
A Rapid Review of Interventions to Increase Hepatitis B Testing, Treatment, and Monitoring among Migrants Living in Australia



Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
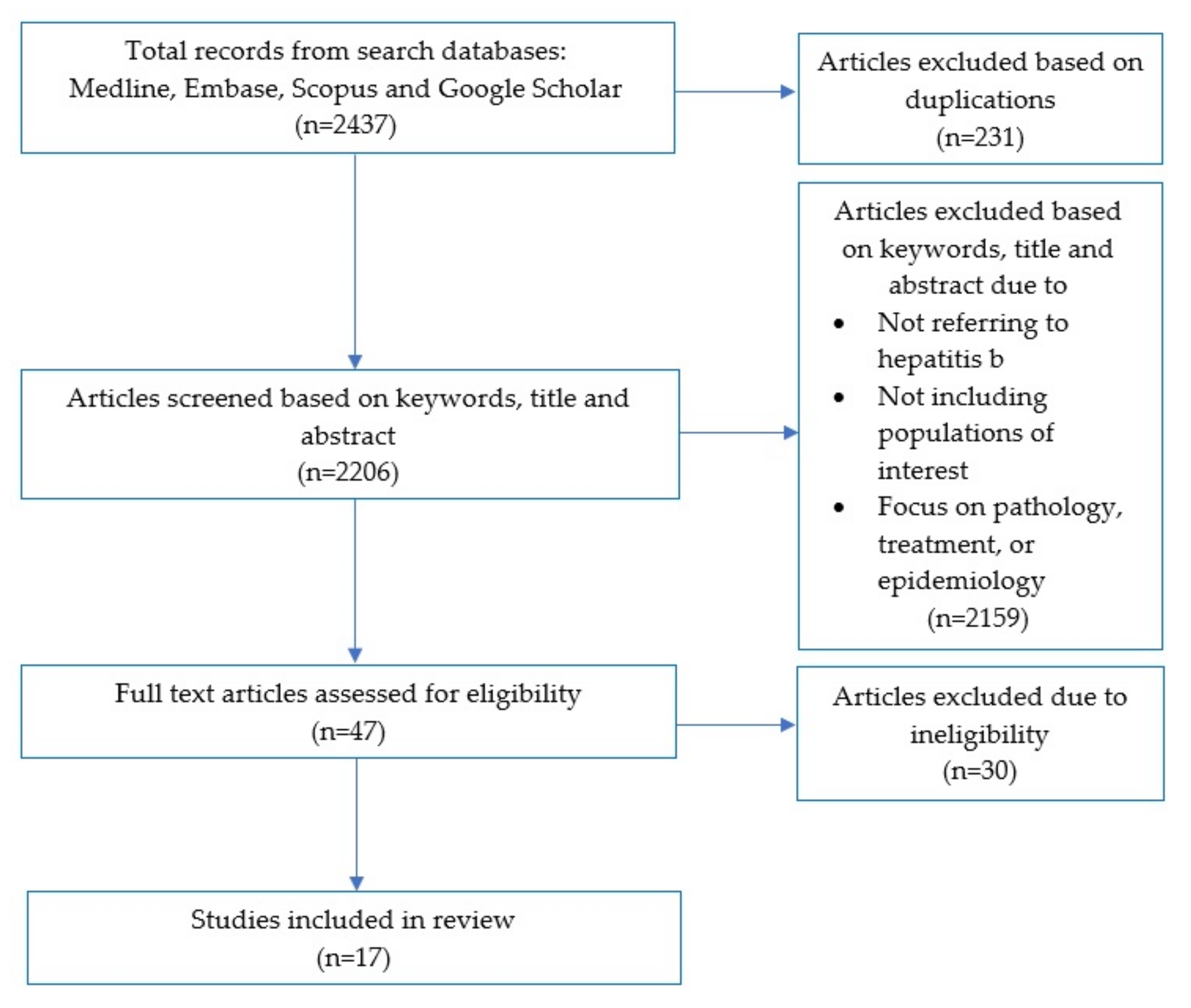
2.3. Screening
2.4. Data Extraction
2.5. Evidence Synthesis
3. Results
3.1. Overview of the Studies
3.2. Participant Characteristics
3.3. Individual Interventions
3.3.1. Outreach Testing
3.3.2. Overview of Outreach Testing Strategies Utilised
3.4. Provider-Initiated Testing
Overview of Provider-Initiated Strategies Utilised
3.5. Community Interventions
Overview of Community Intervention Strategies Utilised
3.6. Structural Interventions
3.7. Study Recommendations
4. Discussion
4.1. Testing
4.2. Treatment and Monitoring
4.3. Impact of Intervention Settings
4.4. Role of Linguistic-Specific and Culturally Appropriate Resources
4.5. Uptake of Intervention Based on Gender
4.6. Study Design and Reporting Limitations
4.7. Strengths and Limitations
4.8. Implications for Research, Policy, and Practice
4.8.1. Research Opportunities
4.8.2. Clinical Practice Opportunities
4.8.3. Health Promotion Opportunities
4.8.4. Policy and Advocacy Opportunities
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Author and Publication Date | Title | Population and Sample Size | Location | Aim | Methodology | Intervention, Intervention Type and Setting | Outcome Measures | Results | Implications for Research, Policy and Practice |
| Ash et al. (2018) [31] | Hepatitis B contact tracing: What works? | Refugees from high-prevalence countries. n = 122 (41% female, 59% male) | Australia | To describe the structure of the contact tracing system; and to determine its effectiveness and identify enablers of success. | A retrospective clinical audit conducted over 2 months. Index cases were CHB-positive patients identified in the practice’s Chronic Disease Management (CDM) Care Plan database. Contacts were individuals listed as household contacts on a ‘contact tracing chart’ by each index case. Interviews were conducted with health professionals across different disciplines to identify enablers of contact tracing (CT) success. | Auditing of clinical records and CT; Individual; Primary care. | Proportion of contacts traced and serologically confirmed as infected, immune or susceptible to HBV, enablers of CT success. | There were 122 index cases and 420 contacts. 339 (80.7%) contacts were immune (121 because of cleared previous HBV infection and 218 through prior vaccination). 34 (8.1%) were already identified as CHB-positive through new arrival screening. 90.5% of contacts were either immune or infected and would not benefit from subsequent vaccination. 379 (90.2%) contacts were already registered at the practice. 380 (90%) contacts were successfully traced. In total, 83 (68%) of index cases had all their contacts successfully traced. CT enabled the identification and immunisation of 27 (6.4%) uninfected susceptible individuals. | CT system used serological evidence, which is likely to be more accurate as it does not rely on patient recall or knowledge of contact tracing. It also does not rely on clinician reports, which may vary depending on individuals’ definitions of successful contact, which can overestimate the success. CT system provided an organised and convenient system of reference in the case of enquiry of immune status. Therefore, if household members changed over time, the CT system ensured a systematic approach to reviewing and updating household contacts and inviting new household members for screening. Integration into the CDM Care Plan scheme provides time for CT, patient education and administration. |
| Chandrasekar et al. (2016) [32] | A novel strategy to increase identification of African-born people with chronic hepatitis B virus infection in the Chicago metropolitan area, 2012–2014 | African-born persons. n = 1000 (51% female, 49% male of 445 screened) | US | To use a novel strategy of chain referral sampling to conduct HBV testing and describe the prevalence of chronic HBV infection among a sample of people born in Africa and now residing in the Chicago Metropolitan area. | A hepatitis education and prevention program was developed in collaboration with academic, clinical, and community partners for immigrant and refugee populations at risk for HBV infection. Community health workers implemented chain referral sampling, a novel strategy for recruiting hard-to-reach participants, targeting African-born participants. Participants were tested in both clinical and non-clinical settings. The clinic settings included community and federally qualified health centres, charitable organizations, solo and small group physician practices, and local hospitals. Physicians briefly educated participants about HBV and offered a free blood test. Non-clinical settings consisted of health fairs and other events hosted by community and faith-based organizations. Screenings followed educational workshops delivered in the target languages of participants or interpreted by trained bilingual community health workers. | Education and chain-referral sampling by community health workers; Community; Community (church groups) and primary care. | HBV testing uptake and linkage to care uptake. | Tested 45% of the target population and identified 8% with chronic HBV infection. The strategy leveraged community health workers, in conjunction with peer and faith-based leaders, who were in the position to engage a hard-to-reach population. Intervention reached a population who needed services but were limited by access and language barriers. Chain referral sampling helped to overcome some challenges of limited English language comprehension, illiteracy, and mistrust. Additionally, the strategy led to the identification of people susceptible to HBV infection and facilitated HBV vaccination. | There is a need for health promotion programs that are culturally appropriate and community-driven. Cultural barriers including denial and social stigma, as well as concerns about the cost of treatment if tested positive, tended to perpetuate racial/ethnic disparities in HBV disease despite the involvement of peers. The recruitment strategy helped to mitigate this distrust because of the natural social networks that contextualized participants’ involvement. Recommendation for HBV testing by respected fellow members of the community promoted buy-in. |
| Chandrasekar et al. (2015) [33] | A comparison of effectiveness of hepatitis B screening and linkage to care among foreign-born populations in clinical and non-clinical settings | Foreign-born Asian Americans, n = 758 (62% female, 38% male) | US | To demonstrate the comparabilityof screening participation and follow-up linkage to care forthe chronically infected in clinical and non-clinical settings. | The Asian Health Coalition (AHC) and its community partners conducted HBV screenings and follow-up linkage to care in both clinical and non-clinical settings. Participants were notified of their test outcome by letter if immune, if susceptible and requiring vaccination or if chronically infected and provided with instructions for seeking medical attention. Screenings in non-clinical settings were held in conjunction with an education session on HBV delivered either in the target language of the community or with interpretation using bilingual community health workers trained by AHC staff in the Hepatitis Education and Prevention Program (HEPP) model. Participants were offered free HBV screenings after the education sessions. | Education and chain-referral sampling by community health workers; Community; Community (church groups) and primary care. | HBV testing uptake and linkage to care uptake. | Prevalence of HBsAg in the sample was 7.3% (n = 55). Individuals who ended up testing positive for the disease were as likely to participate in clinical and non-clinical settings. Of those who tested positive in clinical settings, 9 of 16 (55%) were referred to follow-up medical care. For those tested in a non-clinical setting, 30 out of 39 (77%) were referred to medical care. This shows a higher linkage to care in non-clinical settings. | Demonstrates the merits of using a community-based model for linkage to care. HBV screenings for Asian Americans in non-clinical settings were valued equally to the clinical settings. Findings showed that there were no significant differences. This outcome is consistent with the hypothesis that non-clinical settings can reach a large segment of underserved foreign-born populations who tend to be uninsured and have limited English proficiency. A significant finding was the successful linkage to care available in non-clinical settings as compared to clinical settings. Community health workers in non-clinical settings are also integral pillars for success in overcoming distrust among foreign-born underserved populations. |
| Crawshaw et al. (2018) [34] | Infectious disease testing of UK-bound refugees: A population-based, cross-sectional study | Foreign-born refugees, n = 18,418 (48.8% female, 51.2% male) | UK | To analyse and describe data on the prevalence of all infectious diseases (tuberculosis (TB), HIV, syphilis, hepatitis B and hepatitis C) from a large cohort of refugees who underwent comprehensive pre-entry health assessments as part of the UK resettlement programme. Compare the recorded prevalence against published estimates to assess whether moving to risk-based testing would be feasible. Primary aim of the UK programme and health assessments is to facilitate early integration and linkage of the refugee to appropriate health and social services in the UK. | 22 International Organization for Migration (IOM) clinics were enrolled in 14 countries. All information was entered into the medical module of IOM’s electronic database system, the Migrant Management Operational System Application (MiMOSA), which has a set of data validation rules in place, and further data validation was done by the IOM medical department using statistical and database functions. | Pre-entry health assessment; Structural; Clinical health-service. | HBV screening. | Of 188 cases of HBV, 130 (69%) were male and 132 (70%) were aged between 25 and 49 years. The overall testing yield for HBV was 2.04% (1.77–2.35%) and ranged by nationality from 0.58% (0.19–1.79%) for Iraq to 12.50% (5.24–26.96%) for South Sudan. | This study found higher diagnostic yields than expected for several diseases, including HBV. The UK programme is particularly focused on the resettlement of vulnerable refugees, and whilst the possibility of testing bias cannot be ruled out, it is likely this refugee population significantly differs from the general population of the respective country. |
| Dang et al. (2016) [35] | Increasing hepatitis B testing and linkage to care of foreign-born Asians, Sacramento, California, 2012-2013 | Foreign-born Chinese, Hmong, Korean and Vietnamese. n = 1004 (62.7% female, 37.7% male) | US | To test at least 1000 foreign-born adult Asian Americans who had not been previously serologically tested for HBV. To counsel at least 90% of the people testing positive for HBsAg. | Engaged organisations linked to Chinese, Hmong, Korean and Vietnamese communities to co-sponsor HBV screenings of Asian Americans, post-test counselling and linkage to care. | Outreach testing; Individual; Community (student-run medical clinics, heritage associations and churches). | HBV screening uptake. | 76 of 1004 participants tested positive for HBV and post-test counselling was provided to 51 participants. | Collaborating with community groups and addressing barriers to screening highlighted how community partners can work together to address linguistic, cultural and transportation barriers among an Asian population to implement a successful HBV initiative. |
| Flanagan et al. (2019) [36] | Case finding and therapy for chronic viral hepatitis in primary care (HepFREE): A cluster: randomised controlled trial | Migrants from high-risk countries. n = 90,250 (52% female, 48% male) | UK | To determine whether incentivising and supporting primary-care physicians in areas with a high density of migrants increases the numbers of adult migrants screened for viral hepatitis. | General practices were randomly assigned to an opportunistic screening (control) group or one of four targeted screening (interventional) groups; standard (ie, hospital-based) care and a standard invitation letter; standard care and an enhanced invitation letter; community care and a standard invitation letter; or community care and an enhanced invitation letter. In control screening, general practitioners (GPs) were given a teaching session on viral hepatitis and were asked to test all registered migrants. In the intervention, GPs were paid a nominal sum for setting up searches of records, reimbursed for signed consent forms, and supported by a dedicated clinician. Patients who were eligible for testing and tested positive for viral hepatitis in the intervention groups were eligible to enrol in a second embedded trial of community versus hospital-based care. | Incentivising GPs; Individual; Primary care (general practices). | HBV screening uptake. | Compared to control groups where only 1.7% of eligible participants took up screening, 19.5% of eligible participants in intervention groups took up screening. More than 80% of HBsAg positive participants were linked to care. | Screening migrants for viral hepatitis in primary care is effective if doctors are incentivised and supported. |
| Hargreaves et al. (2020) [37] | Delivering multi-disease screening to migrants for latent TB and blood-borne T viruses in an emergency department setting: A feasibility study | Foreign-born economic migrants, asylum seekers and refugees. n = 96 (48% female, 52% male) | UK | To investigate the delivery of an opportunistic screening model offering new migrants multi- disease screening using a one-stop blood test for latent tuberculosis infection (LTBI) combined with HIV and hepatitis B/C in an emergency department setting. | The PROMOTE study was conducted at St. Mary's Hospital Emergency Department, London, UK, which is a high-migrant area representative of many of the Boroughs across London, and where 49.8% of the resident population was born abroad. Migrant patients meeting the study inclusion criteria were offered combined infection screening in addition to the standard care they received and followed up according to routine care pathways. The screening intervention was a single venesection to test for: (i) LTBI using interferon gamma release assay (QuantiFERON-TB Gold in-tube); (ii) HIV (HIV screening assay); and (iii) hepatitis B surface antigen test (HBsAg) and (iv) hepatitis C antibody test (anti-HCVAb). Participants completed a questionnaire (piloted in this setting) with questions pertaining to time in the UK, nationality, registration with a local primary-care provider, and whether patients had previously been offered any kind of screening since their arrival. They then provided a peripheral venous blood sample, which was obtained by the research nurse. | Opportunistic screening; Individual; Other clinical health service-based (emergency department). | HBV screening uptake. | Of 96 migrants screened, there were 2 cases of HBV (1 case of HBV/LTBI co-infection). | Major gaps in current screening provision to new migrants. Need to promote screening for a more diverse range of key infections in the UK. Feasible to engage migrants in multi-disease screening. |
| Hsu et al. (2013) [38] | Electronic messages increase hepatitis B screening in at-risk Asian American patients: A randomized, controlled trial | Chinese and Vietnamese patients. n = 175 (61.4% female, 38.6% male) in intervention group | US | To determine the effectiveness of electronic health record (EHR) prompts to increase the ordering of HBV tests among primary care providers (PCPs) within an academic health system. | Providers were randomized to either receive an EHR prompt for HBV testing prior to patients’ appointments or usual care. Primary outcomes were the proportion of patients (1) whose physician ordered a HBsAg test and (2) who completed testing. Secondary outcomes were (A) test results and (B) whether the physicians followed up on the results. Providers in the intervention received an electronic prompt 24 hours before their patient’s scheduled appointment that identified the patient as a candidate for HBV testing and urged the provider to evaluate the patient for testing. The message, sent by a hepatologist to the provider’s EHR inbox, consisted of several components including a description of the Centre for Disease Control’s recommendations for HBV testing in at-risk Asian populations, the high prevalence of HBV in Asia, and a list of the appropriate laboratory tests for proper HBV screening. | EHR prompts; Individual; Primary care. | Ordering of HBV tests and linkage to care uptake. | HBsAg tests were ordered for 36/88 (40.9%) of the intervention patients and 1/87 (1.1%) of the control patients. 30 intervention patients (34.1%) and no control patients completed the HBsAg test. From the 30 intervention patients, four (13.3%) of the completed tests were HBsAg-positive, 14 (46.7%) were immune, and 12 (40%) were unprotected from HBV. Two HBsAg-positive patients were referred to specialists, and 3 unprotected patients were vaccinated for HBV. | EHR-based provider prompts significantly increased HBV testing in Chinese and Vietnamese patients. |
| Kelly et al. (2020) [39] | Improving uptake of hepatitis B and hepatitis C testing in South Asian migrants in community and faith settings using educational interventions – A prospective descriptive study | South Asian migrants. n = 219 (53% female, 47% male) | UK | To analyse the feasibility of recruiting South Asian migrants to view an educational film on CVH and the effectiveness of the film in promoting testing and increasing knowledge of CVH, and the methodological issues relevant to scale-up to a randomized controlled trial. | Qualitative data were used to inform the development of a short film to explain CVH, modes of transmission, and how to access testing. South Asian migrants were recruited to view the film in community venues (primary care, religious, community), with dried blood spot CVH testing offered immediately afterwards. Pre/post-film questionnaires assessed the effectiveness of the intervention. | Educational film; Community; Community, religious centres and primary care. | CVH testing uptake. | This study satisfied the major pre-defined criteria for success: 84% versus 40% of participants watching the film being tested. A particular success was the recruitment of the older age group and females (53%) to the film screening. A number of participants (n = 45) requested testing for CVH without having seen the intervention. This may suggest that other factors including community endorsement may be relevant in testing. | This study demonstrated the feasibility of recruiting first-generation migrants to view a community-based educational film promoting CVH testing in this higher-risk group, confirming the value of developing interventions to facilitate the global World Health Organization plan for targeted case finding and elimination, and a future randomized controlled trial. The study highlighted the importance of culturally relevant interventions including faith and culturally sensitive settings, which appear to minimize logistical issues and effectively engage minority groups, allowing ease of access to individuals ‘at risk’. |
| Navarro et al. (2014) [40] | Lower than expected hepatitis B virus infection prevalence among first generation Koreans in the US: Results of HBV screening in the Southern Californian Empire | First-generation Koreans. n = 1007 (60.5% female, 39.5% male) | US | To screen adult individuals to establish HBV serological diagnoses, educate, and establish linkage to care for vaccination and consideration of treatment. | 10 community-screening events across 9 Korean churches over 3.6 months. Advertisements highlighting the importance of HBV testing and details were placed in Korean newspapers and newsletters several weeks prior to each event to target non-church attendees. Flyers were also posted at churches and local primary health clinics predominantly serving Koreans. A bilingual Korean nurse led the events. Screening was preceded by a brief lecture on HBV. Educational materials on HBV were distributed to all attendees. Subjects completed a brief self-administered questionnaire and provided contact information for result notification. A letter describing test results and their interpretation along with medical recommendations was mailed to each participant. | Educational and outreach intervention led by bilingual nurse; Individual; Community (churches). | HBV screening uptake and linkage to care uptake. | Prevalence of HBV was 3.0% (29 participants). Despite this barrier, 2 of the 10 infected women and 6 of the 19 men had effective follow-up visits, for a total of 27.5% (8) success in linkage to care. Of the 8 participants seen in clinic half did not require treatment. The other half was provided guidance on patient medication assistance programs and started antiretroviral therapy. The overall rate of incorrect report of immunization status was 35.1% (342), differing across education levels (p = 0.008) but not between genders (p = 0.888) | Results highlight the importance of complete serological screening among migrants before recommending immunization, as well as serological follow up to confirm successful immunization. With as many as 70% of Koreans in the US attending religious services regularly, most being first-generation immigrants, it is believed that religious congregations are therefore optimal locations for health screenings of this type. |
| Perumalswami et al. (2013) [41] | Hepatitis Outreach Network: A practical strategy for hepatitis screening with linkage to care in foreign-born communities | Foreign-born from countries with a high prevalence of CVH. n = 1603 (50.6% female, 49.4% male) | US | To provide education, screening and linkage to care in communities with a high prevalence of CVH. | Hepatitis Outreach Network combined the expertise and resources of the Mount Sinai School of Medicine, the NYC Department of Health and Mental Hygiene, and community-based organizations, to provide education, screening and linkage to care in communities with a high prevalence of CVH. Comprehensive HBV and HCV screening identifies infected patients, who then receive further evaluation from either local or Mount Sinai physicians, combined with patient navigators who organize follow-up visits. | Educational and outreach intervention; Individual; Community (public schools, places of worship, YMCA’s, public parks, hotels, business centres and train stations). | HBV and HCV screening and linkage to care uptake. | Of the 76 persons (out of 1603) with HBV infection, 43 (57%) received a medical evaluation (31 with local providers and 12 at Mount Sinai). Of the 43 HBV-infected persons evaluated, treatment was recommended and begun in 5. | Successful recruitment into screening of foreign-born persons at high risk of HBV and/or HCV may be due to the engagement of community-based organisations and by employing languages of country of origin in publicizing the events. Non-traditional venues were chosen by partnering ommunity based organizations based on their knowledge and expertise of their community. Non-traditional venues included places that community members frequented often and trusted. |
| Raines-Milenkov et al. (2021) [42] | Hepatitis B virus awareness, infection, and screening multi-ethnic community intervention for foreign-born populations | Refugee immigrant population. n = 1069 (80% female, 20% male) | US | To assess HBV awareness, vaccination status at enrolment, infection and screening among a multi-ethnic, primarily refugee immigrant population enrolled in a community-based cancer prevention intervention. | Trained bilingual and bicultural community health workers (CHWs) representative of 24 different countries of origin provided outreach, enrolment, education and navigation services. Participants were recruited from apartment complexes, faith-based locations, through community leaders and events, word-of-mouth, resettlement agencies and to a lesser degree, clinics that serve the population. CHWs navigated HBV positive participants to health care when accepted by the participants. Screening is thus an opportunity to educate and provide treatment to individuals that test positive for HBV. | Educational and outreach intervention by bicultural CHWs; Individual; Community (churches, mosques, civic groups) and primary care. | HBV screening uptake. | 38% of participants accepted HBV screening after enrolment in the Building Bridges Initiative (BBI) program. More than three-quarters (76%) of those screened reported having never had HBV screening in the past. The HBV positivity rate was 6% among study participants who were screened through the BBI program. More individuals were screened in community settings rather than scheduled for clinics (68% vs 32%). | CHWs have a critical role to link HBV positive individuals to care. Despite several barriers to care being eliminated in this project, some participants with HBV declined and opted to use traditional medicine from their home country to treat their infection. |
| Shankar et al. (2016) [43] | A novel collaborative community-based hepatitis B screening and linkage to care program for African immigrants | African-born persons. n = 955 (24.5% female, 75.5% male) | US | To estimate the prevalence of current HBV infection among African-born NYC residents. To test the effectiveness of a community-based screening and linkage to care program that relies on culturally targeted patient navigators. Assess the role of known risk factors, and identify previously unknown risk factors in this population. | Hepatitis Outreach Network (HONE) partnered with a non-profit organisation to provide targeted screening for HBV to any African born adult >18 years of age. Before screening, participants were provided with a questionnaire to assess demographics and risk factors. Community members were invited to attend the screening events at no cost through public service announcements on local African radio stations, flyers at community venues, announcements by community and religious leaders, and word of mouth by the patient navigator at community events. A trained phlebotomist collected a blood sample on-site for serological testing for each patient. A culturally targeted, multilingual (English-, Arabic-, and French-speaking) professional patient navigator attempted to contact persons with their results via telephone 1 week after their screening. Upon completion of their visit, all persons were provided a round-trip public transportation fare card to cover travel costs and a $20 incentive for attending the visit. | Outreach testing and linkage to care with a culturally targeted patient navigator; Individual; Community (community centres, places of worship and sites of employment). | HBV screening and linkage to care uptake. | Of 955 persons screened for HBV, 919 had no history of liver disease, of whom 88 had a current HBV infection and 679 had exposure. 97% of infected persons were linked to care and 11 were recommended for treatment, of whom 9 started therapy. | Culturally targeted patient navigators are critical to establishing effective community-based viral hepatitis screening and linkage-to-care programs, particularly in programs targeting foreign-born persons. |
| Standford et al. (2016) [44] | Community-engaged strategies to promote hepatitis B testing and linkage to care in immigrants of Florida | Foreign-born nationals. n = 1516 (50.4% female, 49.6% male) | US | To increase the proportion of persons who are aware of their HBV status among individuals born in countries with intermediate or high prevalence of HBV infection; to increase the proportion who receive counselling and are linked to treatment and prevention services. | Community-based HBV screening programs occurred in an urban locale in both clinical and community settings. Screening, testing, and case identification activities included providing foreign-born nationals (FBNs) with an HBV risk assessment and no cost HBV test. FBNs were offered the opportunity to participate in a clinical or community setting. Communication barriers were reduced by translating program materials (i.e., written screening consent, educational materials, and test result notification letters) into 13 different languages. Participants received culturally appropriate education and awareness materials and instructions on receiving post-test counselling and results, and a $15 gift card participation incentive. Outreach post-test counselling events were conducted in conveniently located community settings. Low risk test results were mailed with risk reduction educational materials post-test. More intensive contact attempts were made for participants with high-risk test results, and participants with HBsAg positive results. Participants with high-risk test results were contacted by phone to schedule an in-person appointment to provide test results and conduct post-test counselling. HBsAg positive participants were linked to care and vaccination services accordingly. | Educational and outreach intervention by CHWs and certified medical assistants; Individual; Community (faith-based organisations, refugee servicing organisations), primary care and emergency department. | HBV screening uptake and linkage to care uptake. | 1516 individuals underwent HBV testing and screening, 831 individuals received post-test counselling and, 43 HBsAg positive participants were linked to medical care. | Community-engaged strategies to improve HBV testing and service linkage in FBN populations should be considered when planning programs. |
| Vedio et al. (2013) [45] | Hepatitis B: Report of prevalence and access to healthcare among Chinese residents in Sheffield, UK | Chinese residents. n = 229 (57.5 female, 42.5% male) | UK | To facilitate HBV testing using straightforward methods in culturally appropriate settings to assess the acceptance of this testing method by Chinese residents. To estimate the local rate of undiagnosed infection and to provide access to expert healthcare for those affected. | Identified locations that would be familiar to Chinese members of the community to facilitate testing. Dried blood spot samples were collected from 229 Chinese subjects and tested for HBV and HCV infection. | Educational and outreach intervention; Individual; Community (Kinhon Chinese Centre). | HBV screening uptake and participant feedback. | 28 of 229 patients had evidence of past HBV infection. 20 of 229 were diagnosed with HBsAg. 5 of the participants (4 females and 1 male, age range 23-43 years) were of Chinese origin but were born in the UK, but results were negative for all HBV markers in these 5 participants. Self-reported diagnosis showed that women had the highest rate of having had a previous diagnosis of HBV infection compared to men (5:1). | The study demonstrated the importance of outreach and targeted testing. |
| Xiao et al. (2021) [46] | Assessing the feasibility, acceptability and impacts of an education program on hepatitis B testing uptake among ethnic Chinese in Australia: Results of a randomised controlled pilot study | Individuals of Chinese ethnicity. n = 54 (69% female, 31% male) | Australia | To explore approaches to increase HBV testing in Australia’s Chinese community and inform evaluation planning, specifically to i) assess the feasibility and acceptability of HBV educational programs, and ii) compare HBV testing uptake in people receiving a tailored education resource focussing on liver cancer prevention compared with a standard HBV education package. | People of Chinese ethnicity and unsure of their HBV infection or immunity status were recruited from 10 community sites. Participants were randomised to receive an education package (comprised of a leaflet and in-person one-on-one educational session) with a focus on either 1) standard HBV-related information, or 2) liver cancer prevention. Participants completed a baseline questionnaire prior to receiving the intervention and were followed up at 6 months for a questionnaire and an opt-in semi-structured interview. | Educational and outreach intervention; Individual; Community-based organisations. | HBV testing uptake, intervention acceptability and feasibility of the study. | 54 participants received an education package; baseline and follow-up data from 33 (61%) were available. The study procedures of recruitment and retention were feasible; the acceptability of the education program was moderate with improved HBV-related knowledge observed. 4 participants self-reported being tested: 1 (1/15, 7%) in the standard HBV information group and 3 (3/18, 17%) in the liver cancer prevention information group. | A larger study is required to determine if a liver cancer prevention message would improve HBV testing uptake in the Chinese community than a standard HBV education message. Support from healthcare providers, community-based testing programs, and public health education programs are likely needed to motivate diagnostic testing among Chinese people at risk of HBV infection. |
| Zibrik et al. (2018) [47] | Let’s Talk About B: Barriers to hepatitis B screening and vaccination among Asian and South Asian immigrants in British Columbia | Korean, Chinese, Filipino and South Asian Immigrants. n = 827 (70% female, 30% male) | Canada | To describe different types of viral hepatitis and the severity of infection. Emphasize HBV prevention including screening, vaccination and risk reduction strategies. Outline symptoms and transmission routes of HBV. Describe HBV treatment and pathway for care; identify community resources and supports for people living with HBV Promote a healthy lifestyle to prevent the progression of liver disease. | Culturally tailored HBV education workshops were delivered over 12 months. Data from pre- and post-workshop surveys and 2-week and 1-month follow-up interviews were collected and analysed to evaluate knowledge gaps and challenges around HBV prevention and screening. Barriers, health care service gaps and facilitators identified in the interviews were coded and analysed. | Culturally tailored education workshops; Community; Community (community centres, immigration settlement service centres, organised health events and religious/cultural gathering places). | Self-reported action related to HBV prevention and management. | Data were collected from 827 participants who attended workshops. 633 participants took part in the 2-week and 1-month follow-up interviews conducted via telephone. Of these, 55% took specific action related to HBV prevention or management such as proactively sought out/read information (online or in print) on HBV; talked to their doctor/health professional about HBV testing/care; got tested for HBV following the workshop; scheduled an appointment to see their doctor/health professional; checked their vaccination status or that of a family member; got vaccinated against HBV. | Study findings support the need for culturally tailored HBV public education and outreach programs to further advance HBV immunization and awareness in British Columbia. Addressing barriers and developing targeted programmatic strategies identified in this study will promote more effective HBV education programming and improve uptake of HBV screening and vaccination in British Columbia’s immigrant populations. |
References
- World Health Organization. Combating Hepatitis B and C to Reach Elimination by 2030; WHO: Geneva, Switzerland, 2016; pp. 1–24. [Google Scholar]
- Kim, J.U.; Patrick, I.; Yusuke, S.; Maud, L. Improving care of migrants is key for viral hepatitis elimination in Europe. Bull. World Health Organ. 2021, 99, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Romero, N.; McCulloch, K.; Allard, N.; MacLachlan, J.; Cowie, B. National Surveillance for Hepatitis B Indicators: Measuring the Progress towards the Targets of the National Hepatitis B Strategy—Annual Report 2019; WHO Collaborating Centre for Viral Hepatitis: Melbourne, Australia, 2020. [Google Scholar]
- Brown, C.R.; Allard, N.L.; MacLachlan, J.H.; Cowie, B.C. Deaths from liver cancer continue to rise in Australia: Is elimination by 2030 possible? Intern. Med. J. 2017, 47, 604–605. [Google Scholar] [CrossRef] [PubMed]
- Australian Government Department of Health. Third National Hepatitis B Strategy; Commonwealth of Australia: Canberra, Australia, 2018.
- Carville, K.S.; Cowie, B.C. Recognising the role of infection: Preventing liver cancer in special populations. Cancer Forum 2012, 36, 23–26. [Google Scholar]
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016–2021: Towards Ending Viral Hepatitis; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Guirgis, M.; Nusair, F.; Bu, Y.M.; Yan, K.; Zekry, A.T. Barriers faced by migrants in accessing healthcare for viral hepatitis infection. Intern. Med. J. 2012, 42, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Metusela, C.; Ussher, J.; Perz, J.; Hawkey, A.; Morrow, M.; Narchal, R.; Estoesta, J.; Monteiro, M. “In my culture, we don’t know anything about that”: Sexual and reproductive health of migrant and refugee women. Int. J. Behav. Med. 2017, 24, 836–845. [Google Scholar] [CrossRef] [PubMed]
- Place, V.; Nabb, B.; Viksten Assel, K.; Bäärnhielm, S.; Dalman, C.; Hollander, A. Interventions to increase migrants’ care-seeking behaviour for stigmatised conditions: A scoping review. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 56, 913–930. [Google Scholar] [CrossRef] [PubMed]
- Wallace, J.; Smith, E.; Hajarizadeh, B.; Richmond, J.; Lucke, J. Addressing cultural diversity: The hepatitis B clinical specialist perspective. Ethn. Health 2019, 24, 816–828. [Google Scholar] [CrossRef]
- Hajarizadeh, B.; Wallace, J.; Richmond, J.; Ngo, N.; Enright, C. Hepatitis B knowledge and associated factors among people with chronic hepatitis B. Aust. N. Z. J. Public Health 2015, 39, 563–568. [Google Scholar] [CrossRef]
- Pley, C.M.; McNaughton, A.L.; Matthews, P.C.; Lourenço, J. The global impact of the COVID-19 pandemic on the prevention, diagnosis and treatment of hepatitis B virus (HBV) infection. BMJ Glob. Health 2021, 6, e004275. [Google Scholar] [CrossRef]
- Supramaniam, R.; O'Connell, D.; Tracey, E.; Sitas, F. Differences in cancer incidence by country of birth in New South Wales 1991 to 2001: Healthy migrants, ascertainment bias or salmon swimming upstream? Australas. Epidemiol. 2006, 13, 51. [Google Scholar]
- Robotin, M.C.; Kansil, M.Q.; Porwal, M.; Penman, A.G.; George, J. Community-based prevention of hepatitis-B-related liver cancer: Australian insights. Bull. World Health Organ. 2014, 92, 374–379. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Health Sector Strategy on Sexually Transmitted Infections 2016–2021: Towards Ending STIs; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Whitehead, M. A typology of actions to tackle social inequalities in health. J. Epidemiol. Community Health 2007, 61, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Seedat, F.; Hargreaves, S.; Friedland, J.S. Engaging new migrants in infectious disease screening: A qualitative semi-structured interview study of UK migrant community health-care leads. PLoS ONE 2014, 9, e108261. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.F.; Ma, G.X.; Miranda, J.; Eng, E.; Castille, D.; Brockie, T.; Jones, P.; Airhihenbuwa, C.O.; Farhat, T.; Zhu, L.; et al. Structural interventions to reduce and eliminate health disparities. Am. J. Public Health 2019, 109, S72–S78. [Google Scholar] [CrossRef] [PubMed]
- Blankenship, K.M.; Reinhard, E.; Sherman, S.G.; El-Bassel, N. Structural interventions for HIV prevention among women who use drugs: A global perspective. J. Acquir. Immune Defic. Syndr. 2015, 69, S140–S145. [Google Scholar] [CrossRef]
- Zhou, K.; Fitzpatrick, T.; Walsh, N.; Kim, J.Y.; Chou, R.; Lackey, M.; Scott, J.; Lo, Y.-R.; Tucker, J. Interventions to optimise the care continuum for chronic viral hepatitis: A systematic review and meta-analyses. Lancet Infect. Dis. 2016, 16, 1409–1422. [Google Scholar] [CrossRef]
- Luchenski, S.; Maguire, N.; Aldridge, R.W.; Hayward, A.; Story, A.; Perri, P.; Withers, J.; Clint, S.; Fitzpatrick, S.; Hewett, N. What works in inclusion health: Overview of effective interventions for marginalised and excluded populations. Lancet 2018, 391, 266–280. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O'Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- The World Bank. World Bank Country and Lending Groups. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519%23East_Asia_and_Pacific (accessed on 8 April 2022).
- Garritty, C.; Gartlehner, G.; Nussbaumer-Streit, B.; King, V.J.; Hamel, C.; Kamel, C.; Affengruber, L.; Stevens, A. Cochrane Rapid Reviews Methods Group offers evidence-informed guidance to conduct rapid reviews. J. Clin. Epidemiol. 2021, 130, 13–22. [Google Scholar] [CrossRef]
- International Organization for Migration. Key Migration Terms. Available online: https://www.iom.int/key-migration-terms (accessed on 8 April 2022).
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Cleo, G.; Scott, A.M.; Islam, F.; Julien, B.; Beller, E. Usability and acceptability of four systematic review automation software packages: A mixed method design. Syst. Rev. 2019, 8, 145. [Google Scholar] [CrossRef] [PubMed]
- Waffenschmidt, S.; Knelangen, M.; Sieben, W.; Bühn, S.; Pieper, D. Single screening versus conventional double screening for study selection in systematic reviews: A methodological systematic review. BMC Med. Res. Methodol. 2019, 19. [Google Scholar] [CrossRef] [PubMed]
- Stovold, E.; Beecher, D.; Foxlee, R.; Noel-Storr, A. Study flow diagrams in Cochrane systematic review updates: An adapted PRISMA flow diagram. Syst. Rev. 2014, 3, 54. [Google Scholar] [CrossRef] [PubMed]
- Ash, T.; Mascarenhas, L.; Furler, J.; Temple-Smith, M. Hepatitis B contact tracing: What works? Aust. J. Prim. Health 2018, 24, 470–479. [Google Scholar] [CrossRef]
- Chandrasekar, E.; Song, S.; Johnson, M.; Harris, A.M.; Kaufman, G.I.; Freedman, D.; Quinn, M.T.; Kim, K.E. A novel strategy to increase identification of african-born people with chronic hepatitis B virus infection in the Chicago Metropolitan area, 2012–2014. Prev. Chronic Dis. 2016, 13, E118. [Google Scholar] [CrossRef]
- Chandrasekar, E.; Kaur, R.; Song, S.; Kim, K.E. A comparison of effectiveness of hepatitis B screening and linkage to care among foreign-born populations in clinical and nonclinical settings. J. Multidiscip. Healthc. 2015, 8, 1–9. [Google Scholar] [CrossRef]
- Crawshaw, A.F.; Pareek, M.; Were, J.; Schillinger, S.; Gorbacheva, O.; Wickramage, K.P.; Mandal, S.; Delpech, V.; Gill, N.; Kirkbride, H.; et al. Infectious disease testing of UK-bound refugees: A population-based, cross-sectional study. BMC Med. 2018, 16, 143. [Google Scholar] [CrossRef]
- Dang, J.H.T.; Chen, M.S., Jr. Increasing hepatitis B testing and linkage to care of foreign-born Asians, Sacramento, California, 2012–2013. Public Health Rep. 2016, 131, 119–124. [Google Scholar] [CrossRef]
- Flanagan, S.; Kunkel, J.; Appleby, V.; Eldridge, S.E.; Ismail, S.; Moreea, S.; Griffiths, C.; Walton, R.; Pitt, M.; Salmon, A.; et al. Case finding and therapy for chronic viral hepatitis in primary care (HepFREE): A cluster-randomised controlled trial. Lancet Gastroenterol. Hepatol. 2019, 4, 32–44. [Google Scholar] [CrossRef]
- Hargreaves, S.; Nellums, L.B.; Johnson, C.; Goldberg, J.; Pantelidis, P.; Rahman, A.; Friedland FmedSci, J.S. Delivering multi-disease screening to migrants for latent TB and blood-borne viruses in an emergency department setting: A feasibility study. Travel. Med. Infect. Dis. 2020, 36, 101611. [Google Scholar] [CrossRef]
- Hsu, L.; Bowlus, C.L.; Stewart, S.L.; Nguyen, T.T.; Dang, J.; Chan, B.; Chen, M.S., Jr. Electronic messages increase hepatitis B screening in at-risk Asian American Patients: A randomized controlled trial. Dig. Dis. Sci. 2013, 58, 807–814. [Google Scholar] [CrossRef] [PubMed]
- Kelly, C.; Pericleous, M.; Ahmed, A.; Vandrevala, T.; Hendy, J.; Shafi, S.; Skene, S.S.; Verma, S.; Edge, C.; Nicholls, M.; et al. Improving uptake of hepatitis B and hepatitis C testing in South Asian migrants in community and faith settings using educational interventions—A prospective descriptive study. Int. J. Infect. Dis. 2020, 100, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Navarro, N.; Lim, N.; Kim, J.; Joo, E.; Che, K.; Runyon, B.A.; Mendler, M.H. Lower than expected hepatitis B virus infection prevalence among first generation Koreans in the U.S.: Results of HBV screening in the Southern California Inland Empire. BMC Infect. Dis. 2014, 14, 269. [Google Scholar] [CrossRef] [PubMed]
- Perumalswami, P.V.; Factor, S.H.; Kapelusznik, L.; Friedman, S.L.; Pan, C.Q.; Chang, C.; Di Clemente, F.; Dieterich, D.T. Hepatitis Outreach Network: A practical strategy for hepatitis screening with linkage to care in foreign-born communities. J. Hepatol. 2013, 58, 890–897. [Google Scholar] [CrossRef]
- Raines-Milenkov, A.; Felini, M.; Baker, E.; Acharya, R.; Longanga Diese, E.; Akpan, I.; Hussain, A.; Wagner, T. Hepatitis B virus awareness, infection, and screening multiethnic community intervention for foreign-born populations. J. Community Health 2021, 46, 967–974. [Google Scholar] [CrossRef]
- Shankar, H.; Blanas, D.; Bichoupan, K.; Ndiaye, D.; Carmody, E.; Martel-Laferriere, V.; Culpepper-Morgan, J.; Dieterich, D.T.; Branch, A.D.; Bekele, M.; et al. A novel collaborative community-based hepatitis B screening and linkage to care program for African immigrants. Clin. Infect. Dis. 2016, 62, S289–S297. [Google Scholar] [CrossRef]
- Stanford, J.; Biba, A.; Khubchandani, J.; Webb, F.; Rathore, M.H. Community-engaged strategies to promote hepatitis B testing and linkage to care in immigrants of Florida. J. Epidemiol. Glob. Health 2016, 6, 277–284. [Google Scholar] [CrossRef]
- Vedio, A.B.; Ellam, H.; Rayner, F.; Stone, B.; Kudesia, G.; McKendrick, M.W.; Green, S.T. Hepatitis B: Report of prevalence and access to healthcare among Chinese residents in Sheffield UK. J. Infect. Public Health 2013, 6, 448–455. [Google Scholar] [CrossRef][Green Version]
- Xiao, Y.; Wallace, J.; Ahad, M.; van Gemert, C.; Thompson, A.J.; Doyle, J.; Lam, H.Y.; Chan, K.; Bennett, G.; Adamson, E.; et al. Assessing the feasibility, acceptability and impacts of an education program on hepatitis B testing uptake among ethnic Chinese in Australia: Results of a randomised controlled pilot study. BMC Public Health 2021, 21, 1861. [Google Scholar] [CrossRef]
- Zibrik, L.; Huang, A.; Wong, V.; Novak Lauscher, H.; Choo, Q.; Yoshida, E.M.; Ho, K. Let’s Talk About B: Barriers to hepatitis B screening and vaccination among Asian and South Asian immigrants in British Columbia. J. Racial. Ethn. Health Disparities 2018, 5, 1337–1345. [Google Scholar] [CrossRef]
- Kennedy, C.E.; Fonner, V.A.; Sweat, M.D.; Okero, F.A.; Baggaley, R.; O’Reilly, K.R. Provider-initiated hiv testing and counseling in low- and middle-income countries: A systematic review. AIDS Behav. 2013, 17, 1571–1590. [Google Scholar] [CrossRef] [PubMed]
- Schweitzer, A.; Horn, J.; Mikolajczyk, R.; Krause, G.; Ott, J. Estimations of worldwide prevalence of chronic hepatitis B virus infection: A systematic review of data published between 1965 and 2013. Lancet 2015, 386, 1546–1555. [Google Scholar] [CrossRef]
- Dugas, M.; Bédard, E.; Batona, G.; Kpatchavi, A.C.; Guédou, F.A.; Dubé, E.; Alary, M. Outreach strategies for the promotion of HIV testing and care: Closing the gap between health services and female sex workers in Benin. J. Acquir. Immune Defic. Syndr. 2015, 68, S198–S205. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Hepatitis Report, 2017; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Krishnaswamy, S.; Cheng, A.C.; Wallace, E.M.; Buttery, J.; Giles, M.L. Understanding the barriers to uptake of antenatal vaccination by women from culturally and linguistically diverse backgrounds: A cross-sectional study. Hum. Vaccin Immunother. 2018, 14, 1591–1598. [Google Scholar] [CrossRef] [PubMed]
- Vujcich, D.; Reid, A.; Durham, J.; Mullens, A.B.; Gu, Z.; Debattista, J.; Parma, G.; Mao, L.; Guy, R.; Brown, G.; et al. Migrant Blood-Borne Virus and Sexual Health Survey 2020–2021: Queensland Results; Curtin University Perth: Perth, Australia, 2021. [Google Scholar]
- Allard, N.L.; MacLachlan, J.H.; Cowie, B.C. The cascade of care for Australians living with chronic hepatitis B: Measuring access to diagnosis, management and treatment. Aust. N. Z. J. Public Health 2015, 39, 255–259. [Google Scholar] [CrossRef]
- Hyun, S.; Ko, O.; Kim, S.; Ventura, W.R. Sociocultural barriers to hepatitis B health literacy in an immigrant population: A focus group study in Korean Americans. BMC Public Health 2021, 21, 1–11. [Google Scholar] [CrossRef]
- Alidu, L.; Grunfeld, E.A. Gender differences in beliefs about health: A comparative qualitative study with Ghanaian and Indian migrants living in the United Kingdom. BMC Psychol 2017, 5, 8. [Google Scholar] [CrossRef]
- Yang, Y.; Yan, M.; Yue, M.; Wang, X.; Zhang, W.; Li, J.; Li, S. Prevalence of hepatitis B and knowledge about hepatitis B among migrant workers in Shandong Province, China: A cross-sectional study. Iran. Red. Crescent Med. J. 2015, 17, e26725. [Google Scholar] [CrossRef]
- Papanicolas, I.; Woskie, L.R.; Jha, A.K. Health care spending in the United States and other high-income countries. JAMA 2018, 319, 1024–1039. [Google Scholar] [CrossRef]
- Lippman, S.A.; Chinaglia, M.; Donini, A.A.; Diaz, J.; Reingold, A.; Kerrigan, D.L. Findings from Encontros: A multi-level STI/HIV intervention to increase condom use, reduce STI, and change the social environment among sex workers in Brazil. Sex Transm. Dis. 2012, 39, 209–216. [Google Scholar] [CrossRef]
- Brown, G.; Reeders, D.; Dowsett, G.; Ellard, J.; Carman, M.; Hendry, N.; Wallace, J. Investigating combination HIV prevention: Isolated interventions or complex system. J. Int. AIDS Soc. 2015, 18, 20499. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ottawa Charter for Health Promotion; WHO: Geneva, Switzerland, 1986. [Google Scholar]
- Richmond, J.; Smith, E.; Wallace, J.; Duncan, D.; Lucke, J. Hepatitis B testing and diagnosis experiences of patients and primary care professionals in Australia. Aust. Fam. Physician. 2017, 46, 513–519. [Google Scholar] [PubMed]
- Wallace, J.; Hajarizadeh, B.; Richmond, J.; McNally, S.; Pitts, M. Managing chronic hepatitis B: The role of the GP. Aust. Fam. Physician. 2012, 41, 893–898. [Google Scholar] [PubMed]
- Sweeney, L.; Owiti, J.A.; Beharry, A.; Bhui, K.; Gomes, J.; Foster, G.R.; Greenhalgh, T. Informing the design of a national screening and treatment programme for chronic viral hepatitis in primary care: Qualitative study of at-risk immigrant communities and healthcare professionals. BMC Health Serv. Res. 2015, 15, 97. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, C.T.; Lin, S.Y. Hepatitis B screening in Asian and Pacific Islanders: New guidelines, old barriers. J. Immigr. Minor. Health 2015, 17, 1585–1587. [Google Scholar] [CrossRef]
- Kpozehouen, E.; Heywood, A.E.; Kay, M.; Smith, M.; Paudel, P.; Sheikh, M.; MacIntyre, C.R. Improving access to immunisation for migrants and refugees: Recommendations from a stakeholder workshop. Aust. N. Z. J. Public Health 2017, 41, 118–120. [Google Scholar] [CrossRef]
- Yau, A.H.L.; Ford, J.; Kwan, P.W.C.; Chan, J.; Choo, Q.; Lee, T.K.; Kwong, W.; Huang, A.; Yoshida, E. Hepatitis B awareness and knowledge in Asian communities in British Columbia. Can. J. Gastroenterol. Hepatol. 2016, 2016, 4278724. [Google Scholar] [CrossRef]
- Vedio, A.; Liu, E.Z.H.; Lee, A.C.K.; Salway, S. Improving access to health care for chronic hepatitis B among migrant Chinese populations: A systematic mixed methods review of barriers and enablers. J. Viral. Hepat. 2017, 24, 526–540. [Google Scholar] [CrossRef]
- Australian Government Department of Health. Australian Immunisation Handbook: Vaccination for Migrants, Refugees and People Seeking Asylum in Australia; Commonwealth of Australia: Canberra, Australia, 2018.
- Kärki, T.; Napoli, C.; Riccardo, F.; Fabiani, M.; Grazia Dente, M.; Carballo, M.; Noori, T.; Declich, S. Screening for infectious diseases among newly arrived migrants in EU/EEA countries—Varying practices but consensus on the utility of screening. Int. J. Environ. Res. Public Health 2014, 11, 11004. [Google Scholar] [CrossRef]


{kind=link}
| Author and Publication Date | Title | Population | Sample Size (n) and Gender (Female/Male) | Location | Intervention | Intervention Type | Setting | Outcome Measures | Population Screened | HBV Prevalence | Linkage to Care | Monitoring |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ash et al. (2018) [31] | Hepatitis B contact tracing: what works? | Refugees from high-prevalence countries | 122 (41% female, 59% male) | Australia | Auditing of clinical records and contact tracing (CT) | Individual | Primary care | Proportion of contacts traced and serologically confirmed as infected, immune, or susceptible to HBV, enablers of CT success | N/A | N/A | 6.4% of total participants in the intervention | N/A |
| Chandrasekar et al. (2016) [32] | A novel strategy to increase identification of African-born people with chronic hepatitis B virus infection in the Chicago metropolitan area, 2012–2014 | African-born persons | 1000 (51% female, 49% male of 445 screened) | US | Education and chain-referral sampling by community health workers | Community | Community (church groups) and primary care | HBV testing uptake and linkage to care uptake | 45.0% | 8.0% | N/A | N/A |
| Chandrasekar et al. (2015) [33] | A comparison of the effectiveness of hepatitis B screening and linkage to care among foreign-born populations in clinical and non-clinical settings | Foreign-born Asian Americans | 758 (62% female, 38% male) | US | Educational and outreach intervention using bilingual community health workers | Individual | Community (health fairs organised by churches and social services) and primary care | HBV screening uptake and linkage to care uptake | N/A | 7.3% | 55.0% (clinical), 77.0% (non-clinical) | N/A |
| Crawshaw et al. (2018) [34] | Infectious disease testing of UK-bound refugees: A population-based, cross-sectional study | Foreign-born refugees | 18,418 (48.8% female, 51.2% male) | UK | Pre-entry health assessment | Structural | Clinical health service | HBV screening | N/A | 2.0% | N/A | N/A |
| Dang et al. (2016) [35] | Increasing hepatitis B testing and linkage to care of foreign-born Asians, Sacramento, California, 2012–2013 | Foreign-born Chinese, Hmong, Korean, and Vietnamese | 1004 (62.7% female, 37.7% male) | US | Outreach testing | Individual | Community (student-run medical clinics, heritage associations, and churches) | HBV screening uptake | N/A | 7.6% | 67.1% | N/A |
| Flanagan et al. (2019) [36] | Case finding and therapy for chronic viral hepatitis in primary care (HepFREE): A cluster: randomised controlled trial | Migrants from high-risk countries | 90,250 (52% female, 48% male) | UK | Incentivising GPs | Individual | Primary care (general practices) | HBV screening uptake | 19.5% (intervention group) | 1.1% | >80.0% of HBsAg-positive participants | N/A |
| Hargreaves et al. (2020) [37] | Delivering multi-disease screening to migrants for latent TB and blood-borne T viruses in an emergency department setting: A feasibility study | Foreign-born economic migrants, asylum seekers, and refugees | 96 (48% female, 52% male) | UK | Opportunistic screening | Individual | Other clinical health service-based (emergency department) | HBV screening uptake | N/A | 2.0% | N/A | N/A |
| Hsu et al. (2013) [38] | Electronic messages increase hepatitis B screening in at-risk Asian American patients: A randomized, controlled trial | Chinese and Vietnamese patients | 175 (61.4% female, 38.6% male in intervention group) | US | Electronic health record (EHR) prompts | Individual | Primary care | Ordering of HBV tests and linkage to care uptake | 40.9% | 13.3% | 50.0% of HBsAg+ (referred to specialists), 25.0% of susceptible vaccinated for HBV | Monitored HBsAg-positive or HBV-non-immune for three months post-intervention |
| Kelly et al. (2020) [39] | Improving uptake of hepatitis B and hepatitis C testing in South Asian migrants in community and faith settings using educational interventions—A prospective descriptive study | South Asian migrants | 219 (53% female, 47% male) | UK | Educational film | Community | Community, religious centres, and primary care | CVH testing uptake | 84.0% | 0.9% | N/A | N/A |
| Navarro et al. (2014) [40] | Lower than expected hepatitis B virus infection prevalence among first-generation Koreans in the US: Results of HBV screening in the Southern Californian Empire | First-generation Koreans | 1007 (60.5% female, 39.5% male) | US | Educational and outreach intervention led by a bilingual nurse | Individual | Community (churches) | HBV screening uptake and linkage to care uptake | N/A | 3.0% | 27.5% | N/A |
| Perumalswami et al. (2013) [41] | Hepatitis Outreach Network: A practical strategy for hepatitis screening with linkage to care in foreign-born communities | Foreign-born from countries with a high prevalence of CVH | 1603 (50.6% female, 49.4% male) | US | Educational and outreach intervention | Individual | Community (public schools, places of worship, YMCAs, public parks, hotels, business centres, and train stations) | HBV and HCV screening and linkage to care uptake | N/A | 4.7% | 57.0% | N/A |
| Raines-Milenkov et al. (2021) [42] | Hepatitis B virus awareness, infection, and screening multiethnic community intervention for foreign-born populations | Refugee immigrant population | 1069 (80% female, 20% male) | US | Educational and outreach intervention by bicultural community health workers | Individual | Community (churches, mosques, civic groups) and primary care | HBV screening uptake | 38.0% | 6.0% | N/A | N/A |
| Shankar et al. (2016) [43] | A novel collaborative community-based hepatitis B screening and linkage to care program for African immigrants | African-born persons | 955 (24.5% female, 75.5% male) | US | Outreach testing and linkage to care with a culturally targeted patient navigator | Individual | Community (community centres, places of worship, and sites of employment) | HBV screening and linkage to care uptake | N/A | 9.6% | 97.0% | N/A |
| Standford et al. (2016) [44] | Community-engaged strategies to promote hepatitis B testing and linkage to care in immigrants of Florida | Foreign-born nationals | 1516 (50.4% female, 49.6% male) | US | Educational and outreach intervention by community health workers and certified medical assistants | Individual | Community (faith-based organisations, refugee servicing organisations), primary care, and the emergency department | HBV screening uptake and linkage to care uptake | N/A | 4.4% | 63.0% | N/A |
| Vedio et al. (2013) [45] | Hepatitis B: Report of prevalence and access to healthcare among Chinese residents in Sheffield, UK | Chinese residents | 229 (57.5 female, 42.5% male) | UK | Educational and outreach intervention | Individual | Community (Kinhon Chinese Centre) | HBV screening uptake and participant feedback | N/A | 8.7% | N/A | N/A |
| Xiao et al. (2021) [46] | Assessing the feasibility, acceptability and impacts of an education program on hepatitis B testing uptake among ethnic Chinese in Australia: results of a randomised controlled pilot study | Individuals of Chinese ethnicity | 54 (69% female, 31% male) | Australia | Educational and outreach intervention | Individual | Community-based organisations | HBV testing uptake, intervention acceptability, and feasibility of the study | 12% | N/A | N/A | N/A |
| Zibrik et al. (2018) [47] | Let’s Talk About B: Barriers to hepatitis B screening and vaccination among Asian and South Asian immigrants in British Columbia | Korean, Chinese, Filipino, and South Asian immigrants | 827 (70% female, 30% male) | Canada | Culturally tailored education workshops | Community | Community (community centres, immigration settlement service centres, organised health events, and religious/cultural gathering places) | Self-reported action related to HBV prevention and management | 19.0% | N/A | 1.0% | Participant feedback was obtained two weeks and one month post-intervention |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajkumar, V.; McCausland, K.; Lobo, R. A Rapid Review of Interventions to Increase Hepatitis B Testing, Treatment, and Monitoring among Migrants Living in Australia. Int. J. Environ. Res. Public Health 2022, 19, 5947. https://doi.org/10.3390/ijerph19105947
Rajkumar V, McCausland K, Lobo R. A Rapid Review of Interventions to Increase Hepatitis B Testing, Treatment, and Monitoring among Migrants Living in Australia. International Journal of Environmental Research and Public Health. 2022; 19(10):5947. https://doi.org/10.3390/ijerph19105947
Chicago/Turabian StyleRajkumar, Vishnupriya, Kahlia McCausland, and Roanna Lobo. 2022. "A Rapid Review of Interventions to Increase Hepatitis B Testing, Treatment, and Monitoring among Migrants Living in Australia" International Journal of Environmental Research and Public Health 19, no. 10: 5947. https://doi.org/10.3390/ijerph19105947
APA StyleRajkumar, V., McCausland, K., & Lobo, R. (2022). A Rapid Review of Interventions to Increase Hepatitis B Testing, Treatment, and Monitoring among Migrants Living in Australia. International Journal of Environmental Research and Public Health, 19(10), 5947. https://doi.org/10.3390/ijerph19105947