
Treatment Adherence and Health-Related Quality of Life in Patients with Hemophilia in Hong Kong

 , and
, and 
Abstract
:1. Introduction
2. Methods
2.1. Study Procedures
2.2. HRQoL Assessment Tool
2.3. Adherence Measurement Tool
2.4. Statistical Analysis
3. Results
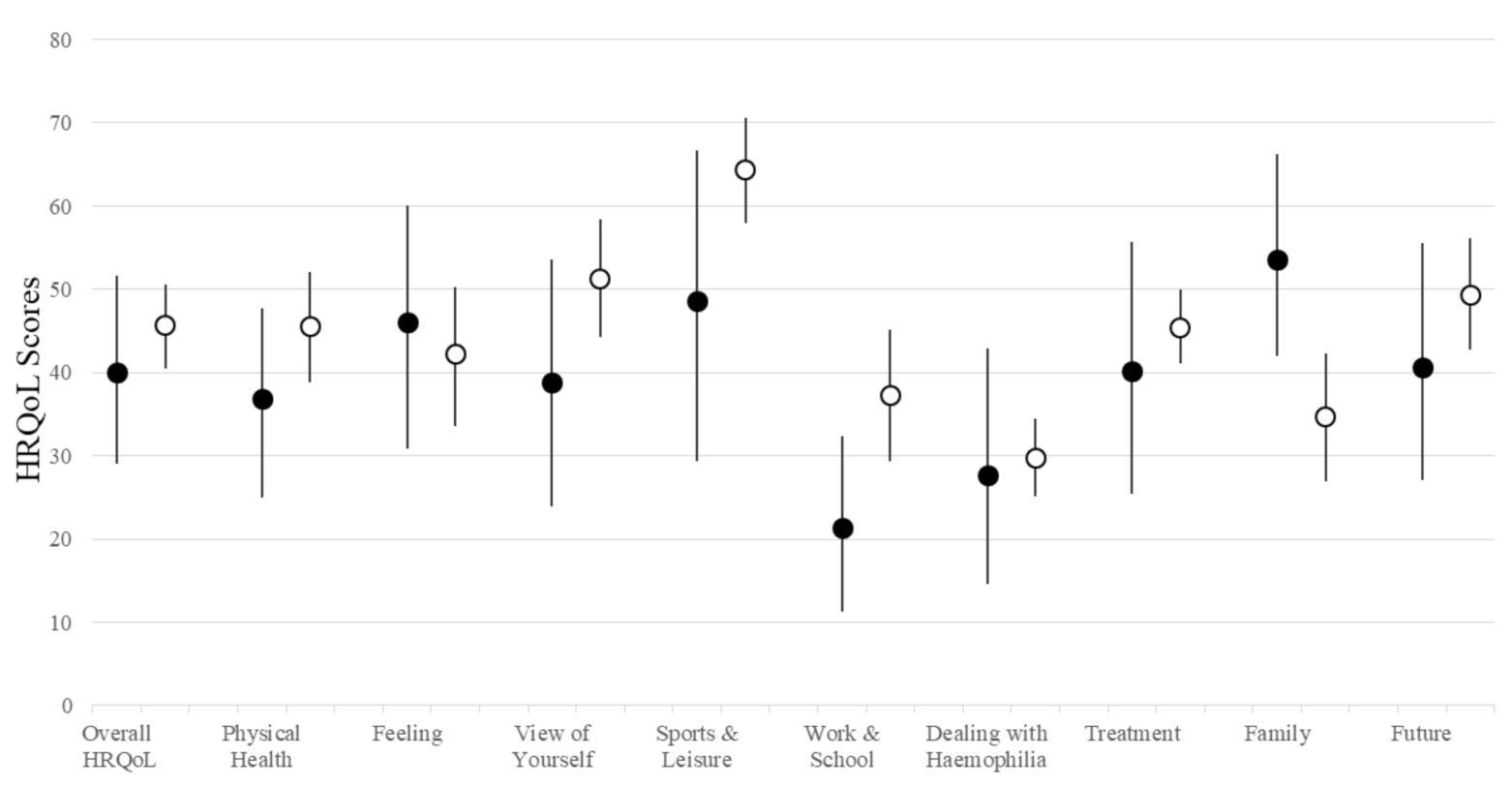
3.1. HRQoL
3.2. Adherence
3.3. Correlation between Adherence and HRQoL
3.4. Exploratory Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berntorp, E.; Shapiro, A.D. Modern haemophilia care. Lancet 2012, 379, 1447–1456. [Google Scholar] [CrossRef]
- Peyvandi, F.; Garagiola, I.; Young, G. The past and future of haemophilia: Diagnosis, treatments, and its complications. Lancet 2016, 388, 187–197. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. United States. Data & Statistics on Hemophilia. National Center on Birth Defects and Developmental Disabilities. Available online: https://www.cdc.gov/ncbddd/hemophilia/data.html (accessed on 17 May 2022).
- Knobe, K.; Berntorp, E. Haemophilia and Joint Disease: Pathophysiology, Evaluation, and Management. J. Comorbidity 2011, 1, 51–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davari, M.; Gharibnaseri, Z.; Ravanbod, R.; Sadeghi, A. Health Status and Quality of Life in Patients with Severe Hemophilia A: A Cross-Sectional Survey. Hematol. Rep. 2019, 11, 7894. [Google Scholar] [CrossRef] [Green Version]
- Baek, H.J.; Park, Y.S.; Yoo, K.Y.; Cha, J.-H.; Kim, Y.-J.; Lee, K.S. Health-related quality of life of moderate and severe haemophilia patients: Results of the haemophilia-specific quality of life index in Korea. PLoS ONE 2020, 15, e0238686. [Google Scholar] [CrossRef]
- Trindade, G.C.; Viggiano, L.G.D.L.; Brant, E.R.; Lopes, C.A.D.O.; de Faria, M.L.; Ribeiro, P.H.N.D.S.; Silva, A.F.D.C.; Souza, D.M.D.R.; Lopes, A.D.F.; Soares, J.M.A.; et al. Evaluation of quality of life in hemophilia patients using the WHOQOL-bref and Haemo-A-Qol questionnaires. Hematol. Transfus. Cell Ther. 2019, 41, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Auerswald, G.; Dolan, G.; Duffy, A.; Hermans, C.; Jiménez-Yuste, V.; Ljung, R.; Morfini, M.; Lambert, T.; Šalek, S.Z. Pain and pain management in haemophilia. Blood Coagul. Fibrinolysis 2016, 27, 845–854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palareti, L.; Potì, S.; Cassis, F.; Emiliani, F.; Matino, D.; Iorio, A. Shared topics on the experience of people with haemophilia living in the UK and the USA and the influence of individual and contextual variables: Results from the HERO qualitative study. Int. J. Qual. Stud. Health Well-Being 2015, 10, 28915. [Google Scholar] [CrossRef] [Green Version]
- Niu, J.; Ning, L.; Zhang, Q.; Liu, Z.; Ma, Y.; Xu, X.; Wu, Q.; Hao, Y.; Cui, Y.; Liu, C. Health-related quality of life of patients with haemophilia: A cross-sectional survey in the Northeast of China. BMJ Open 2022, 12, e056668. [Google Scholar] [CrossRef]
- Furuichi, Y.; Nogami, K.; Yada, K.; Nezu, S.; Obayashi, K.; Saeki, K.; Kurumatani, N.; Nakajima, M.; Kinoshita, S.; Shima, M. Assessment of self-/parent-reported quality of life in Japanese children with haemophilia using the Japanese version of KIDSCREEN-52. Haemophilia 2020, 26, 243–250. [Google Scholar] [CrossRef]
- Franchini, M. The modern treatment of haemophilia: A narrative review. Blood Transfus. 2013, 11, 178. [Google Scholar] [CrossRef] [PubMed]
- Royal, S.; Schramm, W.; Berntorp, E.; Giangrande, P.; Gringeri, A.; Ludlam, C.; Kroner, B.; Szucs, T. Quality-of-life differences between prophylactic and on-demand factor replacement therapy in European haemophilia patients. Haemophilia 2002, 8, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, A.; Santagostino, E.; Dougall, A.; Kitchen, S.; Sutherland, M.; Pipe, S.W.; Carcao, M.; Mahlangu, J.; Ragni, M.V.; Windyga, J.; et al. WFH Guidelines for the Management of Hemophilia, 3rd edition. Haemophilia 2020, 26 (Suppl. S6), 1–158. [Google Scholar] [CrossRef]
- Thornburg, C.D.; Duncan, N.A. Treatment adherence in hemophilia. Patient Prefer. Adherence 2017, 11, 1677–1686. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Z.; Riske, B.; Forsberg, A.D.; Ullman, M.; Baker, J.R.; Koerper, M.A.; Curtis, R.G.; Lou, M.; Joanne, W.; Johnson, K.A. Self-Reported Barriers to Hemophilia Care in People with Factor VIII Deficiency. Am. J. Prev. Med. 2011, 41, S346–S353. [Google Scholar] [CrossRef] [Green Version]
- Bago, M.; Butkovic, A.; Zupan, I.P.; Kotnik, B.F.; Prga, I.; Vrca, V.B.; Salek, S.Z. Association between reported medication adherence and health-related quality of life in adult patients with haemophilia. Int. J. Clin. Pharm. 2021, 43, 1500–1507. [Google Scholar] [CrossRef]
- Du Treil, S.; Rice, J.; Leissinger, C.A. Quantifying adherence to treatment and its relationship to quality of life in a well-characterized haemophilia population. Haemophilia 2007, 13, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Au, W.Y.; Lee, V.; Kho, B.; Ling, A.S.C.; Chan, D.; Chan, E.Y.T.; Chan, G.C.F.; Cheung, W.W.W.; Lau, C.W.; Lee, C.Y.; et al. A synopsis of current haemophilia care in Hong Kong. Hong Kong Med. J. 2011, 17, 189. [Google Scholar] [PubMed]
- Song, X.; Zhong, J.; Xue, F.; Chen, L.; Li, H.; Yuan, D.; Xie, J.; Shi, J.; Zhang, L.; Wu, E.Q.; et al. An overview of patients with haemophilia A in China: Epidemiology, disease severity and treatment strategies. Haemophilia 2021, 27, e51–e59. [Google Scholar] [CrossRef]
- Stonebraker, J.S.; Brooker, M.; Amand, R.E.; Farrugia, A.; Srivastava, A. A study of reported factor VIII use around the world. Haemophilia 2010, 16, 33–46. [Google Scholar] [CrossRef]
- The Government of the Hong Kong SAR. Press Releases. LCQ21: Rare Diseases. Available online: https://www.info.gov.hk/gia/general/202102/24/P2021022400468.htm (accessed on 8 October 2021).
- Von Mackensen, S.; Scalone, L.; Ravera, S.; Mantovani, L.; Gringeri, A. Assessment of health-related quality of life in patients with haemophilia with the newly developed haemophilia-specific instrument Haem-A-QoL. Value Health 2005, 8, A127. [Google Scholar] [CrossRef] [Green Version]
- von Mackensen, S.; Gringeri, A. Health-related Quality of Life in Adult Patients with Haemophilia—Assessment with a New Disease-specific Questionnaire (Haem-A-QoL). J. Thromb. Haemost. 2005, 3, P0813. [Google Scholar]
- Von Mackensen, S.; Bullinger, M. Development and testing of an instrument to assess the Quality of Life of Children with Haemophilia in Europe (Haemo-QoL). Haemophilia 2004, 10 (Suppl. S1), 17–25. [Google Scholar] [CrossRef] [PubMed]
- Bullinger, M.; Von Mackensen, S.; Fischer, K.; Khair, K.; Petersen, C.; Ravens-Sieberer, U.; Rocino, A.; Sagnier, P.; Tusell, J.M.; Berg, M.V.D.; et al. Pilot testing of the ‘Haemo-QoL’ quality of life questionnaire for haemophiliac children in six European countries. Haemophilia 2002, 8 (Suppl. S2), 47–54. [Google Scholar] [CrossRef] [PubMed]
- Bradley, C.S.; Bullinger, M.; McCusker, P.J.; Wakefield, C.D.; Blanchette, V.S.; Young, N.L. Comparing two measures of quality of life for children with haemophilia: The CHO-KLAT and the Haemo-QoL. Haemophilia 2006, 12, 643–653. [Google Scholar] [CrossRef] [PubMed]
- Von Mackensen, S.; Eldar-Lissai, A.; Auguste, P.; Krishnan, S.; Von Maltzahn, R.; Yu, R.; Wyrwich, K.W. Measurement properties of the Haem-A-QoL in haemophilia clinical trials. Haemophilia 2017, 23, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Xu, R.H.; Dong, D.; Luo, N.; Wong, E.L.-Y.; Wu, Y.; Yu, S.; Yang, R.; Liu, J.; Yuan, H.; Zhang, S. Evaluating the psychometric properties of the EQ-5D-5L and SF-6D among patients with haemophilia. Eur. J. Health Econ. 2021, 22, 547–557. [Google Scholar] [CrossRef]
- Duncan, N.; Kronenberger, W.; Roberson, C.; Shapiro, A. VERITAS-Pro: A new measure of adherence to prophylactic regimens in haemophilia. Haemophilia 2010, 16, 247–255. [Google Scholar] [CrossRef]
- Krishnan, S.; Vietri, J.; Furlan, R.; Duncan, N. Adherence to prophylaxis is associated with better outcomes in moderate and severe haemophilia: Results of a patient survey. Haemophilia 2015, 21, 64–70. [Google Scholar] [CrossRef]
- Holstein, K.; Eifrig, B.; Länger, F. Relationship between haemophilia and social status. Thromb. Res. 2014, 134 (Suppl. S1), S53–S56. [Google Scholar] [CrossRef]
- Taber, K.S. The Use of Cronbach’s Alpha When Developing and Reporting Research Instruments in Science Education. Res. Sci. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef]
- Gringeri, A.; Von Mackensen, S.; Auerswald, G.; Bullinger, M.; Garrido, R.P.; Kellermann, E.; Khair, K.; Lenk, H.; Vicariot, M.; Villar, A.; et al. Health status and health-related quality of life of children with haemophilia from six West European countries. Haemophilia 2004, 10 (Suppl. S1), 26–33. [Google Scholar] [CrossRef] [PubMed]
- Mahlangu, J.; Oldenburg, J.; Callaghan, M.U.; Shima, M.; Mancuso, M.E.; Trask, P.; Recht, M.; Garcia, C.; Yang, R.; Lehle, M.; et al. Health-related quality of life and health status in persons with haemophilia A with inhibitors: A prospective, multicentre, non-interventional study (NIS). Haemophilia 2019, 25, 382–391. [Google Scholar] [CrossRef] [PubMed]
- Mercan, A.; Sarper, N.; Inanır, M.; Mercan, H.I.; Zengin, E.; Kılıç, S.; Gökalp, A.S. Hemophilia-Specific Quality of Life Index (Haemo-QoL and Haem-A-QoL questionnaires) of children and adults: Result of a single center from Turkey. Pediatr. Hematol. Oncol. 2010, 27, 449–461. [Google Scholar] [CrossRef]
- Witkop, M.; Guelcher, C.; Forsyth, A.; Hawk, S.; Curtis, R.; Kelley, L.; Frick, N.; Rice, M.; Rosu, G.; Cooper, D.L. Treatment outcomes, quality of life, and impact of hemophilia on young adults (aged 18-30 years) with hemophilia. Am. J. Hematol. 2015, 90 (Suppl. S2), S3–S10. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, A.A.; Leite, I.C.G.; Bustamante-Teixeira, M.T.; Corrêa, C.S.L.; Da Cruz, D.T.; Rodrigues, D.D.O.W.; Ferreira, M.C.B. Health-related quality of life in hemophilia: Results of the hemophilia-Specific quality of life index (Haem-a-Qol) at a Brazilian blood center. Rev. Bras. Hematol. Hemoter. 2013, 35, 314–318. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Huang, J.; Kong, X.; Ma, G.; Fang, Y. Health-related quality of life in children with haemophilia in China: A 4-year follow-up prospective cohort study. Health Qual. Life Outcomes 2019, 17, 28. [Google Scholar] [CrossRef] [Green Version]
- Pratap, R.; Misra, M.; Morampudi, S.; Patil, A.; Reddy, J. The existing scenario of haemophilia care in Canada and China—A review. Hematol. Transfus. Cell Ther. 2020, 42, 356–364. [Google Scholar] [CrossRef]
- Flaherty, L.M.; Schoeppe, J.; Kruse-Jarres, R.; Konkle, B.A. Balance, falls, and exercise: Beliefs and experiences in people with hemophilia: A qualitative study. Res. Pract. Thromb. Haemost. 2017, 2, 147–154. [Google Scholar] [CrossRef] [Green Version]
- Bérubé, S.; Amesse, C.; Sultan, S. Illness perceptions and their relation to physical activity in children and adolescents with hemophilia. Health Psychol. Behav. Med. 2020, 8, 461–474. [Google Scholar] [CrossRef]
- Negrier, C.; Seuser, A.; Forsyth, A.; Lobet, S.; Llinas, A.; Rosas, M.; Heijnen, L. The benefits of exercise for patients with haemophilia and recommendations for safe and effective physical activity. Haemophilia 2013, 19, 487–498. [Google Scholar] [CrossRef] [PubMed]
- Goto, M.; Takedani, H.; Yokota, K.; Haga, N. Strategies to encourage physical activity in patients with hemophilia to improve quality of life. J. Blood Med. 2016, 7, 85–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, B.; Seuser, A.; Krüger, S.; Herzig, M.L.; Hilberg, T.; Ay, C.; Hasenöhrl, T.; Crevenna, R. Establishing an online physical exercise program for people with hemophilia. Wien. Klin. Wochenschr. 2019, 131, 558–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandhu, M.K.; Eisenberger, A.; Cohen, A.J. Complications of Aging In Patients with Hemophilia. Blood 2010, 116, 3671. [Google Scholar] [CrossRef]
- Gong, G.-W.; Chen, Y.-C.; Fang, P.-Q.; Min, R. Medical expenditure for patients with hemophilia in urban China: Data from medical insurance information system from 2013 to 2015. Orphanet J. Rare Dis. 2020, 15, 137. [Google Scholar] [CrossRef]
- Mortensen, G.L.; Strand, A.M.; Almén, L. Adherence to prophylactic haemophilic treatment in young patients transitioning to adult care: A qualitative review. Haemophilia 2018, 24, 862–872. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Nicholas, S.; Yang, Y.; Chen, X.; Maitland, E.; Ma, Y.; Shi, X. Medical costs and hospital utilization for hemophilia A and B urban inpatients in China: A national cross-sectional study. BMC Health Serv. Res. 2022, 22, 230. [Google Scholar] [CrossRef]
- Ar, M.C.; Balkan, C.; Kavaklı, K. Extended Half-Life Coagulation Factors: A New Era in the Management of Haemophilia Patients. Turk. J. Hematol. 2019, 36, 141–154. [Google Scholar] [CrossRef]
- Kulkarni, R. Use of telehealth in the delivery of comprehensive care for patients with haemophilia and other inherited bleeding disorders. Haemophilia 2018, 24, 33–42. [Google Scholar] [CrossRef]
- Qian, W.; Lam, T.T.-N.; Lam, H.H.W.; Li, C.-K.; Cheung, Y.T. Telehealth Interventions for Improving Self-Management in Patients With Hemophilia: Scoping Review of Clinical Studies. J. Med. Internet Res. 2019, 21, e12340. [Google Scholar] [CrossRef]
- Cheung, Y.T.; Lam, P.H.; Lam, T.T.-N.; Lam, H.H.W.; Li, C.K. Technology Acceptance Among Patients With Hemophilia in Hong Kong and Their Expectations of a Mobile Health App to Promote Self-management: Survey Study. JMIR Form. Res. 2021, 5, e27985. [Google Scholar] [CrossRef] [PubMed]
- Bolcato, M.; Russo, M.; Trentino, K.; Isbister, J.; Rodriguez, D.; Aprile, A. Patient blood management: The best approach to transfusion medicine risk management. Transfus. Apher. Sci. 2020, 59, 102779. [Google Scholar] [CrossRef] [PubMed]
- Guedes, V.G.; Corrente, J.E.; Farrugia, A.; Thomas, S.; Wachholz, P.A.; Vidal, E.I.D.O. Comparing objective and self-reported measures of adherence in haemophilia. Haemophilia 2019, 25, 821–830. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total (n = 56) | Adult Patients (n = 42) | Pediatric Patients (n = 14) | Parent of Pediatric Patients (n = 14) | |
|---|---|---|---|---|
| Age (years) mean (SD) [range] | 30.4 (17.4) [5.2–68.4] | 37.2 (14.5) [17.5–68.4] | 10.0 (2.8) [5.2–15.1] | 41.5 (6.6) [34.7–55.9] |
| n (%) | n (%) | n (%) | n (%) | |
| Sex | ||||
| Male | 56 (100.0) | 42 (100.0) | 14 (100.0) | 2 (14.3) |
| Female | 0 (0) | 0 (0) | 0 (0) | 12 (85.7) |
| Diagnosis | ||||
| Hemophilia A | 42 (75.0) | 32 (76.2) | 10 (71.5) | / |
| Hemophilia B | 10 (17.9) | 7 (16.7) | 3 (21.4) | / |
| Missing/unsure | 4 (7.1) | 3 (7.1) | 1 (7.1) | / |
| Treatment type | ||||
| Prophylaxis + on-demand therapy | 38 (67.8) | 26 (61.9) | 12 (85.7) | / |
| On-demand therapy | 17 (30.4) | 15 (35.7) | 2 (14.3) | / |
| Missing/unsure | 1 (1.8) | 1 (2.4) | 0 (0) | / |
| Disease Severity | ||||
| Mild | 4 (7.1) | 4 (9.5) | 0 (0) | |
| Moderate | 16 (28.6) | 14 (33.4) | 2 (14.3) | / |
| Severe | 33 (58.9) | 22 (52.3) | 11 (75.6) | / |
| Missing/ unsure | 3 (5.4) | 2 (4.8) | 1 (7.1) | / |
| Highest Education Attainment | ||||
| Secondary school or below | 30 (53.6) | 16 (38.1) | 14 (100) | 10 (71.4) |
| Post-secondary school or above | 26 (46.4) | 26 (61.9) | 0 (0) | 4 (28.6) |
| Types of Housing | ||||
| Public housing | 26 (46.4) | 21 (50.0) | 5 (35.7) | / |
| Private housing | 30 (53.6) | 21 (50.0) | 9 (64.3) | / |
| Total * | Subscales * | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Total | Physical Health | Feeling | View of Yourself | Sports and Leisure | Work and School | Dealing with Hemophilia | Treatment | Family | Future | |
| Age # | p = 0.011 | p = 0.005 | p = 0.17 | p = 0.008 | p = 0.058 | p < 0.0001 | p = 0.34 | p = 0.041 | p = 0.025 | p = 0.054 |
| r = 0.34 | r = 0.37 | r = 0.19 | r = 0.35 | r = 0.26 | r = 0.59 | r = 0.13 | r = 0.28 | r = −0.30 | r = 0.26 | |
| Disease severity | p = 0.71 | p = 0.21 | p = 0.52 | p = 0.69 | p = 0.85 | p = 0.94 | p = 0.54 | p = 0.33 | p = 0.37 | p = 0.48 |
| Mild-moderate | 41.8 (15.3) | 37.8 (22.3) | 38.2 (22.7) | 45.8 (19.6) | 60.3 (23.1) | 32.2 (23.2) | 29.9 (17.4) | 43.4 (17.2) | 35.3 (25.6) | 44.9 (19.7) |
| Severe | 45.1 (18.6) | 45.6 (21.1) | 44.4 (27.3) | 48.6 (25.9) | 61.2 (24.2) | 32.4 (23.1) | 28.7 (20.1) | 44.4 (20.0) | 41.5 (26.6) | 48.5 (24.3) |
| Treatment type | p = 0.039 | p = 0.24 | p = 0.043 | p = 0.34 | p = 0.31 | p = 0.001 | p = 0.53 | p = 0.17 | p = 0.96 | p = 0.21 |
| Prophylaxis | 41.4 (16.8) | 42.4 (19.5) | 38.3 (23.5) | 45.0 (23.0) | 58.1 (24.9) | 25.8 (18.9) | 28.6 (19.8) | 42.4 (19.1) | 39.5 (25.8) | 44.2 (20.1) |
| On-demand | 52.1 (18.6) | 48.2 (25.9) | 56.8 (26.6) | 55.8 (25.6) | 65.3 (24.6) | 51.5 (26.3) | 30.4 (18.6) | 49.4 (18.5) | 40.1 (26.2) | 55.1 (28.1) |
| Housing type | p = 0.073 | p = 0.13 | p = 0.18 | p = 0.25 | p = 0.51 | p = 0.11 | p = 0.46 | p = 0.71 | p = 0.047 | p = 0.041 |
| Public | 48.8 (17.5) | 48.2 (24.1) | 48.5 (28.6) | 53.1 (24.5) | 63.4 (23.3) | 38.2 (25.4) | 30.1 (16.7) | 43.7 (19.5) | 45.9 (20.5) | 53.1 (23.5) |
| Private | 40.4 (17.8) | 39.3 (19.9) | 38.6 (23.3) | 44.0 (23.0) | 58.0 (25.8) | 29.0 (23.1) | 28.4 (21.2) | 44.3 (19.5) | 33.8 (28.3) | 42.0 (21.9) |
| Education Ɨ (Adult patient) | p = 0.036 | p = 0.066 | p = 0.016 | p = 0.036 | p = 0.51 | p = 0.045 | p = 0.94 | p = 0.89 | p = 0.35 | p = 0.16 |
| <Secondary | 52.8 (16.2) | 53.1 (23.9) | 55.1 (24.8) | 60.9 (23.1) | 67.2 (17.7) | 45.7 (22.8) | 29.2 (17.5) | 46.5 (16.0) | 38.7 (22.8) | 57.2 (23.5) |
| Post-secondary | 41.4 (15.7) | 41.0 (20.0) | 34.4 (24.1) | 45.4 (20.0) | 62.7 (20.6) | 32.0 (24.7) | 30.6 (15.4) | 43.8 (13.7) | 32.2 (26.1) | 44.4 (18.8) |
| Total * | Subscales * | ||||||
|---|---|---|---|---|---|---|---|
Range: 24–120 | Time Range: 4–20 | Dose Range: 4–20 | Plan Range: 4–20 | Remember Range: 4–20 | Skip Range: 4–20 | Communicate Range: 4–20 | |
| Age # | p < 0.0001 | p = 0.001 | p = 0.086 | p = 0.61 | p = 0.001 | p < 0.0001 | p = 0.014 |
| r = 0.66 | r = 0.51 | r = 0.28 | r= −0.09 | r = 0.52 | r = 0.63 | r = 0.40 | |
| Disease severity | p = 0.46 | p = 0.21 | p = 0.68 | p = 0.10 | p = 0.66 | p = 0.46 | p = 0.10 |
| Mild-moderate | 59.6 (11.9) | 11.0 (4.2) | 8.8 (4.0) | 10.0 (2.7) | 9.0 (4.4) | 9.2 (4.2) | 11.6 (3.4) |
| Severe | 56.1 (17.3) | 9.0 (4.2) | 8.7 (2.7) | 8.2 (3.4) | 8.3 (4.2) | 8.2 (4.4) | 13.7 (4.8) |
| Housing type | p = 0.38 | p = 0.38 | p = 0.041 | p = 0.38 | p = 0.76 | p = 0.34 | p = 0.39 |
| Public | 60.0 (16.9) | 8.9 (3.8) | 9.6 (2.9) | 9.4 (3.3) | 8.9 (4.5) | 9.3 (4.6) | 13.9 (4.1) |
| Private | 67.2 (17.4) | 12.4 (5.0) | 9.8 (4.7) | 10.2 (1.9) | 11.2 (5.7) | 10.4 (5.3) | 13.2 (4.0) |
| Education Ɨ (Adult patients) | p = 0.85 | p = 0.40 | p = 0.89 | p = 0.85 | p = 0.98 | p = 0.94 | p = 0.68 |
| <Secondary | 62.6 (12.7) | 9.5 (3.3) | 9.1 (3.3) | 8.9 (2.9) | 9.8 (3.5) | 10.0 (4.3) | 15.4 (2.8) |
| Post-secondary | 64.2 (14.5) | 11.6 (4.1) | 9.3 (3.6) | 8.7 (3.6) | 10.2 (4.4) | 10.0 (4.4) | 14.6 (3.6) |
| HRQoL # | Treatment Adherence * | ||||||
|---|---|---|---|---|---|---|---|
| Total Adherence Score | Time | Dose | Plan | Remember | Skip | Communicate | |
| Total HRQoL score | −0.04 | −0.25 | 0.05 | 0.17 | 0.06 | 0.16 | −0.26 |
| Physical Health | −0.11 | −0.059 | 0.01 | −0.08 | 0.10 | 0.29 | 0.17 |
| Feeling | −0.06 | 0.32 Ɨ | 0.12 | 0.07 | 0.26 | 0.15 | −0.14 |
| View of Yourself | 0.16 | 0.23 | 0.21 | 0.04 | 0.19 | 0.32 Ɨ | −0.06 |
| Sport and Leisure | −0.03 | 0.07 | 0.24 | 0.07 | 0.02 | 0.31 Ɨ | 0.20 |
| Work and School | 0.92 | 0.26 | 0.15 | 0.20 | −0.002 | 0.09 | 0.007 |
| Dealing with Hemophilia | 0.17 | −0.08 | −0.03 | 0.31 Ɨ | 0.10 | 0.16 | −0.13 |
| Treatment | 0.21 | −0.24 | −0.003 | 0.28 Ɨ | 0.08 | 0.11 | −0.18 |
| Future | 0.07 | 0.15 | 0.14 | −0.016 | 0.26 | 0.08 | 0.10 |
| Family | −0.18 | −0.001 | 0.33 Ɨ | 0.26 | 0.09 | 0.11 | −0.19 |
| HRQoL Scores * (All Patients) | HRQoL Scores * (Adult Patients Only) | |||||
|---|---|---|---|---|---|---|
| B | 95% CI | p | B | 95% CI | p | |
| Adherence score # | 0.15 | (−0.19, 0.50) | 0.38 | 0.21 | (−0.13, 0.54) | 0.22 |
| Age # | 0.45 | (0.07, 0.83) | 0.021 | 0.42 | (0.093, 0.75) | 0.014 |
| Disease severity | ||||||
| Mild-moderate | ref | |||||
| Severe | 0.31 | (−0.69, 1.31) | 0.54 | 0.90 | (−8.49, 10.29) | 0.85 |
| Housing type | ||||||
| Private | ref | |||||
| Public | 8.30 | (−1.39, 17.97) | 0.091 | 10.24 | (0.70, 19.77) | 0.036 |
| Education Ɨ (Adult patients only) | ||||||
| <Secondary | / | / | / | ref | ||
| Post-secondary | / | / | / | −1.22 | (−10.8, 8.35) | 0.80 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheung, Y.T.; Lam, P.H.; Lam, H.H.W.; Ma, C.-T.; Leung, A.W.K.; Wong, R.S.M.; Li, C.K. Treatment Adherence and Health-Related Quality of Life in Patients with Hemophilia in Hong Kong. Int. J. Environ. Res. Public Health 2022, 19, 6496. https://doi.org/10.3390/ijerph19116496
Cheung YT, Lam PH, Lam HHW, Ma C-T, Leung AWK, Wong RSM, Li CK. Treatment Adherence and Health-Related Quality of Life in Patients with Hemophilia in Hong Kong. International Journal of Environmental Research and Public Health. 2022; 19(11):6496. https://doi.org/10.3390/ijerph19116496
Chicago/Turabian StyleCheung, Yin Ting, Pok Hong Lam, Henry Hon Wai Lam, Chung-Tin Ma, Alex Wing Kwan Leung, Raymond Siu Ming Wong, and Chi Kong Li. 2022. "Treatment Adherence and Health-Related Quality of Life in Patients with Hemophilia in Hong Kong" International Journal of Environmental Research and Public Health 19, no. 11: 6496. https://doi.org/10.3390/ijerph19116496
APA StyleCheung, Y. T., Lam, P. H., Lam, H. H. W., Ma, C.-T., Leung, A. W. K., Wong, R. S. M., & Li, C. K. (2022). Treatment Adherence and Health-Related Quality of Life in Patients with Hemophilia in Hong Kong. International Journal of Environmental Research and Public Health, 19(11), 6496. https://doi.org/10.3390/ijerph19116496