
Body-Size Perception among First-Generation Chinese Migrants in Italy


 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Setting and Study Population
2.2. Data Collection
2.3. Diagnostic Criteria
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Participants
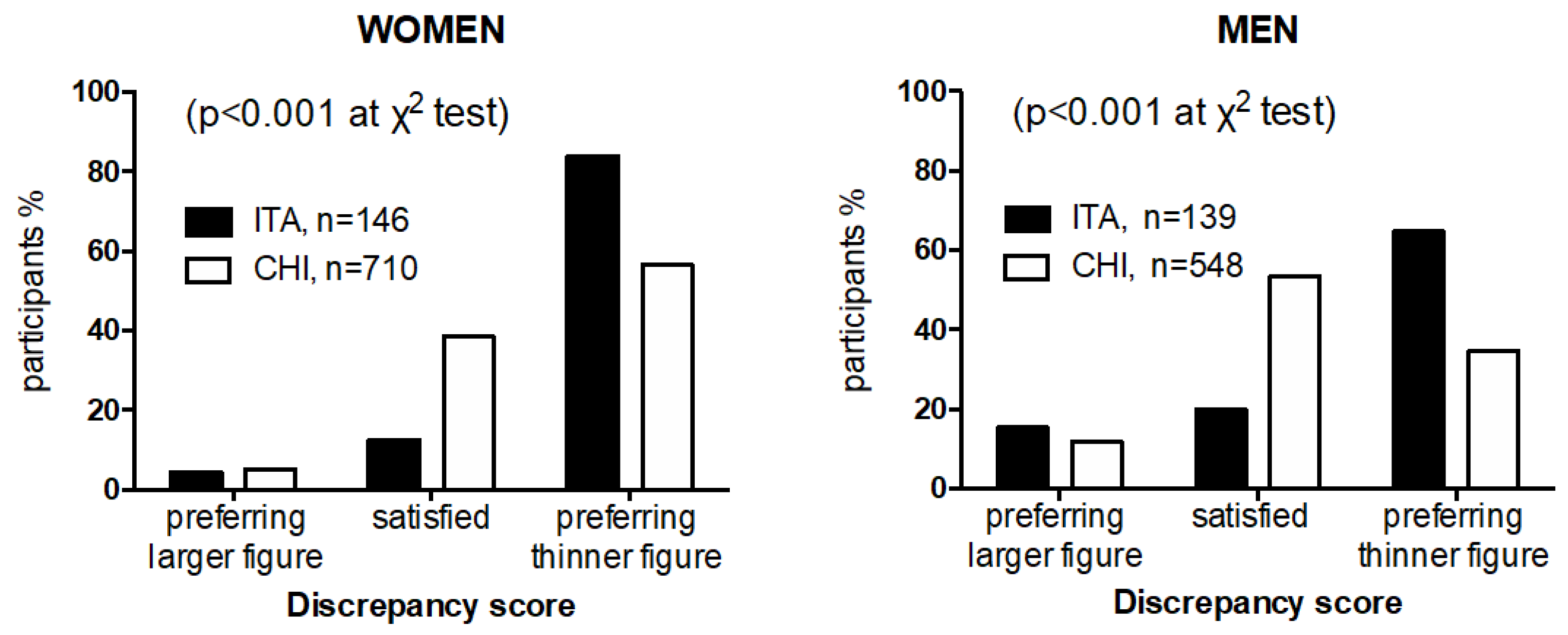
3.2. Body Image Perception
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- (NCD-RisC) NRFC. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 1289 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- WHO. Global Report on Urban Health: Equitable Healthier Cities for Sustainable Development. Report No. 9241565276. 2016. Available online: https://apps.who.int/iris/handle/10665/204715 (accessed on 31 March 2016).
- Yusuf, S.; Reddy, S.; Ounpuu, S.; Anand, S. Global burden of cardiovascular diseases: Part I: General considerations, the epidemiologic transition, risk factors, and impact of urbanization. Circulation 2001, 104, 2746–2753. [Google Scholar] [CrossRef] [PubMed]
- Wagner, K.H.; Brath, H. A global view on the development of non communicable diseases. Prev. Med. 2012, 54, S38–S41. [Google Scholar] [CrossRef] [PubMed]
- Collaboration (NCD-RisC) NRF. Rising rural body-mass index is the main driver of the global obesity epidemic in adults. Nature 2019, 569, 260–264. [Google Scholar] [CrossRef]
- (NCD-RisC) NRFC. Heterogeneous contributions of change in population distribution of body mass index to change in obesity and underweight. Elife 2021, 10, e60060. [Google Scholar] [CrossRef]
- Modesti, P.A.; Bamoshmoosh, M.; Rapi, S.; Massetti, L.; Al-Hidabi, D.; Al Goshae, H. Epidemiology of hypertension in Yemen: Effects of urbanization and geographical area. Hypertens. Res. 2013, 36, 711–717. [Google Scholar] [CrossRef]
- Modesti, P.A.; Bamoshmoosh, M.; Rapi, S.; Massetti, L.; Bianchi, S.; Al-Hidabi, D.; Al Goshae, H. Relationship between hypertension, diabetes and proteinuria in rural and urban households in Yemen. J. Hum. Hypertens. 2013, 27, 572–579. [Google Scholar] [CrossRef][Green Version]
- Burgess, E.; Hassmén, P.; Pumpa, K.L. Determinants of adherence to lifestyle intervention in adults with obesity: A systematic review. Clin. Obes. 2017, 7, 123–135. [Google Scholar] [CrossRef]
- Jarry, J.L.; Kossert, A.L. Self-esteem threat combined with exposure to thin media images leads to body image compensatory self-enhancement. Body Image 2007, 4, 39–50. [Google Scholar] [CrossRef]
- Striegel-Moore, R.; Smolak, L. Eating Disorders: Innovative Directions for Research and Practice, 1st ed.; American Psychological Association: Washington, DC, USA, 2001. [Google Scholar]
- Alm, M.; Soroudi, N.; Wylie-Rosett, J.; Isasi, C.R.; Suchday, S.; Rieder, J.; Khan, U. A qualitative assessment of barriers and facilitators to achieving behavior goals among obese inner-city adolescents in a weight management program. Diabetes Educ. 2008, 34, 277–284. [Google Scholar] [CrossRef]
- Maruf, F.A.; Akinpelu, A.O.; Udoji, N.V. Differential perceptions of body image and body weight among adults of different socioeconomic status in a sub-urban population. J. Biosoc. Sci. 2014, 46, 279–293. [Google Scholar] [CrossRef]
- Wardle, J.; Haase, A.M.; Steptoe, A. Body image and weight control in young adults: International comparisons in university students from 22 countries. Int. J. Obes. 2006, 30, 644–651. [Google Scholar] [CrossRef] [PubMed]
- Fitzgibbon, M.L.; Blackman, L.R.; Avellone, M.E. The relationship between body image discrepancy and body mass index across ethnic groups. Obes. Res. 2000, 8, 582–589. [Google Scholar] [CrossRef] [PubMed]
- Gualdi-Russo, E.; Manzon, V.S.; Masotti, S.; Toselli, S.; Albertini, A.; Celenza, F.; Zaccagni, L. Weight status and perception of body image in children: The effect of maternal immigrant status. Nutr. J. 2012, 11, 85. [Google Scholar] [CrossRef] [PubMed]
- Ohara, K.; Kato, Y.; Mase, T.; Kouda, K.; Miyawaki, C.; Fujita, Y.; Okita, Y.; Nakamura, H. Eating behavior and perception of body shape in Japanese university students. Eat. Weight Disord. 2014, 19, 461–468. [Google Scholar] [CrossRef]
- Ohara, K.; Mase, T.; Kouda, K.; Miyawaki, C.; Momoi, K.; Fujitani, T.; Fujita, Y.; Nakamura, H. Association of anthropometric status, perceived stress, and personality traits with eating behavior in university students. Eat. Weight Disord. 2019, 24, 521–531. [Google Scholar] [CrossRef]
- Noh, J.W.; Kim, J.; Yang, Y.; Park, J.; Cheon, J.; Kwon, Y.D. Body mass index and self-rated health in East Asian countries: Comparison among South Korea, China, Japan, and Taiwan. PLoS ONE 2017, 12, e0183881. [Google Scholar] [CrossRef]
- WHO. Appropriate body-mass index in Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar] [CrossRef]
- Xu, Y.; Wang, L.; He, J.; Bi, Y.; Li, M.; Wang, T.; Wang, L.; Jiang, Y.; Dai, M.; Lu, J.; et al. Prevalence and control of diabetes in Chinese adults. JAMA 2013, 310, 948–959. [Google Scholar] [CrossRef]
- Modesti, P.A.; Han, Y.; Jing, Y.; Xiaoling, W.; Mengyue, Z.; Zihua, Y.; Jia, G.; Perruolo, E.; Bini, L.; Camera, M.; et al. Design and arrangement of the CHIP (CHinese In Prato) study. Epidemiol. Prev. 2014, 38, 357–363. [Google Scholar]
- Modesti, P.A.; Calabrese, M.; Malandrino, D.; Colella, A.; Galanti, G.; Zhao, D. New findings on type 2 diabetes in first-generation Chinese migrants settled in Italy: Chinese in Prato (CHIP) cross-sectional survey. Diabetes Metab. Res. Rev. 2017, 33, e2835. [Google Scholar] [CrossRef] [PubMed]
- Modesti, P.A.; Calabrese, M.; Marzotti, I.; Bing, H.; Malandrino, D.; Boddi, M.; Castellani, S.; Zhao, D. Prevalence, Awareness, Treatment, and Control of Hypertension among Chinese First-Generation Migrants and Italians in Prato, Italy: The CHIP Study. Int. J. Hypertens. 2017, 2017, 6402085. [Google Scholar] [CrossRef] [PubMed]
- Modesti, P.A.; Castellani, S.; Calabrese, M.; Malandrino, D.; Zhao, D. Comparison of type 2 diabetes prevalence in Chinese migrants vs. Caucasians and new perspectives for screening of cerebrovascular disease in Chinese: A proof of concept study. Diabetes Res. Clin. Pract. 2017, 130, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Modesti, P.A.; Calabrese, M.; Perruolo, E.; Bussotti, A.; Malandrino, D.; Bamoshmoosh, M.; Biggeri, A.; Zhao, D. Sleep History and Hypertension Burden in First-Generation Chinese Migrants Settled in Italy: The CHIinese In Prato Cross-Sectional Survey. Medicine 2016, 95, e3229. [Google Scholar] [CrossRef]
- Pulvers, K.M.; Lee, R.E.; Kaur, H.; Mayo, M.S.; Fitzgibbon, M.L.; Jeffries, S.K.; Butler, J.; Hou, Q.; Ahluwalia, J.S. Development of a culturally relevant body image instrument among urban African Americans. Obes. Res. 2004, 12, 1641–1651. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.F.; Cooperative Meta-Analysis Group of the Working Group on Obesity in China. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults--study on optimal cut-off points of body mass index and waist circumference in Chinese adults. Biomed. Environ. Sci. 2002, 15, 83–96. [Google Scholar] [PubMed]
- Greenberg, B.S.; Eastin, M.; Hofschire, L.; Lachlan, K.; Brownell, K.D. Portrayals of overweight and obese individuals on commercial television. Am. J. Public Health 2003, 93, 1342–1348. [Google Scholar] [CrossRef]
- Anschutz, D.J.; Engels, R.C.; Becker, E.S.; van Strien, T. The bold and the beautiful. Influence of body size of televised media models on body dissatisfaction and actual food intake. Appetite 2008, 51, 530–537. [Google Scholar] [CrossRef]
- Yates, A.; Edman, J.; Aruguete, M. Ethnic differences in BMI and body/self-dissatisfaction among Whites, Asian subgroups, Pacific Islanders, and African-Americans. J. Adolesc. Health 2004, 34, 300–307. [Google Scholar] [CrossRef]
- Becker, A.E. Television, disordered eating, and young women in Fiji: Negotiating body image and identity during rapid social change. Cult. Med. Psychiatry 2004, 28, 533–559. [Google Scholar] [CrossRef] [PubMed]
- Waller, G.; Barnes, J. Preconscious processing of body image cues. Impact on body percept and concept. J. Psychosom. Res. 2002, 53, 1037–1041. [Google Scholar] [CrossRef]
- Meyer, C.; McPartlan, L.; Sines, J.; Waller, G. Accuracy of self-reported weight and height: Relationship with eating psychopathology among young women. Int. J. Eat. Disord. 2009, 42, 379–381. [Google Scholar] [CrossRef] [PubMed]
- Orlandi, M.; Rosselli, M.; Pellegrino, A.; Boddi, M.; Stefani, L.; Toncelli, L.; Modesti, P.A. Gender differences in the impact on physical activity and lifestyle in Italy during the lockdown, due to the pandemic. Nutr. Metabol. Cardiovasc. Dis. 2021, 30, 2173–2180. [Google Scholar] [CrossRef]
- Modesti, P.A.; Marzotti, I.; Calabrese, M.; Stefani, L.; Toncelli, L.; Modesti, A.; Galanti, G.; Boddi, M. Gender differences in acculturation and cardiovascular disease risk-factor changes among Chinese immigrants in Italy: Evidence from a large population-based cohort. Int. J. Cardiol. Cardiovasc. Risk Prev. 2021, 11, 200112. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Italians | Chinese | p | |
|---|---|---|---|
| Categorical Variables, n (%) | |||
| Age decades | <0.001 | ||
| 30–39 years | 63 (22.1) | 399 (31.7) | |
| 40–49 years | 108 (37.9) | 496 (39.4) | |
| 50–59 years | 114 (40.0) | 363 (28.9) | |
| Women | 146 (51.2) | 710 (56.4) | 0.010 |
| Health insurance | – | ||
| RHS | 285 (100.0) | 294 (23.4) | |
| TPF | – | 226 (18.0) | |
| No | – | 734 (58.3) | |
| Education | <0.001 | ||
| Illiterate | – | 189 (15.0) | |
| Primary school | 36 (12.6) | 556 (44.2) | |
| Middle school | 186 (65.3) | 487 (38.7) | |
| College or more | 63 (22.1) | 25 (2.0) | |
| BMI ethnically specific categories | <0.001 | ||
| Normal | 126 (44.2) | 705 (56.0) | |
| Overweight | 138 (48.4) | 430 (34.2) | |
| Obese | 21 (7.4) | 123 (9.8) | |
| Smokers | 48 (16.8) | 235 (18.7) | 0.632 |
| Alcohol use | 189 (66.3) | 569 (45.2) | <0.001 |
| Hypertension | 58 (20.4) | 266 (21.1) | 0.832 |
| Diabetes | 21 (7.4) | 157 (12.5) | 0.015 |
| Continuous variables, mean ± SD | |||
| Age (years) | 47.5 ± 7.4 | 44.3 ± 8.1 | <0.001 |
| Height (cm) | 171.2 ± 10.8 | 163.2 ± 7.8 | <0.001 |
| Weight (kg) | 74.6 ± 12.1 | 63.5 ± 10.7 | <0.001 |
| BMI (kg/m2) | 25.4 ± 3.2 | 23.8 ± 3.1 | <0.001 |
| Waist (cm) | 89.2 ± 9.8 | 82.5 ± 9.6 | <0.001 |
| Hip (cm) | 99.3 ± 6.8 | 95.5 ± 6.4 | <0.001 |
| Waist/Hip ratio | 0.898 ± 0.077 | 0.863 ± 0.070 | <0.001 |
| SBP (mmHg) | 120.4 ± 13.9 | 119.6 ± 19.0 | 0.107 |
| DBP (mmHg) | 77.7 ± 10.7 | 79.9 ± 11.7 | <0.001 |
| Glucose (mg/dL) | 103.5 ± 12.9 | 116.8 ± 31.2 | <0.001 |
| Cholesterol (mg/dL) | 190.6 ± 55.6 | 235.2 ± 64.2 | <0.001 |
| Triglycerides (mg/dL) | 163.0 ± 87.2 | 196.8 ± 107.2 | <0.001 |
| Exposures | OR (95% Cl) | p |
|---|---|---|
| Age (years) | 0.921 (0.903 to 0.939) | <0.001 |
| Gender (women) | 0.974 (0.702 to 1.350) | 0.873 |
| BMI (ethnically specific categories) | 0.824 (0.588 to 1.154) | 0.260 |
| Education (categories) | 0.135 (0.102 to 0.179) | <0.001 |
| Discrepancy Score (thinner figure) | 0.546 (0.409 to 0.730) | <0.001 |
| Exposures | Model 1 | Model 2 | ||
|---|---|---|---|---|
| B (95% Cl for B) | p | B (95% Cl for B) | p | |
| Gender (women) | 0.386 (0.313 to 0.459) | <0.001 | 0.425 (0.319 to 0.531) | <0.001 |
| BMI (kg/m2) | 0.102 (0.092 to 0.112) | <0.001 | 0.101 (0.087 to 0.115) | <0.001 |
| Age (years) | −0.008 (−0.012 to −0.004) | <0.001 | −0.009 (−0.015 to −0.003) | 0.002 |
| Time in Italy (years) | - | - | 0.009 (0.000 to 0.018) | 0.042 |
| Multiple r= | 0.553 | 0.557 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castellini, G.; Pellegrino, A.; Tarchi, L.; Calabrese, M.; Boddi, M.; Ricca, V.; Costanzo, G.; Modesti, P.A. Body-Size Perception among First-Generation Chinese Migrants in Italy. Int. J. Environ. Res. Public Health 2022, 19, 6063. https://doi.org/10.3390/ijerph19106063
Castellini G, Pellegrino A, Tarchi L, Calabrese M, Boddi M, Ricca V, Costanzo G, Modesti PA. Body-Size Perception among First-Generation Chinese Migrants in Italy. International Journal of Environmental Research and Public Health. 2022; 19(10):6063. https://doi.org/10.3390/ijerph19106063
Chicago/Turabian StyleCastellini, Giovanni, Alessio Pellegrino, Livio Tarchi, Maria Calabrese, Maria Boddi, Valdo Ricca, Gianfranco Costanzo, and Pietro Amedeo Modesti. 2022. "Body-Size Perception among First-Generation Chinese Migrants in Italy" International Journal of Environmental Research and Public Health 19, no. 10: 6063. https://doi.org/10.3390/ijerph19106063
APA StyleCastellini, G., Pellegrino, A., Tarchi, L., Calabrese, M., Boddi, M., Ricca, V., Costanzo, G., & Modesti, P. A. (2022). Body-Size Perception among First-Generation Chinese Migrants in Italy. International Journal of Environmental Research and Public Health, 19(10), 6063. https://doi.org/10.3390/ijerph19106063