
Risk of Mortality and Readmission among Patients with Pelvic Fracture and Urinary Tract Infection: A Population-Based Cohort Study

 , ,
, ,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
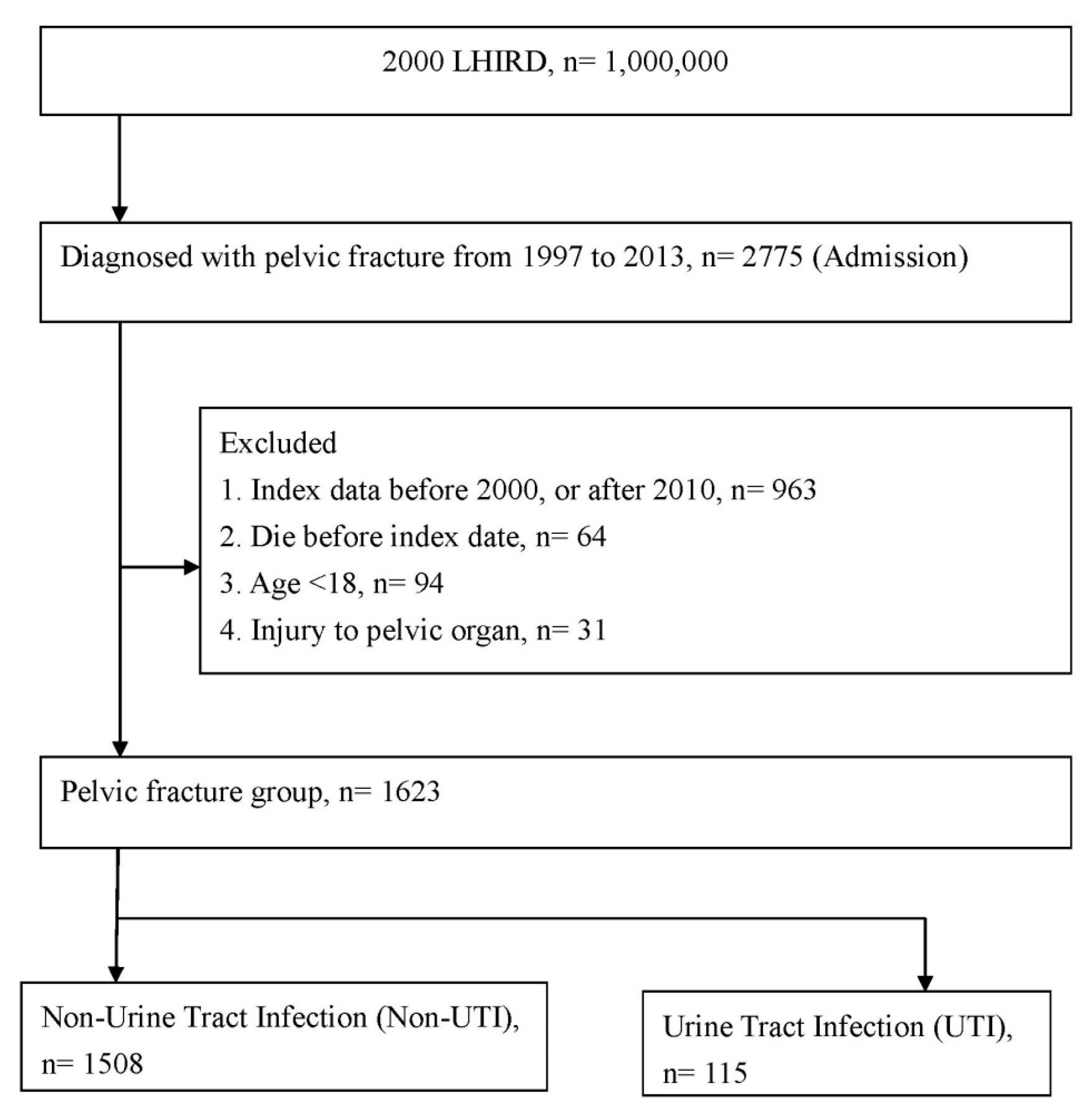
2.2. Study Population
2.3. Characteristics, Comorbidities, and Study Outcomes
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Study Patients
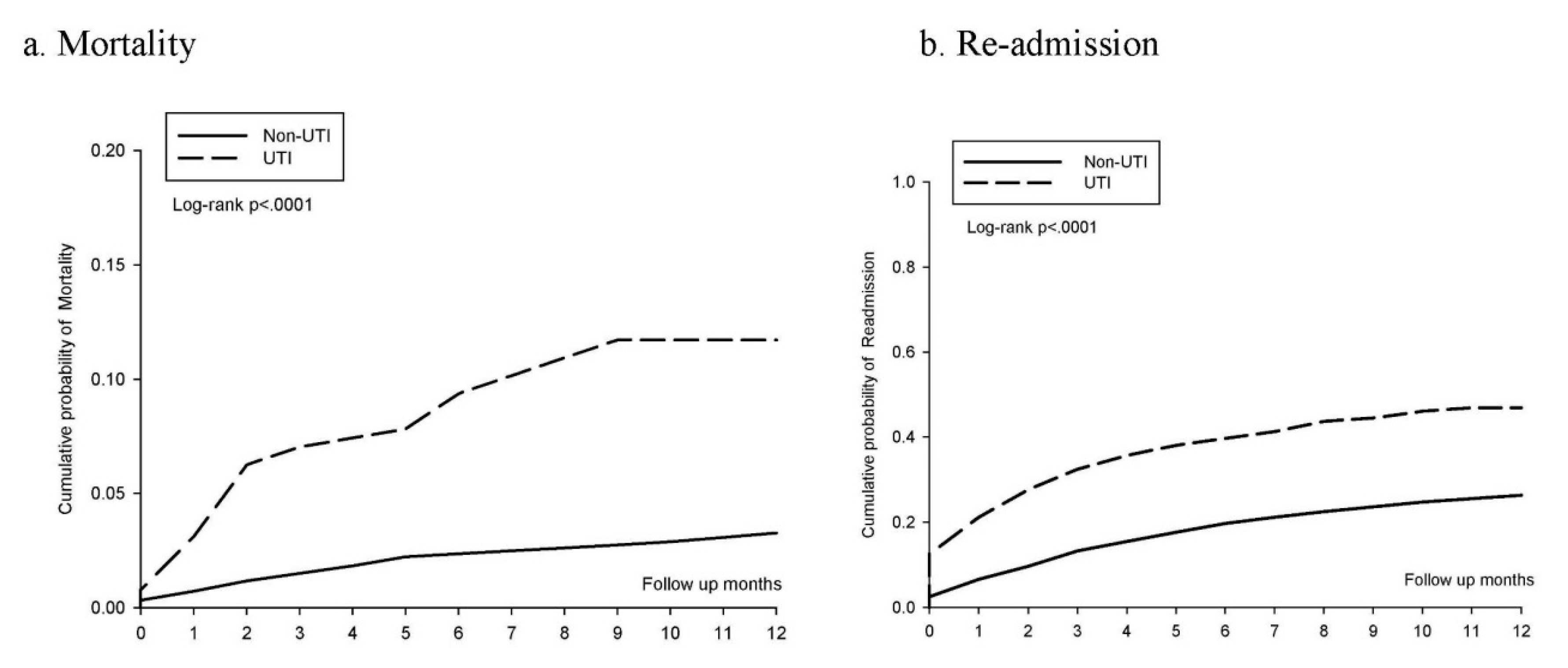
3.2. Risk of UTI after Exposure to Pelvic Fracture
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shim, H.; Jang, J.Y.; Kim, J.W.; Ryu, H.; Jung, P.Y.; Kim, S.; Kwon, H.Y.; Kim, K.M.; Chung, H.; Bae, K.S. Effectiveness and postoperative wound infection of preperitoneal pelvic packing in patients with hemodynamic instability caused by pelvic fracture. PLoS ONE 2018, 13, e0206991. [Google Scholar] [CrossRef] [PubMed]
- Jerrard, D.A. Pelvic fractures. Emerg. Med. Clin. N. Am. 1993, 11, 147–163. [Google Scholar] [CrossRef]
- Kobziff, L. Traumatic pelvic fractures. Orthop. Nurs. 2006, 25, 235–241. [Google Scholar] [CrossRef]
- Rodrigues, I. To log-roll or not to log-roll—that is the question! A review of the use of the log-roll for patients with pelvic fractures. Int. J. Orthop. Trauma Nurs. 2017, 27, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Flint, L.; Cryer, H.G. Pelvic fracture: The last 50 years. J. Trauma 2010, 69, 483–488. [Google Scholar] [CrossRef]
- Wong, J.M.; Bucknill, A. Fractures of the pelvic ring. Injury 2017, 48, 795–802. [Google Scholar] [CrossRef]
- Wiley, M.; Black, S.; Martin, C.; Barnwell, J.; Starr, A.; Sathy, A. Complications after pelvic arteriography in patients with pelvic ring disruptions. J. Am. Acad. Orthop. Surg. 2018, 26, 765–772. [Google Scholar] [CrossRef]
- Lee, M.J.; Wright, A.; Cline, M.; Mazza, M.B.; Alves, T.; Chong, S. Pelvic fractures and associated genitourinary and vascular injuries: A multisystem review of pelvic trauma. AJR Am. J. Roentgenol. 2019, 213, 1297–1306. [Google Scholar] [CrossRef] [PubMed]
- Malik, A.T.; Quatman, C.E.; Phieffer, L.S.; Jain, N.; Khan, S.N.; Ly, T.V. 30-day adverse events, length of stay and re-admissions following surgical management of pelvic/acetabular fractures. J. Clin. Orthop. Trauma 2019, 10, 890–895. [Google Scholar] [CrossRef]
- Eid, A.M. Early urinary complications of fractures of the pelvis. Arch. Orthop. Trauma Surg. 1982, 100, 99–106. [Google Scholar] [CrossRef]
- Laupland, K.B.; Bagshaw, S.M.; Gregson, D.B.; Kirkpatrick, A.W.; Ross, T.; Church, D.L. Intensive care unit-acquired urinary tract infections in a regional critical care system. Crit. Care 2005, 9, R60–R65. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.H.; Chou, Y.H.; Yeh, H.W.; Huang, J.Y.; Yang, S.F.; Yeh, C.B. Risk of cancer after lower urinary tract infection: A population-based cohort study. Int. J. Environ. Res. Public Health 2019, 16, 390. [Google Scholar] [CrossRef] [PubMed]
- Foster, A.L.; Moriarty, T.F.; Zalavras, C.; Morgenstern, M.; Jaiprakash, A.; Crawford, R.; Burch, M.A.; Boot, W.; Tetsworth, K.; Miclau, T.; et al. The influence of biomechanical stability on bone healing and fracture-related infection: The legacy of stephan perren. Injury 2021, 52, 43–52. [Google Scholar] [CrossRef]
- Crouser, N.; Malik, A.T.; Phieffer, L.S.; Ly, T.V.; Khan, S.N.; Quatman, C.E. Urinary tract infection (uti) at time of geriatric hip fracture surgery increases the risk of experiencing adverse 30-day outcomes. J. Clin. Orthop. Trauma 2019, 10, 774–778. [Google Scholar] [CrossRef] [PubMed]
- Du, J.; Park, Y.T.; Theera-Ampornpunt, N.; McCullough, J.S.; Speedie, S.M. The use of count data models in biomedical informatics evaluation research. J. Am. Med. Inform. Assoc. 2012, 19, 39–44. [Google Scholar] [CrossRef]
- Hung, L.C.; Kung, P.T.; Lung, C.H.; Tsai, M.H.; Liu, S.A.; Chiu, L.T.; Huang, K.H.; Tsai, W.C. Assessment of the risk of oral cancer incidence in a high-risk population and establishment of a predictive model for oral cancer incidence using a population-based cohort in taiwan. Int. J. Environ. Res. Public Health 2020, 17, 665. [Google Scholar] [CrossRef]
- Ahmad, R.; Bath, P.A. Identification of risk factors for 15-year mortality among community-dwelling older people using cox regression and a genetic algorithm. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 1052–1058. [Google Scholar] [CrossRef]
- Starr, A.J.; Griffin, D.R.; Reinert, C.M.; Frawley, W.H.; Walker, J.; Whitlock, S.N.; Borer, D.S.; Rao, A.V.; Jones, A.L. Pelvic ring disruptions: Prediction of associated injuries, transfusion requirement, pelvic arteriography, complications, and mortality. J. Orthop. Trauma 2002, 16, 553–561. [Google Scholar] [CrossRef]
- Watnik, N.F.; Coburn, M.; Goldberger, M. Urologic injuries in pelvic ring disruptions. Clin. Orthop. Relat. Res. 1996, 329, 37–45. [Google Scholar] [CrossRef]
- Bjurlin, M.A.; Fantus, R.J.; Mellett, M.M.; Goble, S.M. Genitourinary injuries in pelvic fracture morbidity and mortality using the national trauma data bank. J. Trauma 2009, 67, 1033–1039. [Google Scholar] [CrossRef]
- Poole, G.V.; Ward, E.F.; Griswold, J.A.; Muakkassa, F.F.; Hsu, H.S. Complications of pelvic fractures from blunt trauma. Am. Surg. 1992, 58, 225–231. [Google Scholar]
- Johnsen, N.V.; Vanni, A.J.; Voelzke, B.B. Risk of infectious complications in pelvic fracture urethral injury patients managed with internal fixation and suprapubic catheter placement. J. Trauma Acute Care Surg. 2018, 85, 536–540. [Google Scholar] [CrossRef]
- Dwyer, E.P.; Moed, B.R. Venous thromboembolism after hospital discharge in pelvic and acetabular fracture patients treated operatively. J. Orthop. Surg. 2019, 27, 2309499019832815. [Google Scholar] [CrossRef] [PubMed]
- Poole, G.V.; Ward, E.F. Causes of mortality in patients with pelvic fractures. Orthopedics 1994, 17, 691–696. [Google Scholar] [CrossRef]
- Chong, K.H.; DeCoster, T.; Osler, T.; Robinson, B. Pelvic fractures and mortality. Iowa Orthop. J. 1997, 17, 110–114. [Google Scholar] [PubMed]
- Heyes, G.J.; Tucker, A.; Marley, D.; Foster, A. Predictors for readmission up to 1 year following hip fracture. Arch. Trauma Res. 2015, 4, e27123. [Google Scholar]
- Kates, S.L.; Behrend, C.; Mendelson, D.A.; Cram, P.; Friedman, S.M. Hospital readmission after hip fracture. Arch. Orthop. Trauma Surg. 2015, 135, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Lizaur-Utrilla, A.; Serna-Berna, R.; Lopez-Prats, F.A.; Gil-Guillen, V. Early rehospitalization after hip fracture in elderly patients: Risk factors and prognosis. Arch. Orthop. Trauma Surg. 2015, 135, 1663–1667. [Google Scholar] [CrossRef]
- Pollock, F.H.; Bethea, A.; Samanta, D.; Modak, A.; Maurer, J.P.; Chumbe, J.T. Readmission within 30 days of discharge after hip fracture care. Orthopedics 2015, 38, e7–e13. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.C.; Ho, P.S.; Lin, H.T.; Ho, M.L.; Huang, H.T.; Chang, J.K. One-year readmission risk and mortality after hip fracture surgery: A national population-based study in taiwan. Aging Dis. 2017, 8, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Heyes, G.J.; Tucker, A.; Marley, D.; Foster, A. Predictors for 1-year mortality following hip fracture: A retrospective review of 465 consecutive patients. Eur. J. Trauma Emerg. Surg. 2017, 43, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Meyhoff, C.S.; Thomsen, C.H.; Rasmussen, L.S.; Nielsen, P.R. High incidence of chronic pain following surgery for pelvic fracture. Clin. J. Pain 2006, 22, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Gerbershagen, H.J.; Dagtekin, O.; Isenberg, J.; Martens, N.; Ozgür, E.; Krep, H.; Sabatowski, R.; Petzke, F. Chronic pain and disability after pelvic and acetabular fractures--assessment with the mainz pain staging system. J. Trauma 2010, 69, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Minardi, D.; d’Anzeo, G.; Cantoro, D.; Conti, A.; Muzzonigro, G. Urinary tract infections in women: Etiology and treatment options. Int. J. Gen. Med. 2011, 4, 333–343. [Google Scholar] [CrossRef] [PubMed]
- Aslam, S.; Albo, M.; Brubaker, L. Recurrent urinary tract infections in adult women. JAMA 2020, 323, 658–659. [Google Scholar] [CrossRef] [PubMed]
- Shih, W.Y.; Chang, C.C.; Tsou, M.T.; Chan, H.L.; Chen, Y.J.; Hwang, L.C. Incidence and risk factors for urinary tract infection in an elder home care population in taiwan: A retrospective cohort study. Int. J. Environ. Res. Public Health 2019, 16, 566. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Non-UTI n = 1508 | UTI n = 115 | p-Value |
|---|---|---|---|
| Sex | <0.0001 | ||
| Female | 823(54.58%) | 85(73.91%) | |
| Male | 685(45.42%) | 30(26.09%) | |
| Age | <0.0001 | ||
| 18–40 | 551(36.54%) | 31(26.96%) | |
| 41–65 | 566(37.53%) | 32(27.83%) | |
| >65 | 391(25.93%) | 52(45.22%) | |
| Comorbidities | |||
| Hypertension | 358(23.74%) | 52(45.22%) | <0.0001 |
| Diabetes mellitus | 216(14.32%) | 31(26.96%) | 0.0003 |
| Hyperlipidemia | 145(9.62%) | 23(20%) | 0.0004 |
| Coronary artery disease | 165(10.94%) | 17(14.78%) | 0.2083 |
| Cerebrovascular accident | 131(8.69%) | 23(20%) | <0.0001 |
| CKD | 114(7.56%) | 15(13.04%) | 0.0361 |
| COPD | 169(11.21%) | 16(13.91%) | 0.3787 |
| Chronic liver diseases | 183(12.14%) | 18(15.65%) | 0.2698 |
| Heart failure | 72(4.77%) | 14(12.17%) | 0.0006 |
| Depression | 223(14.79%) | 19(16.52%) | 0.6148 |
| Osteoporosis | 233(15.45%) | 25(21.74%) | 0.0755 |
| Asthma | 75(4.97%) | 9(7.83%) | 0.1832 |
| Osteoarthritis | 378(25.07%) | 37(32.17%) | 0.0922 |
| Surgery for pelvic fracture | 177(11.74%) | 11(9.57%) | 0.4829 |
| Variable | Incidence Density * (95% CI) | cRR * (95% CI) | p-Value | aHR * (95% CI) | p-Value | |
|---|---|---|---|---|---|---|
| Non-UTI | UTI | |||||
| Mortality | ||||||
| from index date to | ||||||
| 1 m | 0.60(0.31–1.17) | 2.67(0.86–8.30) | 4.37(1.18–16.1) | 0.0268 | 2.48(0.63–9.66) | 0.1897 |
| 2 m | 0.54(0.33–0.88) | 2.25(0.93–5.41) | 4.12(1.51–11.2) | 0.0056 | 2.43(0.84–7.03) | 0.1000 |
| 3 m | 0.49(0.32–0.75) | 2.44(1.22–4.89) | 4.87(2.16–10.9) | 0.0001 | 2.50(1.05–5.95) | 0.0369 |
| 6 m | 0.38(0.27–0.53) | 1.72(0.95–3.12) | 4.39(2.22–8.67) | <0.0001 | 2.31(1.11–4.78) | 0.0241 |
| 9 m | 0.31(0.22–0.42) | 1.59(0.96–2.64) | 5.02(2.78–9.07) | <0.0001 | 2.71(1.44–5.11) | 0.0019 |
| 1 year | 0.28(0.21–0.37) | 1.19(0.71–1.98) | 4.14(2.32–7.38) | <0.0001 | 2.32(1.25–4.29) | 0.0070 |
| Readmission | ||||||
| from index date to | ||||||
| 1 m | 4.93(3.90–6.22) | 18.1(11.4–28.8) | 3.47(2.07–5.83) | <0.0001 | 2.95(1.71–5.10) | 0.0001 |
| 2 m | 4.52(3.80–5.38) | 14.5(9.95–21.1) | 3.04(2.00–4.60) | <0.0001 | 2.68(1.73–4.15) | <0.0001 |
| 3 m | 4.16(3.59–4.83) | 12.3(8.78–17.3) | 2.80(1.93–4.07) | <0.0001 | 2.53(1.71–3.73) | <0.0001 |
| 6 m | 3.44(3.05–3.87) | 8.17(6.00–11.1) | 2.25(1.61–3.14) | <0.0001 | 1.98(1.40–2.80) | <0.0001 |
| 9 m | 2.99(2.68–3.32) | 6.61(4.95–8.83) | 2.11(1.55–2.87) | <0.0001 | 1.83(1.33–2.51) | 0.0002 |
| 1 year | 2.61(2.37–2.89) | 5.47(4.13–7.24) | 1.98(1.47–2.67) | <0.0001 | 1.72(1.26–2.34) | 0.0005 |
| Variable | Mortality | Re-Admission | ||
|---|---|---|---|---|
| aHR (95% CI) | p-Value | aHR (95% CI) * | p-Value | |
| UTI | ||||
| No | Reference | Reference | ||
| Yes | 2.32(1.25–4.29) | 0.0070 | 1.72(1.26–2.34) | 0.0005 |
| Sex | ||||
| Female | Reference | Reference | ||
| Male | 1.19(0.68–2.09) | 0.5248 | 1.23(1.01–1.51) | 0.0382 |
| Age | ||||
| 18–40 | Reference | Reference | ||
| 41–65 | 1.34(0.38–4.70) | 0.6434 | 1.01(0.77–1.32) | 0.9209 |
| >65 | 6.55(2.03–21.0) | 0.0016 | 1.57(1.14–2.14) | 0.0047 |
| Comorbidities (ref: non) | ||||
| Hypertension | 1.16(0.63–2.15) | 0.6229 | 0.99(0.76–1.28) | 0.9528 |
| Diabetes mellitus | 1.05(0.58–1.91) | 0.851 | 1.51(1.17–1.94) | 0.0014 |
| Hyperlipidemia | 0.54(0.25–1.15) | 0.1142 | 0.79(0.58–1.06) | 0.1254 |
| Coronary artery disease | 0.55(0.29–1.02) | 0.0581 | 0.88(0.66–1.18) | 0.4048 |
| Cerebrovascular accident | 1.54(0.84–2.82) | 0.1554 | 1.35(1.02–1.78) | 0.0328 |
| CKD | 2.80(1.60–4.90) | 0.0003 | 1.59(1.19–2.12) | 0.0016 |
| COPD | 1.84(1.01–3.37) | 0.0454 | 1.47(1.12–1.93) | 0.0045 |
| Chronic liver diseases | 1.42(0.79–2.58) | 0.2384 | 1.46(1.13–1.87) | 0.0028 |
| Heart failure | 2.79(1.54–5.06) | 0.0007 | 1.35(0.96–1.91) | 0.0777 |
| Depression | 1.09(0.58–2.05) | 0.7717 | 1.20(0.94–1.53) | 0.1335 |
| Osteoporosis | 0.94(0.53–1.67) | 0.8429 | 1.49(1.17–1.90) | 0.0010 |
| Asthma | 1.51(0.76–3.00) | 0.2349 | 1.46(1.01–2.09) | 0.0411 |
| Osteoarthritis | 1.39(0.81–2.39) | 0.2306 | 1.28(1.03–1.58) | 0.0226 |
| Surgery | ||||
| No | Reference | Reference | ||
| Yes | 0.58(0.13–2.50) | 0.4691 | 1.82(1.38–2.40) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-C.; Chuang, C.-H.; Hsieh, M.-H.; Yeh, H.-W.; Yang, S.-F.; Lin, C.-W.; Yeh, Y.-T.; Huang, J.-Y.; Liao, P.-L.; Chan, C.-H.; et al. Risk of Mortality and Readmission among Patients with Pelvic Fracture and Urinary Tract Infection: A Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 4868. https://doi.org/10.3390/ijerph18094868
Chen Y-C, Chuang C-H, Hsieh M-H, Yeh H-W, Yang S-F, Lin C-W, Yeh Y-T, Huang J-Y, Liao P-L, Chan C-H, et al. Risk of Mortality and Readmission among Patients with Pelvic Fracture and Urinary Tract Infection: A Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2021; 18(9):4868. https://doi.org/10.3390/ijerph18094868
Chicago/Turabian StyleChen, Ying-Cheng, Cheng-Hsun Chuang, Ming-Hong Hsieh, Han-Wei Yeh, Shun-Fa Yang, Chiao-Wen Lin, Ying-Tung Yeh, Jing-Yang Huang, Pei-Lun Liao, Chi-Ho Chan, and et al. 2021. "Risk of Mortality and Readmission among Patients with Pelvic Fracture and Urinary Tract Infection: A Population-Based Cohort Study" International Journal of Environmental Research and Public Health 18, no. 9: 4868. https://doi.org/10.3390/ijerph18094868
APA StyleChen, Y.-C., Chuang, C.-H., Hsieh, M.-H., Yeh, H.-W., Yang, S.-F., Lin, C.-W., Yeh, Y.-T., Huang, J.-Y., Liao, P.-L., Chan, C.-H., & Yeh, C.-B. (2021). Risk of Mortality and Readmission among Patients with Pelvic Fracture and Urinary Tract Infection: A Population-Based Cohort Study. International Journal of Environmental Research and Public Health, 18(9), 4868. https://doi.org/10.3390/ijerph18094868