
A Methodology for Harmonizing Safety and Health Scales in Occupational Risk Assessment



Abstract
1. Introduction
1.1. Context
1.2. Difficulty of Predicting Long-Term Health Outcomes in Risk Assessments
2. Research Approach
2.1. Research Purpose
2.2. Selection of Quality of Life as an Output Metric
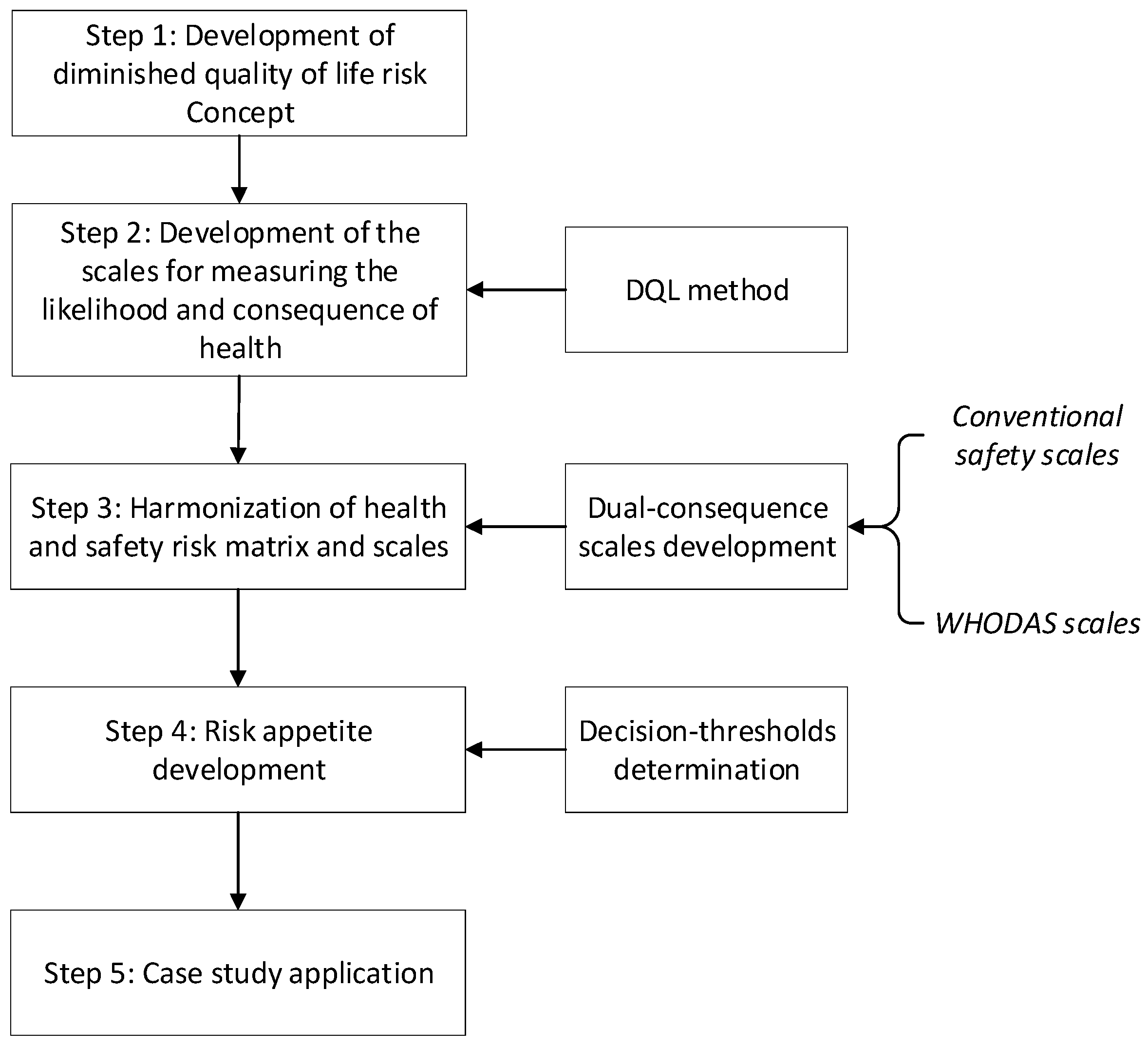
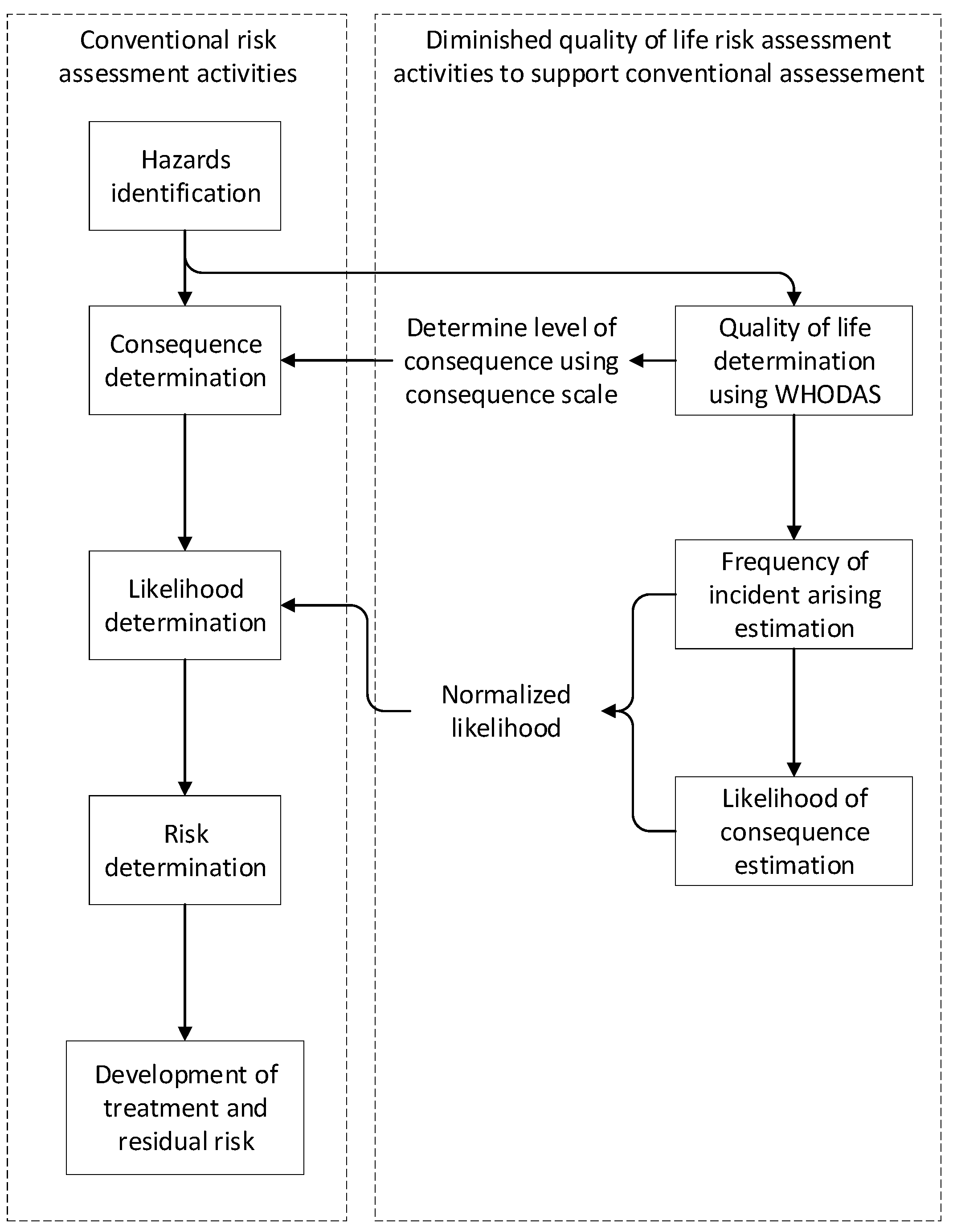
2.3. Methodology for H&S Risk Harmonization
3. Results
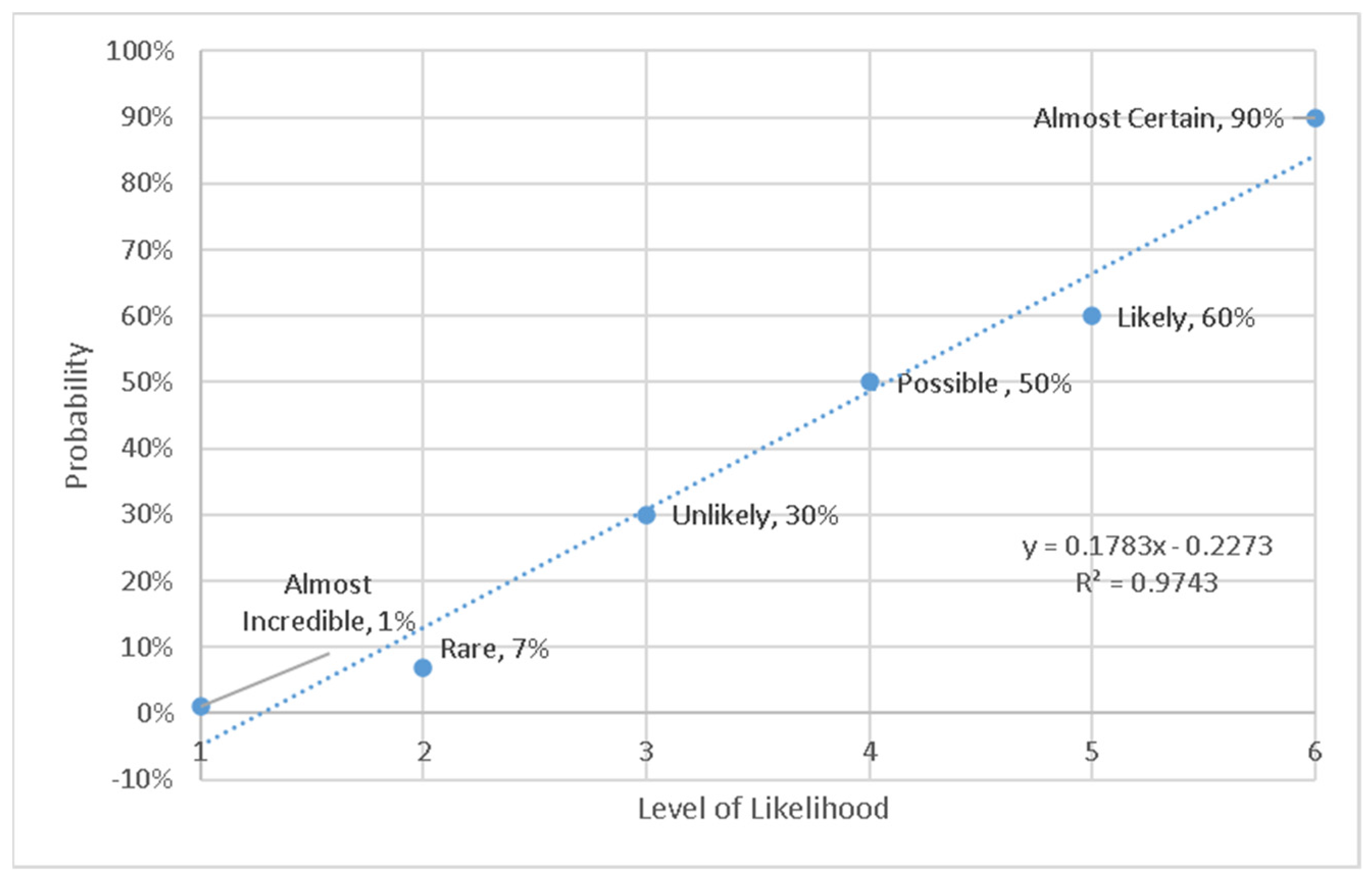
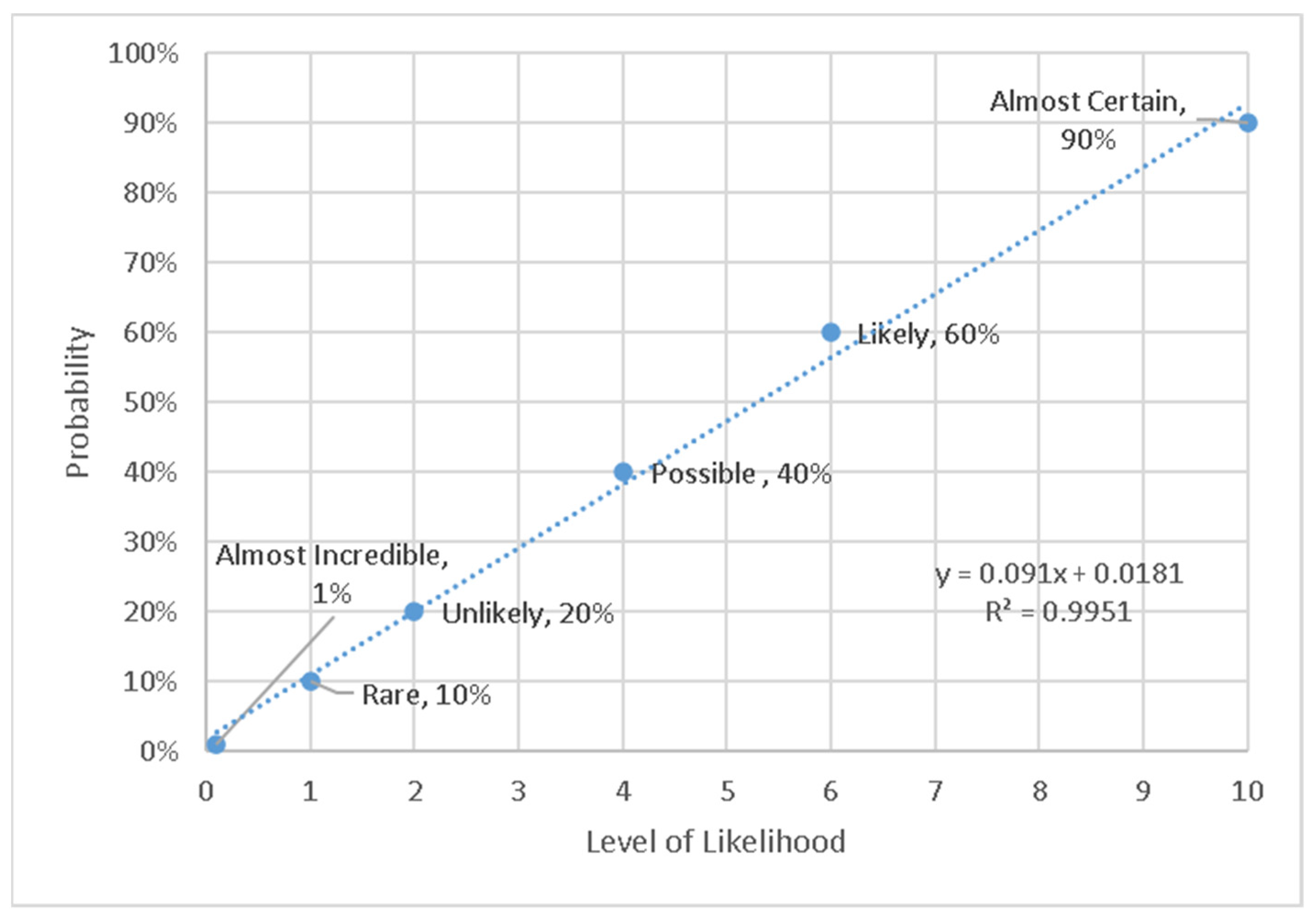
3.1. Harmonized Likelihood Scale
- Needs to be consistent by showing a defendable progression;
- Needs to provide ordinal numbers for a descriptive scale;
- Needs to accommodate a high probability of many events of minor consequence, and low probability of events with extreme consequences;
- Needs to use simple numbers (easy to compute)—this is so the new method can easily be used by industry practitioners in the field on paper, where most risk assessments are conducted.
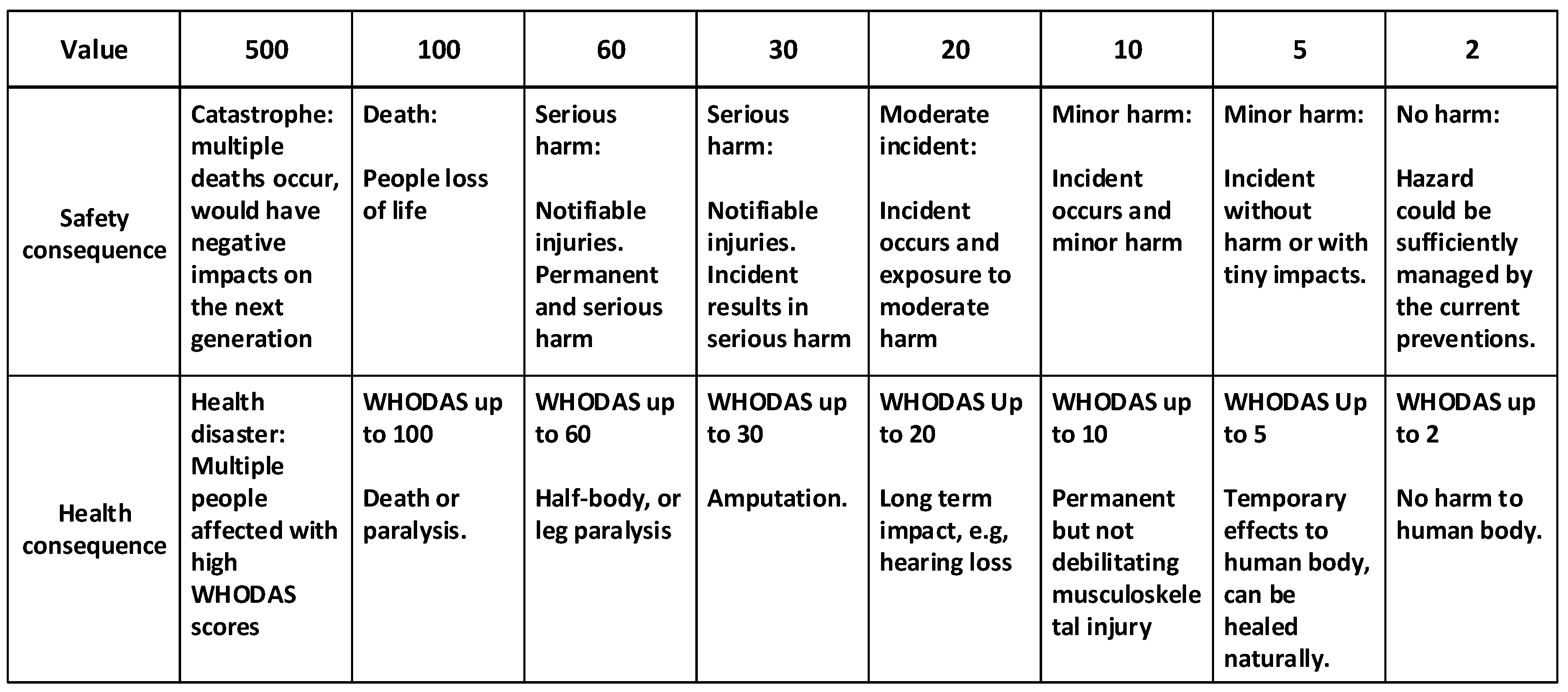
3.2. Harmonizing the Scale of Consequence
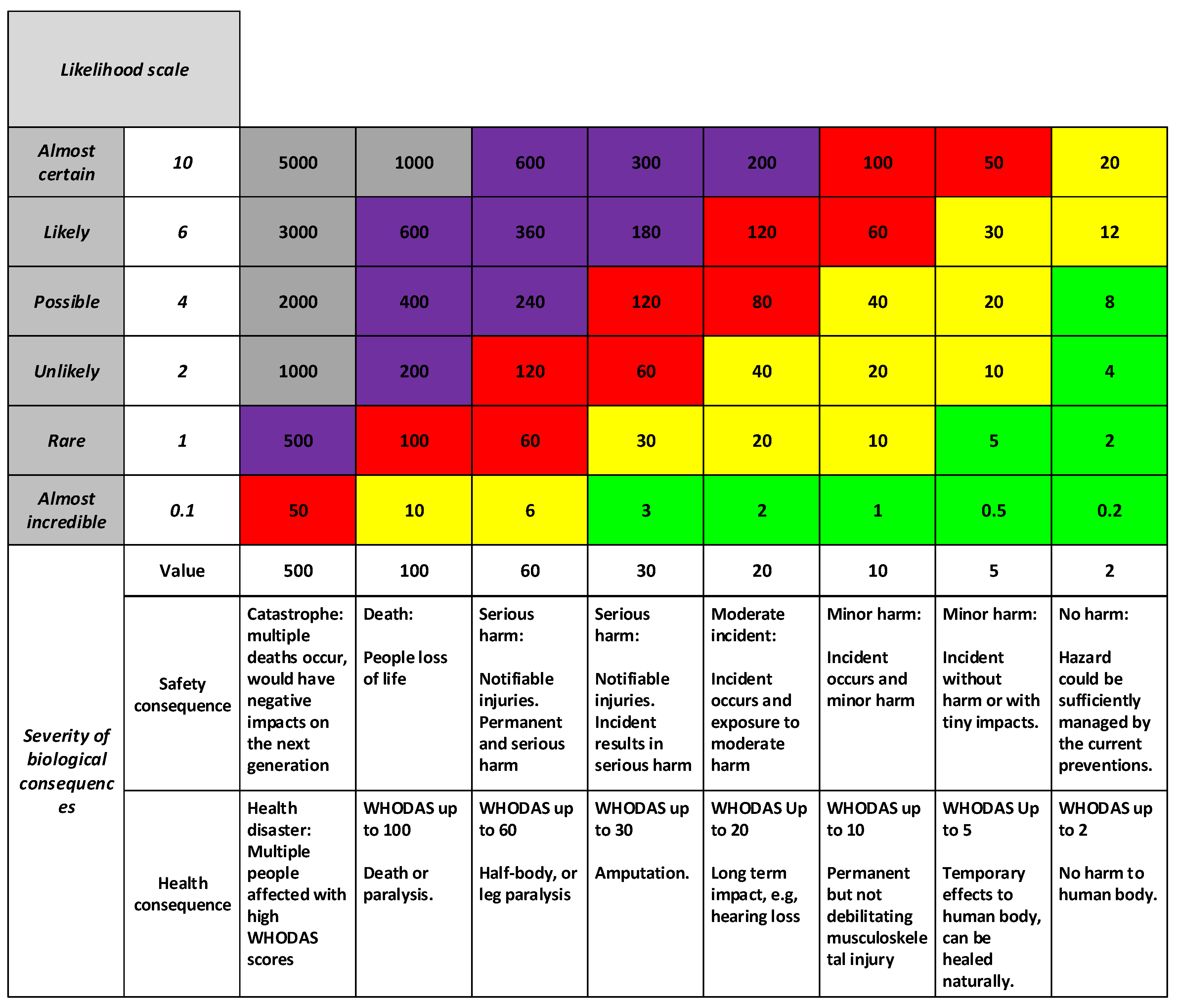
3.3. The DQL Risk Matrix
3.4. Risk Appetite and Response Scale
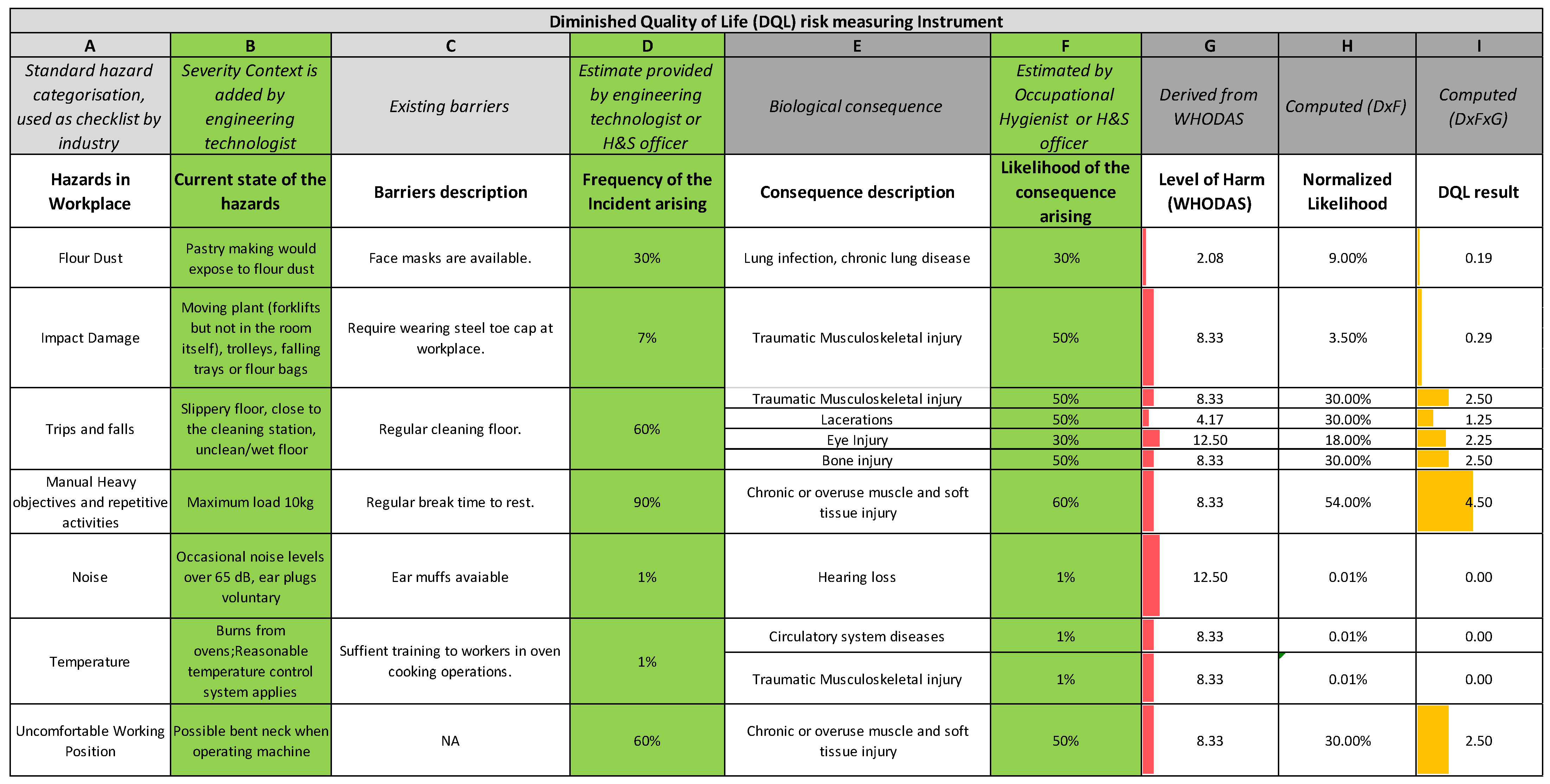
3.5. Application of the Harmonized H&S Risk Assessment Method to Case Study
4. Discussion
4.1. Interpretation
4.2. Implications for Practitioners
4.3. Limitations and Further Research Opportunities
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- International Organization for Standardization. ISO 31000 Risk Management—Principles and Guidelines; ISO: Geneva, Switzerland, 2009; 24p. [Google Scholar]
- Hyun, K.-C.; Min, S.; Choi, H.; Park, J.; Lee, I.-M. Risk analysis using fault-tree analysis (FTA) and analytic hierarchy process (AHP) applicable to shield TBM tunnels. Tunn. Undergr. Space Technol. 2015, 49, 121–129. [Google Scholar] [CrossRef]
- Lo, H.; Liou, J.J.H. A novel multiple-criteria decision-making-based FMEA model for risk assessment. Appl. Soft Comput. J. 2018, 73, 684–696. [Google Scholar] [CrossRef]
- Ji, Z.; Yang, S.-H.; Cao, Y.; Wang, Y.; Zhou, C.; Yue, L.; Zhang, Y. Harmonizing safety and security risk analysis and prevention in cyber-physical systems. Process Saf. Environ. Prot. 2021, 148, 1279–1291. [Google Scholar] [CrossRef]
- Fuentes-Bargues, J.L.; Gonzalez-Gaya, C.; Gonzalez-Cruz, M.C.; Cabrelles-Ramirez, V. Risk assessment of a compound feed process based on HAZOP analysis and linguistic terms. J. Loss Prev. Process Ind. 2016, 44, 44–52. [Google Scholar] [CrossRef]
- Fargnoli, M.; Lombardi, M.; Haber, N.; Guadagno, F. Hazard function deployment: A QFD-based tool for the assessment of working tasks—A practical study in the construction industry. Int. J. Occup. Saf. Ergon. 2020, 26, 348–369. [Google Scholar] [CrossRef]
- Pinto, A.; Nunes, I.L.; Ribeiro, R.A. Occupational risk assessment in construction industry—Overview and reflection. Saf. Sci. 2011, 49, 616–624. [Google Scholar] [CrossRef]
- Peeters, J.F.W.; Basten, R.J.I.; Tinga, T. Improving failure analysis efficiency by combining FTA and FMEA in a recursive manner. Reliab. Eng. Syst. Saf. 2018, 172, 36–44. [Google Scholar] [CrossRef]
- Aneziris, O.N.; Nivolianitou, Z.; Konstandinidou, M.; Mavridis, G.; Plot, E. A Total Safety Management framework in case of a major hazards plant producing pesticides. Saf. Sci. 2017, 100, 183–194. [Google Scholar] [CrossRef]
- Cui, L.; Zhao, J.; Qiu, T.; Chen, B. Layered digraph model for HAZOP analysis of chemical processes. Process Saf. Progress 2008, 27, 293–305. [Google Scholar] [CrossRef]
- Mokhtari, K.; Ren, J.; Roberts, C.; Wang, J. Application of a generic bow-tie based risk analysis framework on risk management of sea ports and offshore terminals. J. Hazard. Mater. 2011, 192, 465–475. [Google Scholar] [CrossRef]
- Ji, Z.; Pons, D.; Pearse, J. Measuring Industrial Health Using a Diminished Quality of Life Instrument. Safety 2018, 4, 55. [Google Scholar] [CrossRef]
- Pons, D.J. Pike River Mine Disaster: Systems-Engineering and Organisational Contributions. Safety 2016, 2, 21. [Google Scholar] [CrossRef]
- New Zealand Legislation. Health and Safety at Work Act 2015; Ministry of Business, Innovation and Employment: Wellington, New Zealand, 2015.
- Pons, D.J. Alignment of the Safety Assessment Method with New Zealand Legislative Responsibilities. Safety 2019, 5, 59. [Google Scholar] [CrossRef]
- Kadota, J.L.; Mccoy, S.I.; Bates, M.N.; Mnyippembe, A.; Njau, P.F.; Prata, N.; Harris-Adamson, C. The impact of heavy load carrying on musculoskeletal pain and disability among women in Shinyanga region, Tanzania. Ann. Glob. Health 2020, 86, 17. [Google Scholar] [CrossRef]
- Cummings, K.J.; Boylstein, R.J.; Stanton, M.L.; Piacitelli, C.A.; Edwards, N.T.; Lebouf, R.F.; Kreiss, K. Respiratory symptoms and lung function abnormalities related to work at a flavouring manufacturing facility. Occup. Environ. Med. 2014, 71, 549–554. [Google Scholar] [CrossRef]
- Cantley, L.F.; Galusha, D.; Cullen, M.R.; Dixon-Ernst, C.; Rabinowitz, P.M.; Neitzel, R.L. Association between ambient noise exposure, hearing acuity, and risk of acute occupational injury. Scand. J. Work Environ. Health 2015, 41, 75–83. [Google Scholar] [CrossRef]
- Reddy, R.K.; Welch, D.; Thorne, P.; Ameratunga, S. Hearing protection use in manufacturing workers: A qualitative study. Noise Health 2012, 14, 202–209. [Google Scholar] [CrossRef]
- Ji, Z.; Pons, D.J.; Pearse, J. Plant system simulation for engineering training workshops. Comput. Appl. Eng. Educ. 2019, 1, 17–30. [Google Scholar] [CrossRef]
- Niemeier, R.T.; Williams, P.R.D.; Rossner, A.; Clougherty, J.E.; Rice, G.E. A Cumulative Risk Perspective for Occupational Health and Safety (OHS) Professionals. Int. J. Environ. Res. Public Health 2020, 17, 6342. [Google Scholar] [CrossRef]
- Brogan, K.; Marcelino, G.; Pedro, C.; Siefert, A. Healing of Graves’ Disease Thorough Lifestyle Changes: A Case Report. Adv. Mind Body Med. 2019, 33, 4–11. [Google Scholar]
- Smith, J.E.; Keeney, R.L. Your money or your life: A prescriptive model for health, safety, and consumption decisions. Manag. Sci. 2005, 51, 1309–1325. [Google Scholar] [CrossRef][Green Version]
- Ponce, R.A.; Wong, E.Y.; Faustman, E.M. Quality Adjusted Life Years (QALYs) and Dose-Response Models in Environmental Health Policy Analysis—Methodological Considerations; Elsevier: Amsterdam, The Netherlands, 2001; pp. 79–91. [Google Scholar]
- Gao, T.; Wang, X.C.; Chen, R.; Ngo, H.H.; Guo, W. Disability adjusted life year (DALY): A useful tool for quantitative assessment of environmental pollution. Sci. Total Environ. 2015, 511, 268–287. [Google Scholar] [CrossRef]
- Üstün, T.B. Measuring Health and Disability: Manual for WHO Disability Assessment Schedule WHODAS 2.0.; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Chiu, T.-Y.; Yen, C.-F.; Chou, C.-H.; Lin, J.-D.; Hwang, A.-W.; Liao, H.-F.; Chi, W.-C. Development of traditional Chinese version of World Health Organization Disability Assessment Schedule 2.0 36—Item (WHODAS 2.0) in Taiwan: Validity and reliability analyses. Res. Dev. Disab. 2014, 35, 2812–2820. [Google Scholar] [CrossRef]
- Ji, Z.; Pons, D.J.; Pearse, J. Integrating occupational health and safety into plant simulation. Saf. Sci. 2020, 130, 104898. [Google Scholar] [CrossRef]
- Ji, Z. Optimising Manufacturing Industrial Production Layout for Occupational Health and Safety. Ph.D. Thesis, University of Canterbury, Christchurch, New Zealand, 2019. [Google Scholar]
- Saa/Snz Hb436. Risk Management Guidelines; Standards Australia: Sydney, Australia, 2005; ISBN 0-7337-5960-2. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Likelihood Description | Likelihood Scale | Descriptor (Adapted from [30]) |
|---|---|---|
| Almost Certain | 10 | Annual occurrence in this situation |
| Likely | 6 | Has occurred several times in your career |
| Possible | 4 | Might occur once in your career |
| Unlikely | 2 | Event does occur somewhere from time to time |
| Rare | 1 | Heard of something like this happening elsewhere |
| Almost Incredible | 0.1 | Theoretically possible but not expected to occur |
| Level of WHODAS Score | Harm Description |
|---|---|
| 100 < WHODAS < 500 | Large group of people been affected, a health disaster, could have negative impact on next generations |
| 60 < WHODAS < 100 | Death or very serious harm |
| 30 < WHODAS < 60 | Serious harm, e.g., half-body paralysis. |
| 20 < WHODAS < 30 | Serious harm, e.g., amputation. |
| 10 < WHODAS < 20 | Moderate but permanent harm |
| 5 < WHODAS < 10 | Minor harm, permanent but not debilitating |
| 2 < WHODAS < 5 | Minor harm, temporary effects to human body, easy to heal |
| 0 < WHODAS < 2 | No harm to human body. |
| DQL Score (C × L) | Severity of Harm (Color in Risk Matrix, See Figure 7) | Description of Treatment | Actions | Authority for Continued Operation | Reporting |
|---|---|---|---|---|---|
| DQL > 1000 | Grey | Cessation. | Immediate intermission must be undertaken. Ensure preventions and recoveries are adequate and can manage the risk in the future operations. | Board members | CEO must report and advise solutions to Board members under urgency. |
| 120 < DQL < 1000 | Purple | Unacceptable risk. | Cease operations immediately until risk has been minimized. Ensure preventions and recoveries are sufficient and it is possible to manage the risk in the future operations. | Board and CEO | CEO needs to report and advise solutions to the Board as soon as practicable. |
| 60 < DQL < 120 | Red | Urgent treatment. | Urgent treatment required. Operations proceed with caution and ongoing monitoring of risk. | Technical manager | Technical manager to advise CEO as soon as possible, and report regularly on status of the risk and its treatment. |
| 10 < DQL < 60 | Yellow | Consider treatment. | Implement treatment in a reasonable time period. Continue the operations with caution. Monitor the risk in case it becomes worse. | Team leader | Team leader to report regularly to Technical manager on the risk and the progress of the treatment plan. |
| 0 < DQL < 10 | Green | Not necessary to have special treatment. | No special treatment required. Continue the operations with ongoing monitoring of the efficacy of existing preventions. | Operators | Staff to report regularly to Team leader on the state of this risk. |
| Hazard Description | Level of Consequence (C) | Likelihood of the Issue Occurrence (L) | Risk (C × L) | Principle of Action |
|---|---|---|---|---|
| Repetitive activities | 3 | 6 | 18 | Urgent treatment needed. |
| Noise | 3 | 3 | 9 | Consider treatment |
| Electrocution | 5 | 2 | 10 | Consider treatment |
| Worker entrapped by operating conveyors | 5 | 3 | 15 | Consider treatment |
| Hazard Description | Level of Consequence (C) | Normalized Likelihood (L) | DQL Score (C × L) | Principle of Action |
|---|---|---|---|---|
| Inhale flour | 2 | 1 | 2 | No further treatment required. |
| Electrocution | 30 | 1 | 30 | Consider treatment |
| Impact damage to human body | 10 | 2 | 20 | Consider treatment |
| Noise | 10 | 2 | 20 | Consider treatment |
| Repetitive operations | 10 | 6 | 60 | Urgent treatment needed |
| Uncomfortable working environment—temperature | 10 | 0.1 | 1 | No further treatment required. |
| Trip issue | 10 | 2 | 20 | Consider treatment |
| Uncomfortable working positions | 10 | 2 | 20 | Consider treatment |
| Trapped by equipment, e.g., conveyor | 30 | 1 | 30 | Consider treatment |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ji, Z.; Pons, D.; Pearse, J. A Methodology for Harmonizing Safety and Health Scales in Occupational Risk Assessment. Int. J. Environ. Res. Public Health 2021, 18, 4849. https://doi.org/10.3390/ijerph18094849
Ji Z, Pons D, Pearse J. A Methodology for Harmonizing Safety and Health Scales in Occupational Risk Assessment. International Journal of Environmental Research and Public Health. 2021; 18(9):4849. https://doi.org/10.3390/ijerph18094849
Chicago/Turabian StyleJi, Zuzhen, Dirk Pons, and John Pearse. 2021. "A Methodology for Harmonizing Safety and Health Scales in Occupational Risk Assessment" International Journal of Environmental Research and Public Health 18, no. 9: 4849. https://doi.org/10.3390/ijerph18094849
APA StyleJi, Z., Pons, D., & Pearse, J. (2021). A Methodology for Harmonizing Safety and Health Scales in Occupational Risk Assessment. International Journal of Environmental Research and Public Health, 18(9), 4849. https://doi.org/10.3390/ijerph18094849