
Profiles of Sleep Duration and Psychological Distress among Puerto Ricans Living in the United States: A Cross-Sectional Survey and Latent Class Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient and Public Involvement
2.2. Latent Class Analysis
2.2.1. Covariates
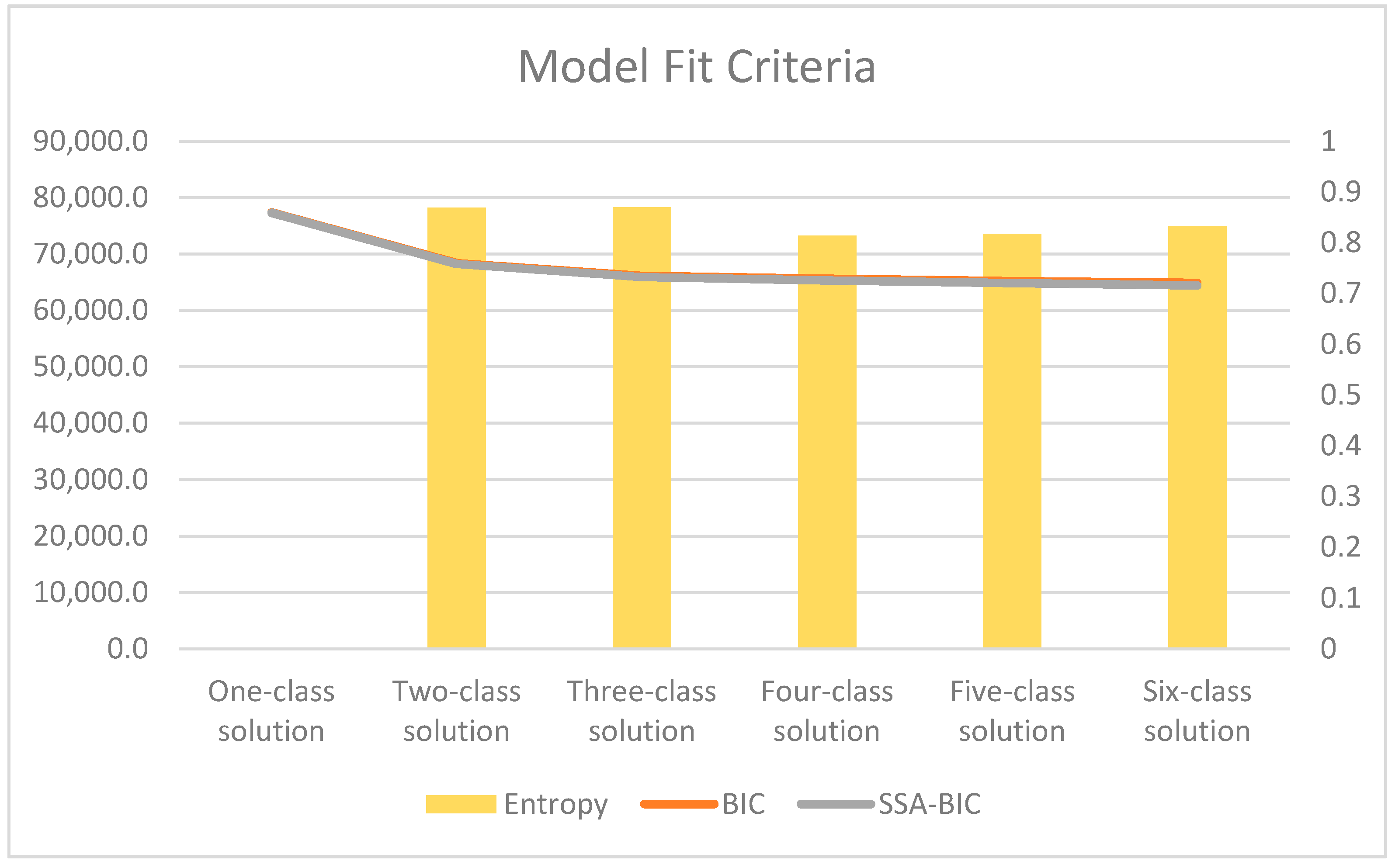
2.2.2. Latent Class Analytic Plan
3. Results
3.1. Latent Class Analysis Findings
3.2. Covariates
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Sleep and Sleep Disorders. 2021. Available online: https://www.cdc.gov/sleep/about_us.html (accessed on 30 September 2021).
- Buxton, O.M.; Marcelli, E. Short and long sleep are positively associated with obesity, diabetes, hypertension, and cardiovascular disease among adults in the United States. Soc. Sci. Med. 2010, 71, 1027–1036. [Google Scholar] [CrossRef] [PubMed]
- Bubu, O.M.; Brannick, M.; Mortimer, J.; Umasabor-Bubu, O.; Sebastião, Y.V.; Wen, Y.; Schwartz, S.; Borenstein, A.R.; Wu, Y.; Morgan, D.; et al. Sleep, Cognitive impairment, and Alzheimer’s disease: A Systematic Review and Meta-Analysis. Sleep 2017, 40, zsw032. [Google Scholar] [CrossRef] [PubMed]
- Ramos, A.R.; Tarraf, W.; Wu, B.; Redline, S.; Cai, J.; Daviglus, M.L.; Gallo, L.; Mossavar-Rahmani, Y.; Perreira, K.M.; Zee, P.; et al. Sleep and neurocognitive decline in the Hispanic Community Health Study/Study of Latinos. Alzheimer’s Dement. 2020, 16, 305–315. [Google Scholar] [CrossRef]
- United States Census Bureau. QuickFacts United States. 2019. Available online: https://www.census.gov/quickfacts/fact/table/US/RHI725219 (accessed on 30 September 2021).
- United States Census Bureau. Hispanic Population to Reach 111 Million by 2060. 2018. Available online: https://www.census.gov/library/visualizations/2018/comm/hispanic-projected-pop.html (accessed on 1 October 2021).
- Hale, L.; Do, D.P. Racial Differences in Self-Reports of Sleep Duration in a Population-Based Study. Sleep 2007, 30, 1096–1103. [Google Scholar] [CrossRef] [Green Version]
- Carnethon, M.R.; De Chavez, P.J.; Zee, P.C.; Kim, K.-Y.A.; Liu, K.; Goldberger, J.J.; Ng, J.; Knutson, K. Disparities in sleep characteristics by race/ethnicity in a population-based sample: Chicago Area Sleep Study. Sleep Med. 2015, 18, 50–55. [Google Scholar] [CrossRef] [Green Version]
- Dudley, K.A.; Weng, J.; Sotres-Alvarez, D.; Simonelli, G.; Feliciano, E.C.; Ramirez, M.; Ramos, A.R.; Loredo, J.S.; Reid, K.J.; Mossavar-Rahmani, Y.; et al. Actigraphic Sleep Patterns of U.S. Hispanics: The Hispanic Community Health Study/Study of Latinos. Sleep 2017, 40, zsw049. [Google Scholar] [CrossRef]
- Gaston, S.A.; E Martinez-Miller, E.; McGrath, J.; Ii, W.B.J.; Napoles, A.; Pérez-Stable, E.; Jackson, C.L. Disparities in multiple sleep characteristics among non-Hispanic White and Hispanic/Latino adults by birthplace and language preference: Cross-sectional results from the US National Health Interview Survey. BMJ Open 2021, 11, e047834. [Google Scholar] [CrossRef]
- Alcántara, C.; Patel, S.; Carnethon, M.; Castaneda, S.; Isasi, C.R.; Davis, S.; Ramos, A.R.; Arredondo, E.; Redline, S.; Zee, P.C.; et al. Stress and sleep: Results from the Hispanic Community Health Study/Study of Latinos Sociocultural Ancillary Study. SSM Popul. Health 2017, 3, 713–721. [Google Scholar] [CrossRef]
- Alegria, M.; Shrout, P.E.; Canino, G.; Alvarez, K.; Wang, Y.; Bird, H.; Markle, S.L.; Ramos-Olazagasti, M.; Rivera, D.V.; Cook, B.L.; et al. The effect of minority status and social context on the development of depression and anxiety: A longitudinal study of Puerto Rican descent youth. World Psychiatry 2019, 18, 298–307. [Google Scholar] [CrossRef] [Green Version]
- Canino, G.; Shrout, P.E.; NeMoyer, A.; Vila, D.; Santiago, K.M.; Garcia, P.; Quiñones, A.; Cruz, V.; Alegria, M. A comparison of the prevalence of psychiatric disorders in Puerto Rico with the United States and the Puerto Rican population of the United States. Soc. Psychiatry 2019, 54, 369–378. [Google Scholar] [CrossRef]
- Garcia, C.; Sheehan, C.M.; Florez-Gonzalez, N.; Ailshire, J.A. Sleep Patterns among US Latinos by Nativity and Country of Origin: Results from the National Health Interview Survey. Ethn. Dis. 2020, 30, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Nylund, K.L.; Asparouhov, T.; Muthén, B.O. Deciding on the Number of Classes in Latent Class Analysis and Growth Mixture Modeling: A Monte Carlo Simulation Study. Struct. Equ. Modeling Multidiscip. J. 2007, 14, 535–569. [Google Scholar] [CrossRef]
- Patel, S.R.; Sotres-Alvarez, D.; Castaneda, S.; Dudley, K.A.; Gallo, L.C.; Hernandez, R.; Medeiros, E.A.; Penedo, F.J.; Mossavar-Rahmani, Y.; Ramos, A.R.; et al. Social and Health Correlates of Sleep Duration in a US Hispanic Population: Results from the Hispanic Community Health Study/Study of Latinos. Sleep 2015, 38, 1515–1522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murillo, R.; Ayalew, L.; Hernandez, D.C. The association between neighborhood social cohesion and sleep duration in Latinos. Ethn. Health 2021, 26, 1000–1011. [Google Scholar] [CrossRef]
- Alegría, M.; Mulvaney-Day, N.; Torres, M.; Polo, A.; Cao, Z.; Canino, G. Prevalence of Psychiatric Disorders Across Latino Subgroups in the United States. Am. J. Public Health 2007, 97, 68–75. [Google Scholar] [CrossRef]
- Scaramutti, C.; Salas-Wright, C.P.; Vos, S.R.; Schwartz, S.J. The Mental Health Impact of Hurricane Maria on Puerto Ricans in Puerto Rico and Florida. Disaster Med. Public Health Prep. 2019, 13, 24–27. [Google Scholar] [CrossRef] [Green Version]
- Orengo-Aguayo, R.; Stewart, R.W.; De Arellano, M.A.; Suárez-Kindy, J.L.; Young, J. Disaster Exposure and Mental Health Among Puerto Rican Youths After Hurricane Maria. JAMA Netw. Open 2019, 2, e192619. [Google Scholar] [CrossRef] [Green Version]
- United States Census Bureau. QuickFacts: Puerto Rico. 2019. Available online: https://www.census.gov/quickfacts/PR (accessed on 18 October 2021).
- Pasch, R.J. Hurricane Maria. In Tropical Cyclone Report; National Hurricane Center: Miami, FL, USA, 2019. [Google Scholar]
- Ma, C.; Smith, T. Vulnerability of Renters and Low-Income Households to Storm Damage: Evidence from Hurricane Maria in Puerto Rico. Am. J. Public Health 2020, 110, 196–202. [Google Scholar] [CrossRef]
- Ho, G.Y.F.; Qian, H.; Kim, M.Y.; Melnik, T.A.; Tucker, K.; Jimenez-Velazquez, I.Z.; Kaplan, R.C.; Lee-Rey, E.T.; Stein, D.T.; Rivera, W.; et al. Health disparities between island and mainland Puerto Ricans. Rev. Panam. Salud Pública 2006, 19, 331–339. [Google Scholar] [CrossRef] [Green Version]
- Ho, G.Y.F.; Figueroa-Vallés, N.R.; De La Torre-Feliciano, T.; Tucker, K.L.; Tortolero-Luna, G.; Rivera, W.T.; Jiménez-Velázquez, I.Z.; Ortiz-Martínez, A.P.; Rohan, T.E. Cancer disparities between mainland and island Puerto Ricans. Rev. Panam. Salud Publica 2009, 25, 394–400. [Google Scholar] [CrossRef] [Green Version]
- Pérez, C.; Ailshire, J.A. Aging in Puerto Rico: A Comparison of Health Status Among Island Puerto Rican and Mainland U.S. Older Adults. J. Aging Health 2017, 29, 1056–1078. [Google Scholar] [CrossRef] [PubMed]
- Duarte, C.S.; Bird, H.R.; Shrout, P.E.; Wu, P.; Lewis-Fernandéz, R.; Shen, S.; Canino, G. Culture and psychiatric symptoms in Puerto Rican children: Longitudinal results from one ethnic group in two contexts. J. Child Psychol. Psychiatry 2008, 49, 563–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohayon, M.M.; Carskadon, M.A.; Guilleminault, C.; Vitiello, M.V. Meta-Analysis of Quantitative Sleep Parameters from Childhood to Old Age in Healthy Individuals: Developing Normative Sleep Values Across the Human Lifespan. Sleep 2004, 27, 1255–1273. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| N | % | |
|---|---|---|
| Gender | ||
| Male | 1813 | 40.8 |
| Female | 2630 | 59.2 |
| Age Category | ||
| Under 55 | 3079 | 69.3 |
| 55 & older | 1364 | 30.7 |
| Sexuality | ||
| Heterosexual | 2636 | 95.9 |
| Bisexual/Homosexual | 114 | 4.2 |
| Marital Status | ||
| Married | 1467 | 33.1 |
| Other (Separated, Divorced, Widowed) | 2965 | 66.9 |
| Education | ||
| High school or less | 2376 | 53.8 |
| 1+ years of college | 2041 | 46.2 |
| Poverty level | ||
| Below poverty | 1362 | 30.7 |
| Above poverty | 3081 | 69.4 |
| Food Insecurity | ||
| High | 2597 | 66.2 |
| Marginal/Low/Very low | 1327 | 33.8 |
| Weight Category | ||
| Underweight/Normal weight | 1294 | 29.8 |
| Overweight/Obese | 3055 | 70.3 |
| Alcohol Drinking Status | ||
| Former/Never drinker | 1957 | 44.4 |
| Current drinker | 2449 | 55.6 |
| Smoke Status | ||
| Never | 2759 | 62.2 |
| Former/Current | 1676 | 37.8 |
| Language of Interview | ||
| Spanish/English & Spanish/Other | 813 | 18.3 |
| English | 3630 | 81.7 |
| Place of Birth | ||
| Continental US | 2049 | 46.2 |
| US territory | 2390 | 53.8 |
| Mean (SE) | |||
|---|---|---|---|
| Sleep duration in hours | 6.87 (1.60) | ||
| N | % | ||
| Trouble falling asleep | |||
| None | 1875 | 60.7 | |
| Some | 659 | 21.3 | |
| High degree | 554 | 18.0 | |
| Trouble staying asleep | |||
| None | 1922 | 62.3 | |
| Some | 545 | 17.7 | |
| High degree | 620 | 20.1 | |
| Worried | |||
| Never | 1010 | 44.6 | |
| A few times a year | 540 | 23.8 | |
| Weekly to monthly | 714 | 31.5 | |
| Feeling tired in last three months | |||
| Never | 764 | 33.8 | |
| Some days | 1089 | 48.1 | |
| Most days | 264 | 11.7 | |
| Every day | 144 | 6.4 | |
| Feeling sad | |||
| None of the time | 2978 | 66.9 | |
| A little to some of the time | 1204 | 27.0 | |
| Most to all of the time | 270 | 6.1 | |
| Feeling restless | |||
| None of the time | 2821 | 63.3 | |
| A little to some of the time | 1236 | 27.7 | |
| Most to all of the time | 400 | 9.0 | |
| Feeling nervous | |||
| None of the time | 2833 | 63.6 | |
| A little to some of the time | 1292 | 29.0 | |
| Most to all of the time | 329 | 7.4 | |
| Feeling hopeless | |||
| None of the time | 3641 | 81.7 | |
| A little to some of the time | 624 | 14.0 | |
| Most to all of the time | 191 | 4.3 | |
| Feelings interfere with life in past month | |||
| A lot | 263 | 16.0 | |
| Some | 406 | 24.7 | |
| A little | 429 | 26.1 | |
| None of the time | 547 | 33.3 | |
| Everything felt like an effort | |||
| None of the time | 3067 | 68.8 | |
| A little to some of the time | 966 | 21.7 | |
| Most to all of the time | 422 | 9.5 |
| Class 1 | Class 2 | Class 3 | Class 4 | Class 5 | Class 6 | |
|---|---|---|---|---|---|---|
| Troubled Shortest Sleep | Highly Troubled Short Sleep | Some Disturbed and Shortened sleep | Undisturbed and Shortened Sleep | Normal/Average Sleep | Long Sleep | |
| N = 244 | N = 343 | N = 430 | N = 1238 | N = 2175 | N = 53 | |
| 5% of Sample | 8% of Sample | 10% of Sample | 28% of Sample | 49% of Sample | 1% of Sample | |
| Hours slept at night (Mean) | 5.47 | 5.55 | 6.71 | 6.88 | 7.23 | 12.24 |
| Trouble falling asleep | ||||||
| None | 0.10 | 0.14 | 0.36 | 0.54 | 0.87 | 0.46 |
| Some | 0.09 | 0.06 | 0.40 | 0.43 | 0.09 | 0.21 |
| High degree | 0.82 | 0.80 | 0.24 | 0.04 | 0.04 | 0.33 |
| Trouble staying asleep | ||||||
| None | 0.12 | 0.03 | 0.48 | 0.62 | 0.85 | 0.64 |
| Some | 0.10 | 0.05 | 0.30 | 0.33 | 0.10 | 0.16 |
| High degree | 0.78 | 0.92 | 0.22 | 0.06 | 0.06 | 0.21 |
| Worried | ||||||
| Never | 0.01 | 0.19 | 0.07 | 0.21 | 0.79 | 0.14 |
| A few times a year | 0.96 | 0.39 | 0.64 | 0.19 | 0.04 | 0.78 |
| Weekly to monthly | 0.03 | 0.42 | 0.29 | 0.60 | 0.17 | 0.08 |
| Feeling tired in last three months | ||||||
| Never | 0.06 | 0.09 | 0.10 | 0.15 | 0.60 | 0.05 |
| Some days | 0.23 | 0.59 | 0.57 | 0.69 | 0.36 | 0.25 |
| Most days | 0.33 | 0.20 | 0.29 | 0.11 | 0.03 | 0.38 |
| Every day | 0.38 | 0.13 | 0.04 | 0.06 | 0.01 | 0.32 |
| Feeling sad | ||||||
| None of the time | 0.01 | 0.53 | 0.03 | 0.63 | 0.95 | 0.27 |
| A little to some of the time | 0.27 | 0.43 | 0.89 | 0.36 | 0.05 | 0.37 |
| Most to all of the time | 0.72 | 0.05 | 0.07 | 0.02 | 0.00 | 0.37 |
| Feeling restless | ||||||
| None of the time | 0.04 | 0.34 | 0.09 | 0.46 | 0.99 | 0.35 |
| A little to some of the time | 0.18 | 0.47 | 0.82 | 0.50 | 0.01 | 0.24 |
| Most to all of the time | 0.79 | 0.19 | 0.10 | 0.05 | 0.00 | 0.41 |
| Feeling nervous | ||||||
| None of the time | 0.06 | 0.46 | 0.09 | 0.47 | 0.97 | 0.28 |
| A little to some of the time | 0.20 | 0.42 | 0.80 | 0.51 | 0.04 | 0.37 |
| Most to all of the time | 0.74 | 0.12 | 0.11 | 0.02 | 0.00 | 0.35 |
| Feeling hopeless | ||||||
| None of the time | 0.06 | 0.83 | 0.20 | 0.91 | 1.00 | 0.29 |
| A little to some of the time | 0.37 | 0.15 | 0.77 | 0.09 | 0.01 | 0.28 |
| Most to all of the time | 0.58 | 0.02 | 0.03 | 0.00 | 0.00 | 0.43 |
| Feelings interfere with life in past month | ||||||
| A lot | 0.61 | 0.10 | 0.16 | 0.00 | 0.04 | 0.49 |
| Some | 0.27 | 0.29 | 0.41 | 0.15 | 0.08 | 0.20 |
| A little | 0.07 | 0.32 | 0.33 | 0.30 | 0.16 | 0.07 |
| None of the time | 0.06 | 0.29 | 0.11 | 0.55 | 0.73 | 0.25 |
| Everything felt like an effort | ||||||
| None of the time | 0.06 | 0.54 | 0.06 | 0.62 | 0.98 | 0.28 |
| A little to some of the time | 0.24 | 0.38 | 0.81 | 0.29 | 0.02 | 0.16 |
| Most to all of the time | 0.70 | 0.08 | 0.14 | 0.09 | 0.01 | 0.55 |
| Troubled Shortest Sleep | Highly Troubled Short Sleep | Some Disturbed and Shortened Sleep | Undisturbed and Shortened Sleep | Long Sleep | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 95% CI | 95% CI | 95% CI | 95% CI | 95% CI | |||||||||||
| AOR | Lower | Upper | AOR | Lower | Upper | AOR | Lower | Upper | AOR | Lower | Upper | AOR | Lower | Upper | |
| Female | 1.48 | 0.86 | 2.57 | 2.79 | 1.70 | 4.59 | 2.32 | 1.46 | 3.70 | 1.37 | 0.95 | 1.99 | 1.00 | 0.38 | 2.61 |
| 55 or older | 1.19 | 0.73 | 1.95 | 1.16 | 0.68 | 1.99 | 1.19 | 0.73 | 1.94 | 0.81 | 0.54 | 1.21 | 3.58 | 1.10 | 11.64 |
| Bisexual/Homosexual | 1.73 | 0.49 | 6.20 | 2.22 | 0.77 | 6.38 | 0.83 | 0.18 | 3.86 | 1.36 | 0.51 | 3.59 | 1.83 | 0.35 | 9.44 |
| Married | 2.37 | 1.18 | 4.77 | 1.03 | 0.66 | 1.61 | 1.27 | 0.81 | 2.00 | 1.14 | 0.80 | 1.63 | 3.90 | 1.15 | 13.25 |
| 1+ years of college | 0.56 | 0.29 | 1.06 | 0.89 | 0.58 | 1.37 | 1.00 | 0.67 | 1.50 | 1.12 | 0.80 | 1.57 | 1.31 | 0.38 | 4.48 |
| Above poverty line | 0.76 | 0.42 | 1.38 | 0.50 | 0.30 | 0.84 | 0.45 | 0.28 | 0.70 | 1.03 | 0.68 | 1.58 | 0.78 | 0.32 | 1.91 |
| Food insecurity | 6.22 | 3.28 | 11.80 | 2.90 | 1.85 | 4.56 | 3.74 | 2.29 | 6.08 | 2.03 | 1.33 | 3.08 | 4.47 | 1.29 | 15.50 |
| Current/Former smoker | 2.64 | 1.35 | 5.19 | 1.94 | 1.26 | 2.99 | 2.39 | 1.53 | 3.71 | 1.18 | 0.81 | 1.73 | 2.10 | 0.75 | 5.87 |
| Current alcohol drinker | 0.94 | 0.51 | 1.72 | 1.26 | 0.73 | 2.18 | 1.20 | 0.73 | 1.99 | 1.65 | 1.14 | 2.37 | 1.59 | 0.58 | 4.39 |
| Overweight/Obese | 1.46 | 0.78 | 2.75 | 1.94 | 1.15 | 3.27 | 0.74 | 0.48 | 1.14 | 0.76 | 0.53 | 1.09 | 0.77 | 0.24 | 2.43 |
| Language of Interview: English | 1.24 | 0.74 | 2.07 | 1.96 | 0.91 | 4.22 | 1.04 | 0.61 | 1.80 | 2.28 | 1.31 | 3.97 | 1.56 | 0.56 | 4.33 |
| Born in US territory | 1.21 | 0.76 | 2.03 | 1.24 | 0.80 | 1.93 | 1.77 | 1.17 | 2.70 | 1.38 | 0.99 | 1.93 | 0.89 | 0.36 | 2.22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villalobos, K.; Montiel Ishino, F.A.; Williams, F. Profiles of Sleep Duration and Psychological Distress among Puerto Ricans Living in the United States: A Cross-Sectional Survey and Latent Class Analysis. Int. J. Environ. Res. Public Health 2022, 19, 6363. https://doi.org/10.3390/ijerph19116363
Villalobos K, Montiel Ishino FA, Williams F. Profiles of Sleep Duration and Psychological Distress among Puerto Ricans Living in the United States: A Cross-Sectional Survey and Latent Class Analysis. International Journal of Environmental Research and Public Health. 2022; 19(11):6363. https://doi.org/10.3390/ijerph19116363
Chicago/Turabian StyleVillalobos, Kevin, Francisco A. Montiel Ishino, and Faustine Williams. 2022. "Profiles of Sleep Duration and Psychological Distress among Puerto Ricans Living in the United States: A Cross-Sectional Survey and Latent Class Analysis" International Journal of Environmental Research and Public Health 19, no. 11: 6363. https://doi.org/10.3390/ijerph19116363