
Can an E-Mail-Delivered CBT for Insomnia Validated in the West Be Effective in the East? A Randomized Controlled Trial

 ,
, 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Sample Size
2.3. Study Design
2.4. Measurements
2.4.1. Primary Outcomes
2.4.2. Secondary Outcomes
2.5. Intervention
2.5.1. Intervention (REFRESH) Group
2.5.2. Self-Monitoring Group
2.6. Statistical Analysis
3. Results
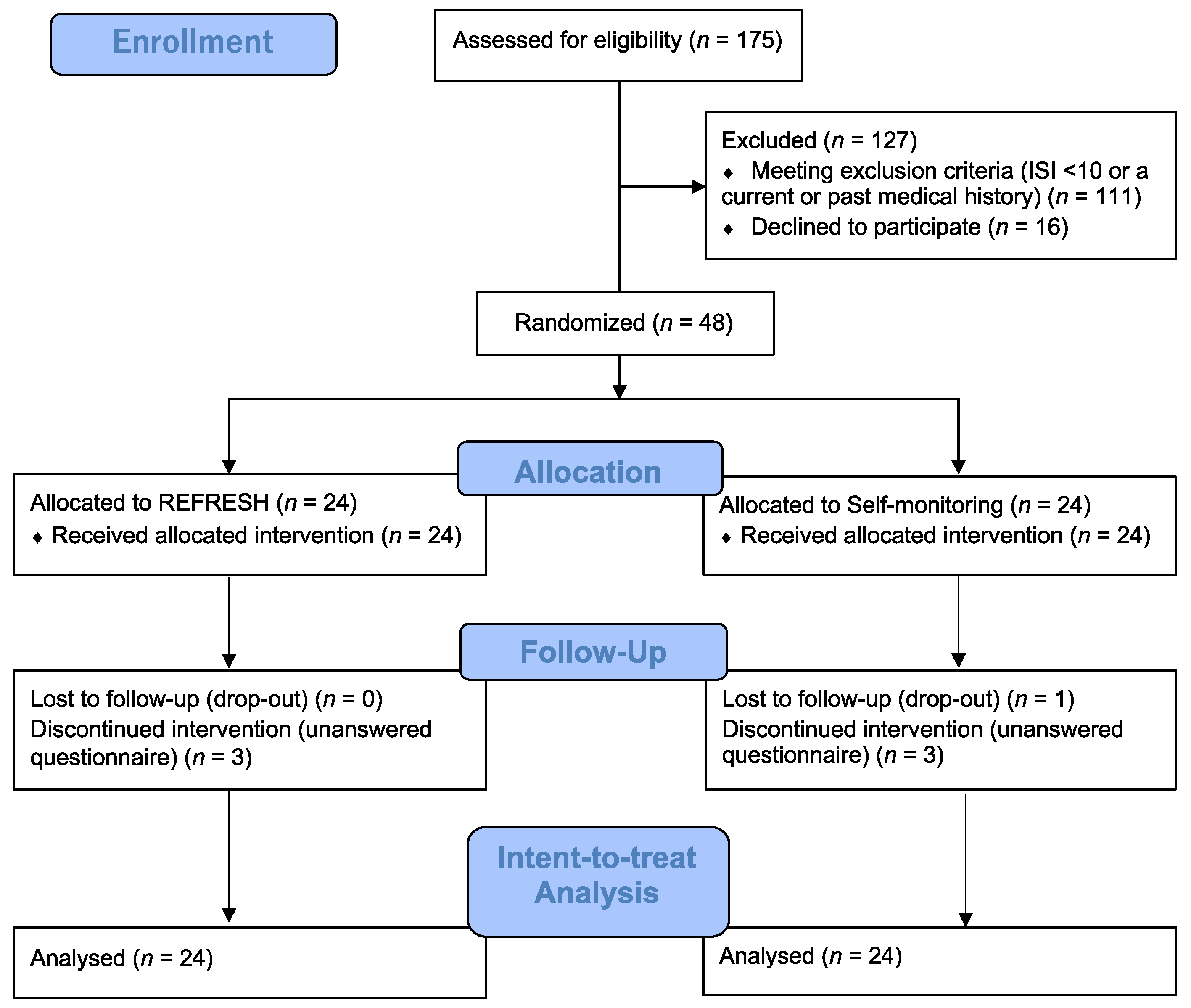
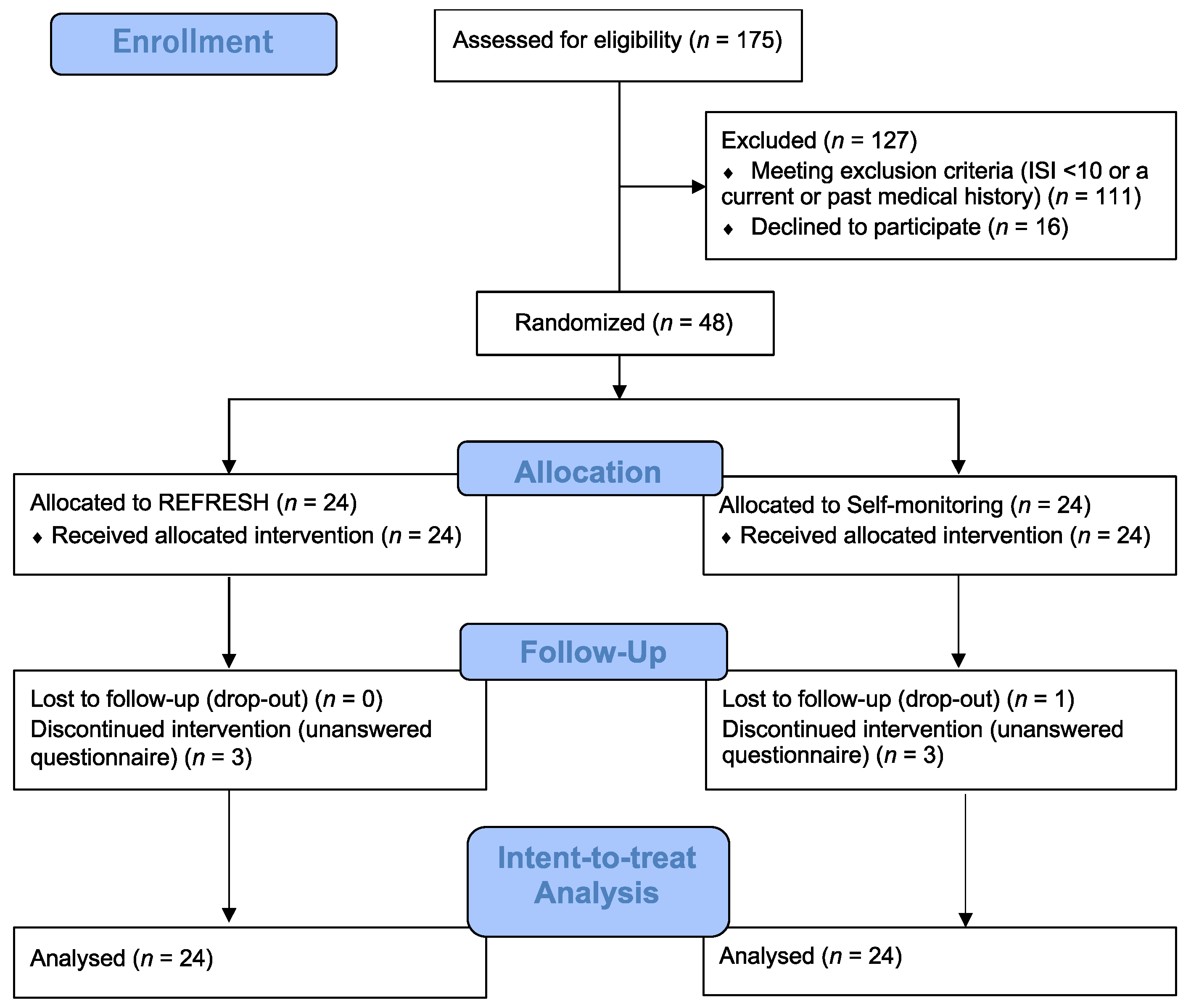
3.1. Adherence and Attrition
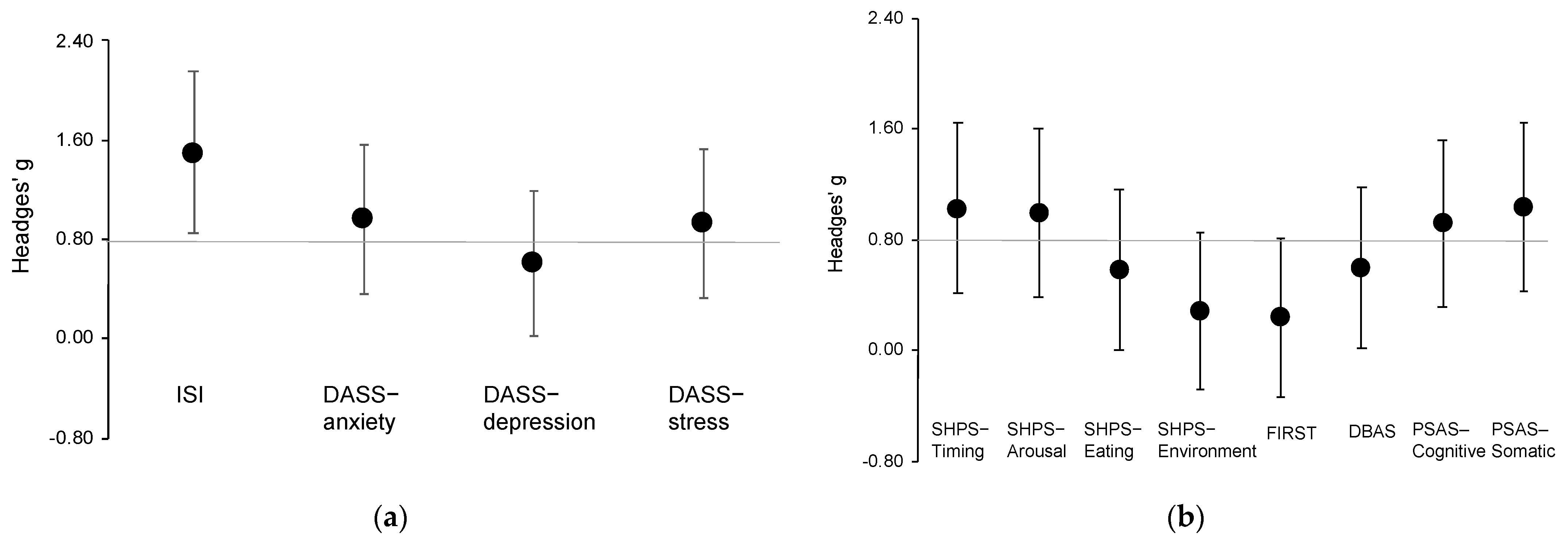
3.2. Main Outcomes: Insomnia Severity, Depression, Anxiety, and Stress
3.3. Secondary Outcomes: Sleep Hygiene Practice, Stress Reactivity, Dysfunctional Beliefs, and Pre-Sleep Arousal
3.4. Clinically Significant Improvement
4. Discussion
4.1. Effects in Improvement of Insomnia and Affective Symptoms
4.2. Reduction in Insomnia-Related Symptoms
4.3. Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Morin, C.M.; Jarrin, D.C.; Ivers, H.; Mérette, C.; LeBlanc, M.; Savard, J. Incidence, Persistence, and Remission Rates of Insomnia Over 5 Years. JAMA Netw. Open 2020, 3, e2018782. [Google Scholar] [CrossRef] [PubMed]
- Hertenstein, E.; Feige, B.; Gmeiner, T.; Kienzler, C.; Spiegelhalder, K.; Johann, A.; Jansson-Fröjmark, M.; Palagini, L.; Rücker, G.; Riemann, D.; et al. Insomnia as a Predictor of Mental Disorders: A Systematic Review and Meta-Analysis. Sleep Med. Rev. 2019, 43, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Lund, H.G.; Reider, B.D.; Whiting, A.B.; Prichard, J.R. Sleep Patterns and Predictors of Disturbed Sleep in a Large Population of College Students. J. Adolesc. Health 2010, 46, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.E.; Ramsay Roberts, C.; Chan, W. Persistence and Change in Symptoms of Insomnia among Adolescents. Sleep 2008, 31, 177–184. [Google Scholar] [CrossRef]
- Li, S.X.; Chan, N.Y.; Man Yu, M.W.; Lam, S.P.; Zhang, J.; Yan Chan, J.W.; Li, A.M.; Wing, Y.K. Eveningness Chronotype, Insomnia Symptoms, and Emotional and Behavioural Problems in Adolescents. Sleep Med. 2018, 47, 93–99. [Google Scholar] [CrossRef]
- Morioka, H.; Itani, O.; Kaneita, Y.; Ikeda, M.; Kondo, S.; Yamamoto, R.; Osaki, Y.; Kanda, H.; Higuchi, S.; Ohida, T. Associations between Sleep Disturbance and Alcohol Drinking: A Large-Scale Epidemiological Study of Adolescents in Japan. Alcohol 2013, 47, 619–628. [Google Scholar] [CrossRef]
- Miyake, Y.; Okamoto, Y.; Jinnin, R.; Nagasawa, I.; Yashiki, H.; Uchino, T.; Isobe, N.; Takata, J.; Kojima, N.; Nihonmatsu, M.; et al. Insomnia disorder in university students. Bull. Health Serivice Cent. Hiroshima Univ. 2015, 31, 7–12. [Google Scholar] [CrossRef]
- Becker, S.P.; Dvorsky, M.R.; Holdaway, A.S.; Luebbe, A.M. Sleep Problems and Suicidal Behaviors in College Students. J. Psychiatr. Res. 2018, 99, 122–128. [Google Scholar] [CrossRef]
- Williams, A.B.; Dzierzewski, J.M.; Griffin, S.C.; Lind, M.J.; Dick, D.; Rybarczyk, B.D. Insomnia Disorder and Behaviorally Induced Insufficient Sleep Syndrome: Prevalence and Relationship to Depression in College Students. Behav. Sleep Med. 2020, 18, 275–286. [Google Scholar] [CrossRef]
- Hershner, S.; O’Brien, L.M. The Impact of a Randomized Sleep Education Intervention for College Students. J. Clin. Sleep Med. 2018, 14, 337–347. [Google Scholar] [CrossRef] [Green Version]
- Trockel, M.; Manber, R.; Chang, V.; Thurston, A.; Tailor, C.B. An E-Mail Delivered CBT for Sleep-Health Program for College Students: Effects on Sleep Quality and Depression Symptoms. J. Clin. Sleep Med. 2011, 07, 276–281. [Google Scholar] [CrossRef]
- Mak, W.W.; Chio, F.H.; Chan, A.T.; Lui, W.W.; Wu, E.K. The Efficacy of Internet-Based Mindfulness Training and Cognitive-Behavioral Training with Telephone Support in the Enhancement of Mental Health among College Students and Young Working Adults: Randomized Controlled Trial. J. Med. Internet Res. 2017, 19, e84. [Google Scholar] [CrossRef] [PubMed]
- Ho, F.Y.-Y.; Chung, K.-F.; Yeung, W.-F.; Ng, T.H.; Kwan, K.-S.; Yung, K.-P.; Cheng, S.K. Self-Help Cognitive-Behavioral Therapy for Insomnia: A Meta-Analysis of Randomized Controlled Trials. Sleep Med. Rev. 2015, 19, 17–28. [Google Scholar] [CrossRef]
- Espie, C.A.; Emsley, R.; Kyle, S.D.; Gordon, C.; Drake, C.L.; Siriwardena, A.N.; Cape, J.; Ong, J.C.; Sheaves, B.; Foster, R.; et al. Effect of Digital Cognitive Behavioral Therapy for Insomnia on Health, Psychological Well-Being, and Sleep-Related Quality of Life: A Randomized Clinical Trial. JAMA Psychiatry 2019, 76, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Tamura, N. Sleep Education with Self-Help Treatment and Sleep Health Promotion for Mental and Physical Wellness in Japan. Sleep Biol. Rhythm. 2016, 14, 89–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edinger, J.D.; Arnedt, J.T.; Bertisch, S.M.; Carney, C.E.; Harrington, J.J.; Lichstein, K.L.; Sateia, M.J.; Troxel, W.M.; Zhou, E.S.; Kazmi, U.; et al. Behavioral and Psychological Treatments for Chronic Insomnia Disorder in Adults: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2021, 17, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Japan Student Services Organization. Summary of Result on an Annual Survey of International Students in Japan in 2019; Japan Student Services Organization: Tokyo, Japan, 2019. [Google Scholar]
- Munezawa, T.; Inoue, Y.; Morin, C.M.; Nedate, K. Development of the Japanese version of the Insomnia Severity Index (ISI-J). Jpn. J. Psychiatr. Treat. 2009, 24, 219–225. [Google Scholar]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the Insomnia Severity Index as an Outcome Measure for Insomnia Research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Lovibond, P.F.; Lovibond, S.H. The Structure of Negative Emotional States: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Hara, S.; Nonaka, S.; Ishii, M.; Ogawa, Y.; Yang, C.-M.; Okajima, I. Validation of the Japanese Version of the Sleep Hygiene Practice Scale. Sleep Med. 2021, 80, 204–209. [Google Scholar] [CrossRef]
- Yang, C.-M.; Lin, S.-C.; Hsu, S.-C.; Cheng, C.-P. Maladaptive Sleep Hygiene Practices in Good Sleepers and Patients with Insomnia. J. Health Psychol. 2010, 15, 147–155. [Google Scholar] [CrossRef]
- Morin, C.M.; Vallières, A.; Ivers, H. Dysfunctional Beliefs and Attitudes about Sleep (DBAS): Validation of a Brief Version (DBAS-16). Sleep 2007, 30, 1547–1554. [Google Scholar] [CrossRef] [Green Version]
- Munezawa, T.; Morin, C.M.; Inoue, Y.; Nedate, K. Development of the Japanese version of Dysfunctional Beliefs and Attitudes about Sleep Scale (DBAS-J). Jpn. Sleep Med. 2009, 3, 396–403. [Google Scholar]
- Drake, C.L.; Pillai, V.; Roth, T. Stress and Sleep Reactivity: A Prospective Investigation of the Stress-Diathesis Model of Insomnia. Sleep 2014, 37, 1295–1304. [Google Scholar] [CrossRef] [Green Version]
- Drake, C.; Richardson, G.; Roehrs, T.; Scofield, H.; Roth, T. Vulnerability to Stress-Related Sleep Disturbance and Hyperarousal. Sleep 2004, 27, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, S.; Okajima, I.; Sasai, T.; Kobayashi, M.; Furudate, N.; Drake, C.L.; Roth, T.; Inoue, Y. Validation of the Japanese Version of the Ford Insomnia Response to Stress Test and the Association of Sleep Reactivity with Trait Anxiety and Insomnia. Sleep Med. 2014, 15, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Nicassio, P.M.; Mendlowitz, D.R.; Fussell, J.J.; Petras, L. The Phenomenology of the Pre-Sleep State: The Development of the Pre-Sleep Arousal Scale. Behav. Res. Ther. 1985, 23, 263–271. [Google Scholar] [CrossRef]
- Okajima, I.; Ishii, M.; Ochi, M.; Nicassio, P.M. Development and Validity of the Japanese Version of the Pre-Sleep Arousal Scale. Tohoku J. Exp. Med. 2020, 252, 169–176. [Google Scholar] [CrossRef]
- Okajima, I.; Akitomi, J.; Kajiyama, I.; Ishii, M.; Murakami, H.; Yamaguchi, M. Effects of a Tailored Brief Behavioral Therapy Application on Insomnia Severity and Social Disabilities Among Workers With Insomnia in Japan: A Randomized Clinical Trial. JAMA Netw. Open 2020, 3, e202775. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Hillsdale, N.J., Ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Åslund, L.; Lekander, M.; Wicksell, R.K.; Henje, E.; Jernelöv, S. Cognitive-Behavioral Therapy for Insomnia in Adolescents with Comorbid Psychiatric Disorders: A Clinical Pilot Study. Clin. Child Psychol. Psychiatry 2020, 25, 958–971. [Google Scholar] [CrossRef]
- Okajima, I.; Chen, J. The Effect of Insomnia on Changes in Anxiety, Depression, and Social Function after a Transdiagnostic Treatment Targeting Excessive Worry. Sleep Biol. Rhythm. 2017, 15, 243–249. [Google Scholar] [CrossRef]
- Lancee, J.; Eisma, M.C.; van Straten, A.; Kamphuis, J.H. Sleep-Related Safety Behaviors and Dysfunctional Beliefs Mediate the Efficacy of Online CBT for Insomnia: A Randomized Controlled Trial. Cogn. Behav. Ther. 2015, 44, 406–422. [Google Scholar] [CrossRef]
- Lancee, J.; Effting, M.; van der Zweerde, T.; van Daal, L.; van Straten, A.; Kamphuis, J.H. Cognitive Processes Mediate the Effects of Insomnia Treatment: Evidence from a Randomized Wait-List Controlled Trial. Sleep Med. 2019, 54, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Palagini, L.; Mauri, M.; Dell’Osso, L.; Riemann, D.; Drake, C.L. Trait- and Pre-Sleep-State-Dependent Arousal in Insomnia Disorders: What Role May Sleep Reactivity and Sleep-Related Metacognitions Play? A Pilot Study. Sleep Med. 2016, 25, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Riemann, D.; Spiegelhalder, K.; Feige, B.; Voderholzer, U.; Berger, M.; Perlis, M.; Nissen, C. The Hyperarousal Model of Insomnia: A Review of the Concept and Its Evidence. Sleep Med. Rev. 2010, 14, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Vincent, N.; Walsh, K. Stepped Care for Insomnia: An Evaluation of Implementation in Routine Practice. J. Clin. Sleep Med. 2013, 9, 227–234. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Scales | REFRESH Group | Self-Monitoring Group | p-Values | ||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Group | Time | Interaction | |
| ISI | 13.63 (0.66) | 7.01 (0.70) | 14.00 (0.66) | 12.31 (0.72) | <0.001 | <0.001 | <0.001 |
| DASS-anxiety | 3.97 (0.53) | 1.55 (0.56) | 4.79 (0.53) | 4.27 (0.57) | 0.009 | 0.001 | 0.026 |
| DASS-depression | 6.29 (0.81) | 2.97 (0.85) | 6.29 (0.81) | 5.57 (0.87) | ns | 0.002 | 0.041 |
| DASS-stress | 6.83 (0.73) | 3.10 (0.78) | 8.38 (0.73) | 6.75 (0.79) | 0.005 | <0.001 | 0.084 |
| SHPS-timing | 26.79 (1.29) | 19.87 (1.36) | 28.21 (1.29) | 26.91 (1.38) | 0.012 | <0.001 | 0.006 |
| SHPS-arousal | 28.83 (1.33) | 22.29 (1.42) | 29.75 (1.33) | 29.43 (1.45) | 0.007 | 0.014 | 0.024 |
| SHPS-eating | 16.04 (0.77) | 12.99 (0.78) | 14.96 (0.77) | 15.39 (0.84) | ns | 0.074 | 0.019 |
| SHPS-environment | 22.68 (1.25) | 21.24 (1.32) | 23.96 (1.25) | 23.15 (1.35) | ns | ns | ns |
| FIRST | 25.46 (1.00) | 22.58 (1.05) | 26.13 (1.00) | 23.83 (1.07) | ns | 0.001 | ns |
| DBAS | 91.96 (3.31) | 74.89 (3.50) | 92.88 (3.31) | 85.37 (3.57) | ns | <0.001 | 0.082 |
| PSAS-cognitive | 24.67 (1.28) | 16.99 (1.36) | 25.54 (1.28) | 23.28 (1.39) | 0.021 | <0.001 | 0.022 |
| PSAS-somatic | 16.33 (1.05) | 12.43 (1.09) | 18.17 (1.05) | 18.13 (1.11) | 0.007 | 0.007 | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okajima, I.; Tanizawa, N.; Harata, M.; Suh, S.; Yang, C.-M.; Li, S.X.; Trockel, M.T. Can an E-Mail-Delivered CBT for Insomnia Validated in the West Be Effective in the East? A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 186. https://doi.org/10.3390/ijerph19010186
Okajima I, Tanizawa N, Harata M, Suh S, Yang C-M, Li SX, Trockel MT. Can an E-Mail-Delivered CBT for Insomnia Validated in the West Be Effective in the East? A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(1):186. https://doi.org/10.3390/ijerph19010186
Chicago/Turabian StyleOkajima, Isa, Noriko Tanizawa, Megumi Harata, Sooyeon Suh, Chien-Ming Yang, Shirley Xin Li, and Mickey T. Trockel. 2022. "Can an E-Mail-Delivered CBT for Insomnia Validated in the West Be Effective in the East? A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 1: 186. https://doi.org/10.3390/ijerph19010186
APA StyleOkajima, I., Tanizawa, N., Harata, M., Suh, S., Yang, C.-M., Li, S. X., & Trockel, M. T. (2022). Can an E-Mail-Delivered CBT for Insomnia Validated in the West Be Effective in the East? A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 19(1), 186. https://doi.org/10.3390/ijerph19010186