
Analysis of Work Related Factors, Behavior, Well-Being Outcome, and Job Satisfaction of Workers of Emergency Medical Service: A Systematic Review


Abstract
:1. Introduction
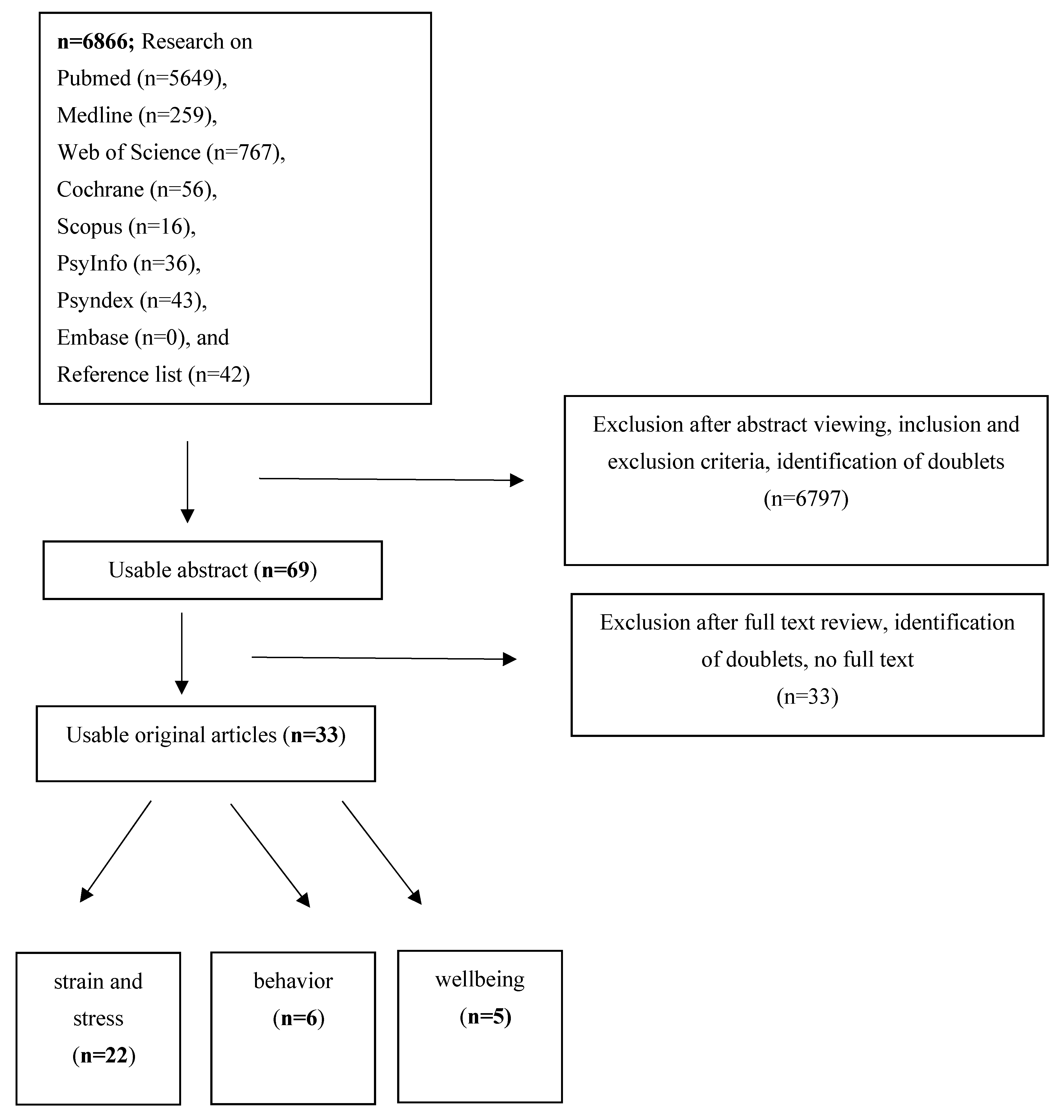
2. Materials and Methods
3. Results
3.1. General Results
3.2. Interpretations of the Studies on Behavior
3.3. Interpretations of the Studies on Stress and Strain
3.4. Interpretations of the Studies on Well-Being
3.5. Evaluation Quality Assessment (EPHPP)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schumann, H. Belastungen und Beanspruchungen von Einsatzkräften im Rettungsdienst—Eine vergleichende Analyse Zwischen Hilfsorganisationen und Berufsfeuerwehren, 1st ed.; Stumpf+Kossendey Verlag: Edewecht, Germany, 2020; ISBN 978-3-96461-028-7. [Google Scholar]
- Donnelly, E. Work-Related Stress and Posttraumatic Stress in Emergency Medical Services. Prehospital Emerg. Care 2012, 16, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Mountfort, S.; Wilson, J. EMS Provider Health And Wellness; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Goh, J.; Pfeffer, J.; Zenios, S.A.; Rajpal, S. Workplace stressors & health outcomes: Health policy for the workplace. Behav. Sci. Policy 2015, 1, 43–52. [Google Scholar]
- Thielmann, B.; Pohl, R.; Böckelmann, I. Heart rate variability as a strain indicator for psychological stress for emergency physicians during work and alert intervention: A systematic review. J. Occup. Med. Toxicol. 2021, 16, 24. [Google Scholar] [CrossRef] [PubMed]
- Mache, S.; Vitzthum, K.; Klapp, B.F.; Danzer, G. Surgeons’ work engagement: Influencing factors and relations to job and life satisfaction. Surgeon 2014, 12, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Faragher, E.B.; Cass, M.; Cooper, C. The relationship between job satisfaction and health: A meta-analysis. Occup. Environ. Med. 2005, 62, 105–112. [Google Scholar] [CrossRef]
- Leedal, J.M.; Smith, A.F. Methodological approaches to anaesthetists’ workload in the operating theatre. Br. J. Anaesth. 2005, 94, 702–709. [Google Scholar] [CrossRef] [Green Version]
- Maharaj, S.; Lees, T.; Lal, S. Prevalence and Risk Factors of Depression, Anxiety, and Stress in a Cohort of Australian Nurses. Int. J. Environ. Res. Public Health 2018, 16, 61. [Google Scholar] [CrossRef] [Green Version]
- Backé, E.M.; Seidler, A.; Latza, U.; Rossnagel, K.; Schumann, B. The role of psychosocial stress at work for the development of cardiovascular diseases: A systematic review. Int. Arch. Occup. Environ. Health 2012, 85, 67–79. [Google Scholar] [CrossRef] [Green Version]
- Rohmert, W.; Rutenfranz, J. Arbeitswissenschaftliche Beurteilung der Belastung und Beanspruchung an Unterschiedlichen Industriellen Arbeitsplätzen; Bundesminister für Arbeit und Sozialordnung, Referat Öffentlichkeitsarbeit: Bonn, Germany, 1975. [Google Scholar]
- Kallus, K.W.; Uhlig, T. Erholungsforschung: Neue Perspektiven zum Verständnis von Streß. In Psychologie 2000. Bericht über den 42. Kongreß der Deutschen Gesellschaft für Psychologie in Jena 2000; Silbereisen, R.K., Reitzle, M., Eds.; Pabst Science Publishers: Lengerich, Germany; Berlin, Germany; Riga, Latvia; Rome, Italy; Vienna, Austria; Zagreb, Croatia, 2001; pp. 364–379. [Google Scholar]
- Lecic-Tosevski, D.; Vukovic, O.; Stepanovic, J. Stress and personality. Psychiatriki 2011, 22, 290–297. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Evans, N.; Lasen, M.; Tsey, K. A Systematic Review of Rural Development Research: Characteristics, Design Quality and Engagement with Sustainability, 1st ed.; Springer: Cham, Germany, 2015; ISBN 978-3-319-17283-5. [Google Scholar]
- Van der Ploeg, E. Acute and chronic job stressors among ambulance personnel: Predictors of health symptoms. Occup. Environ. Med. 2003, 60, i40–i46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soravia, L.M.; Schwab, S.; Walther, S.; Muller, T. Rescuers at Risk: Posttraumatic Stress Symptoms Among Police Officers, Fire Fighters, Ambulance Personnel, and Emergency and Psychiatric Nurses. Front. Psychiatry 2020, 11, 602064. [Google Scholar] [CrossRef] [PubMed]
- Rybojad, B.; Aftyka, A.; Baran, M.; Rzońca, P. Risk Factors for Posttraumatic Stress Disorder in Polish Paramedics: A Pilot Study. J. Emerg. Med. 2016, 50, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Popa, F.; Arafat, R.; Purcărea, V.; Lală, A.; Bobîrnac, G. Occupational Burnout levels in Emergency Medicine–a nationwide study and analysis. J. Med. Life 2010, 3, 207–215. [Google Scholar]
- Okada, N.; Ishii, N.; Nakata, M.; Nakayama, S. Occupational Stress among Japanese Emergency Medical Technicians: Hyogo Prefecture. Prehospital Disaster Med. 2005, 20, 115–121. [Google Scholar] [CrossRef]
- Mishra, S.; Goebert, D.; Char, E.; Dukes, P.; Ahmed, I. Trauma exposure and symptoms of post-traumatic stress disorder in emergency medical services personnel in Hawaii. Emerg. Med. J. 2010, 27, 708–711. [Google Scholar] [CrossRef]
- Maguire, B.J.; Browne, M.; O’Neill, B.J.; Dealy, M.T.; Clare, D.; O’Meara, P. International Survey of Violence Against EMS Personnel: Physical Violence Report. Prehospital Disaster Med. 2018, 33, 526–531. [Google Scholar] [CrossRef]
- Ma, I.C.; Chang, W.H.; Wu, C.L.; Lin, C.H. Risks of post-traumatic stress disorder among emergency medical technicians who responded to the 2016 Taiwan earthquake. J. Formos. Med. Assoc. 2020, 119, 1360–1371. [Google Scholar] [CrossRef]
- Khashaba, E.O.; Neatmatallah, M.A.; El-Sherif, M.A.F.; Ibrahim, A.A.W. Work-related psychosocial hazards among emergency medical responders (EMRS) in Mansoura city. Indian J. Community Med. 2014, 39, 103–110. [Google Scholar] [CrossRef]
- Jonsson, A.; Segesten, K.; Mattsson, B. Post-traumatic stress among Swedish ambulance personnel. Emerg. Med. J. 2003, 20, 79–84. [Google Scholar] [CrossRef] [Green Version]
- Iranmanesh, S.; Tirgari, B.; Bardsiri, H.S. Post-traumatic stress disorder among paramedic and hospital emergency personnel in south-east Iran. World J. Emerg. Med. 2013, 4, 26–31. [Google Scholar] [CrossRef] [Green Version]
- Iorga, M.; Dascalu, N.; Soponaru, C.; Ioan, B. Burnout syndrome among public ambulance staff. Rev. Med. Chir. Soc. Med. Nat. Iasi. 2015, 119, 1128–1132. [Google Scholar]
- Hruska, B.; Barduhn, M.S. Dynamic psychosocial risk and protective factors associated with mental health in Emergency Medical Service (EMS) personnel. J. Affect. Disord. 2021, 282, 9–17. [Google Scholar] [CrossRef]
- Deniz, T.; Saygun, M.; Eroğlu, O.; Ülger, H.; Azapoğlu, B. Effect of exposure to violence on the development of burnoutsyndrome in ambulance staff. Turk. J. Med. Sci. 2016, 46, 296–302. [Google Scholar] [CrossRef]
- Crowe, R.P.; Bower, J.K.; Cash, R.E.; Panchal, A.R.; Rodriguez, S.A.; Olivo-Marston, S.E. Association of Burnout with Workforce-Reducing Factors among EMS Professionals. Prehospital Emerg. Care 2018, 22, 229–236. [Google Scholar] [CrossRef]
- Cash, R.E.; Anderson, S.E.; Lancaster, K.E.; Lu, B.; Rivard, M.K.; Camargo, A.C., Jr.; Panchal, A.R. Comparing the Prevalence of Poor Sleep and Stress Metrics in Basic versus Advanced Life Support Emergency Medical Services Personnel. Prehospital Emerg. Care 2020, 24, 644–656. [Google Scholar] [CrossRef]
- Braun, D.; Theiler, L.; Brähler, E.; Petrowski, K. Hormonal and Subjectively Perceived Stress of the Emergency Physicians of the Airborne Rescue Service. J. Clin. Psychol. Med. Settings 2021, 28, 771–780. [Google Scholar] [CrossRef]
- Berth, H.; Rohleder, P.M. Berufliche Gratifikationskrisen im Rettungsdienst—Eine Querschnittstudie zu Häufigkeit und Einflussfaktoren bei hauptamtlich tätigem Rettungsdienstpersonal. PPmP—Psychother. Psychosom. Med. Psychol. 2019, 69, 224–230. [Google Scholar] [CrossRef]
- Berger, W.; Figueira, I.; Maurat, A.M.; Bucassio, P.; Vieira, I.; Jardim, S.R.; Coutinho, E.S.F.; Mari, J.J.; Mendlowicz, M.V. Partial and full PTSD in Brazilian ambulance workers: Prevalence and impact on health and on quality of life. J. Trauma. Stress 2007, 20, 637–642. [Google Scholar] [CrossRef]
- Bennett, P.; Williams, Y.; Page, N.; Hood, K.; Woollard, M.; Vetter, N.; Reicher, S. Associations between organizational and incident factors and emotional distress in emergency ambulance personnel. Br. J. Clin. Psychol. 2005, 44, 215–226. [Google Scholar] [CrossRef]
- Almutairi, M.N.; El Mahalli, A.A. Burnout and Coping Methods among Emergency Medical Services Professionals. J. Multidiscip. Health 2020, 13, 271–279. [Google Scholar] [CrossRef] [Green Version]
- Alexander, D.A.; Klein, S. Ambulance personnel and critical incidents. Br. J. Psychiatry 2001, 178, 76–81. [Google Scholar] [CrossRef] [Green Version]
- Bahadori, M.; Ravangard, R.; Raadabadi, M.; Hosseini-Shokouh, S.M.; Behzadnia, M.J. Job Stress and Job Burnout Based on Personality Traits among Emergency Medical Technicians. Trauma Mon. 2019, 24, 24–31. [Google Scholar] [CrossRef]
- Thielmann, B.; Böckelmann, I.; Schumann, H. Work-Related Behavior and Experience Patterns Among Ambulance Service Personnel of Different Organizational Structures in Urban and Rural Regions. J. Occup. Environ. Med. 2021, 64, 26–33. [Google Scholar] [CrossRef]
- Sterud, T.; Hem, E.; Ekeberg, O.; Lau, B. Occupational Stress and Alcohol Use: A Study of Two Nationwide Samples of Operational Police and Ambulance, Personnel in Norway. J. Stud. Alcohol Drugs 2007, 68, 896–904. [Google Scholar] [CrossRef]
- Nirel, N.; Goldwag, R.; Feigenberg, Z.; Abadi, D.; Halpern, P. Stress, Work Overload, Burnout, and Satisfaction among Paramedics in Israel. Prehospital Disaster Med. 2008, 23, 537–546. [Google Scholar] [CrossRef] [Green Version]
- Kirby, R.; Shakespeare-Finch, J.; Palk, G. Adaptive and maladaptive coping strategies predict posttrauma outcomes in ambulance personnel. Traumatology 2011, 17, 25–34. [Google Scholar] [CrossRef] [Green Version]
- Guadagni, V.; Cook, E.; Hart, C.; Burles, F.; Iaria, G. Poor sleep quality affects empathic responses in experienced paramedics. Sleep Biol. Rhythm. 2018, 16, 365–368. [Google Scholar] [CrossRef]
- Sterud, T.; Hem, E.; Lau, B.; Ekeberg, O. Suicidal ideation and suicide attempts in a nationwide sample of operational Norwegian ambulance personnel. J. Occup. Health 2008, 50, 406–414. [Google Scholar] [CrossRef] [Green Version]
- Sterud, T.; Hem, E.; Ekeberg, O.; Lau, B. Health problems and help-seeking in a nationwide sample of operational Norwegian ambulance personnel. BMC Public Health 2008, 8, 3. [Google Scholar] [CrossRef] [Green Version]
- Heringshausen, G.; Karutz, H.; Brauchle, G. Wohlbefinden, Lebenszufriedenheit und Work-Family-Konflikt bei Einsatzkräften im Rettungsdienst. Notf. Rett. 2010, 13, 227–233. [Google Scholar] [CrossRef]
- Gayton, S.D.; Lovell, G.P. Resilience in ambulance service paramedics and its relationships with well-being and general health. Traumatology 2012, 18, 58–64. [Google Scholar] [CrossRef]
- Schumann, H.; Böckelmann, I.; Thielmann, B. Belastungserleben während der Corona-Pandemie-Wellen. Was denken die Einsatzkräfte? Rettungsdienst 2021, 44, 712–715. [Google Scholar]
- Schumann, H.; Nübling, M.; Stoltze, K.; Böckelmann, I. Auswirkungen von Führungsverhalten und sozialer Beziehung auf Belastungsfolgen im Rettungsdienst. Zbl. Arb. 2017, 67, 245–254. [Google Scholar] [CrossRef]
- Scheuch, K. Disease caused by psychological stress on the job—what is assured? Dtsch. Med. Wochenschr. 2007, 132, 601–602. [Google Scholar] [CrossRef]
- Roth, K.; Baier, N.; Felgner, S.; Busse, R.; Henschke, C. Association between Safety Culture and Risk of Burnout: A Survey of Non-Medical Rescue Workers. Gesundheitswesen 2022, 84, 199–207. [Google Scholar]
- Cerasoli, C.P.; Nicklin, J.M.; Ford, M.T. Intrinsic motivation and extrinsic incentives jointly predict performance: A 40-year meta-analysis. Psychol. Bull. 2014, 140, 980–1008. [Google Scholar] [CrossRef]

{kind=link}
| Author t Country | Subject Number; Gender; Age (Mean ± SD, Years) | Questionnaire Task |
|---|---|---|
| Bahadori #, 2019 [38] Iran | 308 EMS; 100% ♂; 30.0 ± 5.4 | HSE, MBI NEO-FFI |
| Guadagni, 2018 [43] Canada | 41 (12 PM, 13 PM trainees, 16 CG); 51% ♀, 49% ♂; PM 33.2 ± 5.47; PM trainees 25.8 ± 6; CG 23 ± 7.1 | PSQI, STAI, BDI, Davidson Trauma Scale, Emotional Empathy task |
| Kirby, 2011 [42] Australia | 118; 34% ♀, 66% ♂; 37.0 ± 10.5 | PTGI, IES-R, R- COPE |
| Nirel √, 2008 [41] Israel | 328 PM; 13% ♀, 87% ♂; 22 to ->40 | n.s. work overload, satisfaction with choice of profession, job satisfaction, burnout measure, satisfaction with the choice of profession |
| Sterud, 2007 [40] Norway | 1096; 23% ♀, 77% ♂, 36.8 ± 9.3 (18–66) | AUDIT, Drinking to cope, MBI, Job Stress Survey, BCI |
| Thielmann, 2021 [39] Germany | 276 (125 AOT, 70 PFD, 81 AOC); 5.4% ♀, 94.6% ♂; 39.3 ± 8.0 | AVEM |
| Author t Country | Subjects Number; Gender; Age (Mean ± SD, Years) | Questionnaire Task |
|---|---|---|
| Alexander, 2001 [37] UK | 110 (40 PM, 70 EMT); 14% ♀, 86% ♂; 30–39 | GHQ-28, IES, MBI, HS, PMI, CMC |
| ALmutairi, 2020 [36] Saudi Arabia | 270 EMS; 100% ♂; 30–38 | MBI, CMC |
| Bennett ≈, 2005 [35] UK | 617 (194 EMT, 380 PM, 43 n.n.); 15% ♀, 83% ♂; 2% n.r. 39,6 ± 10.6 | AWSQ, PDS, HADS, CAQ |
| Berger, 2007 [34] Brazil | 234 (29 % EP); 23% ♀, 77% ♂; 32.6 ± 8.1 | PCL-L, SF-36 |
| Berth, 2018 [33] Germany | 82 EMS; 27% ♀, 73% ♂; 32.8 ± 10.9 | ERI, SOP-2, OSSS, MOB-K, PHQ-4 |
| Braun, 2021 [32] Germany, Switzerland | 40 EP; 30% ♀, 70% ♂; 40.7 ± 6.5 | CAR, HRV, TICS, PSS |
| Cash, 2020 [31] USA | 17,522 EMS; 27% ♀, 73% ♂; 34.2 ± 0.1 | PSQI, PSS, Chronic burden scale |
| Crowe, 2019 [30] USA | 1721 EMS; 26% ♀, 74% ♂; 19–75 | CBI, Questionnaire of job demands and resources proposed by Demerouti et al. as a foundation, |
| Deniz, 2015 [29] Turkey | 120 ambulance staff; 47% ♀, 53% ♂; 29.5 ± 6.5 | MBI, exposure to violence |
| Hruska ≈, 2021 [28] USA | 79 EMS; 49% ♀, 51% ♂; 30.7 ± 9.4 | SF-PCL-5, MHI-d, Checklist for occupational stressors, Consensus Sleep diary (CSD), social conflict, 3-items of the Brief COPE, PEAT, ISSB, Perceived Prosocial Impact |
| Iorga, 2015 [27] Romania | 122 EP, EMS; 51% ♀, 49% ♂; age n.r. | TAS-20, MBI, Job Satisfaction Questionnaire |
| Iranmanesh, 2013 [26] Iran | 400 (150 PM, 250 HEP); 43% ♀, 57% ♂; PM: 29.3 ± 6.0 EMS: 31.2 ± 6.3 | M-PTSD |
| Jonsson, 2003 [25] Sweden | 362 EMS; 21% ♀, 79% ♂; 38.4 ± 7.9 | SOC, IES-15, PTSS-10, traumatic events |
| Khashaba, 2014 [24] Egypt | 280 (140 EMT, 140 CG); 100% ♂; 37 ± 9.4 | MBI, BDI, DTS |
| Ma, 2020 [23] Taiwan | 447 EMT; 6.5% ♀, 93.5% ♂; 38.8 ± 8.4 | PCL |
| Maguire, 2018 [22] US international | 1.747; 31% ♀, 69% ♂; ≤25 to >55 | n.s. |
| Mishra, 2010 [21] USA | 101 EMS; 43% ♀, 57% ♂; 35–54 | PCL-C |
| Okada, 2005 [20] Japan | 1551 PM/EMT; 1% ♀, 99% ♂; 34.6 ± 8.2 | n.s. physical stress, mental stress (environment, worksite, symptoms) |
| Popa, 2010 [19] Romania | 258 PM, 1.395 ambulance drivers, 243 EP; n.r.; n.r. | MBI-HSS |
| Rybojad, 2016 [18] Poland | 100 EMS; 14% ♀, 86% ♂; 33.6 ± 9.3 | IES-R |
| Soravia, 2021 [17] Switzerland | 97; 43% ♀, 57% ♂; 38.7 ± 10.0 | PTSS, GHQ-12, BSI, PSES, Coping strategies, Suicidal ideation |
| van der Ploeg, 2003 [16] Netherland | 123; 14% ♀, 86% ♂; 39.8 ± 7.1 | QEAW, IES, CIS, MBI |
| Author t Country | Subjects Number; Gender; Age (Mean ± SD, Years) | Questionnaire Task |
|---|---|---|
| Gayton, 2012 [47] Austria | 219; 11% ♀, 89% ♂; age groups (mean 22–43) | CD-RISC, SFWL, GHQ-28 |
| Heringshausen ∞, 2010 [46] Austria/Germany | 545 EMS; 11% ♀, 89% ♂; 38.0 ± 9.6 | WHO-5, SWLS, WFC |
| Sterud, 2008a [45] Norway | 1180 EMS, 31,987 CG; 23% ♀, 77% ♂; 36.8 ± 9.3 | HADS, Karolinska Sleep Questionnaire, SHC, Need for Recovery after Work Scale |
| Sterud, 2008b [44] Norway | 1180 EMS; 23% ♀, 77% ♂; 36.8 ± 9.3 | HADS, BCI, RSES, JSS, MBI-HSS, Paykel’s Suicidal Feelings in the General Population questionnaire, SHC |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thielmann, B.; Schnell, J.; Böckelmann, I.; Schumann, H. Analysis of Work Related Factors, Behavior, Well-Being Outcome, and Job Satisfaction of Workers of Emergency Medical Service: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 6660. https://doi.org/10.3390/ijerph19116660
Thielmann B, Schnell J, Böckelmann I, Schumann H. Analysis of Work Related Factors, Behavior, Well-Being Outcome, and Job Satisfaction of Workers of Emergency Medical Service: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(11):6660. https://doi.org/10.3390/ijerph19116660
Chicago/Turabian StyleThielmann, Beatrice, Julia Schnell, Irina Böckelmann, and Heiko Schumann. 2022. "Analysis of Work Related Factors, Behavior, Well-Being Outcome, and Job Satisfaction of Workers of Emergency Medical Service: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 11: 6660. https://doi.org/10.3390/ijerph19116660
APA StyleThielmann, B., Schnell, J., Böckelmann, I., & Schumann, H. (2022). Analysis of Work Related Factors, Behavior, Well-Being Outcome, and Job Satisfaction of Workers of Emergency Medical Service: A Systematic Review. International Journal of Environmental Research and Public Health, 19(11), 6660. https://doi.org/10.3390/ijerph19116660