
Relationships between Expenditure of Regional Governments and Suicide Mortalities Caused by Six Major Motives in Japan


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Dependent Variables
2.2. Independent Variables
2.3. Statistical Analysis
3. Results
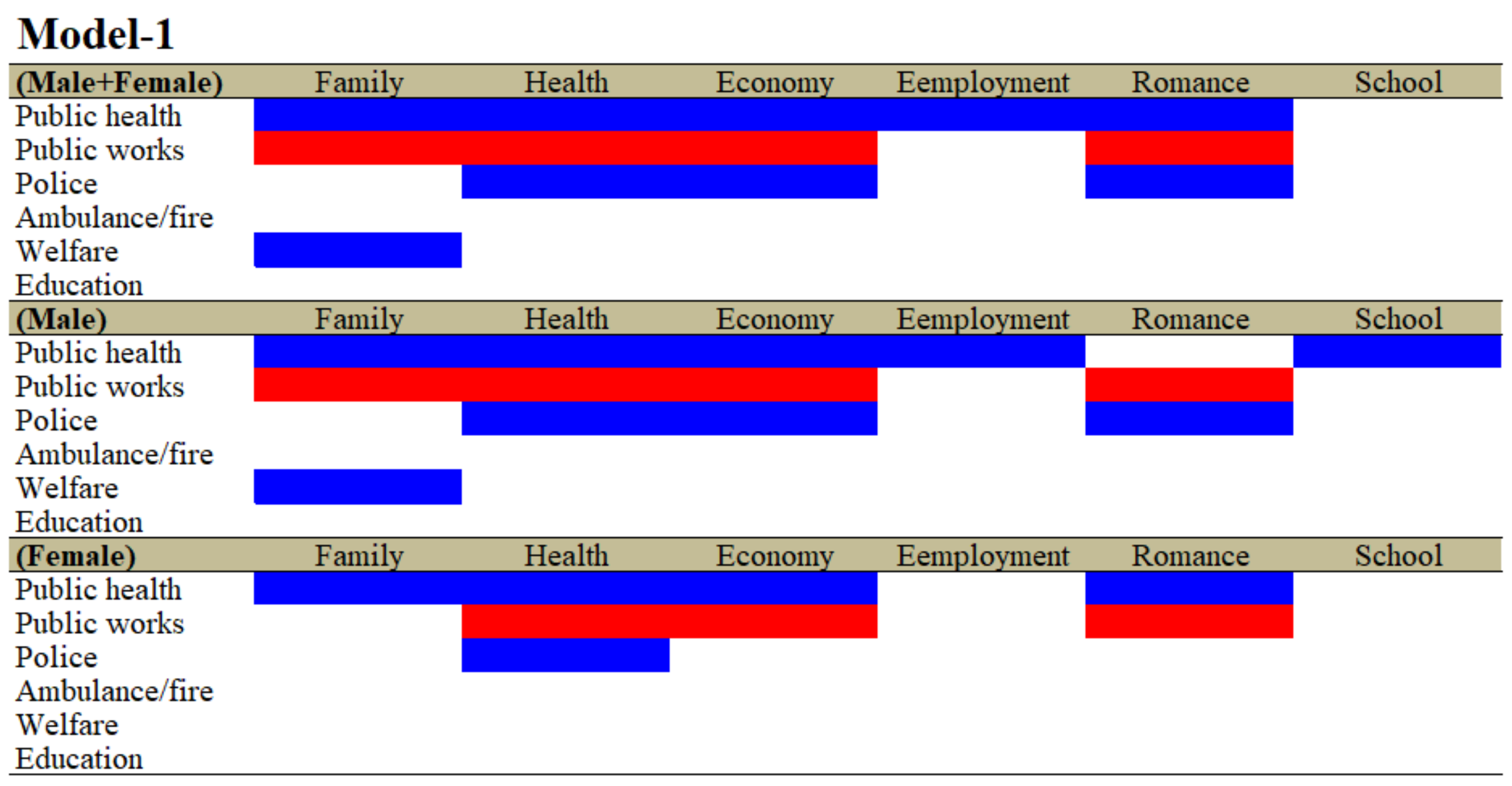
3.1. Relationship between Total Amount of Regional Financial Expenditure of Six Divisions and Suicide Mortalities Caused by Six Major Motives (Model-1)
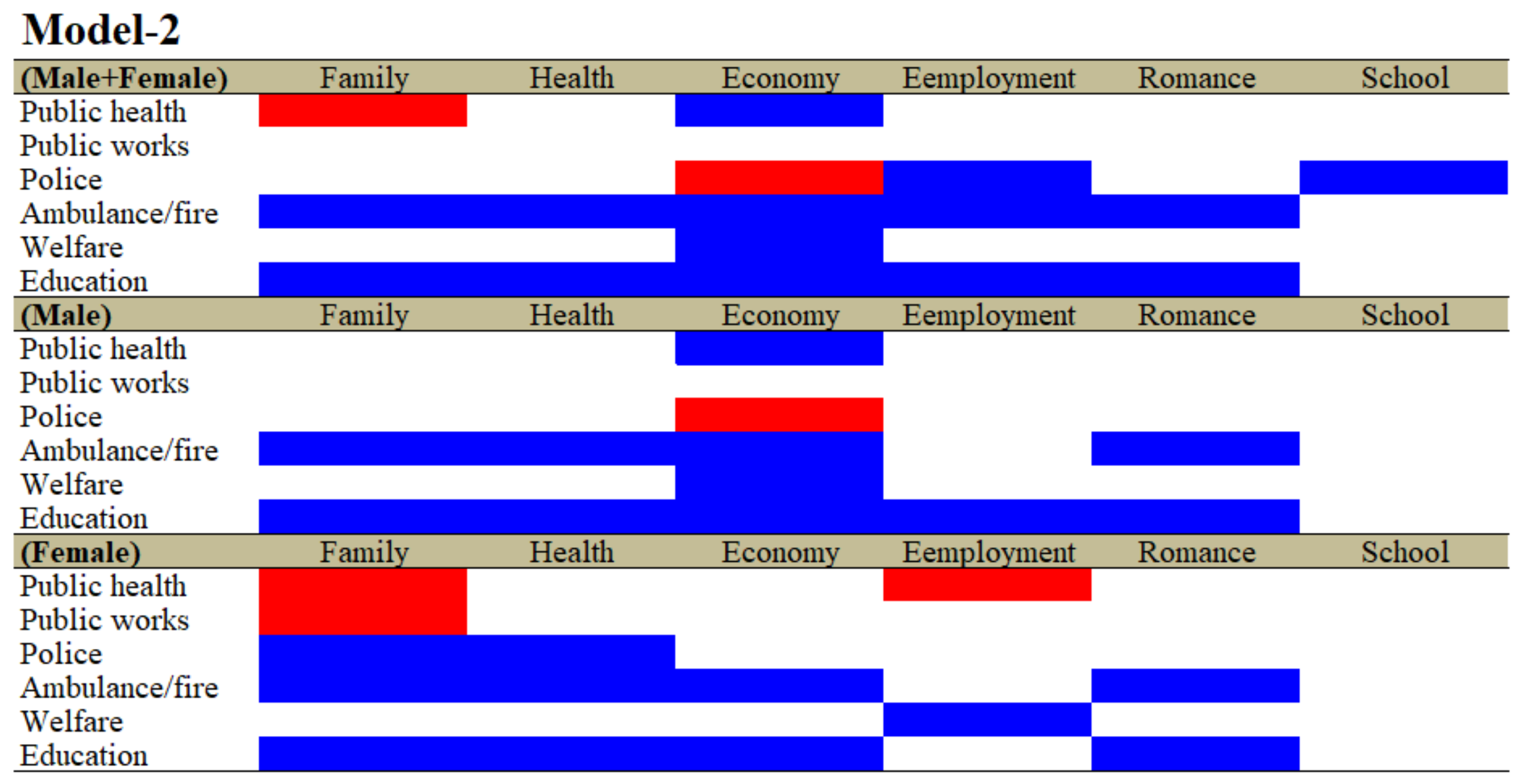
3.2. Relationship between Regional Financial Expenditure Per Capita of Six Divisions and Suicide Mortalities Caused by Six Major Motives (Model-2)
3.3. Relationship between Financial Expenditure Per Capita of Divisions and Subdivision of Education and Suicide Mortalities Caused by Motives (Model-3)
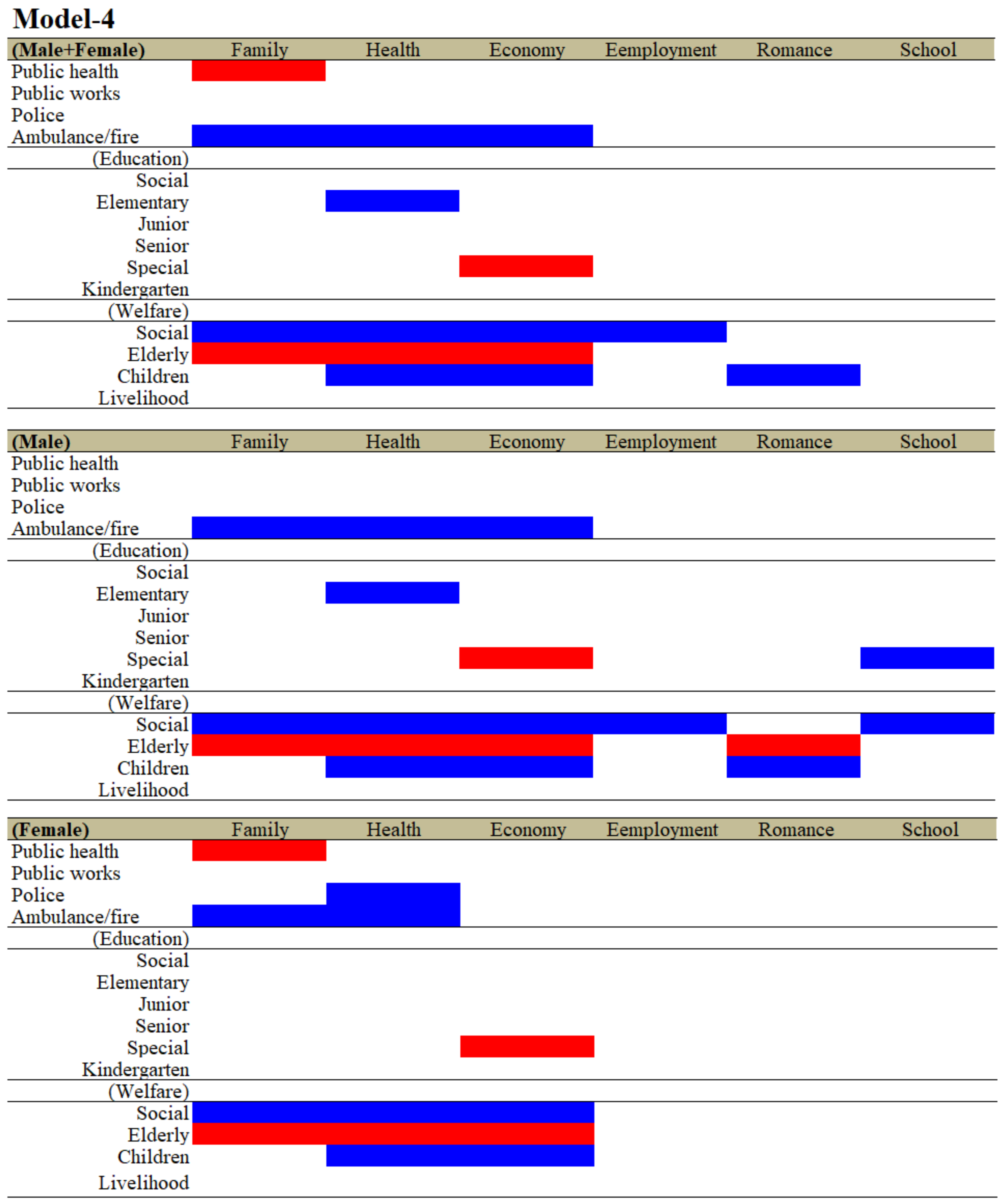
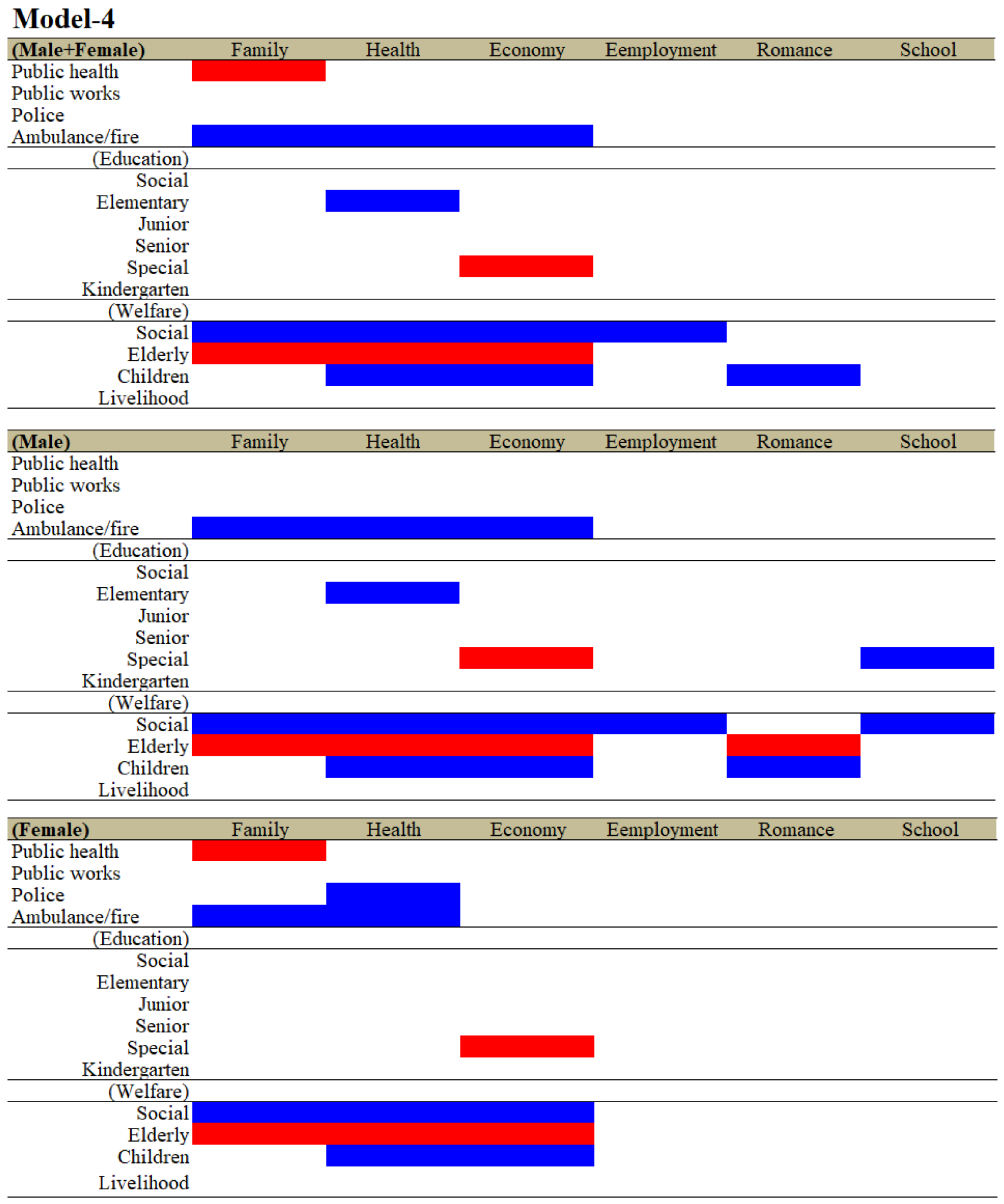
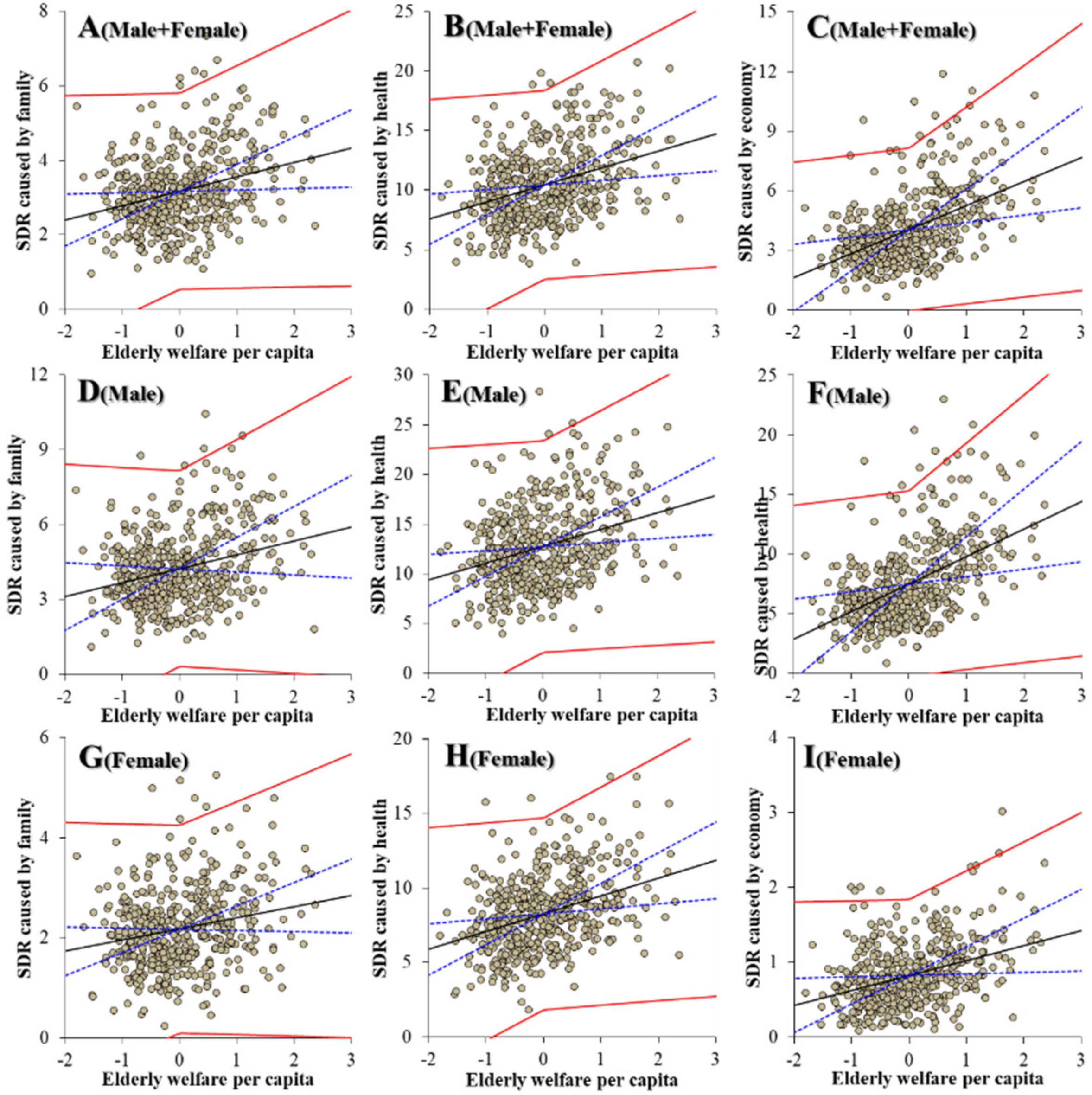
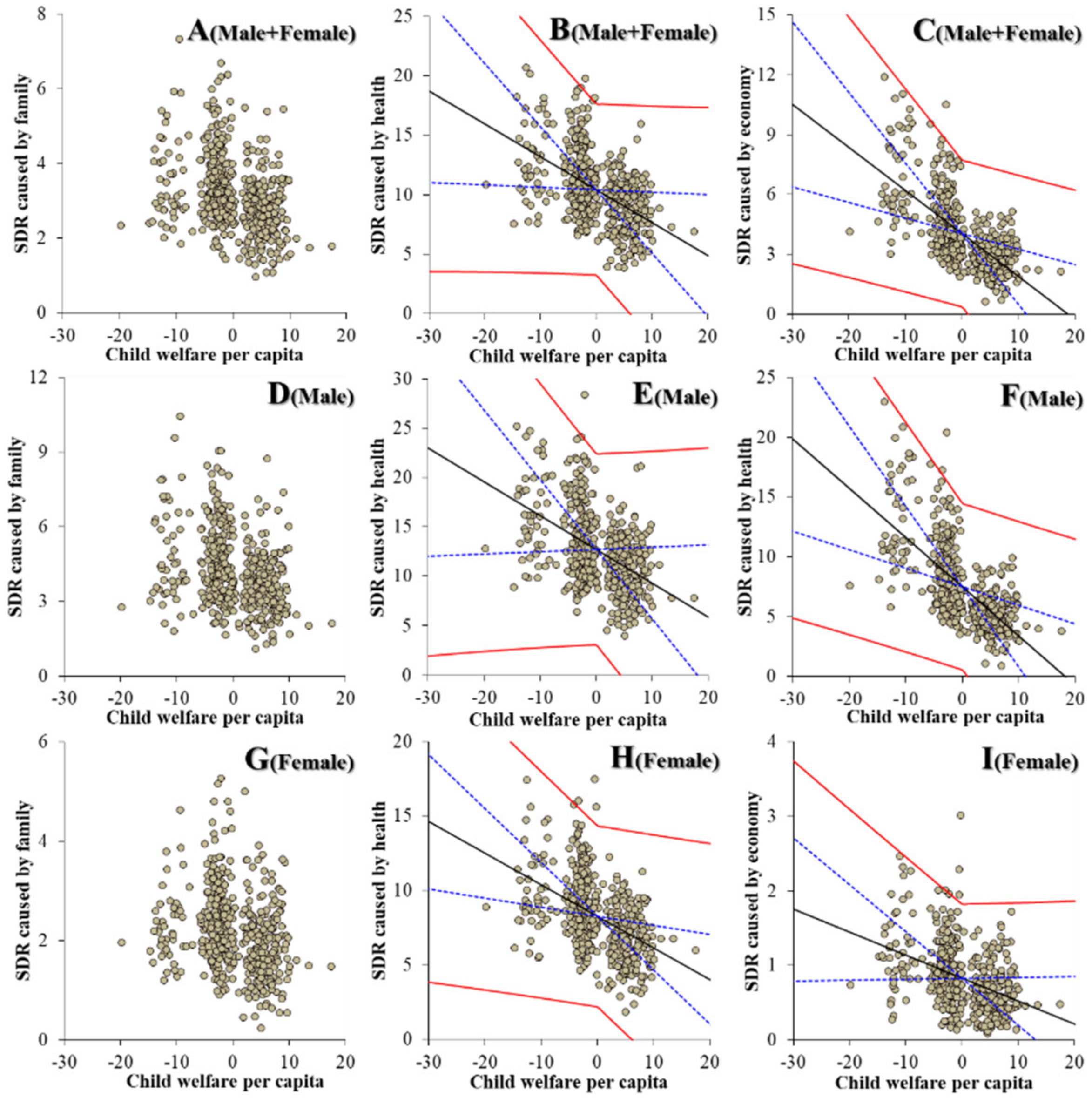
3.4. Relationship between Financial Expenditure Per Capita of Divisions and Subdivisions of Education and Welfare, and Suicide Mortalities Caused by Motives (Model-4)
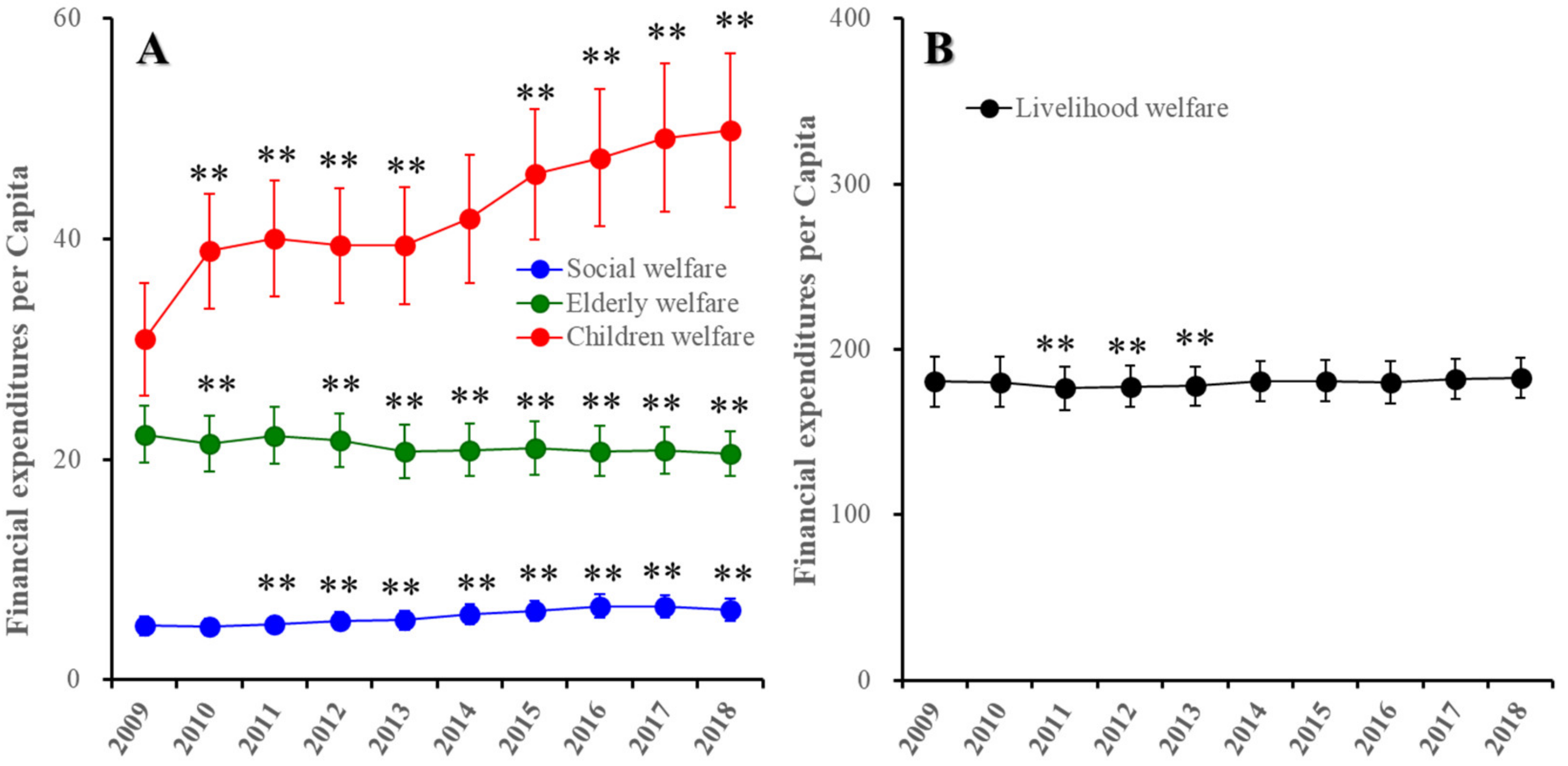
3.5. Trends of Regional Financial Expenditure of Welfare Subdivision in Japan between 2009 and 2018
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Suicide Data. Available online: https://www.who.int/mental_health/prevention/suicide/countrydata/en/ (accessed on 1 December 2019).
- World Health Organization. Suicide: One Person Dies Every 40 Seconds. Available online: https://www.who.int/news/item/09-09-2019-suicide-one-person-dies-every-40-seconds (accessed on 18 November 2020).
- World Health Organization. Preventing Suicide: A Resource for Pesticide Registrars and Regulators. Available online: https://www.who.int/publications/i/item/9789241516389 (accessed on 18 November 2020).
- World Health Organization. Preventing Suicide: A Global Imperative. Available online: https://www.who.int/publications/i/item/preventing-suicide-a-global-imperative (accessed on 18 November 2020).
- World Health Organization. Preventing Suicide: A Resource for Filmmakers and Others Working on Stage and Screen. Available online: https://www.who.int/publications/i/item/preventing-suicide-a-resource-for-filmmakers-and-others-working-on-stage-and-screen (accessed on 18 November 2020).
- Kino, S.; Jang, S.-N.; Gero, K.; Kato, S.; Kawachi, I. Age, period, cohort trends of suicide in Japan and Korea (1986–2015): A tale of two countries. Soc. Sci. Med. 2019, 235, 112385. [Google Scholar] [CrossRef]
- Kato, R.; Okada, M. Can Financial Support Reduce Suicide Mortality Rates? Int. J. Environ. Res. Public Health 2019, 16, 4797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health. 2020 White Paper on Suicide Prevention. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/jisatsuhakusyo2020.html (accessed on 1 June 2021).
- Ministry of Health. Basic Data on Suicide in The Region. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000140901.html (accessed on 1 June 2021).
- Chen, Y.-Y.; Wu, K.C.-C.; Yousuf, S.; Yip, P.S.F. Suicide in Asia: Opportunities and Challenges. Epidemiol. Rev. 2011, 34, 129–144. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Kim, M.-H.; Kawachi, I.; Cho, Y. Comparative Epidemiology of Suicide in South Korea and Japan: Effects of Age, Gender and Suicide Methods. Crisis 2011, 32, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Dhungel, B.; Sugai, M.K.; Gilmour, S. Trends in Suicide Mortality by Method from 1979 to 2016 in Japan. Int. J. Environ. Res. Public Health 2019, 16, 1794. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.-S.; Gunnell, D.; Sterne, J.A.; Lu, T.-H.; Cheng, A.T. Was the economic crisis 1997–1998 responsible for rising suicide rates in East/Southeast Asia? A time–trend analysis for Japan, Hong Kong, South Korea, Taiwan, Singapore and Thailand. Soc. Sci. Med. 2009, 68, 1322–1331. [Google Scholar] [CrossRef]
- Yoshikawa, H. Japan’s lost decade: What have we learned and where are we heading? Asian Econ. Policy Rev. 2007, 2, 186–203. [Google Scholar] [CrossRef]
- Nakamoto, M.; Nakagawa, T.; Murata, M.; Okada, M. Impacts of Dual-Income Household Rate on Suicide Mortalities in Japan. Int. J. Environ. Res. Public Health 2021, 18, 5670. [Google Scholar] [CrossRef]
- Okada, M.; Hasegawa, T.; Kato, R.; Shiroyama, T. Analysing regional unemployment rates, GDP per capita and financial support for regional suicide prevention programme on suicide mortality in Japan using governmental statistical data. BMJ Open 2020, 10, e037537. [Google Scholar] [CrossRef]
- Barr, B.; Kinderman, P.; Whitehead, M. Trends in mental health inequalities in England during a period of recession, austerity and welfare reform 2004 to 2013. Soc. Sci. Med. 2015, 147, 324–331. [Google Scholar] [CrossRef]
- Barr, B.; Taylor-Robinson, D.; Scott-Samuel, A.; McKee, M.; Stuckler, D. Suicides associated with the 2008-10 economic recession in England: Time trend analysis. BMJ 2012, 345, e5142. [Google Scholar] [CrossRef] [Green Version]
- Rambotti, S. Is there a relationship between welfare-state policies and suicide rates? Evidence from the U.S. states, 2000–2015. Soc. Sci. Med. 2020, 246, 112778. [Google Scholar] [CrossRef] [Green Version]
- Reeves, A.; Basu, S.; McKee, M.; Marmot, M.; Stuckler, D. Austere or not? UK coalition government budgets and health inequalities. J. R. Soc. Med. 2013, 106, 432–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor-Robinson, D.; Whitehead, M.; Barr, B. Great leap backwards. BMJ 2014, 349, g7350. [Google Scholar] [CrossRef] [Green Version]
- Antonakakis, N.; Collins, A. The impact of fiscal austerity on suicide: On the empirics of a modern Greek tragedy. Soc. Sci. Med. 2014, 112, 39–50. [Google Scholar] [CrossRef] [Green Version]
- Antonakakis, N.; Collins, A. The impact of fiscal austerity on suicide mortality: Evidence across the ‘Eurozone periphery’. Soc. Sci. Med. 2015, 145, 63–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Branas, C.C.; Kastanaki, A.E.; Michalodimitrakis, M.; Tzougas, J.; Kranioti, E.F.; Theodorakis, P.N.; Carr, B.G.; Wiebe, D.J. The impact of economic austerity and prosperity events on suicide in Greece: A 30-year interrupted time-series analysis. BMJ Open 2015, 5, e005619. [Google Scholar] [CrossRef] [Green Version]
- Karanikolos, M.; Mladovsky, P.; Cylus, J.; Thomson, S.; Basu, S.; Stuckler, D.; Mackenbach, J.P.; McKee, M. Financial crisis, austerity, and health in Europe. Lancet 2013, 381, 1323–1331. [Google Scholar] [CrossRef]
- Rachiotis, G.; Stuckler, D.; McKee, M.; Hadjichristodoulou, C. What has happened to suicides during the Greek economic crisis? Findings from an ecological study of suicides and their determinants (2003–2012). BMJ Open 2015, 5, e007295. [Google Scholar] [CrossRef] [Green Version]
- Simou, E.; Koutsogeorgou, E. Effects of the economic crisis on health and healthcare in Greece in the literature from 2009 to 2013: A systematic review. Health Policy 2014, 115, 111–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granados, J.A.T.; Rodriguez, J.M. Health, economic crisis, and austerity: A comparison of Greece, Finland and Iceland. Health Policy 2015, 119, 941–953. [Google Scholar] [CrossRef]
- Toffolutti, V.; Suhrcke, M. Does austerity really kill? Econ. Hum. Biol. 2019, 33, 211–223. [Google Scholar] [CrossRef]
- Konieczna, A.; Jakobsen, S.G.; Larsen, C.P.; Christiansen, E. Recession and risk of suicide in Denmark during the 2009 global financial crisis: An ecological register-based study. Scand. J. Public Health 2021, 14034948211013270. [Google Scholar] [CrossRef]
- Ministry of Health. Grant for Enhance Community-Based Suicide Countermeasures. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/tiikijisatsutaisakukyokazigyo.html (accessed on 1 June 2021).
- Ministry of Health. Regional Suicide Countermeasures Emergency Enhancement Fund. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/kyoukakikin.html (accessed on 18 November 2021).
- Ministry of Health. National Plan for Prevention of Suicide. Available online: https://www.mhlw.go.jp/kokoro/nation/about.html (accessed on 18 November 2021).
- Nakano, T.; Hasegawa, T.; Okada, M. Analysing the Impacts of Financial Support for Regional Suicide Prevention Programmes on Suicide Mortality Caused by Major Suicide Motives in Japan Using Statistical Government Data. Int. J. Environ. Res. Public Health 2021, 18, 3414. [Google Scholar] [CrossRef] [PubMed]
- Shiroyama, T.; Fukuyama, K.; Okada, M. Effects of Financial Expenditure of Prefectures/Municipalities on Regional Suicide Mortality in Japan. Int. J. Environ. Res. Public Health 2021, 18, 8639. [Google Scholar] [CrossRef] [PubMed]
- You, B.-S.; Jeong, K.-H.; Cho, H.J. Regional Suicide Rate Change Patterns in Korea. Int. J. Environ. Res. Public Health 2020, 17, 6973. [Google Scholar] [CrossRef]
- Reeves, A.; McKee, M.; Stuckler, D. Economic suicides in the Great Recession in Europe and North America. Br. J. Psychiatry 2014, 205, 246–247. [Google Scholar] [CrossRef] [Green Version]
- Mattei, G.; Pistoresi, B. Unemployment and suicide in Italy: Evidence of a long-run association mitigated by public unemployment spending. Eur. J. Health Econ. 2019, 20, 569–577. [Google Scholar] [CrossRef]
- Mattei, G.; Pistoresi, B.; De Vogli, R. Impact of the economic crises on suicide in Italy: The moderating role of active labor market programs. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 54, 201–208. [Google Scholar] [CrossRef]
- Robinson, R.J.; Palka, J.M.; Brown, E.S. The Relationship Between State Mental Health Agency and Medicaid Spending with Outcomes. Community Ment. Health J. 2021, 57, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Swain, P.K.; Tripathy, M.R.; Priyadarshini, S.; Acharya, S.K. Forecasting suicide rates in India: An empirical exposition. PLoS ONE 2021, 16, e0255342. [Google Scholar] [CrossRef]
- Hasegawa, T.; Matsumoto, R.; Yamamoto, Y.; Okada, M. Analysing effects of financial support for regional suicide prevention programmes on methods of suicide completion in japan between 2009 and 2018 using governmental statistical data. BMJ Open 2021, 11. e049538. [Google Scholar] [PubMed]
- GEBC Studio Production. The Fifth Basic Plan for Gender Equality. Available online: https://www.gender.go.jp/english_contents/about_danjo/whitepaper/pdf/5th_bpg.pdf (accessed on 1 May 2021).
- Service Provider Providing Global Communications Solutions. Surveys of Population, Population Change and The Number of Households Based on the Basic Resident Registration. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&toukei=00200241&tstat=000001039591 (accessed on 1 May 2021).
- Kawaguchi, H.; Koike, S. Association between the Density of Physicians and Suicide Rates in Japan: Nationwide Ecological Study Using a Spatial Bayesian Model. PLoS ONE 2016, 11, e0148288. [Google Scholar] [CrossRef] [PubMed]
- MIC. White Paper on Local Public Finance. Available online: https://www.soumu.go.jp/menu_seisaku/hakusyo/chihou/r03data/index.html (accessed on 1 May 2021).
- e-Stat Is A Portal Site for Japanese Government Statistics. Survey on Local Public Finance. Available online: https://www.e-stat.go.jp/en/statistics/00200251 (accessed on 1 May 2021).
- Grumbach, J.M. From Backwaters to Major Policymakers: Policy Polarization in the States, 1970–2014. Perspect. Politics 2018, 16, 416–435. [Google Scholar] [CrossRef] [Green Version]
- Enns, P.K.; Kelly, N.J.; Masaki, T.; Wohlfarth, P.C. Don’t jettison the general error correction model just yet: A practical guide to avoiding spurious regression with the GECM. Res. Politics 2016, 3, 3. [Google Scholar] [CrossRef]
- Hoechle, D. Robust Standard Errors for Panel Regressions with Cross-Sectional Dependence. Stata J. Promot. Commun. Stat. Stata 2007, 7, 281–312. [Google Scholar] [CrossRef] [Green Version]
- Nakano, T.; Hasegawa, T.; Suzuki, D.; Motomura, E.; Okada, M. Amantadine Combines Astroglial System Xc− Activation with Glutamate/NMDA Receptor Inhibition. Biomolecules 2019, 9, 191. [Google Scholar] [CrossRef] [Green Version]
- Okada, M.; Fukuyama, K.; Kawano, Y.; Shiroyama, T.; Ueda, Y. Memantine protects thalamocortical hyper-glutamatergic transmission induced by nmda receptor antagonism via activation of system xc. Pharmacol. Res. Perspect. 2019, 7, e00457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okada, M.; Fukuyama, K.; Nakano, T.; Ueda, Y. Pharmacological Discrimination of Effects of MK801 on Thalamocortical, Mesothalamic, and Mesocortical Transmissions. Biomolecules 2019, 9, 746. [Google Scholar] [CrossRef] [Green Version]
- Fukuyama, K.; Okada, M. Age-Dependent and Sleep/Seizure-Induced Pathomechanisms of Autosomal Dominant Sleep-Related Hypermotor Epilepsy. Int. J. Mol. Sci. 2020, 21, 8142. [Google Scholar] [CrossRef] [PubMed]
- Fukuyama, K.; Fukuzawa, M.; Shiroyama, T.; Okada, M. Pathomechanism of nocturnal paroxysmal dystonia in autosomal dominant sleep-related hypermotor epilepsy with S284L-mutant α4 subunit of nicotinic ACh receptor. Biomed. Pharmacother. 2020, 126, 110070. [Google Scholar] [CrossRef]
- Japanese Public Fibance Fact Sheet. Available online: https://www.mof.go.jp/english/policy/budget/budget/fy2020/04.pdf (accessed on 1 June 2021).
- Matsubayashi, T.; Sekijima, K.; Ueda, M. Government spending, recession, and suicide: Evidence from Japan. BMC Public Health 2020, 20, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fishback, P.V.; Haines, M.R.; Kantor, S. Births, Deaths, and New Deal Relief during the Great Depression. Rev. Econ. Stat. 2007, 89, 1–14. [Google Scholar] [CrossRef]
- Knipe, D.W.; Chang, S.S.; Dawson, A.; Eddleston, M.; Konradsen, F.; Metcalfe, C.; Gunnell, D. Suicide prevention through means restriction: Impact of the 2008-2011 pesticide restrictions on suicide in sri lanka. PLoS ONE 2017, 12, e0172893. [Google Scholar]
- Baumbach, A.; Gulis, G. Impact of financial crisis on selected health outcomes in Europe. Eur. J. Public Health 2014, 24, 399–403. [Google Scholar] [CrossRef]
- Stuckler, D.; Basu, S.; Suhrcke, M.; Coutts, A.; McKee, M. The public health effect of economic crises and alternative policy responses in Europe: An empirical analysis. Lancet 2009, 374, 315–323. [Google Scholar] [CrossRef]
- Toffolutti, V.; Suhrcke, M. Assessing the short term health impact of the Great Recession in the European Union: A cross-country panel analysis. Prev. Med. 2014, 64, 54–62. [Google Scholar] [CrossRef]
- Cabinet Office. 2012 Declining Birthrate White Paper. Available online: https://www8.cao.go.jp/shoushi/shoushika/whitepaper/measures/english/w-2012/index.html (accessed on 1 May 2021).
- Cabinet Office. Outline of Measures for Society with Decreasing Birthrate. Available online: https://www8.cao.go.jp/shoushi/shoushika/law/taikou2.html (accessed on 1 May 2021).
- Cabinet Office. Annual Report on the Ageing Society 2020. Available online: https://www8.cao.go.jp/kourei/english/annualreport/2019/pdf/2019.pdf (accessed on 1 May 2021).
- e-Stat Is A Portal Site for Japanese Government Statistics. Family Income and Expenditure Survey. Available online: https://www.e-stat.go.jp/en/stat-search/files?page=1&layout=normal&toukei=00200561 (accessed on 1 May 2021).



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hasegawa, T.; Fukuyama, K.; Okada, M. Relationships between Expenditure of Regional Governments and Suicide Mortalities Caused by Six Major Motives in Japan. Int. J. Environ. Res. Public Health 2022, 19, 84. https://doi.org/10.3390/ijerph19010084
Hasegawa T, Fukuyama K, Okada M. Relationships between Expenditure of Regional Governments and Suicide Mortalities Caused by Six Major Motives in Japan. International Journal of Environmental Research and Public Health. 2022; 19(1):84. https://doi.org/10.3390/ijerph19010084
Chicago/Turabian StyleHasegawa, Toshiki, Kouji Fukuyama, and Motohiro Okada. 2022. "Relationships between Expenditure of Regional Governments and Suicide Mortalities Caused by Six Major Motives in Japan" International Journal of Environmental Research and Public Health 19, no. 1: 84. https://doi.org/10.3390/ijerph19010084
APA StyleHasegawa, T., Fukuyama, K., & Okada, M. (2022). Relationships between Expenditure of Regional Governments and Suicide Mortalities Caused by Six Major Motives in Japan. International Journal of Environmental Research and Public Health, 19(1), 84. https://doi.org/10.3390/ijerph19010084