.; Quezada, V.C.L.; Hernández, M.J.M.; Reinoso, D.A.S.; de la Rosa, J.F.B. Effect of Ankle Range of Motion Modification on Dynamic Valgus Index during a Monopodal Squat in Female Soccer Players. Retos 2022, 45, 952–959. [Google Scholar] [CrossRef]
- Mauntel, T.C.; Frank, B.S.; Begalle, R.L.; Blackburn, J.T.; Padua, D.A. Kinematic Differences between Those with and without Medial Knee Displacement during a Single-Leg Squat. J. Appl. Biomech. 2014, 30, 707–712. [Google Scholar] [CrossRef]
- Mauntel, T.C.; Begalle, R.; Cram, T.; Frank, B.; Hirth, C.; Blackburn, T.; Padua, D. The Effects of Lower Extremity Muscle Activation and Passive Range of Motion on Single Leg Squat Performance. J. Strength Cond. Res. 2013, 27, 1813–1823. [Google Scholar] [CrossRef]
- Miyamoto, N.; Hirata, K.; Kimura, N.; Miyamoto-Mikami, E. Contributions of Hamstring Stiffness to Straight-Leg-Raise and Sit-and-Reach Test Scores. Int. J. Sports Med. 2018, 39, 110–114. [Google Scholar] [CrossRef]
- Sonesson, S.; Hägglund, M.; Kvist, J.; Torvaldsson, K.; Lindblom, H.; Fältström, A. Neuromuscular Control and Hop Performance in Youth and Adult Male and Female Football Players. Phys. Ther. Sport 2022, 55, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Willson, J.D.; Davis, I.S. Utility of the Frontal Plane Projection Angle in Females with Patellofemoral Pain. J. Orthop. Sports Phys. Ther. 2008, 38, 606–615. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics (n = 43) | Scores |
|---|---|
| Age (years), median (IQR) | 13.2 (1.7) |
| Height (cm), mean (SD) | 164.3 (9.3) |
| Body mass (kg), median (IQR) | 45.7 (13.6) |
| APHV, mean (SD) | 14.0 (0.6) |
| Maturity offset (years), mean (SD) | −0.6 (1.0) |
| Football training experience (years), median (IQR) | 6.0 (3.0) |
| Variables (n = 43) | Scores |
|---|---|
| Range of Motion | |
| PSLR (degrees), median (IQR) | 75.0 (17.0) |
| Hip IR (degrees), median (IQR) | 40.0 (18.0) |
| Hip ER (degrees), mean (SD) | 45.2 (12.2) |
| Sit and Reach Test (cm), mean (SD) | 3.1 (5.4) |
| WBLT (cm) median (IQR) | 12.0 (5.0) |
| mSEBT—Dynamic Balance | |
| ANT (LL%), median (IQR) | 68.5 (16.8) |
| PL (LL%), mean (SD) | 99.8 (13.2) |
| PM (LL%), median (IQR) | 98.2 (10.2) |
| COM (LL%), median (IQR) | 89.0 (12.6) |
| Jump Performance | |
| CMJ (cm), mean (SD) | 30.7 (4.9) |
| SLHD (cm), median (IQR) | 184.3 (26.6) |
| FPPA—Dynamic Valgus Angles | |
| SLS (degrees), mean (SD) | 16.4 (8.6) |
| SLL (degrees), median (IQR) | 6.66 (11.33) |
| Knee Valgus Angles (FPPA) | ||||
|---|---|---|---|---|
| Single-Leg Squat | Single-Leg Landing | |||
| Correlation Coefficient | p-Value | Correlation Coefficient | p-Value | |
| Range of Motion | ||||
| PSLR | −0.264 b | 0.086 | −0.157 b | 0.313 |
| Hip IR ROM | −0.114 b | 0.467 | −0.321 b | 0.036 * |
| Hip ER ROM | −0.341 a | 0.029 * | −0.345 b | 0.023 * |
| Sit and Reach test | 0.341 a | 0.025 * | 0.329 b | 0.031 * |
| WBLT | 0.009 b | 0.949 | −0.347 b | 0.022 * |
| Anthropometric characteristics | ||||
| Age | −0.154 b | 0.323 | −0.176 b | 0.323 |
| Maturity offset | −0.141 a | 0.368 | 0.277 a | 0.860 |
| APHV | −0.062 a | 0.694 | −0.255 a | 0.098 |
| Knee Valgus Angles (FPPA) | ||||
|---|---|---|---|---|
| Single-Leg Squat | Single-Leg Landing | |||
| Correlation Coefficient | p-Value | Correlation Coefficient | p-Value | |
| SEBT—Dynamic Balance | ||||
| ANT | −0.066 b | 0.674 | −0.149 b | 0.334 |
| PL | 0.076 a | 0.627 | −0.085 b | 0.586 |
| PM | −0.046 b | 0.768 | −0.275 b | 0.074 * |
| COM left | −0.031 b | 0.841 | −0.188 b | 0.226 |
| COM right | −0.035 b | 0.822 | −0.132 b | 0.397 |
| Jump Performance | ||||
| CMJ | −0.232 a | 0.147 | −0.115 b | 0.463 |
| SLHD | −0.200 b | 0.198 | −0.106 b | 0.499 |
| r | r2 | p-Value | Strength | |
|---|---|---|---|---|
| Single-Leg Squat | ||||
| Hip ER ROM | 0.336 | 0.113 | 0.027 * | Moderate |
| Sit and reach test | 0.341 | 0.116 | 0.025 * | Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilczyński, B.; Radzimiński, Ł.; Sobierajska-Rek, A.; Zorena, K. Association between Selected Screening Tests and Knee Alignment in Single-Leg Tasks among Young Football Players. Int. J. Environ. Res. Public Health 2022, 19, 6719. https://doi.org/10.3390/ijerph19116719
Wilczyński B, Radzimiński Ł, Sobierajska-Rek A, Zorena K. Association between Selected Screening Tests and Knee Alignment in Single-Leg Tasks among Young Football Players. International Journal of Environmental Research and Public Health. 2022; 19(11):6719. https://doi.org/10.3390/ijerph19116719
Chicago/Turabian StyleWilczyński, Bartosz, Łukasz Radzimiński, Agnieszka Sobierajska-Rek, and Katarzyna Zorena. 2022. "Association between Selected Screening Tests and Knee Alignment in Single-Leg Tasks among Young Football Players" International Journal of Environmental Research and Public Health 19, no. 11: 6719. https://doi.org/10.3390/ijerph19116719
APA StyleWilczyński, B., Radzimiński, Ł., Sobierajska-Rek, A., & Zorena, K. (2022). Association between Selected Screening Tests and Knee Alignment in Single-Leg Tasks among Young Football Players. International Journal of Environmental Research and Public Health, 19(11), 6719. https://doi.org/10.3390/ijerph19116719