
Air Pollution and Respiratory Hospital Admissions in Kuwait: The Epidemiological Applicability of Predicted PM2.5 in Arid Regions


 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Admissions Data
2.2. Environmental Data
2.3. Study Design & Statistical Analysis
3. Results
3.1. Summary Statistics
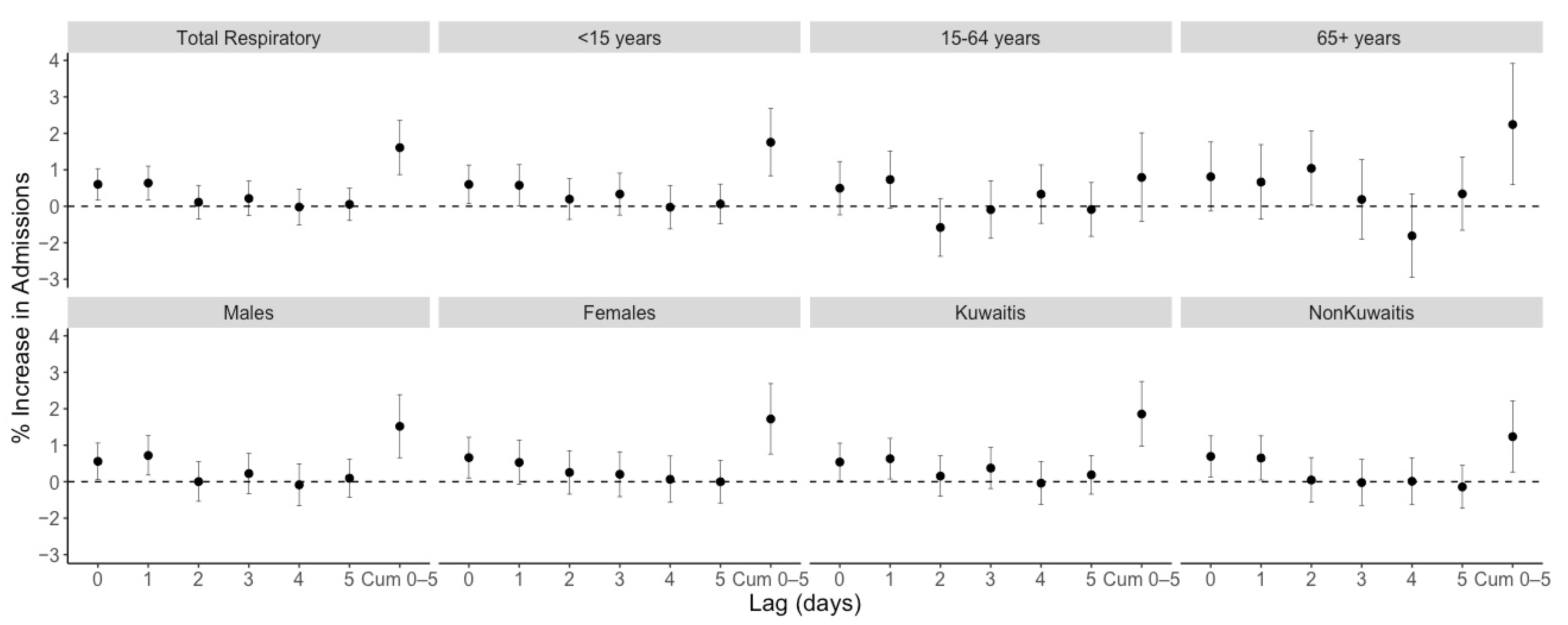
3.2. Regression Results
3.3. Admissions Averted by Reducing Exposures
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khalaf, F.; Al-Ajmi, D. Aeolian processes and sand encroachment problems in Kuwait. Geomorphology 1993, 6, 111–134. [Google Scholar] [CrossRef]
- Al-Awadhi, J.M.; Omar, S.A.; Misak, R.F. Land degradation indicators in Kuwait. Land Degrad. Dev. 2005, 16, 163–176. [Google Scholar] [CrossRef]
- Goudie, A.S. Desert dust and human health disorders. Environ. Int. 2014, 63, 101–113. [Google Scholar] [CrossRef] [PubMed]
- Alahmad, B.; Al-Hemoud, A.; Kang, C.-M.; Almarri, F.; Kommula, V.; Wolfson, J.M.; Bernstein, A.S.; Garshick, E.; Schwartz, J.; Koutrakis, P. A two-year assessment of particulate air pollution and sources in Kuwait. Environ. Pollut. 2021, 282, 117016. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. What Are the Who Air Quality Guidelines? Available online: https://www.who.int/news-room/feature-stories/detail/what-are-the-who-air-quality-guidelines#:~:text=The%20WHO%20Air%20quality%20guidelines%20are%20a%20set%20of%20evidence,the%20guidelines%20was%20in%201987 (accessed on 30 April 2022).
- Brunekreef, B.; Beelen, R.; Hoek, G.; Schouten, L.; Bausch-Goldbohm, S.; Fischer, P.; Armstrong, B.; Hughes, E.; Jerrett, M.; van den Brandt, P. Effects of long-term exposure to traffic-related air pollution on respiratory and cardiovascular mortality in the Netherlands: The NLCS-AIR study. Res. Rep. Health Eff. Inst. 2009, 139, 5–71. [Google Scholar]
- Shi, L.; Zanobetti, A.; Kloog, I.; Coull, B.A.; Koutrakis, P.; Melly, S.J.; Schwartz, J.D. Low-concentration PM2.5 and mortality: Estimating acute and chronic effects in a population-based study. Environ. Health Perspect. 2016, 124, 46–52. [Google Scholar] [CrossRef] [Green Version]
- Ibrahimou, B.; Salihu, H.; Gasana, J.; Owusu, H. Risk of low birth weight and very low birth weight from exposure to particulate matter (PM2.5) speciation metals during pregnancy. Gynecol. Obs. 2014, 4, 2161-0932. [Google Scholar]
- Wu, H.; Jiang, B.; Geng, X.; Zhu, P.; Liu, Z.; Cui, L.; Yang, L. Exposure to fine particulate matter during pregnancy and risk of term low birth weight in Jinan, China, 2014–2016. Int. J. Hyg. Environ. Health 2018, 221, 183–190. [Google Scholar] [CrossRef]
- Atkinson, R.W.; Kang, S.; Anderson, H.R.; Mills, I.C.; Walton, H.A. Epidemiological time series studies of PM2.5 and daily mortality and hospital admissions: A systematic review and meta-analysis. Thorax 2014, 69, 660–665. Available online: http://www.ncbi.nlm.nih.gov/pubmed/24706041 (accessed on 2 January 2019). [CrossRef] [Green Version]
- Bell, M.L.; Ebisu, K.; Leaderer, B.P.; Gent, J.F.; Lee, H.J.; Koutrakis, P.; Wang, Y.; Dominici, F.; Peng, R.D. Associations of PM2.5 Constituents and Sources with Hospital Admissions: Analysis of Four Counties in Connecticut and Massachusetts (USA) for Persons ≥ 65 Years of Age. Environ. Health Perspect. 2014, 122, 138–144. [Google Scholar] [CrossRef] [Green Version]
- Linares, C.; Diaz, J. Short-term effect of PM2.5 on daily hospital admissions in Madrid (2003–2005). Int. J. Environ. Health Res. 2010, 20, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Ostro, B.; Roth, L.; Malig, B.; Marty, M. The Effects of Fine Particle Components on Respiratory Hospital Admissions in Children. Environ. Health Perspect. 2009, 117, 475–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tecer, L.H.; Alagha, O.; Karaca, F.; Tuncel, G.; Eldes, N. Particulate Matter (PM2.5, PM10–2.5, and PM10) and Children’s Hospital Admissions for Asthma and Respiratory Diseases: A Bidirectional Case-Crossover Study. J. Toxicol. Environ. Health Part A 2008, 71, 512–520. [Google Scholar] [CrossRef] [PubMed]
- E Gordian, M.; Ozkaynak, H.; Xue, J.; Morris, S.S.; Spengler, J.D. Particulate air pollution and respiratory disease in Anchorage, Alaska. Environ. Health Perspect. 1996, 104, 290–297. [Google Scholar] [CrossRef]
- Sheppard, L.; Levy, D.; Norris, G.; Larson, T.V.; Koenig, J.Q. Effects of ambient air pollution on nonelderly asthma hospital admissions in Seattle, Washington, 1987–1994. Epidemiology 1999, 10, 23–30. Available online: http://www.jstor.org/stable/3702178 (accessed on 20 June 2021). [CrossRef]
- Thalib, L.; Al-Taiar, A. Dust storms and the risk of asthma admissions to hospitals in Kuwait. Sci. Total Environ. 2012, 433, 347–351. [Google Scholar] [CrossRef]
- Guarnieri, M.; Balmes, J.R. Outdoor air pollution and asthma. Lancet 2014, 383, 1581–1592. [Google Scholar] [CrossRef] [Green Version]
- Al-Hemoud, A.; Gasana, J.; Al-Dabbous, A.; Alajeel, A.; Al-Shatti, A.; Behbehani, W.; Malak, M. Exposure levels of air pollution (PM2.5) and associated health risk in Kuwait. Environ. Res. 2019, 179, 108730. [Google Scholar] [CrossRef]
- Li, J.; Garshick, E.; Hart, J.E.; Li, L.; Shi, L.; Al-Hemoud, A.; Huang, S.; Koutrakis, P. Estimation of ambient PM2.5 in Iraq and Kuwait from 2001 to 2018 using machine learning and remote sensing. Environ. Int. 2021, 151, 106445. [Google Scholar] [CrossRef]
- Alahmad, B.; Shakarchi, A.; Alseaidan, M.; Fox, M. The effects of temperature on short-term mortality risk in Kuwait: A time-series analysis. Environ. Res. 2019, 171, 278–284. [Google Scholar] [CrossRef]
- Alahmad, B.; Shakarchi, A.F.; Khraishah, H.; Alseaidan, M.; Gasana, J.; Al-Hemoud, A.; Koutrakis, P.; Fox, M.A. Extreme temperatures and mortality in Kuwait: Who is vulnerable? Sci. Total Environ. 2020, 732, 139289. [Google Scholar] [CrossRef] [PubMed]
- Dominici, F.; Peng, R.D.; Bell, M.L.; Pham, L.; McDermott, A.; Zeger, S.L.; Samet, J.M. Fine Particulate Air Pollution and Hospital Admission for Cardiovascular and Respiratory Diseases. JAMA 2006, 295, 1127–1134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krishna, B.; Mandal, S.; Madhipatla, K.; Reddy, K.S.; Prabhakaran, D.; Schwartz, J.D. Daily nonaccidental mortality associated with short-term PM2.5 exposures in Delhi, India. Environ. Epidemiol. 2021, 5, e167. [Google Scholar] [CrossRef] [PubMed]
- Ren, Z.; Liu, X.; Liu, T.; Chen, D.; Jiao, K.; Wang, X.; Suo, J.; Yang, H.; Liao, J.; Ma, L. Effect of ambient fine particulates (PM2.5) on hospital admissions for respiratory and cardiovascular diseases in Wuhan, China. Respir. Res. 2021, 22, 128. [Google Scholar] [CrossRef]
- Peled, R. Air pollution exposure: Who is at high risk? Atmos. Environ. 2011, 45, 1781–1785. [Google Scholar] [CrossRef]
- Simon, A.K.; Hollander, G.A.; McMichael, A. Evolution of the immune system in humans from infancy to old age. Proc. R. Soc. B Biol. Sci. 2015, 282, 20143085. [Google Scholar] [CrossRef]
- Tao, Y.; Mi, S.; Zhou, S.; Wang, S.; Xie, X. Air pollution and hospital admissions for respiratory diseases in Lanzhou, China. Environ. Pollut. 2014, 185, 196–201. [Google Scholar] [CrossRef]
- Ito, K.; de Leon, S.F.; Lippmann, M. Associations between Ozone and Daily Mortality: Analysis and Meta-Analysis. Epidemiology 2005, 16, 446–457. Available online: http://www.jstor.org/stable/20486080 (accessed on 30 May 2021). [CrossRef]
- Lippmann, M.; Ito, K.; Nádas, A.; Burnett, R.T. Association of particulate matter components with daily mortality and morbidity in urban populations. Res. Rep. (Health Eff. Inst.) 2000, 95, 5–72. [Google Scholar]
- Gasana, J.; Dillikar, D.; Mendy, A.; Forno, E.; Vieira, E.R. Motor vehicle air pollution and asthma in children: A meta-analysis. Environ. Res. 2012, 117, 36–45. [Google Scholar] [CrossRef]
- Bell, M.L.; Son, J.-Y.; Peng, R.D.; Wang, Y.; Dominici, F. Brief Report, Ambient PM2.5 and Risk of Hospital Admissions Do Risks Differ for Men and Women? Epidemiology 2015, 26, 575–579. [Google Scholar] [CrossRef] [PubMed]
- Shakerkhatibi, M.; Seifipour, H.; Sabeti, Z.; Kahe, D.; Asghari Jafarabadi, M.; Zoroufchi Benis, K.; Hajaghazadeh, M. Correlation of ambient particulate matters (PM10, PM2.5) with respiratory hospital admissions: A case-crossover study in Urmia, Iran. Hum. Ecol. Risk Assess. Int. J. 2021, 27, 2184–2201. [Google Scholar] [CrossRef]
- Denton, M.; Prus, S.; Walters, V. Gender differences in health: A Canadian study of the psychosocial, structural and behavioural determinants of health. Soc. Sci. Med. 2004, 58, 2585–2600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- PACI. The Public Authority for Civil Information; Government of Kuwait: Kuwait City, Kuwait, 2019.
- Achilleos, S.; Al-Ozairi, E.; Alahmad, B.; Garshick, E.; Neophytou, A.M.; Bouhamra, W.; Yassin, M.F.; Koutrakis, P. Acute effects of air pollution on mortality: A 17-year analysis in Kuwait. Environ. Int. 2019, 126, 476–483. [Google Scholar] [CrossRef]
- Zhang, Y.; Ding, Z.; Xiang, Q.; Wang, W.; Huang, L.; Mao, F. Short-term effects of ambient PM1 and PM2.5 air pollution on hospital admission for respiratory diseases: Case-crossover evidence from Shenzhen, China. Int. J. Hyg. Environ. Health 2019, 224, 113418. [Google Scholar] [CrossRef] [PubMed]
- Delfino, R.J.; Staimer, N.; Tjoa, T.; Gillen, D.; Kleinman, M.T.; Sioutas, C.; Cooper, D. Personal and Ambient Air Pollution Exposures and Lung Function Decrements in Children with Asthma. Environ. Health Perspect. 2008, 116, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Hanley, Q.S.; Koenig, J.Q.; Larson, T.V.; Anderson, T.L.; Van Belle, G.; Rebolledo, V.; Covert, D.S.; Pierson, W.E. Response of Young Asthmatic Patients to Inhaled Sulfuric Acid. Am. Rev. Respir. Dis. 1992, 145, 326–331. [Google Scholar] [CrossRef]
- Jung, K.H.; Torrone, D.; Lovinsky-Desir, S.; Perzanowski, M.; Bautista, J.; Jezioro, J.R.; Hoepner, L.; Ross, J.; Perera, F.P.; Chillrud, S.N.; et al. Short-term exposure to PM2.5 and vanadium and changes in asthma gene DNA methylation and lung function decrements among urban children. Respir. Res. 2017, 18, 63. [Google Scholar] [CrossRef] [Green Version]
- Koenig, J.; Larson, T.; Hanley, Q.; Rebolledo, V.; Dumler, K.; Checkoway, H.; Wang, S.; Lin, D.; Pierson, W. Pulmonary Function Changes in Children Associated with Fine Particulate Matter. Environ. Res. 1993, 63, 26–38. [Google Scholar] [CrossRef]
- Karakatsani, A.; Analitis, A.; Perifanou, D.; Ayres, J.G.; Harrison, R.M.; Kotronarou, A.; Kavouras, I.; Pekkanen, J.; Hämeri, K.; Kos, G.P.; et al. Particulate matter air pollution and respiratory symptoms in individuals having either asthma or chronic obstructive pulmonary disease: A European multicentre panel study. Environ. Health 2012, 11, 75. [Google Scholar] [CrossRef] [Green Version]
- Williams, A.M.; Phaneuf, D.J.; Barrett, M.A.; Su, J.G. Short-term impact of PM2.5 on contemporaneous asthma medication use: Behavior and the value of pollution reductions. Proc. Natl. Acad. Sci. USA 2018, 116, 5246–5253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.; Zhong, T.; Zhu, Y.; Ge, D.; Lin, X.; Li, Q. Effects of particulate matter (PM) on childhood asthma exacerbation and control in Xiamen, China. BMC Pediatr. 2019, 19, 194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baldacci, S.; Maio, S.; Cerrai, S.; Sarno, G.; Baïz, N.; Simoni, M.; Annesi-Maesano, I.; Viegi, G. Allergy and asthma: Effects of the exposure to particulate matter and biological allergens. Respir. Med. 2015, 109, 1089–1104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heinrich, J.; Hoelscher, B.; Wjst, M.; Ritz, B.; Cyrys, J.; Wichmann, H. Respiratory diseases and allergies in two polluted areas in East Germany. Environ. Health Perspect. 1999, 107, 53–62. [Google Scholar] [CrossRef]
- Gavett, S.H.; Koren, H.S. The Role of Particulate Matter in Exacerbation of Atopic Asthma. Int. Arch. Allergy Immunol. 2001, 124, 109–112. [Google Scholar] [CrossRef]
- Seaton, A.; Godden, D.; MacNee, W.; Donaldson, K. Particulate air pollution and acute health effects. Lancet 1995, 345, 176–178. [Google Scholar] [CrossRef]

{kind=link}
| Total | Mean | SD | Median | Min | IQR | Max | |
|---|---|---|---|---|---|---|---|
| Cause of Admissions (adm./day) | |||||||
| Total Respiratory | 218,403 | 66.77 | 24.84 | 66 | 3 | 35 | 151 |
| Asthma | 22,701 | 6.99 | 4.15 | 6 | 1 | 5 | 50 |
| Sex (adm./day) | |||||||
| Male | 124,622 | 38.10 | 14.37 | 38 | 1 | 20 | 85 |
| Female | 93,781 | 28.67 | 11.78 | 28 | 2 | 16 | 76 |
| Nationality (adm./day) | |||||||
| Kuwaiti | 128,533 | 39.32 | 15.89 | 38 | 1 | 23 | 91 |
| Non-Kuwaiti | 89,870 | 27.45 | 10.73 | 27 | 2 | 14 | 78 |
| Age groups (adm./day) | |||||||
| <15 | 134,191 | 41.05 | 18.25 | 40 | 2 | 25 | 100 |
| 15–64 | 59,655 | 18.22 | 7.30 | 18 | 1 | 10 | 63 |
| 65+ | 24,557 | 7.51 | 3.49 | 7 | 0 | 5 | 25 |
| Exposure | |||||||
| PM2.5 (μg/m3) | - | 46.93 | 16.89 | 44 | 11.91 | 15.09 | 403.80 |
| Average Temperature (°C) | - | 27.26 | 9.84 | 28 | 5.70 | 18.50 | 43.90 |
| Average relative humidity (%) | - | 33.80 | 20.01 | 28.50 | 6.40 | 32.00 | 93.20 |
| Lag | % Increase in Admissions | 95% CI | |
|---|---|---|---|
| Lo % | Hi % | ||
| Distributed Lags | |||
| 0 | 0.60 * | 0.17 | 1.03 |
| 1 | 0.64 * | 0.18 | 1.1 |
| 2 | 0.11 | −0.35 | 0.57 |
| 3 | 0.21 | −0.26 | 0.69 |
| 4 | −0.02 | −0.51 | 0.47 |
| 5 | 0.05 | −0.39 | 0.5 |
| Cumulative 0–5 (main model) | 1.61 * | 0.87 | 2.35 |
| Moving Average Lags | |||
| 3 | 1.32 * | 0.77 | 1.87 |
| 5 | 1.38 * | 0.7 | 2.05 |
| Subgroup | % Increase in Admissions | 95% CI | |
|---|---|---|---|
| Lo % | Hi % | ||
| Nationality | |||
| Kuwaiti | 1.85 * | 0.97 | 2.75 |
| Non-Kuwaiti | 1.24 * | 0.27 | 2.21 |
| Sex | |||
| Male | 1.52 * | 0.66 | 2.39 |
| Female | 1.72 * | 0.76 | 2.69 |
| Age | |||
| <15 years | 1.76 * | 0.84 | 2.68 |
| 15–64 years | 0.79 | −0.42 | 2.01 |
| 65+ years | 2.24 * | 0.60 | 3.92 |
| Nationality | Sex | Age | % Increase in Admissions | 95% CI | |
|---|---|---|---|---|---|
| Lo% | Hi% | ||||
| Kuwaiti | Male | ||||
| Total | 1.60 * | 0.52 | 2.70 | ||
| <15 | 1.59 * | 0.29 | 2.90 | ||
| 15–64 | 1.38 | −0.72 | 3.53 | ||
| 65+ | 1.62 | −1.28 | 4.61 | ||
| Female | |||||
| Total | 2.15 * | 0.99 | 3.32 | ||
| <15 | 2.38 * | 0.90 | 3.89 | ||
| 15–64 | 1.27 | −0.93 | 3.53 | ||
| 65+ | 2.03 | −0.48 | 4.60 | ||
| Non-Kuwaiti | Male | ||||
| Total | 2.15 * | 0.99 | 3.32 | ||
| <15 | 1.79 * | 0.29 | 3.32 | ||
| 15–64 | 0.12 | −1.83 | 2.10 | ||
| 65+ | 3.20 | −1.01 | 7.59 | ||
| Female | |||||
| Total | 0.99 | −0.42 | 2.42 | ||
| <15 | 1.18 | −0.58 | 2.97 | ||
| 15–64 | −0.20 | −2.82 | 2.49 | ||
| 65+ | 1.75 | −2.46 | 6.14 | ||
| Group | Total Admissions | Reduction in Number of Admissions per Year for 10 μg/m3 Reduction in PM2.5 (95% CI) |
|---|---|---|
| Overall | 218,403 | 391 (211, 571) |
| <15 | 134,191 | 262 (125, 351) |
| 15–64 | 59,655 | 53 (−28, 134) |
| 65+ | 24,557 | 62 (17, 107) |
| Male | 124,622 | 211 (92, 331) |
| Female | 93,781 | 180 (80, 281) |
| Kuwaiti | 128,533 | 265 (139, 393) |
| Non-Kuwaiti | 89,870 | 124 (0, 222) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albahar, S.; Li, J.; Al-Zoughool, M.; Al-Hemoud, A.; Gasana, J.; Aldashti, H.; Alahmad, B. Air Pollution and Respiratory Hospital Admissions in Kuwait: The Epidemiological Applicability of Predicted PM2.5 in Arid Regions. Int. J. Environ. Res. Public Health 2022, 19, 5998. https://doi.org/10.3390/ijerph19105998
Albahar S, Li J, Al-Zoughool M, Al-Hemoud A, Gasana J, Aldashti H, Alahmad B. Air Pollution and Respiratory Hospital Admissions in Kuwait: The Epidemiological Applicability of Predicted PM2.5 in Arid Regions. International Journal of Environmental Research and Public Health. 2022; 19(10):5998. https://doi.org/10.3390/ijerph19105998
Chicago/Turabian StyleAlbahar, Soad, Jing Li, Mustafa Al-Zoughool, Ali Al-Hemoud, Janvier Gasana, Hassan Aldashti, and Barrak Alahmad. 2022. "Air Pollution and Respiratory Hospital Admissions in Kuwait: The Epidemiological Applicability of Predicted PM2.5 in Arid Regions" International Journal of Environmental Research and Public Health 19, no. 10: 5998. https://doi.org/10.3390/ijerph19105998
APA StyleAlbahar, S., Li, J., Al-Zoughool, M., Al-Hemoud, A., Gasana, J., Aldashti, H., & Alahmad, B. (2022). Air Pollution and Respiratory Hospital Admissions in Kuwait: The Epidemiological Applicability of Predicted PM2.5 in Arid Regions. International Journal of Environmental Research and Public Health, 19(10), 5998. https://doi.org/10.3390/ijerph19105998