
Dental Caries Prevalence and Experience (ICDAS II Criteria) of 5-, 12- and 15-Year-Old Children and Adolescents with an Immigrant Background in Greece, Compared with the Host Population: A Cross-Sectional Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Calibration
2.3. Clinical Examination
2.4. Questionnaire Information
- Sociodemographic characteristics: father’s and mother’s country of origin; years of stay in Greece of the father and the mother; country of student’s birth; gender of the student: male or female; location: urban or rural; father’s and mother’s level of education: (1) up to lower secondary, (2) upper secondary or non-university tertiary or (3) university.
- Dental health-related behaviours: (A) 5-year-old age group: is toothbrushing performed on the child’s teeth? (no/yes). If yes, who brushes your child’s teeth? (1) The child without adult supervision; (2) the child supervised by an adult; (3) an adult. How often is toothbrushing performed? (1) Occasionally; (2) once per day; (3) twice per day. Is toothpaste used during toothbrushing? (no/yes). If yes, what kind of toothpaste is used? (1) Child; (2) adult. Up to what age did your child use a baby bottle? (1) 18 months; (2) 3 years; (3) >3 years. Your child was fed milk with a baby bottle (1) before he/she went for sleep, while he/she was still awake or (2) in his/her bed while sleeping. Did you clean the child’s teeth after baby bottle use? (no/yes). (B) For the 12- and the 15-year-old age groups: Do you brush your teeth and, if yes, how often? (1) Never; (2) occasionally/when I remember it; (3) once per day; (4) twice per day.
- Dietary habits (for the 5-year-old age group): How often does your child consume the following: (1) sugary food, such as biscuits, cake and chocolate (rarely; 3–6 times per week; once per day; 2 or 3 times per day; >3 times per day); (2) sugary drinks such as packaged juice, chocolate milk and sugary milk (rarely; 3–6 times per week; once per day; 2 or 3 times per day; >3 times per day); (3) confectionary products, such as sugary chewing gums, lollipops and candies (rarely; 3–6 times per week; once per day; 2 or 3 times per day; >3 times per day).
2.5. Data Analysis
2.5.1. Calculation of the Caries Indices
2.5.2. Independent Variables Description
2.5.3. Statistical Analysis
3. Results
3.1. Descriptive Analysis (Immigrant Population)
3.2. Negative Binomial Regression Analysis (Immigrant Population)
3.3. Comparison with the Host Population
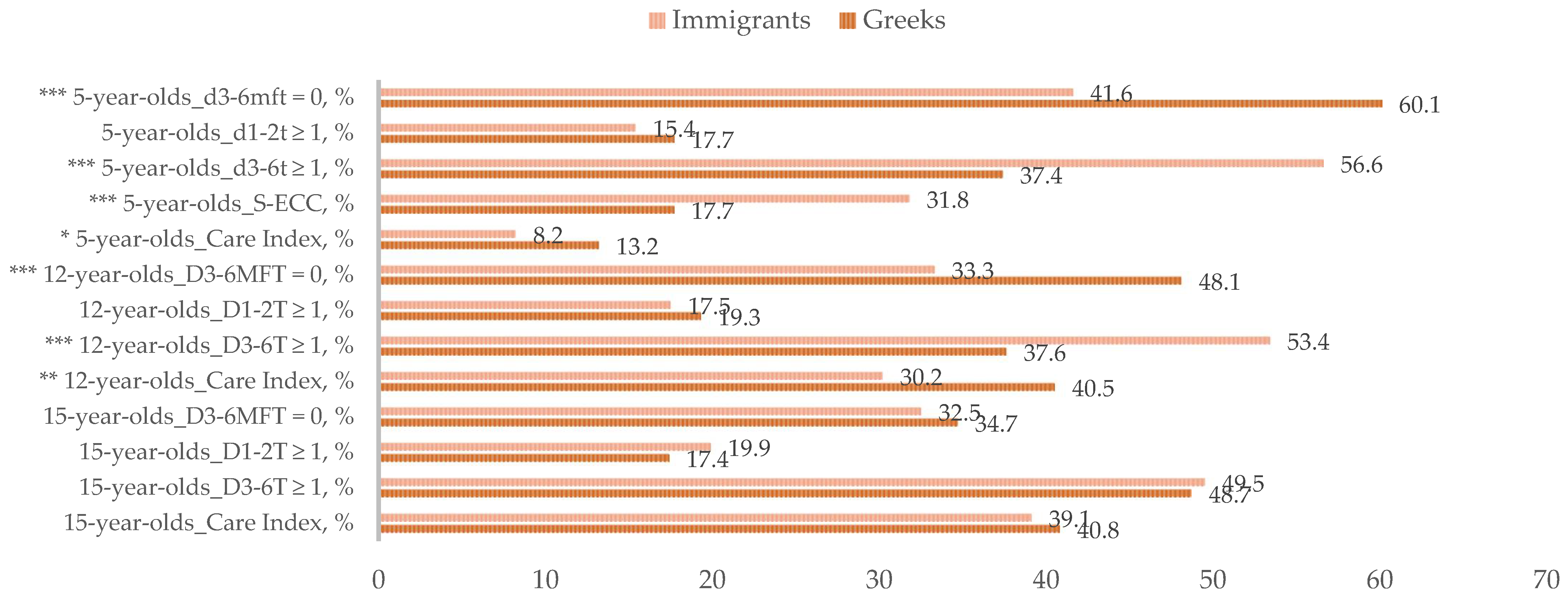
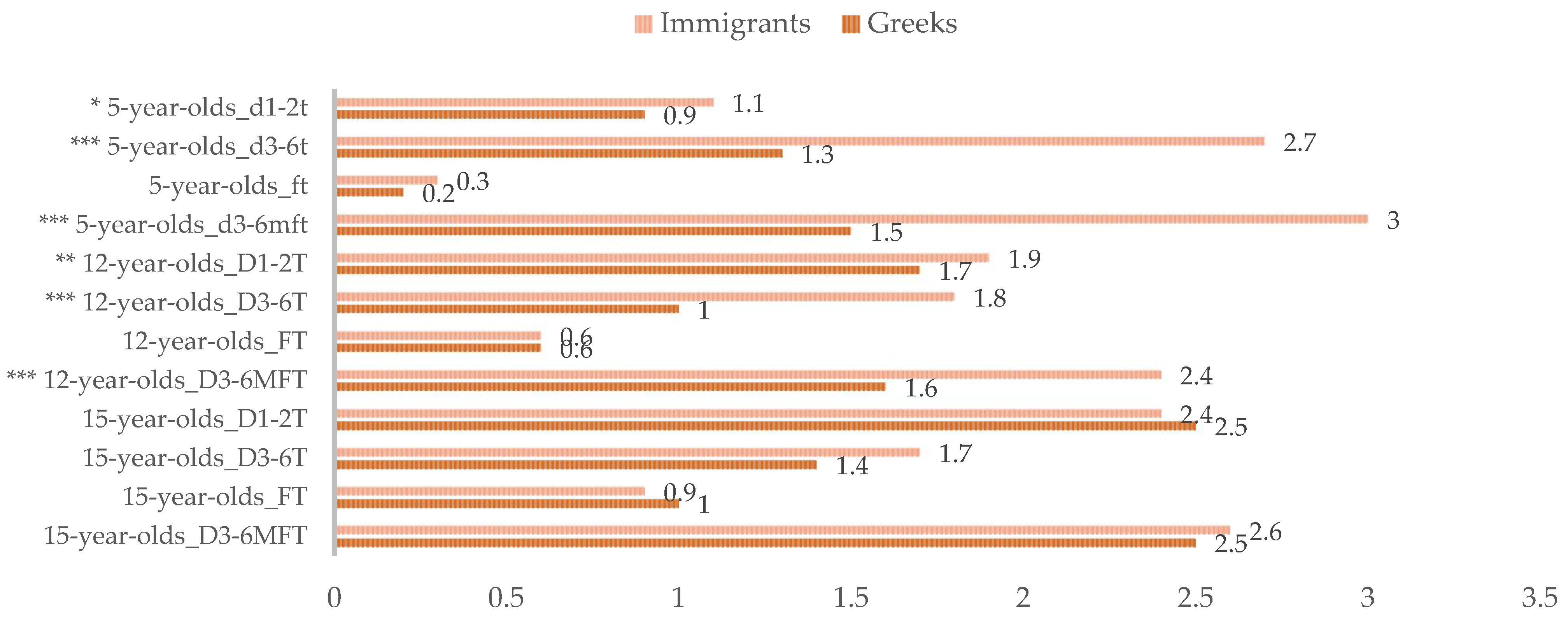
3.3.1. Caries Indices
3.3.2. Sociodemographic and Behavioural Parameters
3.3.3. Negative Binomial Regression Analysis (Total, Immigrant and Greek Population)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Greeks (n = 1222) | Immigrants (n = 267) | p-Value ‡ | |
|---|---|---|---|
| Nocturnal baby bottle feeding practice n † (%) | |||
| No | 1069 (90.8) | 212 (85.5) | 0.029 |
| Yes | 108 (9.2) | 36 (14.5) | |
References
- Cavounidis, J. The migration experience of Greece and the impact of the economic crisis on its migrant and native populations. Eur. J. Public Health 2018, 28 (Suppl. 5), 20–23. [Google Scholar] [CrossRef]
- Cavounidis, J. Migration and the economic and social landscape of Greece. South-East. Eur. J. Econ. 2013, 11, 59–78. [Google Scholar]
- Mattheoudakis, M.; Chatzidaki, A.; Maligkoudi, C. Heritage language classes and bilingual competence: The case of Albanian immigrant children in Greece. Int. J. Biling. Educ. Biling. 2017, 23, 1019–1035. [Google Scholar] [CrossRef]
- Dahlan, R.; Badri, P.; Saltaji, H.; Amin, M. Impact of acculturation on oral health among immigrants and ethnic minorities: A systematic review. PLoS ONE 2019, 28, e0212891. [Google Scholar] [CrossRef] [Green Version]
- Pabbla, A.; Duijster, D.; Grasveld, A.; Sekundo, C.; Agyemang, C.; van der Heijden, G. Oral health status, oral health behaviours and oral health care utilisation among migrants residing in Europe: A systematic review. J. Immigr. Minor. Health 2021, 23, 373–388. [Google Scholar] [CrossRef]
- Pitts, N. The impact of diagnostic criteria on estimates of prevalence, extent and severity of dental caries. In Dental Caries: The Disease and Its Clinical Management, 2nd ed.; Fejerskov, O., Kidd, E., Eds.; Blackwell Munksgaard Ltd.: Oxford, UK, 2008; pp. 147–159. ISBN 978-1-4051-5889-5. [Google Scholar]
- Kühnisch, J.; Berger, S.; Goddon, I.; Senkel, H.; Pitts, N.; Heinrich-Weltzien, R. Occlusal caries detection in permanent molars according to WHO basic methods, ICDAS II and laser fluorescence measurements. Community Dent. Oral Epidemiol. 2008, 36, 475–484. [Google Scholar] [CrossRef]
- Pitts, N.B.; Ekstrand, K.R. ICDAS Foundation. International Caries Detection and Assessment System (ICDAS) and its International Caries Classification and Management System (ICCMS)—Methods for staging of the caries process and enabling dentists to manage caries. Community Dent. Oral Epidemiol. 2013, 41, 41–52. [Google Scholar] [CrossRef]
- Assaf, A.V.; de Castro Meneghim, M.; Zanin, L.; Tengan, C.; Pereira, A.C. Effect of different diagnostic thresholds on dental caries calibration—A 12-month evaluation. Community Dent. Oral Epidemiol. 2006, 34, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Cvikl, B.; Haubenberger-Praml, G.; Drabo, P.; Hagmann, M.; Gruber, R.; Moritz, A.; Nell, A. Migration background is associated with caries in Viennese school children, even if parents have received a higher education. BMC Oral Health 2014, 14, 51. [Google Scholar] [CrossRef] [Green Version]
- Diamanti, I.; Berdouses, E.D.; Kavvadia, K.; Arapostathis, K.N.; Reppa, C.; Sifakaki, M.; Panagopoulou, O.; Polychronopoulou, A.; Oulis, C.J. Caries prevalence and caries experience (ICDAS II criteria) of 5-, 12- and 15-year-old Greek children in relation to socio-demographic risk indicators. Trends at the national level in a period of a decade. Eur. Arch. Paediatr. Dent. 2021, 22, 619–631. [Google Scholar] [CrossRef] [PubMed]
- Diamanti, I.; Berdouses, E.D.; Kavvadia, K.; Arapostathis, K.N.; Polychronopoulou, A.; Oulis, C.J. Oral hygiene and periodontal condition of 12- and 15-year-old Greek adolescents. Socio-behavioural risk indicators, self-rated oral health and changes in 10 years. Eur. J. Paediatr. Dent. 2021, 22, 98–106. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Oral Health Surveys: Basic Methods, 4th ed.; World Health Organization: Geneva, Switzerland, 1997; pp. 1–66. ISBN 9241544937. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Gatou, T.; Koletsi Kounari, H.; Mamai-Homata, E. Dental caries prevalence and treatment needs of 5- to 12-year-old children in relation to area-based income and immigrant background in Greece. Int. Dent. J. 2011, 61, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Topping, G.V.A.; Pitts, N.B. Clinical visual caries detection. Monogr. Oral Sci. 2009, 21, 15–41. [Google Scholar] [CrossRef]
- Drury, T.F.; Horowitz, A.M.; Ismail, A.I.; Maertens, M.P.; Rozier, R.G.; Selwitz, R.H. Diagnosing and Reporting Early Childhood Caries for Research Purposes: A Report of a Workshop Sponsored by the National Institute of Dental and Craniofacial Research, the Health Resources and Services Administration, and the Health Care Financing Administration. J. Public Health Dent. 1999, 59, 192–197. [Google Scholar] [CrossRef]
- Bratthall, D. Introducing the Significant Caries Index together with a proposal for a new global oral health goal for 12-year-olds. Int. Dent. J. 2000, 50, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Braga, M.M.; Oliveira, L.B.; Bonini, G.A.; Bönecker, M.; Mendes, F.M. Feasibility of the International Caries Detection and Assessment System (ICDAS-II) in epidemiological surveys and comparability with standard World Health Organization criteria. Caries Res. 2009, 43, 245–249. [Google Scholar] [CrossRef]
- Iranzo-Cortés, J.E.; Montiel-Company, J.M.; Almerich-Silla, J.M. Caries diagnosis: Agreement between WHO and ICDAS II criteria in epidemiological surveys. Community Dent. Health 2013, 30, 108–111. [Google Scholar]
- Greene, J.C.; Vermillion, J.R. The Simplified Oral Hygiene Index. J. Am. Dent. Assoc. 1964, 68, 7–13. [Google Scholar] [CrossRef]
- Mantonanaki, M.; Hatzichristos, T.; Koletsi-Kounari, H.; Papaioannou, W. Socio-demographic and area-related factors associated with the prevalence of caries among preschool children in Greece. Community Dent. Health 2017, 34, 112–117. [Google Scholar] [CrossRef]
- Delgado-Angulo, E.K.; Marcenes, W.; Harding, S.; Bernabé, E. Ethnicity, migration status and dental caries experience among adults in East London. Community Dent. Oral Epidemiol. 2018, 46, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Marcenes, W.; Muirhead, V.E.; Murray, S.; Redshaw, P.; Bennett, U.; Wright, D. Ethnic disparities in the oral health of three- to four-year-old children in East London. Br. Dent. J. 2013, 215, E4:1–E4:5. [Google Scholar] [CrossRef] [PubMed]
- Julihn, A.; Ekbom, A.; Modéer, T. Migration background: A risk factor for caries development during adolescence. Eur. J. Oral Sci. 2010, 118, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Bissar, A.R.; Oikonomou, C.; Koch, M.J.; Schulte, A.G. Dental health, received care, and treatment needs in 11- to 13-year-old children with immigrant background in Heidelberg, Germany. Int. J. Paediatr. Dent. 2007, 17, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Sundby, A.; Petersen, P.E. Oral health status in relation to ethnicity of children in the Municipality of Copenhagen, Denmark. Int. J. Paediatr. Dent. 2003, 13, 150–157. [Google Scholar] [CrossRef]
- Petersen, P.E. Changing oral health profiles of children in Central and Eastern Europe. Challenges for the 21st century. IC Dig. 2003, 2, 12–13. [Google Scholar]
- Hysi, D.; Caglar, E.; Droboniku, E.; Toti, C.; Kuscu, O.O. Dental caries experience among Albanian pre-school children: A national survey. Community Dent. Health 2017, 34, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Hysi, D.; Droboniku, E.; Toti, C. Caries experience and treatment needs among Albanian 12-year-olds. Community Dent. Health 2014, 31, 141–144. [Google Scholar]
- Oulis, C.J.; Tsinidou Vadiakas, G.; Mamai-Homata, E.; Polychronopoulou, A.; Athanasouli, T. Caries prevalence of 5, 12 and 15-year-old Greek children: A national pathfinder survey. Community Dent. Health. 2012, 29, 29–32. [Google Scholar] [PubMed]
- Al-Haj Ali, S.N.; Alshabaan, S.H. What do parents know about oral health and care for preschool children in the central region of Saudi Arabia? Pesqui. Bras. Odontopediatria Clin. Integr. 2020, 20, e0103. [Google Scholar] [CrossRef]
- Skeie, M.S.; Klock, K.S. Dental caries prevention strategies among children and adolescents with immigrant or low socioeconomic backgrounds- do they work? A systematic review. BMC Oral Health 2018, 18, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- André Kramer, A.C.; Petzold, M.; Hakeberg, M.; Östberg, A.L. Multiple Socioeconomic Factors and Dental Caries in Swedish Children and Adolescents. Caries Res. 2018, 52, 42–50. [Google Scholar] [CrossRef]
- Vadiakas, G.; Oulis, C.J.; Tsinidou, K.; Mamai-Homata, E.; Polychronopoulou, A. Socio-behavioural factors influencing oral health of 12- and 15-year-old Greek adolescents. A national pathfinder survey. Eur. Arch. Paediatr. Dent. 2011, 12, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Mock-Muñoz de Luna, C.J.; Vitus, K.; Torslev, M.K.; Krasnik, A.; Jervelund, S.S. Ethnic inequalities in child and adolescent health in the Scandinavian welfare states: The role of parental socioeconomic status—A systematic review. Scand. J. Public Health 2019, 47, 679–689. [Google Scholar] [CrossRef] [PubMed]
- Christensen, L.B.; Twetman, S.; Sundby, A. Oral health in children and adolescents with different socio-cultural and socio-economic backgrounds. Acta Odontol. Scand. 2010, 68, 34–42. [Google Scholar] [CrossRef]
- Jacobsson, B.; Koch, G.; Magnusson, T.; Hugoson, A. Oral health in young individuals with foreign and Swedish backgrounds—A ten-year perspective. Eur. Arch. Paediatr. Dent. 2011, 12, 151–158. [Google Scholar] [CrossRef]
- Almerich-Silla, J.M.; Montiel-Company, J.M. Influence of immigration and other factors on caries in 12- and 15-yr-old children. Eur. J. Oral. Sci. 2007, 115, 378–383. [Google Scholar] [CrossRef]
- Rouxel, P.; Chandola, T. Socioeconomic and ethnic inequalities in oral health among children and adolescents living in England, Wales and Northern Ireland. Community Dent. Oral Epidemiol. 2018, 46, 426–434. [Google Scholar] [CrossRef] [Green Version]
- West, P. Health inequalities in the early years: Is there equalisation in youth? Soc. Sci. Med. 1997, 44, 833–858. [Google Scholar] [CrossRef]
- van der Tas, J.T.; Kragt, L.; Elfrink, M.E.C.; Bertens, L.C.M.; Jaddoe, V.W.V.; Moll, H.A.; Ongkosuwito, E.M.; Wolvius, E.B. Social inequalities and dental caries in six-year-old children from the Netherlands. J. Dent. 2017, 62, 18–24. [Google Scholar] [CrossRef]
- Verrips, G.H.; Kalsbeek, H.; Eijkman, M.A. Ethnicity and maternal education as risk indicators for dental caries, and the role of dental behavior. Community Dent. Oral Epidemiol. 1993, 21, 209–214. [Google Scholar] [CrossRef] [PubMed]
| n† | d3–6mft = 0 n (%) | d1–6mft = 0 n (%) | d1–2t ≥ 1 n (%) | d3–6t ≥ 1 n (%) | S-ECC n (%) | d1–2t (±SD) | d3–6mft (±SD) | d3–6t (±SD) | mt (±SD) | ft (±SD) | d3–6mfs (±SD) | CI n (%) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Area of residence | |||||||||||||
| Rural | 70 | 33 (47.1) | 20 (28.6) | 13 (18.6) | 34 (48.6) | 24 (34.3) | 1.2 (1.6) | 2.8 (4.0) | 2.4 (4.0) | 0.1 (0.8) | 0.4 (1.2) | 5.2 (8.8) | 10 (14.7) |
| Urban | 197 | 78 (39.6) | 50 (25.4) | 28 (14.2) | 117 (59.4) | 61 (31.0) | 1.0 (1.5) | 3.1 (3.7) | 2.8 (3.6) | 0.0 (0.1) | 0.2 (1.1) | 4.9 (7.6) | 12 (6.2) |
| Gender | |||||||||||||
| Male | 137 | 56 (40.9) | 38 (27.7) | 18 (13.1) | 80 (58.4) | 43 (31.4) | 1.1 (1.6) | 3.2 (4.1) | 3.0 (3.9) | 0.0 (0.0) | 0.2 (1.1) | 5.5 (8.9) | 6 (4.6) * |
| Female | 130 | 55 (42.3) | 32 (24.6) | 23 (17.7) | 71 (54.6) | 42 (32.3) | 1.1 (1.5) | 2.8 (3.5) | 2.4 (3.4) | 0.1 (0.6) | 0.4 (1.2) | 4.5 (6.6) | 16 (12.2) |
| Father’s education | |||||||||||||
| ≤Lower secondary | 98 | 35 (35.7) | 21 (21.4) | 14 (14.3) | 61 (62.2) | 39 (39.8) * | 1.1 (1.4) | 3.5 (4.3) | 3.4 (4.2) | 0.0 (0.1) | 0.1 (0.5) | 6.1 (8.9) | 6 (5.9) |
| Upper secondary or non-university tertiary | 120 | 52 (43.3) | 34 (28.3) | 18 (15.0) | 65 (54.2) | 31 (25.8) | 1.1 (1.7) | 2.6 (3.3) | 2.2 (3.2) | 0.1 (0.6) | 0.4 (1.3) | 4.0 (6.5) | 13 (11.0) |
| University | 31 | 18 (58.1) | 13 (42.0) | 5 (16.1) | 13 (41.9) | 7 (22.6) | 1.0 (1.4) | 2.1 (3.4) | 1.7 (2.3) | 0.0 (0.0) | 0.4 (2.0) | 4.1 (9.1) | 2 (6.9) |
| Mother’s education | |||||||||||||
| ≤Lower secondary | 89 | 33 (37.1) | 23 (25.8) | 10 (11.2) | 54 (60.7) | 37 (41.6) * | 1.0 (1.4) | 3.7 (4.4) | 3.6 (4.4) | 0.1 (0.7) | 0.1 (0.6) | 6.0 (8.6) | 6 (6.6) |
| Upper secondary or non-university tertiary | 119 | 53 (44.5) | 36 (30.3) | 17 (14.3) | 64 (53.8) | 31 (26.1) | 1.1 (1.7) | 2.4 (3.2) | 2.2 (3.1) | 0.0 (0.0) | 0.2 (1.0) | 4.1 (6.6) | 10 (8.5) |
| University | 43 | 21 (48.8) | 10 (23.3) | 11 (25.6) | 21 (48.8) | 8 (18.6) | 1.3 (1.7) | 2.2 (3.4) | 1.7 (2.6) | 0.0 (0.0) | 0.6 (2.1) | 4.3 (9.2) | 5 (12.5) |
| Total | 267 | 111 (41.6) | 70 (26.2) | 41 (15.4) | 151 (56.6) | 85 (31.8) | 1.1 (1.6) | 3.0 (3.8) | 2.7 (3.9) | 0.0 (0.4) | 0.3 (1.1) | 5.0 (7.9) | 22 (8.2) |
| n† | D3–6MFT = 0 n (%) | D1–6MFT = 0 n (%) | D1–2T ≥ 1 n (%) | D3–6T ≥ 1 n (%) | D1–2T (±SD) | D3–6MFT (±SD) | D3–6T (±SD) | MT (±SD) | FT (±SD) | D3–6MFS (±SD) | CI n (%) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Area of residence | ||||||||||||
| Rural | 66 | 21 (31.8) | 8 (12.5) | 13 (19.7) | 34 (51.5) | 2.1 (2.7) | 2.7 (2.8) | 1.8 (2.6) | 0.1 (0.2) | 0.6 (1.2) | 4.5 (5.7) | 24 (35.7) |
| Urban | 168 | 57 (33.9) | 29 (17.4) | 28 (16.7) | 91 (54.2) | 1.8 (1.7) | 2.4 (2.4) | 1.7 (2.3) | 0.0 (0.1) | 0.6 (1.2) | 3.3 (3.7) | 47 (28.0) |
| Gender | ||||||||||||
| Male | 114 | 42 (36.8) | 20 (17.7) | 22 (19.3) | 56 (49.1) | 1.6 (1.8) | 2.2 (2.4) | 1.6 (2.3) | 0.0 (0.0) | 0.5 (1.1) | 3.2 (4.0) | 33 (29.3) |
| Female | 118 | 35 (29.7) | 16 (13.8) | 19 (16.1) | 68 (57.6) | 2.1 (2.3) | 2.7 (2.6) | 1.9 (2.4) | 0.0 (0.2) | 0.7 (1.3) | 4.0 (4.7) | 37 (31.2) |
| Father’s education | ||||||||||||
| ≤Lower secondary | 107 | 25 (23.4) * | 7 (6.7) * | 18 (16.8) | 68 (63.6) * | 1.9 (1.8) | 3.1 (2.8) * | 2.4 (2.7) * | 0.0 (0.1) | 0.7 (1.3) | 4.8 (5.3) * | 28 (26.6) |
| Upper secondary or non-university tertiary | 86 | 35 (40.7) | 18 (20.9) | 17 (19.8) | 40 (46.5) | 2.0 (2.4) | 2.0 (2.2) | 1.3 (1.8) | 0.0 (0.2) | 0.6 (1.2) | 2.7 (3.3) | 28 (32.3) |
| University | 36 | 16 (44.4) | 11 (30.6) | 5 (13.9) | 15 (41.7) | 1.5 (1.9) | 1.6 (1.8) | 1.0 (1.6) | 0.0 (0.0) | 0.5 (1.2) | 2.1 (2.2) | 14 (37.9) |
| Mother’s education | ||||||||||||
| ≤Lower secondary | 108 | 24 (22.2) * | 9 (8.6) * | 15 (13.9) | 69 (63.9) * | 1.8 (1.9) | 3.1 (2.7) * | 2.3 (2.7) * | 0.0 (0.2) | 0.6 (1.2) | 4.9 (5.2) * | 32 (29.2) |
| Upper secondary or non-university tertiary | 83 | 33 (39.8) | 13 (15.7) | 20 (24.1) | 41 (49.4) | 2.3 (2.4) | 2.0 (2.2) | 1.4 (1.8) | 0.0 (0.1) | 0.7 (1.2) | 2.7 (3.3) | 20 (24.5) |
| University | 39 | 20 (51.3) | 14 (35.9) | 6 (15.4) | 13 (33.3) | 1.4 (1.7) | 1.5 (2.0) | 0.9 (1.7) | 0.0 (0.0) | 0.5 (1.2) | 2.0 (2.5) | 19 (47.8) |
| Total | 234 | 78 (33.3) | 37 (16.0) | 41 (17.5) | 125 (53.4) | 1.9 (2.1) | 2.4 (2.5) | 1.8 (2.4) | 0.0 (0.1) | 0.6 (1.2) | 3.6 (4.4) | 71 (30.2) |
| n† |
D3–6MFT = 0
n (%) |
D1–6MFT = 0 n (%) |
D1–2T ≥ 1
n (%) |
D3–6T ≥ 1
n (%) |
D1–2T
(±SD) |
D3–6MFT
(±SD) |
D3–6T
(±SD) |
MT
(±SD) |
FT
(±SD) |
D3–6MFS
(±SD) |
CI
n (%) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Area of residence | ||||||||||||
| Rural | 40 | 13 (32.5) | 3 (7.5) | 10 (25.0) | 18 (45.0) | 2.8 (4.0) | 2.8 (2.9) | 1.7 (2.4) | 0.1 (0.3) | 1.1 (1.7) | 3.7 (4.1) | 19 (47.5) |
| Urban | 166 | 54 (32.5) | 23 (13.9) | 31 (18.7) | 84 (50.6) | 2.3 (2.7) | 2.5 (2.8) | 1.6 (2.4) | 0.0 (0.2) | 0.9 (1.5) | 3.7 (5.0) | 61 (37.0) |
| Gender | ||||||||||||
| Male | 87 | 30 (34.5) | 15 (17.2) | 15 (17.2) | 44 (50.6) | 2.0 (2.6) | 2.3 (2.8) | 1.7 (2.5) | 0.1 (0.2) | 0.6 (1.1) | 3.5 (5.0) | 29 (32.8) |
| Female | 119 | 37 (31.1) | 11 (9.2) | 26 (21.8) | 58 (48.7) | 2.7 (3.2) | 2.7 (2.9) | 1.6 (2.4) | 0.0 (0.2) | 1.1 (1.8) | 3.9 (4.6) | 52 (43.4) |
| Father’s education | ||||||||||||
| ≤Lower secondary | 52 | 17 (32.7) | 5 (9.6) | 12 (23.1) | 30 (57.7) * | 2.7 (3.2) | 2.5 (2.9) | 1.8 (2.6) | 0.1 (0.3) | 0.7 (1.4) | 3.6 (4.4) | 14 (27.8) |
| Upper secondary or non-university tertiary | 101 | 30 (29.7) | 15 (14.9) | 15 (14.9) | 53 (52.5) | 2.2 (2.8) | 2.8 (2.9) | 1.8 (2.5) | 0.0 (0.2) | 1.0 (1.5) | 4.1 (5.3) | 39 (39.1) |
| University | 49 | 19 (38.8) | 6 (12.2) | 13 (26.5) | 17 (34.7) | 2.6 (3.2) | 2.2 (2.8) | 1.3 (2.2) | 0.0 (0.0) | 1.0 (1.7) | 3.1 (4.3) | 26 (52.8) |
| Mother’s education | ||||||||||||
| ≤Lower secondary | 55 | 13 (23.6) | 4 (7.3) | 9 (16.4) | 33 (60.0) * | 2.2 (2.7) | 3.2 (3.0) * | 2.1 (2.8) * | 0.1 (0.3) | 1.1 (1.6) | 4.7 (4.6) * | 20 (37.2) |
| Upper secondary or non-university tertiary | 80 | 26 (32.5) | 11 (13.8) | 15 (18.8) | 44 (55.0) | 2.5 (3.0) | 2.7 (3.0) | 1.9 (2.5) | 0.0 (0.2) | 0.9 (1.6) | 4.3 (5.7) | 25 (31.1) |
| University | 70 | 28 (40.0) | 11 (15.7) | 17 (24.3) | 24 (34.3) | 2.4 (3.2) | 1.9 (2.4) | 1.0 (1.9) | 0.0 (0.1) | 0.8 (1.4) | 2.3 (3.4) | 36 (52.1) |
| Total | 206 | 67 (32.5) | 26 (12.6) | 41 (19.9) | 102 (49.5) | 2.4 (3.0) | 2.6 (2.9) | 1.7 (2.4) | 0.0 (0.2) | 0.9 (1.5) | 3.7 (4.8) | 81 (39.1) |
| Independent Variable | Independent Variable | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Mother’s Education Level (Ref. University) | Father’s Education Level (Ref. University) | ||||||||
| Dependent variable | d3–6mfs | 5-year-olds (n = 248) | 5-year-olds (n = 248) | ||||||
| B | IRR † | 95% C.I. | p-Value | B | IRR ‡ | 95% C.I. | p-Value | ||
| −0.001 | 1.00 1 | (0.48. 2.07) | 0.998 | −0.002 | 1.00 1 | (0.42. 2.40) | 0.997 | ||
| 0.216 | 1.24 2 | (0.55. 2.80) | 0.604 | 0.291 | 1.34 2 | (0.51. 3.52) | 0.556 | ||
| Dependent variable | D3–6MFS | 12-year-olds (n = 227) | 12-year-olds (n = 227) | ||||||
| B | IRR † | 95% C.I. | p-Value | B | IRR ‡ | 95% C.I. | p-Value | ||
| 0.262 | 1.30 1 | (0.76. 2.22) | 0.337 | 0.090 | 1.09 1 | (0.67. 1.79) | 0.719 | ||
| 0.614 | 1.85 2 | (1.08. 3.17) | 0.025 | 0.444 | 1.56 2 | (0.96. 2.55) | 0.076 | ||
| Dependent variable | D3–6MFS | 15-year-olds (n = 202) | 15-year-olds (n = 202) | ||||||
| B | IRR † | 95% C.I. | p-Value | B | IRR ‡ | 95% C.I. | p-Value | ||
| 0.631 | 1.88 1 | (1.20. 2.95) | 0.006 | 0.034 | 1.04 1 | (0.64. 1.69) | 0.890 | ||
| 0.877 | 2.40 2 | (1.56. 3.71) | <0.001 | −0.281 | 0.76 2 | (0.46. 1.25) | 0.276 | ||
| 5-Year-Olds | 12-Year-Olds | 15-Year-Olds | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Greeks | Immigrants | p-Value ‡ | Greeks | Immigrants | p-Value ‡ | Greeks | Immigrants | p-Value ‡ | |
| (n = 1222) | (n = 267) | (n = 1252) | (n = 234) | (n = 1228) | (n = 206) | ||||
| Area of residence n † (%) | |||||||||
| Rural | 463 (37.9) | 70 (26.2) | <0.001 | 426 (34.0) | 66 (28.2) | 0.096 | 438 (35.7) | 40 (19.4) | <0.001 |
| Urban | 759 (62.1) | 197 (73.8) | 826 (66.0) | 168 (71.8) | 790 (64.3) | 166 (80.6) | |||
| Gender n † (%) | |||||||||
| Male | 595 (48.7) | 137 (51.3) | 0.458 | 612 (49.2) | 114 (49.1) | 1.000 | 569 (46.4) | 87 (42.2) | 0.29 |
| Female | 627 (51.3) | 130 (48.7) | 631 (50.8) | 118 (50.9) | 658 (53.6) | 119 (57.8) | |||
| Father’s education n † (%) | |||||||||
| ≤Lower secondary | 193 (16.0) | 98 (39.4) | 286 (22.9) | 107 (46.7) | 276 (22.5) | 52 (25.7) | |||
| Upper secondary/ | 738 (61.3) | 120 (48.2) | <0.001 | 580 (46.5) | 86 (37.6) | <0.001 | 545 (44.5) | 101 (50.0) | 0.049 |
| non-university tertiary | |||||||||
| University | 272 (22.6) | 31 (12.4) | 381 (30.6) | 36 (15.7) | 403 (32.9) | 49 (24.3) | |||
| Mother’s education n † (%) | |||||||||
| ≤Lower secondary | 94 (7.8) | 89 (35.5) | 236 (18.9) | 108 (47.0) | 213 (17.4) | 55 (26.8) | |||
| Upper secondary/ | 774 (64.0) | 119 (47.4) | <0.001 | 612 (49.1) | 83 (36.1) | <0.001 | 590 (48.1) | 80 (39.0) | 0.003 |
| non-university tertiary | |||||||||
| University | 342 (28.3) | 43 (17.1) | 399 (32.0) | 39 (17.0) | 423 (34.5) | 70 (34.1) | |||
| DI-S score n † (%) | |||||||||
| Good (0.0–0.6) | 671 (54.9) | 93 (34.8) | <0.001 | 549 (43.9) | 79 (33.8) | 0.002 | 698 (56.9) | 103 (50.0) | 0.173 |
| Fair (0.7–1.8) | 525 (43.0) | 163 (61.1) | 647 (51.7) | 135 (57.7) | 494 (40.3) | 197 (47.1) | |||
| Poor (1.9–3.0) | 26 (2.1) | 11 (4.1) | 55 (4.4) | 20 (8.5) | 35 (2.9) | 6 (2.9) | |||
| Toothbrushing frequency n † (%) | |||||||||
| No/occasionally | 219 (17.9) | 51 (19.1) | 0.797 | 147 (11.8) | 42 (18.0) | 0.033 | 138 (11.3) | 19 (9.2) | 0.643 |
| Once per day | 741 (60.6) | 156 (58.4) | 537 (43.0) | 96 (41.0) | 433 (35.3) | 77 (37.4) | |||
| Twice per day | 262 (21.4) | 60 (22.5) | 565 (45.2) | 96 (41.0) | 655 (53.4) | 110 (53.4) | |||
| Subject who performs the toothbrushing n † (%) | |||||||||
| The child, unsupervised | 195 (16.3) | 65 (25.4) | |||||||
| The child, supervised by an adult | 772 (64.4) | 168 (65.6) | <0.001 | N/A | N/A | ||||
| An adult | 231 (19.3) | 23 (9.0) | |||||||
| Frequency of consumption of sugary food (e.g., biscuits, cake, chocolate) n † (%) | |||||||||
| ≤Once per day | 1048 (88.7) | 220 (86.3) | |||||||
| ≥Twice per day | 134 (11.3) | 35 (13.7) | 0.285 | Ν/A | Ν/A | ||||
| Frequency of consumption of confectionery products (e.g., lollipops, sugary chewing gums, candies) n † (%) | |||||||||
| ≤Once per day | 1166 (98.0) | 240 (93.4) | <0.001 | N/A | N/A | ||||
| ≥Twice per day | 23 (2.0) | 17 (6.6) | |||||||
| Frequency of consumption of sugar-sweetened beverages (e.g., packaged juices, chocolate milk, sugary milk n † (%) | |||||||||
| ≤Once per day | 1142 (96.2) | 234 (90.3) | <0.001 | N/A | N/A | ||||
| ≥Twice per day | 46 (3.8) | 25 (9.7) | |||||||
| Dependent Variable | Independent Variable | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 5-year-olds | |||||||||
| Crude (n = 1489) | Adjusted (n = 1450) | ||||||||
| d3–6mfs | Ethnic background (ref. Greek) | B | IRR | 95% C.I. | p-Value | B | IRR † | 95% C.I. | p-Value |
| 0.792 | 2.21 1 | (1.77. 2.76) | <0.001 | 0.479 | 1.61 1 | (1.22. 2.14) | 0.001 | ||
| 12-year-olds | |||||||||
| Crude (n = 1486) | Adjusted (n = 1460) | ||||||||
| D3–6MFS | Ethnic background (ref. Greek) | B | IRR | 95% C.I. | p-Value | B | IRR † | 95% C.I. | p-Value |
| 0.494 | 1.64 1 | (1.37. 1.95) | <0.001 | 0.241 | 1.27 1 | (1.07. 1.51) | 0.006 | ||
| 15-year-olds | |||||||||
| Crude (n = 1434) | Adjusted (n = 1422) | ||||||||
| D3–6MFS | Ethnic background (ref. Greek) | B | IRR | 95% C.I. | p-Value | B | IRR † | 95% C.I. | p-Value |
| 0.089 | 1.09 1 | (0.90. 1.32) | 0.357 | 0.099 | 1.10 1 | (0.90. 1.35) | 0.331 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diamanti, I.; Berdouses, E.D.; Kavvadia, K.; Arapostathis, K.N.; Polychronopoulou, A.; Oulis, C.J. Dental Caries Prevalence and Experience (ICDAS II Criteria) of 5-, 12- and 15-Year-Old Children and Adolescents with an Immigrant Background in Greece, Compared with the Host Population: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 14. https://doi.org/10.3390/ijerph19010014
Diamanti I, Berdouses ED, Kavvadia K, Arapostathis KN, Polychronopoulou A, Oulis CJ. Dental Caries Prevalence and Experience (ICDAS II Criteria) of 5-, 12- and 15-Year-Old Children and Adolescents with an Immigrant Background in Greece, Compared with the Host Population: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(1):14. https://doi.org/10.3390/ijerph19010014
Chicago/Turabian StyleDiamanti, Iliana, Elias D. Berdouses, Katerina Kavvadia, Konstantinos N. Arapostathis, Argy Polychronopoulou, and Constantine J. Oulis. 2022. "Dental Caries Prevalence and Experience (ICDAS II Criteria) of 5-, 12- and 15-Year-Old Children and Adolescents with an Immigrant Background in Greece, Compared with the Host Population: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 1: 14. https://doi.org/10.3390/ijerph19010014
APA StyleDiamanti, I., Berdouses, E. D., Kavvadia, K., Arapostathis, K. N., Polychronopoulou, A., & Oulis, C. J. (2022). Dental Caries Prevalence and Experience (ICDAS II Criteria) of 5-, 12- and 15-Year-Old Children and Adolescents with an Immigrant Background in Greece, Compared with the Host Population: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(1), 14. https://doi.org/10.3390/ijerph19010014