
Risk of Glaucoma Associated with Components of Metabolic Disease in Taiwan: A Nationwide Population-Based Study



Abstract
1. Introduction
2. Study Population and Methods
2.1. Data Source
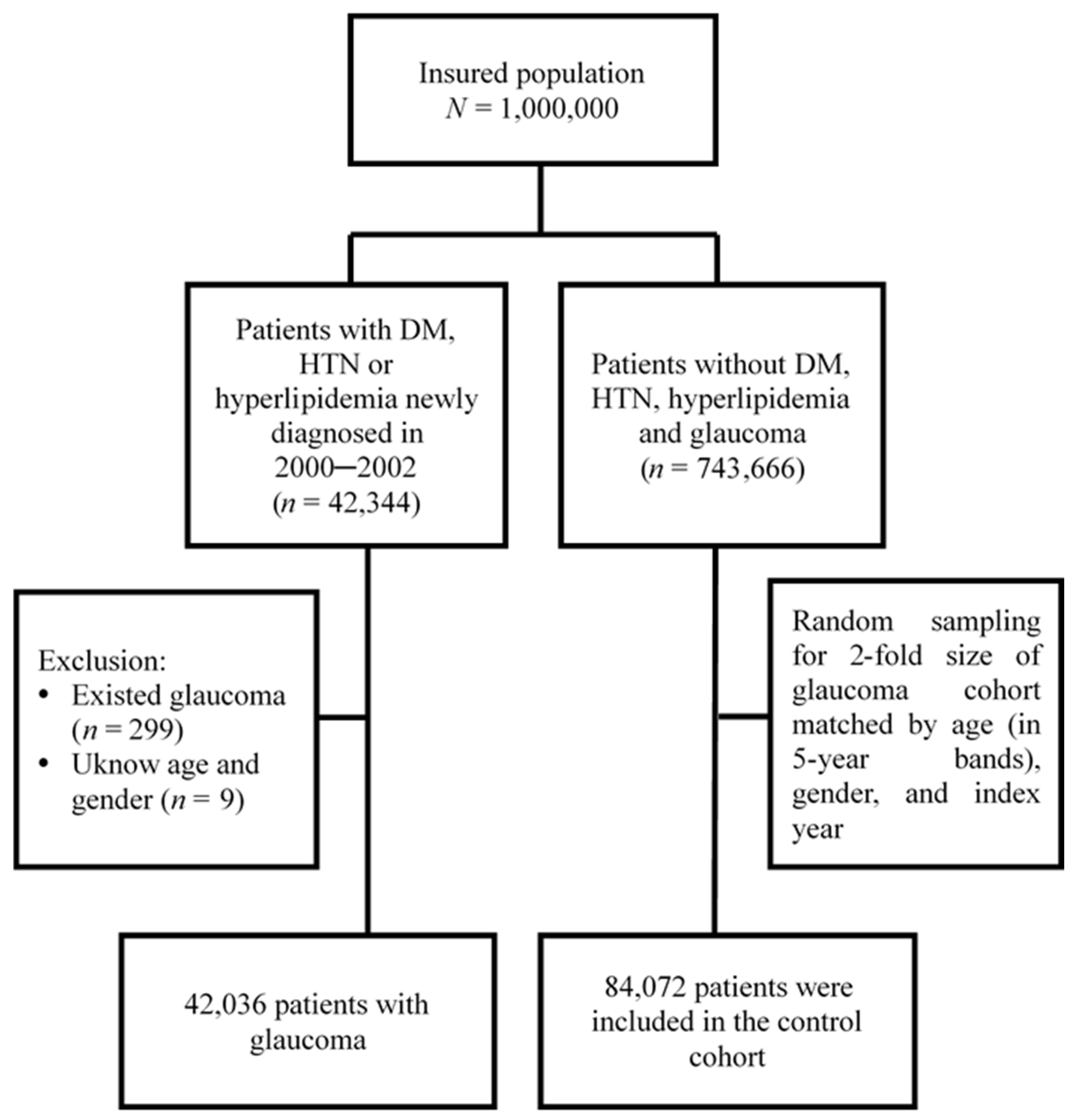
2.2. Study Cohorts Selection
2.3. Comorbidities and Drugs
2.4. Statistical Analysis
3. Results
3.1. Basic Characteristics of Study Cohorts
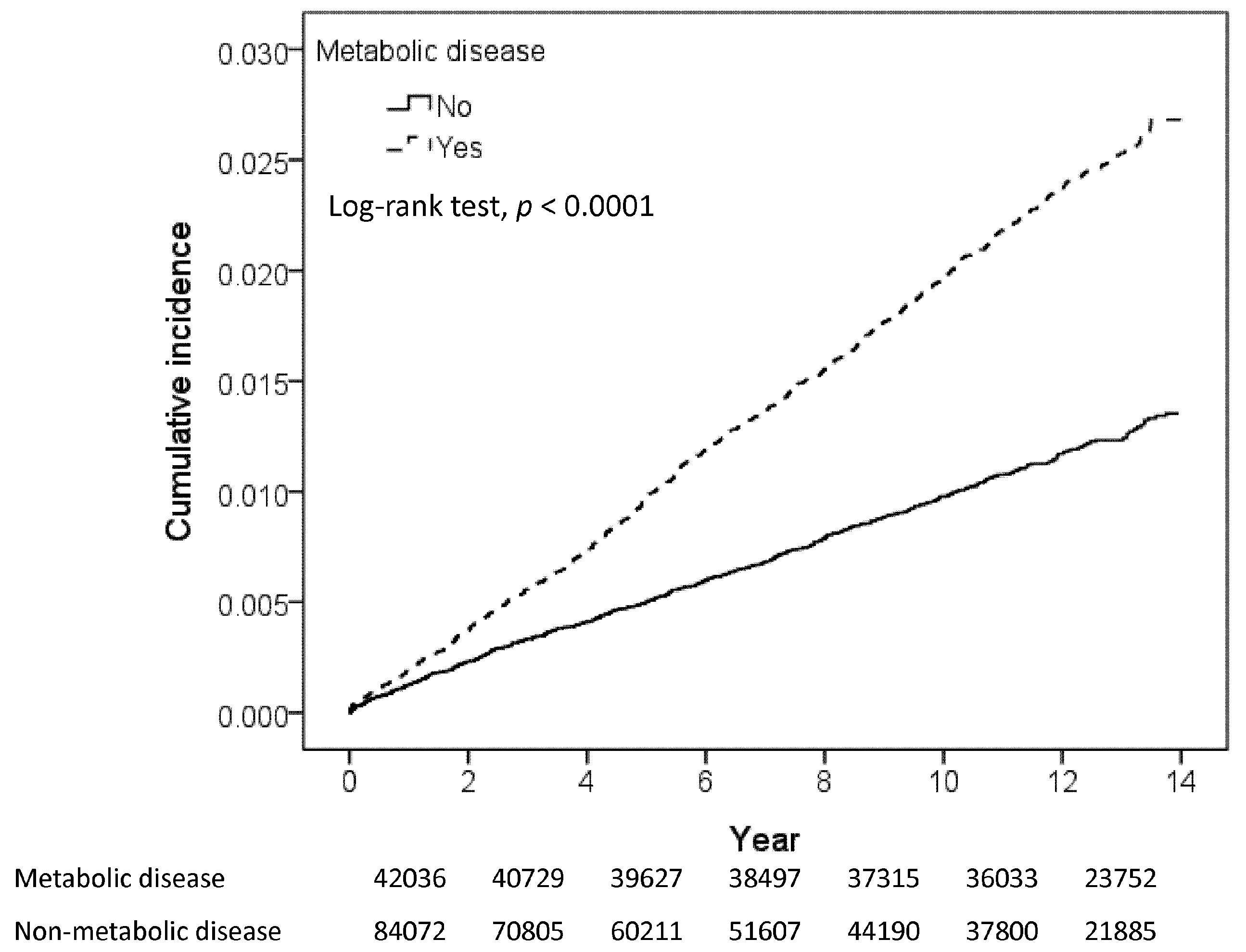
3.2. Association between Metabolic Disease and Glaucoma
4. Discussion
4.1. Components of Metabolic Disease and Glaucoma
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: The Right to Sight: An analysis for the Global Burden of Disease Study. Lancet Glob. Health 2021, 9, e144–e160. [CrossRef]
- Casson, R.J.; Chidlow, G.; Wood, J.P.; Crowston, J.G.; Goldberg, I. Definition of glaucoma: Clinical and experimental concepts. Clin. Exp. Ophthalmol. 2012, 40, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Cho, J.; Kim, M.H.; Friedman, D.S.; Guallar, E. Diabetes, fasting glucose, and the risk of glaucoma: A meta-analysis. Ophthalmology 2015, 122, 72–78. [Google Scholar] [CrossRef]
- Agrawal, A.; Singh, A.; Mittal, S.K. Glaucoma in Asia- An epidemiological perspective. Nepal. J. Ophthalmol. 2017, 9, 208–211. [Google Scholar] [CrossRef]
- Varma, R.; Lee, P.P.; Goldberg, I.; Kotak, S. An assessment of the health and economic burdens of glaucoma. Am. J. Ophthalmol. 2011, 152, 515–522. [Google Scholar] [CrossRef]
- Tham, Y.C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: A systematic review and meta-analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef]
- Bae, H.W.; Lee, N.; Lee, H.S.; Hong, S.; Seong, G.J.; Kim, C.Y. Systemic hypertension as a risk factor for open-angle glaucoma: A meta-analysis of population-based studies. PLoS ONE 2014, 9, e108226. [Google Scholar] [CrossRef]
- Gupta, D.; Chen, P.P. Glaucoma. Am. Fam. Physician 2016, 93, 668–674. [Google Scholar]
- Wright, C.; Tawfik, M.A.; Waisbourd, M.; Katz, L.J. Primary angle-closure glaucoma: An update. Acta Ophthalmol. 2016, 94, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Poh, S.; Mohamed Abdul, R.B.; Lamoureux, E.L.; Wong, T.Y.; Sabanayagam, C. Metabolic syndrome and eye diseases. Diabetes Res. Clin. Pr. 2016, 113, 86–100. [Google Scholar] [CrossRef]
- Alberti, K.G.; Zimmet, P.; Shaw, J. The metabolic syndrome--a new worldwide definition. Lancet 2005, 366, 1059–1062. [Google Scholar] [CrossRef]
- Belete, R.; Ataro, Z.; Abdu, A.; Sheleme, M. Global prevalence of metabolic syndrome among patients with type I diabetes mellitus: A systematic review and meta-analysis. Diabetol. Metab. Syndr. 2021, 13, 25. [Google Scholar] [CrossRef] [PubMed]
- Yin, X.; Li, J.; Zhang, B.; Lu, P. Association of glaucoma with risk of retinal vein occlusion: A meta-analysis. Acta Ophthalmol. 2019, 97, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.T.; Tsai, S.S.; Shih, T.S.; Lin, M.H.; Chou, T.C.; Ting, H.; Wu, T.N.; Liou, S.H. The Association between Obstructive Sleep Apnea and Metabolic Markers and Lipid Profiles. PLoS ONE 2015, 10, e0130279. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Touros, A.; Kim, W.R. Nonalcoholic Fatty Liver Disease and Metabolic Syndrome. Clin. Liver Dis. 2018, 22, 133–140. [Google Scholar] [CrossRef]
- Skilton, M.R.; Moulin, P.; Terra, J.L.; Bonnet, F. Associations between anxiety, depression, and the metabolic syndrome. Biol. Psychiatry 2007, 62, 1251–1257. [Google Scholar] [CrossRef] [PubMed]
- Tang, F.; Wang, G.; Lian, Y. Association between anxiety and metabolic syndrome: A systematic review and meta-analysis of epidemiological studies. Psychoneuroendocrinology 2017, 77, 112–121. [Google Scholar] [CrossRef]
- Uzunlulu, M.; Yorulmaz, E.; Oguz, A. Prevalence of subclinical hypothyroidism in patients with metabolic syndrome. Endocr. J. 2007, 54, 71–76. [Google Scholar] [CrossRef]
- Zhao, D.; Cho, J.; Kim, M.H.; Guallar, E. The association of blood pressure and primary open-angle glaucoma: A meta-analysis. Am. J. Ophthalmol. 2014, 158, 615–627.e9. [Google Scholar] [CrossRef]
- Newman-Casey, P.A.; Talwar, N.; Nan, B.; Musch, D.C.; Stein, J.D. The relationship between components of metabolic syndrome and open-angle glaucoma. Ophthalmology 2011, 118, 1318–1326. [Google Scholar] [CrossRef]
- Rasoulinejad, S.A.; Kasiri, A.; Montazeri, M.; Rashidi, N.; Montazeri, M.; Montazeri, M.; Hedayati, H. The association between primary open angle glaucoma and clustered components of metabolic syndrome. Open Ophthalmol. J. 2015, 9, 149. [Google Scholar] [CrossRef]
- Kim, H.A.; Han, K.; Lee, Y.A.; Choi, J.A.; Park, Y.M. Differential Association of Metabolic Risk Factors with Open Angle Glaucoma according to Obesity in a Korean Population. Sci. Rep. 2016, 6, 38283. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.Y.; Lin, C.L. Comparison of medical comorbidity between patients with primary angle-closure glaucoma and a control cohort: A population-based study from Taiwan. BMJ Open 2019, 9, e024209. [Google Scholar] [CrossRef] [PubMed]
- Ah-Kee, E.Y.; Egong, E.; Shafi, A.; Lim, L.T.; Yim, J.L. A review of drug-induced acute angle closure glaucoma for non-ophthalmologists. Qatar Med. J. 2015, 2015, 6. [Google Scholar] [CrossRef]
- Yang, M.C.; Lin, K.Y. Drug-induced Acute Angle-closure Glaucoma: A Review. J. Curr. Glaucoma Pract. 2019, 13, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Vajaranant, T.S.; Nayak, S.; Wilensky, J.T.; Joslin, C.E. Gender and glaucoma: What we know and what we need to know. Curr. Opin. Ophthalmol. 2010, 21, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.K.; Kee, C. Population-based glaucoma prevalence studies in Asians. Surv Ophthalmol. 2014, 59, 434–447. [Google Scholar] [CrossRef]
- Zetterberg, M. Age-related eye disease and gender. Maturitas 2016, 83, 19–26. [Google Scholar] [CrossRef]
- Cook, C.; Foster, P. Epidemiology of glaucoma: What’s new? Can. J. Ophthalmol. J. Can. D’ophtalmol. 2012, 47, 223–226. [Google Scholar] [CrossRef]
- Mabry, R.M.; Reeves, M.M.; Eakin, E.G.; Owen, N. Gender differences in prevalence of the metabolic syndrome in Gulf Cooperation Council Countries: A systematic review. Diabet. Med. A J. Br. Diabet. Assoc. 2010, 27, 593–597. [Google Scholar] [CrossRef]
- Ford, E.S.; Giles, W.H.; Dietz, W.H. Prevalence of the metabolic syndrome among US adults: Findings from the third National Health and Nutrition Examination Survey. JAMA 2002, 287, 356–359. [Google Scholar] [CrossRef]
- Kuo, C.Y.; Ko, Y.C.; Kuang, T.M.; Chou, P.; Chiou, S.H.; Liu, C.J. Prevalence of glaucoma in the elderly population in Taiwan: The Shihpai Eye Study. J. Chin. Med. Assoc. JCMA 2020, 83, 880–884. [Google Scholar] [CrossRef]
- Wong, V.H.; Bui, B.V.; Vingrys, A.J. Clinical and experimental links between diabetes and glaucoma. Clin. Exp. Optom. 2011, 94, 4–23. [Google Scholar] [CrossRef]
- Song, B.J.; Aiello, L.P.; Pasquale, L.R. Presence and Risk Factors for Glaucoma in Patients with Diabetes. Curr Diab. Rep. 2016, 16, 124. [Google Scholar] [CrossRef] [PubMed]
- Husain, S.; Abdul, Y.; Singh, S.; Ahmad, A.; Husain, M. Regulation of nitric oxide production by δ-opioid receptors during glaucomatous injury. PLoS ONE 2014, 9, e110397. [Google Scholar] [CrossRef]
- Alexander, J.P.; Acott, T.S. Involvement of protein kinase C in TNFalpha regulation of trabecular matrix metalloproteinases and TIMPs. Investig. Ophthalmol. Vis. Sci. 2001, 42, 2831–2838. [Google Scholar]
- Wang, S.; Bao, X. Hyperlipidemia, Blood Lipid Level, and the Risk of Glaucoma: A Meta-Analysis. Investig. Ophthalmol. Vis. Sci. 2019, 60, 1028–1043. [Google Scholar] [CrossRef]
- Qian, H.; Zhao, X.; Cao, P.; Lei, J.; Yan, N.; Gong, X. Structure of the Human Lipid Exporter ABCA1. Cell 2017, 169, 1228–1239.e10. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Chen, D.; Huang, H.; Wang, J.; Wan, X.; Xu, C.; Li, C.; Ma, H.; Yu, C.; Li, Y. Caveolin1 protects against diet induced hepatic lipid accumulation in mice. PLoS ONE 2017, 12, e0178748. [Google Scholar] [CrossRef]
- Langman, M.J.; Lancashire, R.J.; Cheng, K.K.; Stewart, P.M. Systemic hypertension and glaucoma: Mechanisms in common and co-occurrence. Br. J. Ophthalmol. 2005, 89, 960–963. [Google Scholar] [CrossRef]
- Jung, Y.; Han, K.; Park, H.Y.L.; Lee, S.H.; Park, C.K. Metabolic Health, Obesity, and the Risk of Developing Open-Angle Glaucoma: Metabolically Healthy Obese Patients versus Metabolically Unhealthy but Normal Weight Patients. Diabetes Metab. J. 2010, 44, 415–425. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | With Metabolic Disease N = 42,036 | Without Metabolic Disease N = 84,072 | p Value |
|---|---|---|---|
| n (%) | n (%) | ||
| Obesity | <0.0001 | ||
| No | 41,762 (99.3) | 84,028 (99.95) | |
| Yes | 274 (0.65) | 44 (0.05) | |
| Age, year | 0.99 | ||
| <40 | 8846 (21.0) | 17,692 (21.0) | |
| 40–64 | 25,194 (59.9) | 50,388 (59.9) | |
| 65+ | 7996 (19.0) | 15,992 (19.0) | |
| Mean(SD) | 51.4(14.6) | 51.2(14.6) | 0.20 |
| Gender | 0.99 | ||
| Female | 19,217 (45.7) | 38,434 (45.7) | |
| Male | 22,819 (54.3) | 45,638 (54.3) | |
| Monthly income, NTD | 0.006 | ||
| <20,000 | 24,712 (58.8) | 49,579 (59.0) | |
| 20,000–40,000 | 11,990 (28.5) | 24,333 (28.9) | |
| >40,000 | 5334 (12.7) | 10,160 (12.1) | |
| Comorbidity | |||
| Hypothyroidism | 99 (0.24) | 86 (0.10) | <0.0001 |
| OSA | 55 (0.13) | 30 (0.04) | <0.0001 |
| Depression | 1027 (2.44) | 1013 (1.20) | <0.0001 |
| Anxiety | 49 (0.12) | 45 (0.05) | 0.0001 |
| Headaches | 5670 (13.5) | 5843 (6.95) | <0.0001 |
| Liver diseases | 9338 (22.2) | 7308 (8.69) | <0.0001 |
| Peptic ulcers | 12,085 (28.8) | 16,543 (19.7) | <0.0001 |
| Cataract | 3828 (9.11) | 5936 (7.06) | <0.0001 |
| CRVO | 9 (0.02) | 4 (0.05) | 0.014 |
| AMD | 473 (1.13) | 562 (0.67) | <0.0001 |
| Glaucomas-associated drug | 22,356 (53.2) | 33,349 (39.7) | <0.0001 |
| Variables | Glaucoma n | Person-Years | Rate | Crude HR (95% CI) | p | Adjusted HR (95% CI) | p |
|---|---|---|---|---|---|---|---|
| Metabolic disease | |||||||
| No | 659 | 662,371 | 0.99 | Ref. | Ref. | ||
| Yes | 951 | 478,927 | 1.99 | 2.00 (1.81–2.21) | < 0.0001 | 1.66 (1.50–1.85) | <0.0001 |
| Obesity | |||||||
| No | 1606 | 1,137,703 | 1.41 | Ref. | |||
| Yes | 4 | 3595 | 1.11 | 0.78 (0.29–2.09) | 0.6270 | ||
| Age (year) | |||||||
| <40 | 136 | 290,859 | 0.47 | Ref. | Ref. | ||
| 40–64 | 1025 | 691,465 | 1.48 | 3.19 (2.67–3.82) | < 0.0001 | 2.83 (2.36–3.38) | <0.0001 |
| 65+ | 449 | 158,975 | 2.82 | 6.16 (5.08–7.47) | < 0.0001 | 3.72 (3.03–4.58) | <0.0001 |
| Gender | |||||||
| Female | 822 | 522,015 | 1.57 | 1.24 (1.12–1.36) | < 0.0001 | 1.13 (1.03–1.25) | 0.0142 |
| Male | 788 | 619,283 | 1.27 | Ref. | Ref. | ||
| Monthly income, NTD | |||||||
| <20,000 | 926 | 656,740 | 1.41 | 1.04 (0.89–1.21) | 0.6418 | ||
| 20,000–40,000 | 479 | 333,856 | 1.43 | 1.06 (0.90–1.24) | 0.5206 | ||
| >40,000 | 205 | 150,702 | 1.36 | Ref. | |||
| Comobidity | |||||||
| Hypothyroidism | |||||||
| No | 1607 | 1,139,616 | 1.41 | Ref. | |||
| Yes | 3 | 1682 | 1.78 | 1.26 (0.41–3.92) | 0.6860 | ||
| OSA | |||||||
| No | 1608 | 1,140,454 | 1.41 | Ref. | |||
| Yes | 2 | 844 | 2.37 | 1.68 (0.42–6.70) | 0.4658 | ||
| Depression | |||||||
| No | 1570 | 1,123,495 | 1.40 | Ref. | Ref. | ||
| Yes | 40 | 17,803 | 2.25 | 1.61 (1.17–2.20) | 0.0031 | 1.21 (0.88–1.66) | 0.2501 |
| Anxiety | |||||||
| No | 1609 | 1,140,420 | 1.41 | Ref. | |||
| Yes | 1 | 878 | 1.14 | 0.81 (0.11–5.73) | 0.8295 | ||
| Headaches | |||||||
| No | 1437 | 1,036,655 | 1.39 | Ref. | Ref. | ||
| Yes | 173 | 104,643 | 1.65 | 1.19 (1.02–1.39) | 0.0300 | 0.92 (0.78–1.09) | 0.3309 |
| Liver diseases | |||||||
| No | 1339 | 987,052 | 1.36 | Ref. | Ref. | ||
| Yes | 271 | 154,246 | 1.76 | 1.29 (1.13–1.47) | 0.0001 | 1.12 (0.97–1.28) | 0.1132 |
| Peptic ulcers | |||||||
| No | 1120 | 893,273 | 1.25 | Ref. | Ref. | ||
| Yes | 490 | 248,025 | 1.98 | 1.58 (1.42–1.75) | < 0.0001 | 1.13 (1.01–1.26) | 0.0401 |
| Cataract | |||||||
| No | 1260 | 1,070,736 | 1.18 | Ref. | Ref. | ||
| Yes | 350 | 70,562 | 4.96 | 4.24 (3.76–4.77) | < 0.0001 | 1.90 (1.66–2.19) | <0.0001 |
| CRVO | |||||||
| No | 1610 | 1,141,191 | 1.41 | Ref. | |||
| Yes | 0 | 108 | 0.00 | NA | |||
| AMD | |||||||
| No | 1557 | 1,132,905 | 1.37 | Ref. | Ref. | ||
| Yes | 53 | 8393 | 6.31 | 4.60 (3.50–6.05) | < 0.0001 | 2.11 (1.59–2.80) | <0.0001 |
| Glaucomas associated drug | |||||||
| No | 787 | 649,874 | 1.21 | Ref. | Ref. | ||
| Yes | 823 | 491,424 | 1.67 | 1.38 (1.25–1.52) | < 0.0001 | 1.10 (0.99–1.22) | 0.0810 |
| Variables | N | Glaucoma No. | Person-Years | Rate | Adjusted HR (95% CI) | p |
|---|---|---|---|---|---|---|
| None | 84,072 | 659 | 662,371 | 0.99 | Ref. | |
| Only Hypertension | 21,863 | 478 | 244,949 | 1.95 | 1.48 (1.31–1.67) | <0.0001 |
| Only Diabetes | 6365 | 163 | 68,391 | 2.38 | 2.14 (1.80–2.55) | <0.0001 |
| Only Hyperlipidemia | 11,490 | 239 | 138,752 | 1.72 | 1.79 (1.54–2.09) | <0.0001 |
| Diabetes + Hypertension | 439 | 17 | 4510 | 3.77 | 2.87 (1.78–4.66) | <0.0001 |
| Diabetes + Hyperlipidemia | 1094 | 35 | 12,979 | 2.70 | 2.63 (1.87–3.69) | <0.0001 |
| Hypertension + Hyperlipidemia | 680 | 12 | 8110 | 1.48 | 1.33 (0.75–2.36) | 0.3275 |
| Diabetes + Hypertension + Hyperlipidemia | 105 | 7 | 1235 | 5.67 | 4.95 (2.35–10.4) | <0.0001 |
| Patients with One or More Metabolic Disease | Controls | |||||||
|---|---|---|---|---|---|---|---|---|
| Outcome | Glaucoma (n) | Person-Years | Rate | Glaucoma (n) | Person-Years | Rate | Adjusted HR (95% CI) | p |
| Overall | 951 | 478,927 | 1.99 | 659 | 662,371 | 0.99 | 1.66 (1.50–1.85) | <0.0001 |
| Open angle glaucoma | 487 | 478,927 | 1.02 | 292 | 662,371 | 0.44 | 2.03 (1.75–2.36) | <0.0001 |
| Closure angle glaucoma | 464 | 478,927 | 0.97 | 367 | 662,371 | 0.55 | 1.44 (1.25–1.66) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, Y.-W.; Sung, F.-C.; Tzeng, Y.-L.; Mou, C.-H.; Tien, P.-T.; Su, C.-W.; Teng, Y.-K. Risk of Glaucoma Associated with Components of Metabolic Disease in Taiwan: A Nationwide Population-Based Study. Int. J. Environ. Res. Public Health 2022, 19, 305. https://doi.org/10.3390/ijerph19010305
Chang Y-W, Sung F-C, Tzeng Y-L, Mou C-H, Tien P-T, Su C-W, Teng Y-K. Risk of Glaucoma Associated with Components of Metabolic Disease in Taiwan: A Nationwide Population-Based Study. International Journal of Environmental Research and Public Health. 2022; 19(1):305. https://doi.org/10.3390/ijerph19010305
Chicago/Turabian StyleChang, Ya-Wen, Fung-Chang Sung, Ya-Ling Tzeng, Chih-Hsin Mou, Peng-Tai Tien, Cheng-Wen Su, and Yu-Kuei Teng. 2022. "Risk of Glaucoma Associated with Components of Metabolic Disease in Taiwan: A Nationwide Population-Based Study" International Journal of Environmental Research and Public Health 19, no. 1: 305. https://doi.org/10.3390/ijerph19010305
APA StyleChang, Y.-W., Sung, F.-C., Tzeng, Y.-L., Mou, C.-H., Tien, P.-T., Su, C.-W., & Teng, Y.-K. (2022). Risk of Glaucoma Associated with Components of Metabolic Disease in Taiwan: A Nationwide Population-Based Study. International Journal of Environmental Research and Public Health, 19(1), 305. https://doi.org/10.3390/ijerph19010305