
Association of Subjective Quality and Quantity of Sleep with Quality of Life among a General Population

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Measures
2.3. Statistical Analysis
3. Results
3.1. Correlation between Variables
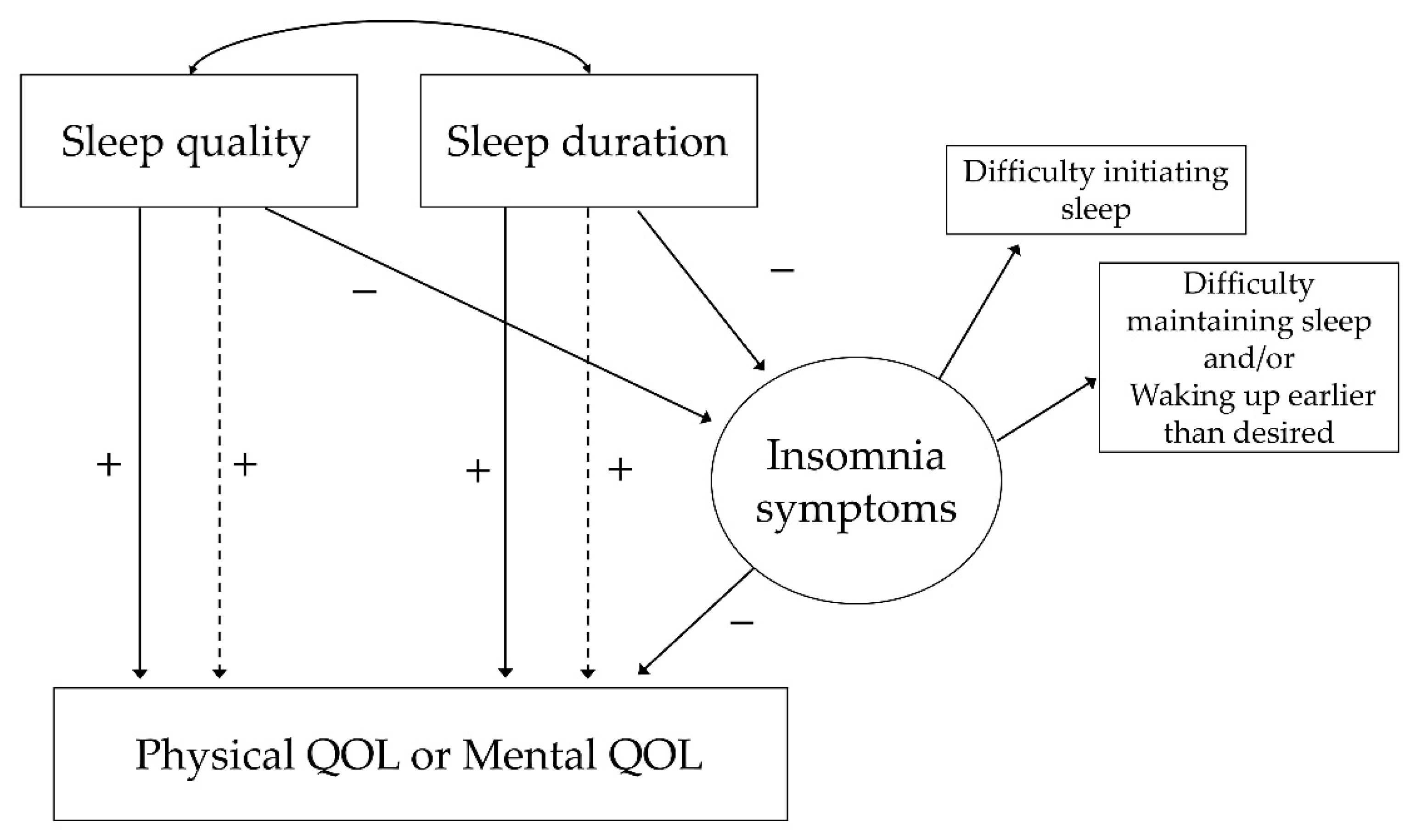
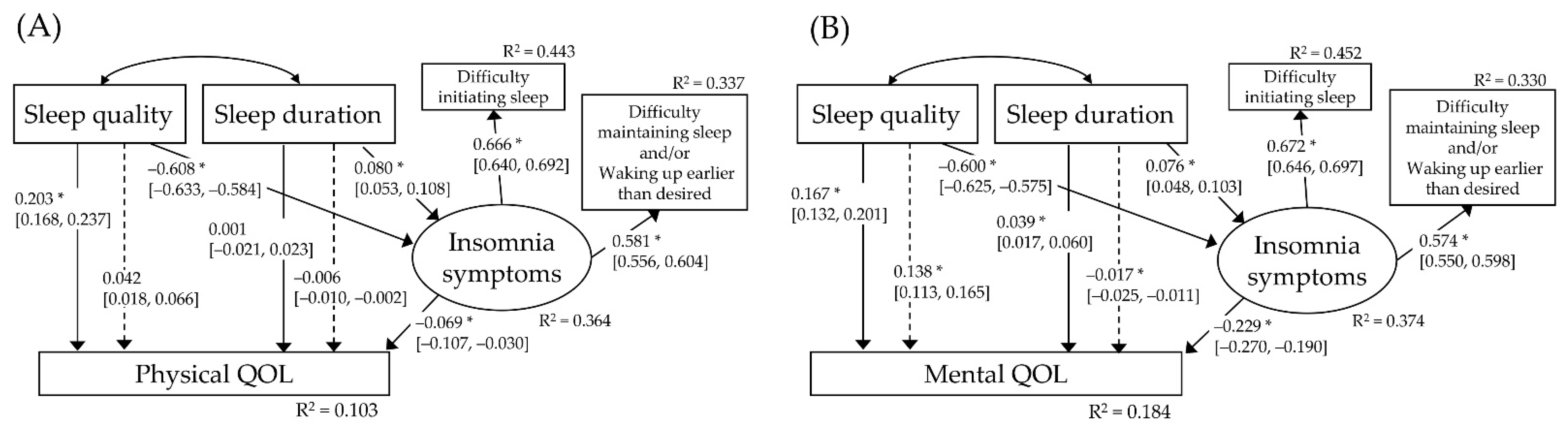
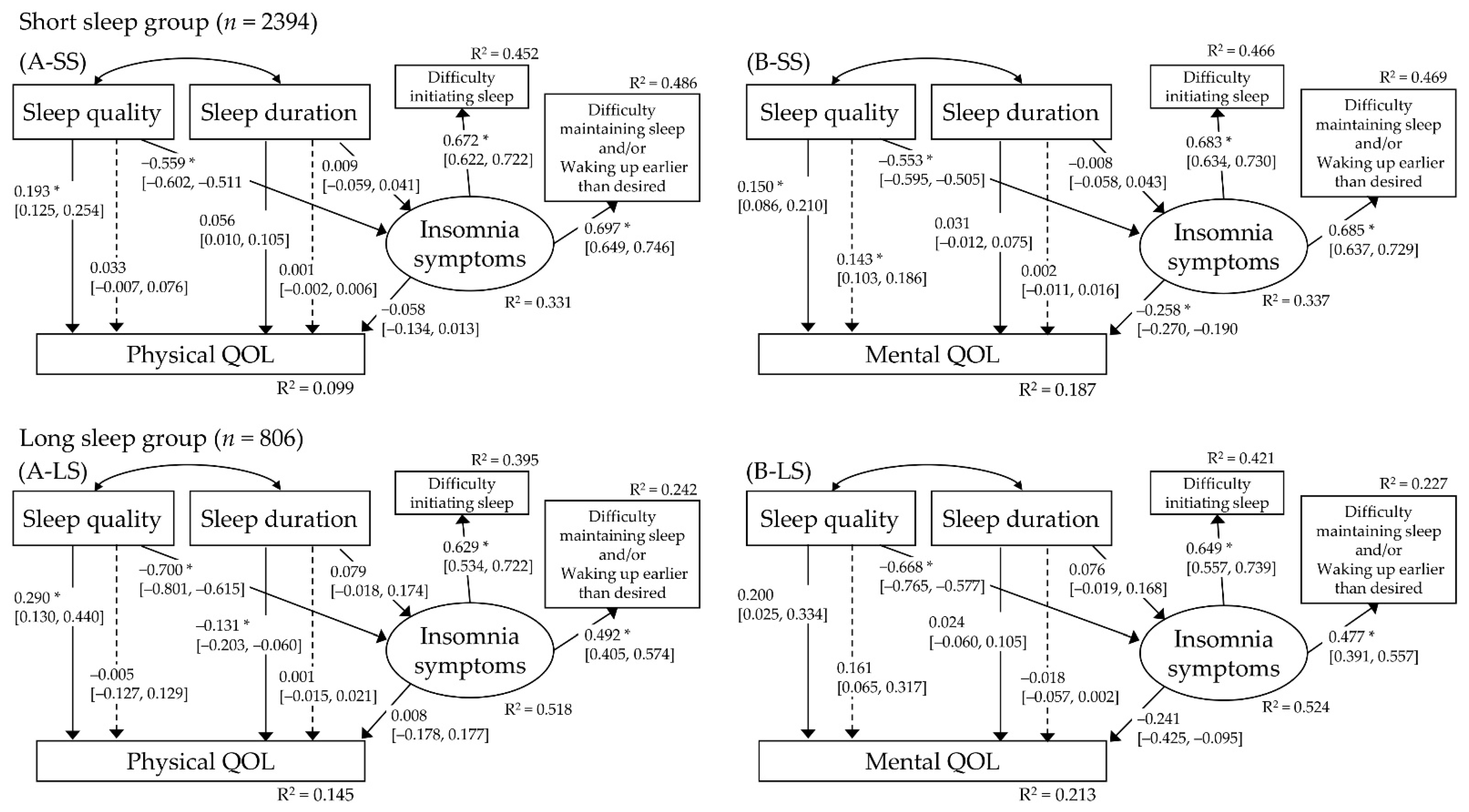
3.2. Mediation Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The WHOQOL Group. The World Health Organization quality of life assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar] [CrossRef]
- Fayers, P.M.; Machin, D. Quality of Life: The Assessment, Analysis and Reporting of Patient-Reported Outcomes; John Wiley & Sons: Hoboken, NJ, USA, 2015. [Google Scholar]
- Verster, J.C.; Pandi-Perumal, S.R.; Streiner, D.L. Sleep and Quality of Life in Clinical Medicine; Springer: Berlin/Heidelberg, Germany, 2008. [Google Scholar]
- Stranges, S.; Dorn, J.M.; Shipley, M.J.; Kandala, N.B.; Trevisan, M.; Miller, M.A.; Donahue, R.P.; Hovey, K.M.; Ferrie, J.E.; Marmot, M.G.; et al. Correlates of short and long sleep duration: A cross-cultural comparison between the United Kingdom and the United States: The Whitehall II Study and the Western New York Health Study. Am. J. Epidemiol. 2008, 168, 1353–1364. [Google Scholar] [CrossRef] [PubMed]
- Magee, C.A.; Caputi, P.; Iverson, D.C. Relationships between self-rated health, quality of life and sleep duration in middle aged and elderly Australians. Sleep Med. 2011, 12, 346–350. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Park, E.C.; Yoo, K.B.; Park, S. The Association between Short or Long Sleep Times and Quality of Life (QOL): Results of the Korea National Health and Nutrition Examination Survey (KNHANES IV-V). J. Clin. Sleep Med. 2015, 11, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Cohrdes, C.; Mensink, G.B.M.; Hölling, H. How you live is how you feel? Positive associations between different lifestyle factors, cognitive functioning, and health-related quality of life across adulthood. Qual. Life Res. 2018, 27, 3281–3292. [Google Scholar] [CrossRef] [PubMed]
- Matsui, K.; Kuriyama, K.; Yoshiike, T.; Nagao, K.; Ayabe, N.; Komada, Y.; Okajima, I.; Ito, W.; Ishigooka, J.; Nishimura, K.; et al. The effect of short or long sleep duration on quality of life and depression: An internet-based survey in Japan. Sleep Med. 2020, 76, 80–85. [Google Scholar] [CrossRef]
- Lallukka, T.; Sivertsen, B.; Kronholm, E.; Bin, Y.S.; Øverland, S.; Glozier, N. Association of sleep duration and sleep quality with the physical, social, and emotional functioning among Australian adults. Sleep Health 2018, 4, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Zeitlhofer, J.; Schmeiser-Rieder, A.; Tribl, G.; Rosenberger, A.; Bolitschek, J.; Kapfhammer, G.; Saletu, B.; Katschnig, H.; Holzinger, B.; Popovic, R. Sleep and quality of life in the Austrian population. Acta Neurol. Scand. 2000, 102, 249–257. [Google Scholar] [CrossRef]
- Sasai, T.; Inoue, Y.; Komada, Y.; Nomura, T.; Matsuura, M.; Matsushima, E. Effects of insomnia and sleep medication on health-related quality of life. Sleep Med. 2010, 11, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Kido, K.; Hatakeyama, S.; Imai, A.; Yamamoto, H.; Tobisawa, Y.; Yoneyama, T.; Yoneyama, T.; Hashimoto, Y.; Koie, T.; Nakaji, S.; et al. Sleep Disturbance Has a Higher Impact on General and Mental Quality of Life Reduction than Nocturia: Results from the Community Health Survey in Japan. Eur. Urol. Focus 2019, 5, 1120–1126. [Google Scholar] [CrossRef] [PubMed]
- Marques, D.R.; Meia-Via, A.M.S.; da Silva, C.F.; Gomes, A.A. Associations between sleep quality and domains of quality of life in a non-clinical sample: Results from higher education students. Sleep Health 2017, 3, 348–356. [Google Scholar] [CrossRef]
- Darchia, N.; Oniani, N.; Sakhelashvili, I.; Supatashvili, M.; Basishvili, T.; Eliozishvili, M.; Maisuradze, L.; Cervena, K. Relationship between Sleep Disorders and Health Related Quality of Life-Results from the Georgia SOMNUS Study. Int. J. Environ. Res. Public Health 2018, 15, 1588. [Google Scholar] [CrossRef] [PubMed]
- Franquelo-Morales, P.; Sánchez-López, M.; Notario-Pacheco, B.; Miota-Ibarra, J.; Lahoz-García, N.; Gómez-Marcos, M.; Martínez-Vizcaíno, V. Association Between Health-Related Quality of Life, Obesity, Fitness, and Sleep Quality in Young Adults: The Cuenca Adult Study. Behav. Sleep Med. 2018, 16, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Mahirah, D.; Sauter, C.; Thach, T.Q.; Dunleavy, G.; Nazeha, N.; Christopoulos, G.; Soh, C.K.; Car, J. Factors associated with health-related quality of life in a working population in Singapore. Epidemiol. Health 2020, 42, e2020048. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.K.; Fiecas, M.; Afolalu, E.F.; Wolke, D. Changes in Sleep Duration, Quality, and Medication Use Are Prospectively Associated With Health and Well-being: Analysis of the UK Household Longitudinal Study. Sleep 2017, 40. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Mollayeva, T.; Thurairajah, P.; Burton, K.; Mollayeva, S.; Shapiro, C.M.; Colantonio, A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 25, 52–73. [Google Scholar] [CrossRef]
- Dewald, J.F.; Meijer, A.M.; Oort, F.J.; Kerkhof, G.A.; Bögels, S.M. The influence of sleep quality, sleep duration and sleepiness on school performance in children and adolescents: A meta-analytic review. Sleep Med. Rev. 2010, 14, 179–189. [Google Scholar] [CrossRef]
- Cappuccio, F.P.; D’Elia, L.; Strazzullo, P.; Miller, M.A. Quantity and quality of sleep and incidence of type 2 diabetes: A systematic review and meta-analysis. Diabetes Care 2010, 33, 414–420. [Google Scholar] [CrossRef]
- Pilcher, J.J.; Ginter, D.R.; Sadowsky, B. Sleep quality versus sleep quantity: Relationships between sleep and measures of health, well-being and sleepiness in college students. J. Psychosom. Res. 1997, 42, 583–596. [Google Scholar] [CrossRef]
- Hooper, D.; Coughlan, J.; Mullen, M.R. Equation modelling: Guidelines for determining model fit. Electron. J. Bus. Res. Methods 2008, 6, 53–60. [Google Scholar] [CrossRef]
- Markus, K.A. Principles and Practice of Structural Equation Modeling by Rex B. Kline; Taylor & Francis: Boca Raton, FL, USA, 2012. [Google Scholar]
- Ito, W.; Komada, Y.; Okajima, I.; Inoue, Y. Excessive daytime sleepiness in adults with possible attention deficit/hyperactivity disorder (ADHD): A web-based cross-sectional study. Sleep Med. 2017, 32, 4–9. [Google Scholar] [CrossRef]
- Flegal, K.M.; Graubard, B.I.; Williamson, D.F.; Gail, M.H. Excess deaths associated with underweight, overweight, and obesity. JAMA 2005, 293, 1861–1867. [Google Scholar] [CrossRef]
- Lefante, J.J., Jr.; Harmon, G.N.; Ashby, K.M.; Barnard, D.; Webber, L.S. Use of the SF-8 to assess health-related quality of life for a chronically ill, low-income population participating in the Central Louisiana Medication Access Program (CMAP). Qual. Life Res. 2005, 14, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Tokuda, Y.; Okubo, T.; Ohde, S.; Jacobs, J.; Takahashi, O.; Omata, F.; Yanai, H.; Hinohara, S.; Fukui, T. Assessing items on the SF-8 Japanese version for health-related quality of life: A psychometric analysis based on the nominal categories model of item response theory. Value Health 2009, 12, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Doi, Y.; Minowa, M.; Uchiyama, M.; Okawa, M.; Kim, K.; Shibui, K.; Kamei, Y. Psychometric assessment of subjective sleep quality using the Japanese version of the Pittsburgh Sleep Quality Index (PSQI-J) in psychiatric disordered and control subjects. Psychiatry Res. 2000, 97, 165–172. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Pub: Arlington, VA, USA, 2013. [Google Scholar]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders, 3rd ed.; (ICSD-3); American Academy of Sleep Medicine: Darien, IL, USA, 2014. [Google Scholar]
- Stevens, J.P. Applied Multivariate Statistics for the Social Sciences, 5th ed.; Routledge: New York, NY, USA, 2009. [Google Scholar] [CrossRef]
- Wang, C.; Bangdiwala, S.I.; Rangarajan, S.; Lear, S.A.; AlHabib, K.F.; Mohan, V.; Teo, K.; Poirier, P.; Tse, L.A.; Liu, Z.; et al. Association of estimated sleep duration and naps with mortality and cardiovascular events: A study of 116 632 people from 21 countries. Eur. Heart J. 2019, 40, 1620–1629. [Google Scholar] [CrossRef]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation Coefficients: Appropriate Use and Interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef] [PubMed]
- Westfall, P.H.; Henning, K.S.S. Understanding Advanced Statistical Methods, 1st ed.; Chapman and Hall/CRC: New York, NY, USA, 2013. [Google Scholar] [CrossRef]
- Sonnentag, S.; Binnewies, C.; Mojza, E.J. “Did you have a nice evening?” A day-level study on recovery experiences, sleep, and affect. J. Appl. Psychol. 2008, 93, 674–684. [Google Scholar] [CrossRef]
- Hülsheger, U.R.; Lang, J.W.; Depenbrock, F.; Fehrmann, C.; Zijlstra, F.R.; Alberts, H.J. The power of presence: The role of mindfulness at work for daily levels and change trajectories of psychological detachment and sleep quality. J. Appl. Psychol. 2014, 99, 1113–1128. [Google Scholar] [CrossRef]
- Schleupner, R.; Kühnel, J. Fueling Work Engagement: The Role of Sleep, Health, and Overtime. Front. Public Health 2021, 9, 592850. [Google Scholar] [CrossRef] [PubMed]
- Spielman, A.J.; Saskin, P.; Thorpy, M.J. Treatment of chronic insomnia by restriction of time in bed. Sleep 1987, 10, 45–56. [Google Scholar] [CrossRef]
- Edinger, J.D.; Means, M.K. Cognitive-behavioral therapy for primary insomnia. Clin. Psychol. Rev. 2005, 25, 539–558. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Germain, A.; Moul, D.E.; Franzen, P.L.; Brar, L.K.; Fletcher, M.E.; Begley, A.; Houck, P.R.; Mazumdar, S.; Reynolds, C.F., 3rd; et al. Efficacy of brief behavioral treatment for chronic insomnia in older adults. Arch. Intern. Med. 2011, 171, 887–895. [Google Scholar] [CrossRef]
- Miller, C.B.; Espie, C.A.; Epstein, D.R.; Friedman, L.; Morin, C.M.; Pigeon, W.R.; Spielman, A.J.; Kyle, S.D. The evidence base of sleep restriction therapy for treating insomnia disorder. Sleep Med. Rev. 2014, 18, 415–424. [Google Scholar] [CrossRef]
- Thorndike, F.P.; Ritterband, L.M.; Gonder-Frederick, L.A.; Lord, H.R.; Ingersoll, K.S.; Morin, C.M. A randomized controlled trial of an internet intervention for adults with insomnia: Effects on comorbid psychological and fatigue symptoms. J. Clin. Psychol. 2013, 69, 1078–1093. [Google Scholar] [CrossRef]
- Shimodera, S.; Watanabe, N.; Furukawa, T.A.; Katsuki, F.; Fujita, H.; Sasaki, M.; Perlis, M.L. Change in quality of life after brief behavioral therapy for insomnia in concurrent depression: Analysis of the effects of a randomized controlled trial. J. Clin. Sleep Med. 2014, 10, 433–439. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chen, X.; Gelaye, B.; Williams, M.A. Sleep characteristics and health-related quality of life among a national sample of American young adults: Assessment of possible health disparities. Qual. Life Res. 2014, 23, 613–625. [Google Scholar] [CrossRef]
- Ge, Y.; Xin, S.; Luan, D.; Zou, Z.; Liu, M.; Bai, X.; Gao, Q. Association of physical activity, sedentary time, and sleep duration on the health-related quality of life of college students in Northeast China. Health Qual. Life Outcomes 2019, 17, 124. [Google Scholar] [CrossRef] [PubMed]
- Do, Y.K.; Shin, E.; Bautista, M.A.; Foo, K. The associations between self-reported sleep duration and adolescent health outcomes: What is the role of time spent on Internet use? Sleep Med. 2013, 14, 195–200. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Age | - | ||||||||||||
| 2. Sex | 0.003 | - | |||||||||||
| 3. Categorized BMI | 0.127 * | −0.269 * | - | ||||||||||
| 4. Current smoker | 0.014 | −0.194 * | 0.056 * | - | |||||||||
| 5. Habitual alcohol consumption | 0.073 * | −0.238 * | 0.054 * | 0.158 * | - | ||||||||
| 6. Regular worker | −0.195 * | −0.442 * | 0.115 * | 0.158 * | 0.192 * | - | |||||||
| 7. Existence of currently treated diseases | 0.308 * | −0.023 | 0.121 * | −0.023 | 0.012 | −0.067 * | - | ||||||
| 8. Physical QOL (PCS) | −0.054 * | 0.000 | −0.065 * | −0.032 | 0.029 | 0.001 | −0.190 * | - | |||||
| 9. Mental QOL (MCS) | 0.242 * | −0.046 * | 0.066 * | −0.013 | 0.016 | −0.029 | 0.045 * | −0.045 * | - | ||||
| 10. Difficulty initiating sleep (C2 in PSQI) | −0.098 * | 0.101 * | −0.015 | 0.040 * | −0.042 * | −0.096 * | 0.025 | −0.132 * | −0.229 * | - | |||
| 11. Difficulty maintaining sleep and/or waking up earlier than desired (C5a in PSQI) | 0.107 * | 0.047 * | −0.008 | −0.014 | 0.043 * | −0.056 * | 0.098 * | −0.140 * | −0.166 * | 0.378 * | - | ||
| 12. Sleep quality (C1 in PSQI) | −0.103 * | 0.058 * | −0.005 | 0.034 | −0.017 | −0.008 | 0.022 | −0.254 * | −0.323 * | 0.374 * | 0.322 * | - | |
| 13. Habitual sleep duration (min) | −0.019 | 0.028 | −0.044 * | −0.044 * | −0.003 | −0.090 * | 0.010 | 0.058 * | 0.078 * | −0.008 | −0.008 | −0.209 * | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsui, K.; Yoshiike, T.; Nagao, K.; Utsumi, T.; Tsuru, A.; Otsuki, R.; Ayabe, N.; Hazumi, M.; Suzuki, M.; Saitoh, K.; et al. Association of Subjective Quality and Quantity of Sleep with Quality of Life among a General Population. Int. J. Environ. Res. Public Health 2021, 18, 12835. https://doi.org/10.3390/ijerph182312835
Matsui K, Yoshiike T, Nagao K, Utsumi T, Tsuru A, Otsuki R, Ayabe N, Hazumi M, Suzuki M, Saitoh K, et al. Association of Subjective Quality and Quantity of Sleep with Quality of Life among a General Population. International Journal of Environmental Research and Public Health. 2021; 18(23):12835. https://doi.org/10.3390/ijerph182312835
Chicago/Turabian StyleMatsui, Kentaro, Takuya Yoshiike, Kentaro Nagao, Tomohiro Utsumi, Ayumi Tsuru, Rei Otsuki, Naoko Ayabe, Megumi Hazumi, Masahiro Suzuki, Kaori Saitoh, and et al. 2021. "Association of Subjective Quality and Quantity of Sleep with Quality of Life among a General Population" International Journal of Environmental Research and Public Health 18, no. 23: 12835. https://doi.org/10.3390/ijerph182312835
APA StyleMatsui, K., Yoshiike, T., Nagao, K., Utsumi, T., Tsuru, A., Otsuki, R., Ayabe, N., Hazumi, M., Suzuki, M., Saitoh, K., Aritake-Okada, S., Inoue, Y., & Kuriyama, K. (2021). Association of Subjective Quality and Quantity of Sleep with Quality of Life among a General Population. International Journal of Environmental Research and Public Health, 18(23), 12835. https://doi.org/10.3390/ijerph182312835