
A Comparative Assessment of Cooling Center Preparedness across Twenty-Five U.S. Cities


Abstract
1. Introduction
2. Data and Methodology
2.1. Data
2.1.1. Cooling Center
2.1.2. Weather
2.1.3. Road Network
2.1.4. Demographic and Socioeconomic Subpopulations
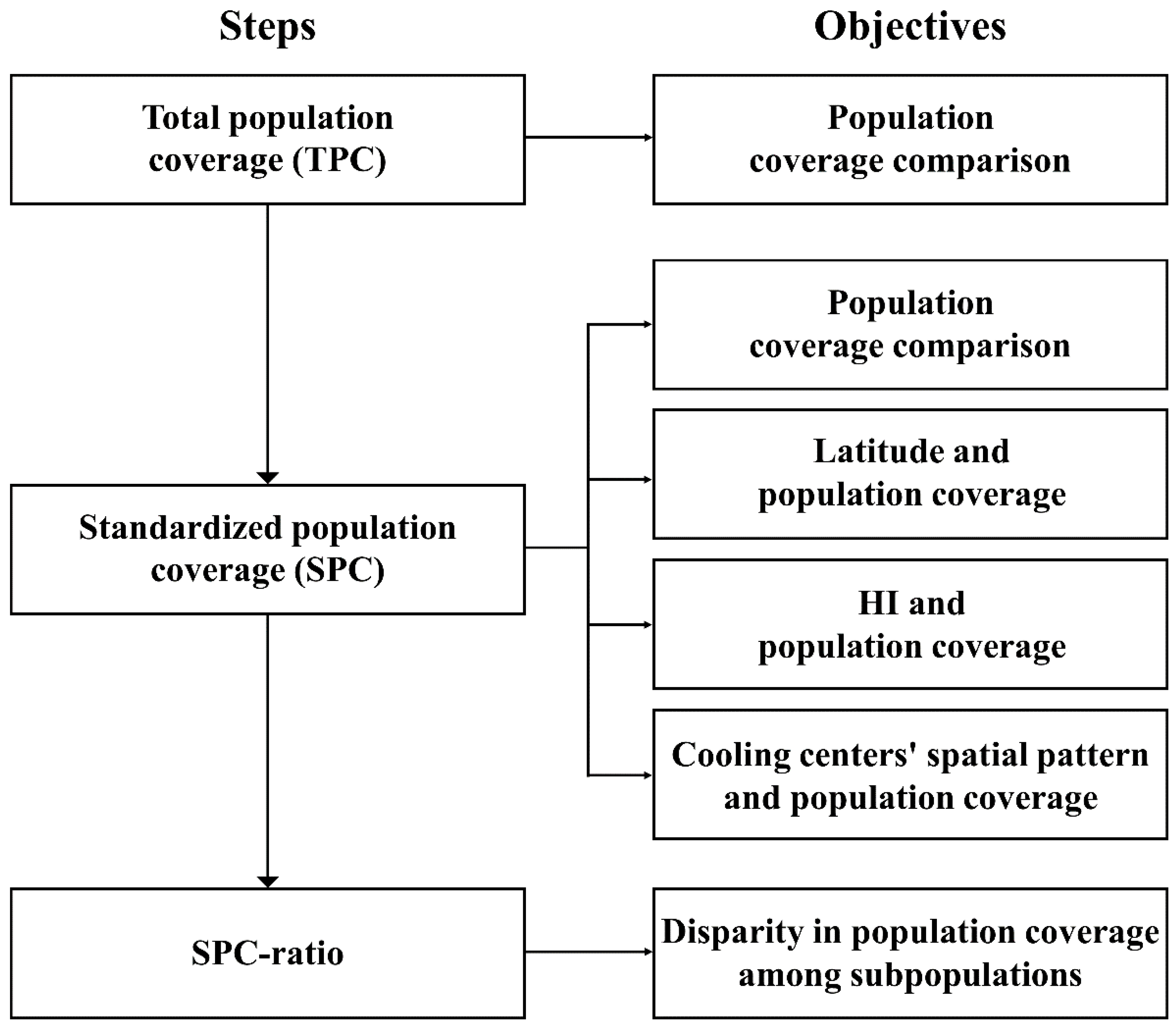
2.2. Methodology
3. Results
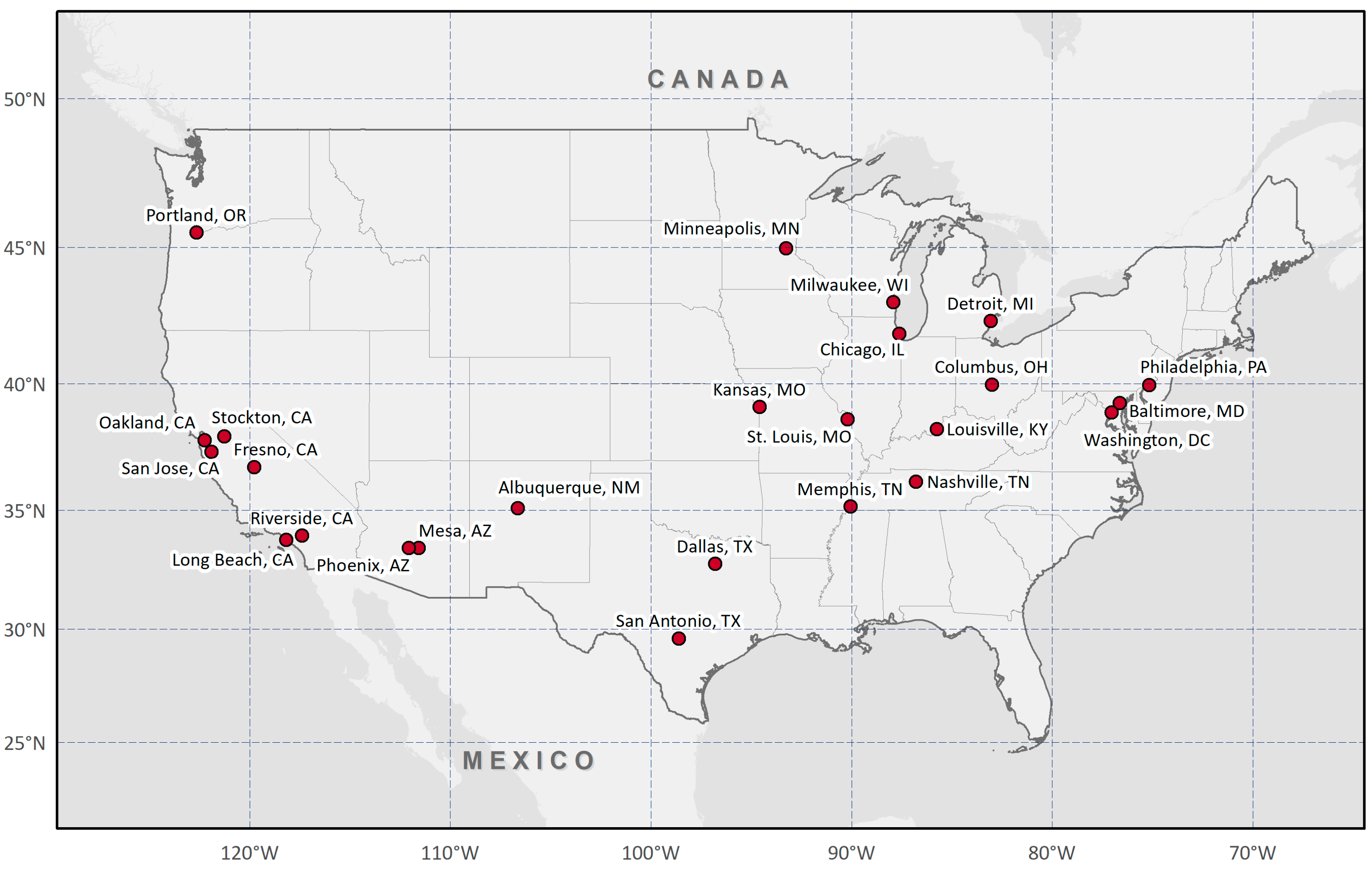
3.1. Descriptive Summary
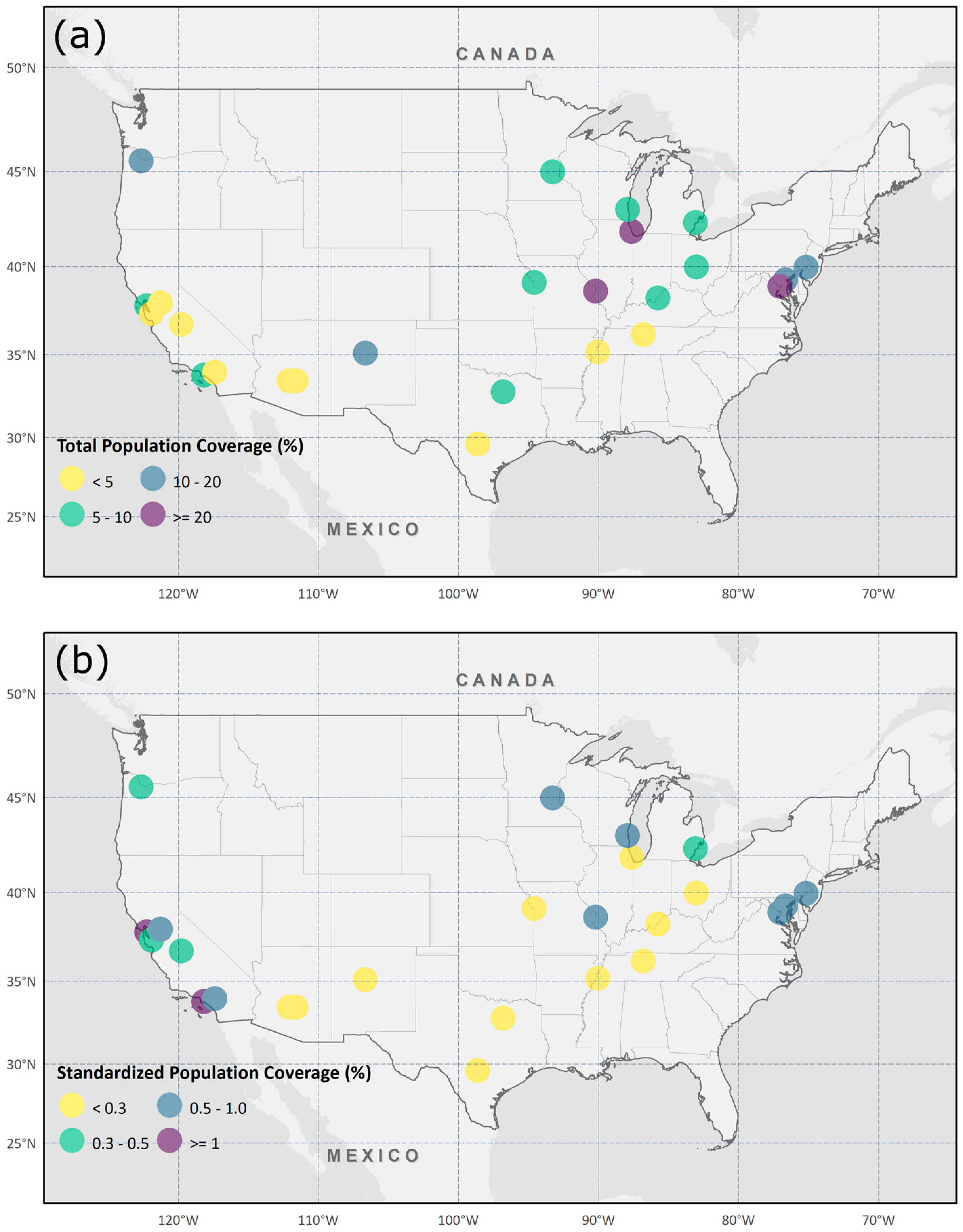
3.2. Population Coverage Level Comparison between Cities
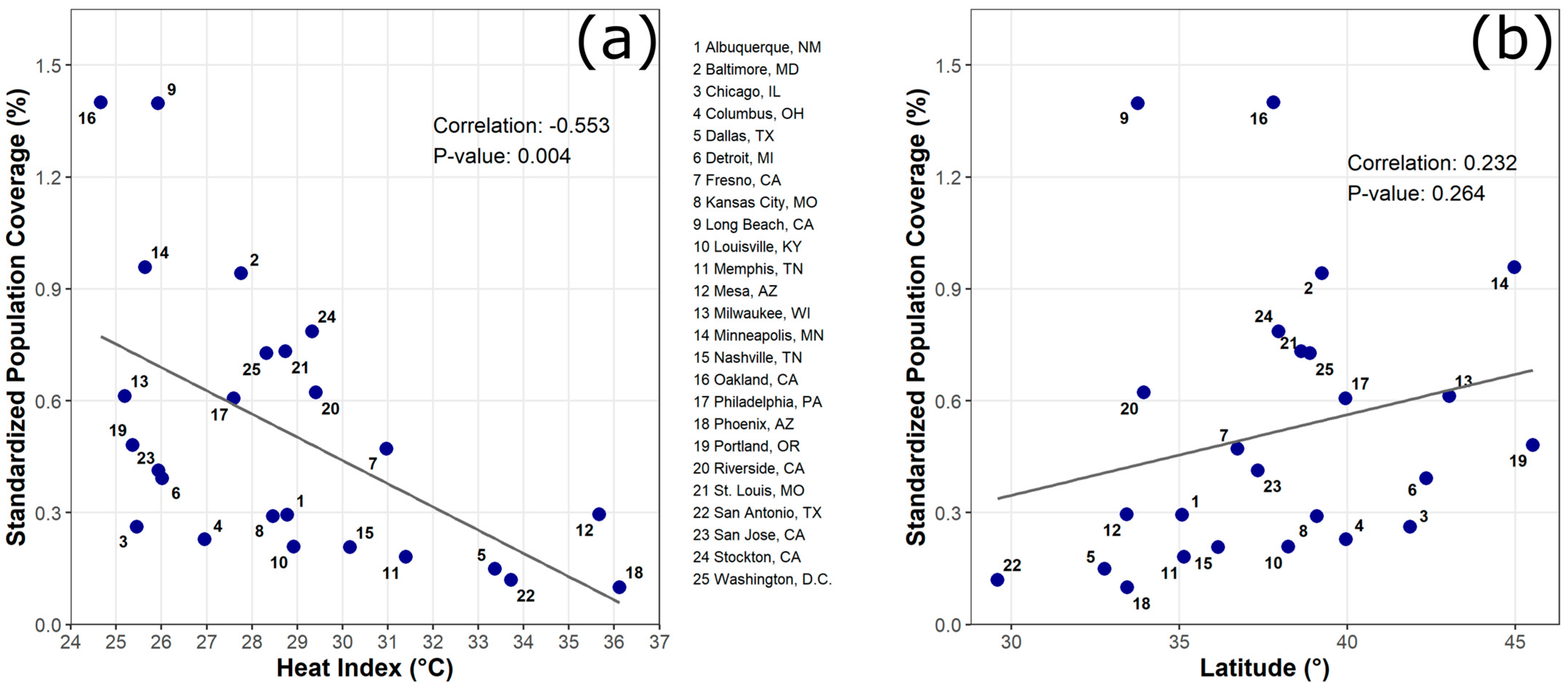
3.3. The Association between Latitude/HI and SPC
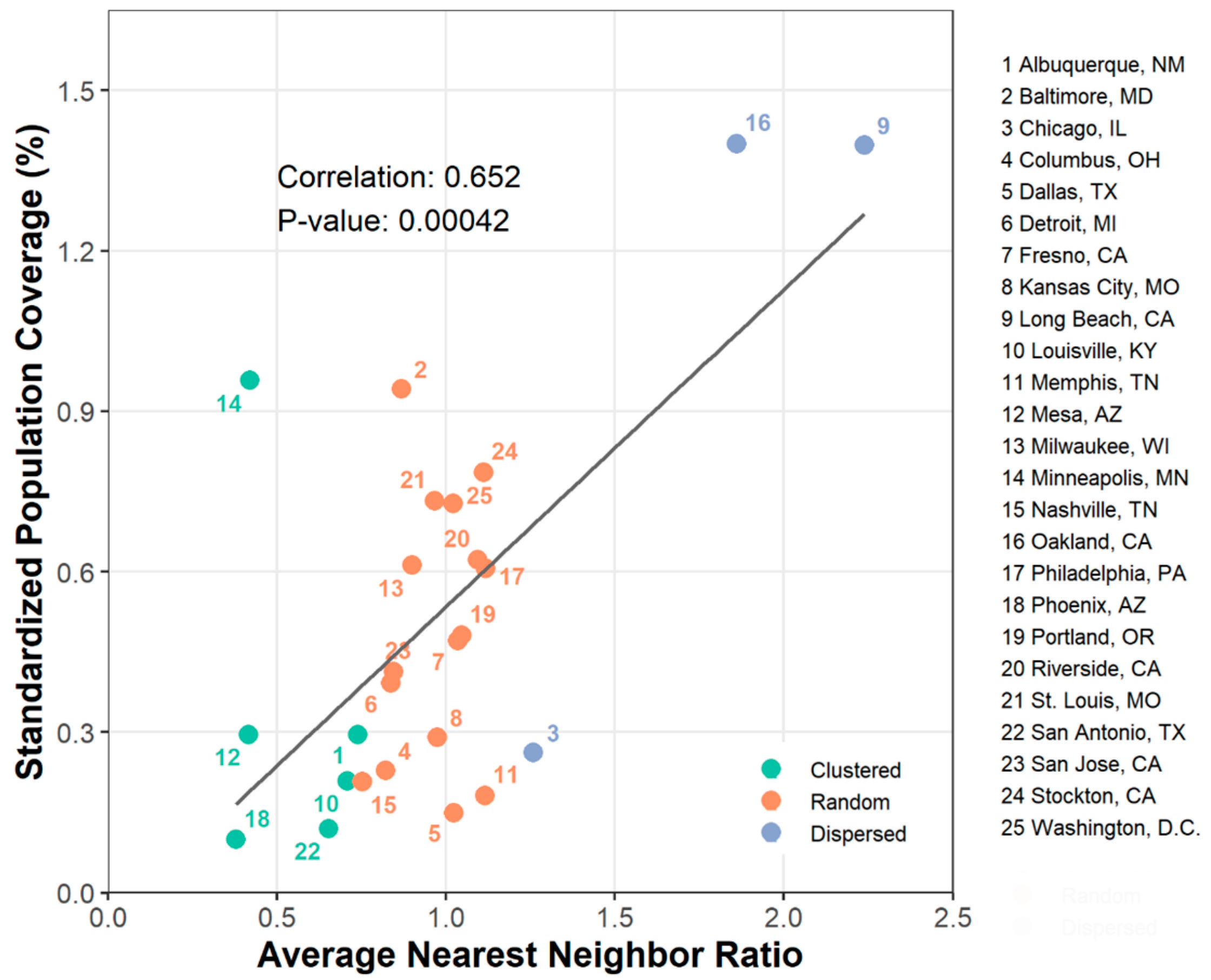
3.4. The Association between ANN Ratio and SPC
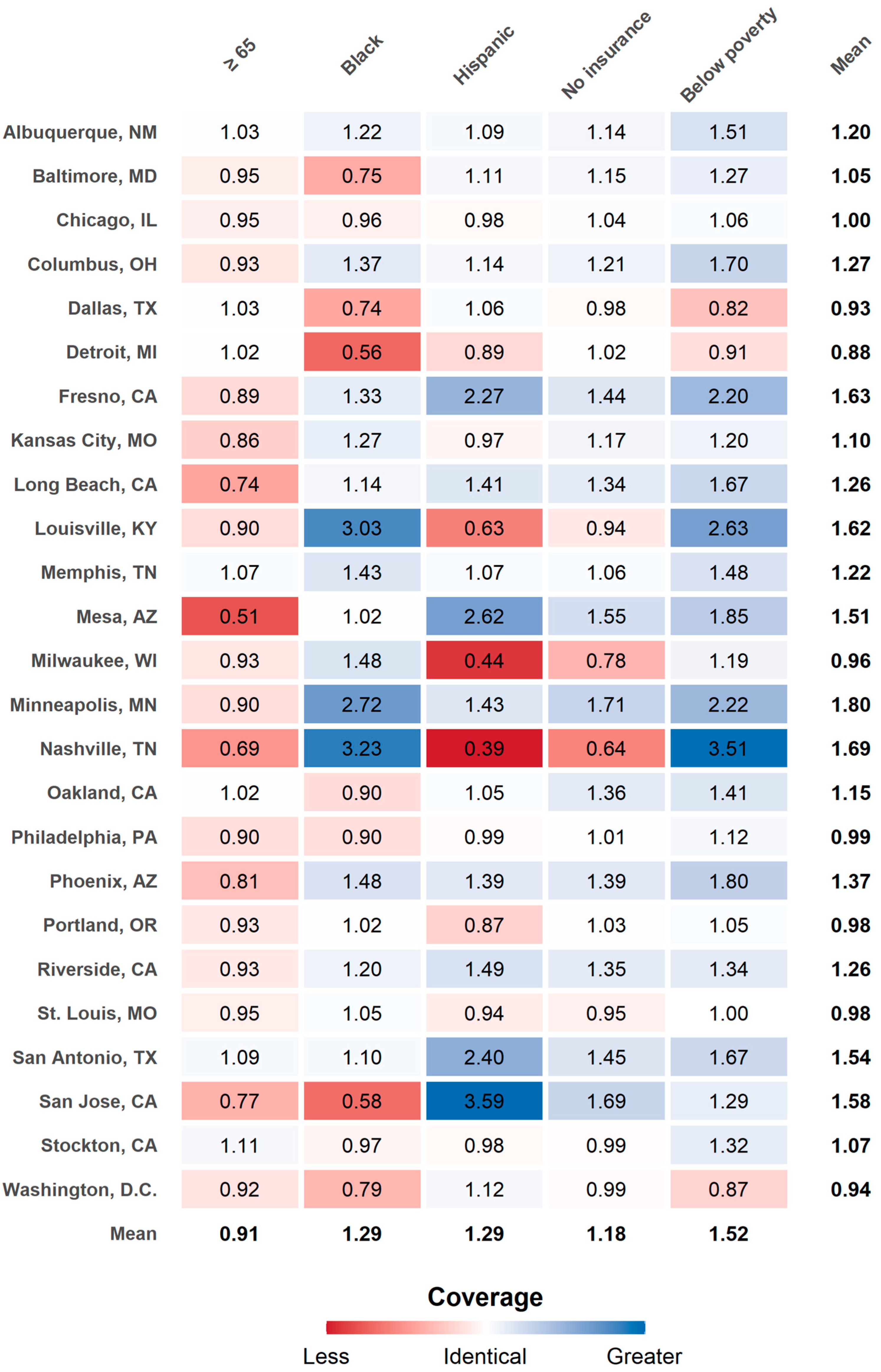
3.5. Disparity in Population Coverage Level for Subpopulation Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- IPCC. Climate Change 2014: Synthesis Report; Contribution of Working Groups I, II and III to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; IPCC: Geneva, Switzerland, 2014; Available online: https://ar5-syr.ipcc.ch/ipcc/ipcc/resources/pdf/IPCC_SynthesisReport.pdf (accessed on 13 February 2021).
- Meehl, G.A. More Intense, More Frequent, and Longer Lasting Heat Waves in the 21st Century. Science 2004, 305, 994–997. [Google Scholar] [CrossRef] [PubMed]
- Beniston, M.; Stephenson, D.B.; Christensen, O.B.; Ferro, C.A.T.; Frei, C.; Goyette, S.; Halsnaes, K.; Holt, T.; Jylhä, K.; Koffi, B.; et al. Future Extreme Events in European Climate: An Exploration of Regional Climate Model Projections. Clim. Chang. 2007, 81, 71–95. [Google Scholar] [CrossRef]
- Li, M.; Gu, S.; Bi, P.; Yang, J.; Liu, Q. Heat Waves and Morbidity: Current Knowledge and Further Direction-a Comprehensive Literature Review. Int. J. Environ. Res. Public Health 2015, 12, 5256–5283. [Google Scholar] [CrossRef]
- Sherbakov, T.; Malig, B.; Guirguis, K.; Gershunov, A.; Basu, R. Ambient Temperature and Added Heat Wave Effects on Hospitalizations in California from 1999 to 2009. Environ. Res. 2018, 160, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Xu, Z.; Bambrick, H.; Prescott, V.; Wang, N.; Zhang, Y.; Su, H.; Tong, S.; Hu, W. Cardiorespiratory Effects of Heatwaves: A Systematic Review and Meta-Analysis of Global Epidemiological Evidence. Environ. Res. 2019, 177, 108610. [Google Scholar] [CrossRef]
- McGinnis, J.M.; Foege, W.H. Actual Causes of Death in the United States. JAMA 1993, 270, 2207–2212. [Google Scholar] [CrossRef]
- Mokdad, A.H. Actual Causes of Death in the United States, 2000. JAMA 2004, 291, 1238. [Google Scholar] [CrossRef]
- Fraser, A.M.; Chester, M.V.; Eisenman, D. Strategic Locating of Refuges for Extreme Heat Events (or Heat Waves). Urban Clim. 2018, 25, 109–119. [Google Scholar] [CrossRef]
- Bouchama, A.; Dehbi, M.; Mohamed, G.; Matthies, F.; Shoukri, M.; Menne, B. Prognostic Factors in Heat Wave-Related Deaths: A Meta-Analysis. Arch. Intern. Med. 2007, 167, 2170–2176. [Google Scholar] [CrossRef]
- World Health Organization. WHO Housing and Health Guidelines. Available online: https://www.who.int/publications-detail-redirect/9789241550376 (accessed on 12 February 2021).
- Farbotko, C.; Waitt, G. Residential Air-Conditioning and Climate Change: Voices of the Vulnerable. Health Promot. J. Aust. 2011, 22, 13–15. [Google Scholar]
- Hayden, M.H.; Brenkert-Smith, H.; Wilhelmi, O.V. Differential Adaptive Capacity to Extreme Heat: A Phoenix, Arizona, Case Study. Weather Clim. Soc. 2011, 3, 269–280. [Google Scholar] [CrossRef]
- Sampson, N.R.; Gronlund, C.J.; Buxton, M.A.; Catalano, L.; White-Newsome, J.L.; Conlon, K.C.; O’Neill, M.S.; McCormick, S.; Parker, E.A. Staying Cool in a Changing Climate: Reaching Vulnerable Populations during Heat Events. Glob. Environ. Chang. 2013, 23, 475–484. [Google Scholar] [CrossRef]
- Bradford, K.; Abrahams, L.; Hegglin, M.; Klima, K. A Heat Vulnerability Index and Adaptation Solutions for Pittsburgh, Pennsylvania. Environ. Sci. Technol. 2015, 49, 11303–11311. [Google Scholar] [CrossRef] [PubMed]
- Widerynski, S.; Schramm, P.J.; Conlon, K.C.; Noe, R.S.; Grossman, E.; Hawkins, M.; Nayak, S.U.; Roach, M.; Hilts, A.S. Use of Cooling Centers to Prevent Heat-Related Illness: Summary of Evidence and Strategies for Implementation; U.S. Centers for Disease Control and Prevention: Atlanta, GA, USA, 2017.
- Nayak, S.G.; Shrestha, S.; Sheridan, S.C.; Hsu, W.-H.; Muscatiello, N.A.; Pantea, C.I.; Ross, Z.; Kinney, P.L.; Zdeb, M.; Hwang, S.-A.A.; et al. Accessibility of Cooling Centers to Heat-Vulnerable Populations in New York State. J. Transp. Health 2019, 14, 100563. [Google Scholar] [CrossRef]
- Fraser, A.M.; Chester, M.V.; Eisenman, D.; Hondula, D.M.; Pincetl, S.S.; English, P.; Bondank, E. Household Accessibility to Heat Refuges: Residential Air Conditioning, Public Cooled Space, and Walkability. Environ. Plan. B Urban Anal. City Sci. 2017, 44, 1036–1055. [Google Scholar] [CrossRef]
- McGrail, M.R.; Humphreys, J.S. Measuring Spatial Accessibility to Primary Care in Rural Areas: Improving the Effectiveness of the Two-Step Floating Catchment Area Method. Appl. Geogr. 2009, 29, 533–541. [Google Scholar] [CrossRef]
- Horner, M.W.; Duncan, M.D.; Wood, B.S.; Valdez-Torres, Y.; Stansbury, C. Do Aging Populations Have Differential Accessibility to Activities? Analyzing the Spatial Structure of Social, Professional, and Business Opportunities. Travel Behav. Soc. 2015, 2, 182–191. [Google Scholar] [CrossRef]
- Berisha, V.; Hondula, D.; Roach, M.; White, J.R.; McKinney, B.; Bentz, D.; Mohamed, A.; Uebelherr, J.; Goodin, K. Assessing Adaptation Strategies for Extreme Heat: A Public Health Evaluation of Cooling Centers in Maricopa County, Arizona. Weather Clim. Soc. 2017, 9, 71–80. [Google Scholar] [CrossRef]
- Voelkel, J.; Hellman, D.; Sakuma, R.; Shandas, V. Assessing Vulnerability to Urban Heat: A Study of Disproportionate Heat Exposure and Access to Refuge by Socio-Demographic Status in Portland, Oregon. Int. J. Environ. Res. Public Health 2018, 15, 640. [Google Scholar] [CrossRef]
- Basu, R.; Samet, J.M. Relation between Elevated Ambient Temperature and Mortality: A Review of the Epidemiologic Evidence. Epidemiol. Rev. 2002, 24, 190–202. [Google Scholar] [CrossRef]
- Kravchenko, J.; Abernethy, A.P.; Fawzy, M.; Lyerly, H.K. Minimization of Heatwave Morbidity and Mortality. Am. J. Prev. Med. 2013, 44, 274–282. [Google Scholar] [CrossRef] [PubMed]
- McGeehin, M.A.; Mirabelli, M. The Potential Impacts of Climate Variability and Change on Temperature-Related Morbidity and Mortality in the United States. Environ. Health Perspect. 2001, 109, 185–189. [Google Scholar]
- Gao, J.; Sun, Y.; Liu, Q.; Zhou, M.; Lu, Y.; Li, L. Impact of Extreme High Temperature on Mortality and Regional Level Definition of Heat Wave: A Multi-City Study in China. Sci. Total Environ. 2015, 505, 535–544. [Google Scholar] [CrossRef]
- White, A.N. Accessibility and Public Facility Location. Econ. Geogr. 1979, 55, 18. [Google Scholar] [CrossRef]
- Ye, H.; Kim, H. Locating Healthcare Facilities Using a Network-Based Covering Location Problem. GeoJournal 2016, 81, 875–890. [Google Scholar] [CrossRef]
- Daly, C.; Halbleib, M.; Smith, J.I.; Gibson, W.P.; Doggett, M.K.; Taylor, G.H.; Curtis, J.; Pasteris, P.P. Physiographically Sensitive Mapping of Climatological Temperature and Precipitation across the Conterminous United States. Int. J. Climatol. J. R. Meteorol. Soc. 2008, 28, 2031–2064. [Google Scholar] [CrossRef]
- Steadman, R.G. The Assessment of Sultriness. Part I: A Temperature-Humidity Index Based on Human Physiology and Clothing Science. J. Appl. Meteorol. Climatol. 1979, 18, 861–873. [Google Scholar] [CrossRef]
- Boeing, G. OSMnx: New Methods for Acquiring, Constructing, Analyzing, and Visualizing Complex Street Networks. Comput. Environ. Urban Syst. 2017, 65, 126–139. [Google Scholar] [CrossRef]
- Neukart, F.; Compostella, G.; Seidel, C.; von Dollen, D.; Yarkoni, S.; Parney, B. Traffic Flow Optimization Using a Quantum Annealer. Front. ICT 2017, 4, 29. [Google Scholar] [CrossRef]
- Hofer, C.; Jäger, G.; Füllsack, M. Large Scale Simulation of CO2 Emissions Caused by Urban Car Traffic: An Agent-Based Network Approach. J. Clean. Prod. 2018, 183, 1–10. [Google Scholar] [CrossRef]
- Ren, Y.; Cheng, T.; Zhang, Y. Deep Spatio-Temporal Residual Neural Networks for Road-Network-Based Data Modeling. Int. J. Geogr. Inf. Sci. 2019, 33, 1894–1912. [Google Scholar] [CrossRef]
- U.S. Census Bureau. Understanding and Using American Community Survey Data: What All Data Users Need to Know; U.S. Government Publishing Office: Washington, DC, USA, 2020.
- Hall, D.M.; Xu, L.; Drake, V.J.; Oberley, L.W.; Oberley, T.D.; Moseley, P.L.; Kregel, K.C. Aging Reduces Adaptive Capacity and Stress Protein Expression in the Liver after Heat Stress. J. Appl. Physiol. 2000, 89, 749–759. [Google Scholar] [CrossRef]
- Hanna, E.; Tait, P. Limitations to Thermoregulation and Acclimatization Challenge Human Adaptation to Global Warming. Int. J. Environ. Res. Public Health 2015, 12, 8034–8074. [Google Scholar] [CrossRef]
- Horowitz, M.; Robinson, S.D.M. Heat shock proteins and the heat shock response during hyperthermia and its modulation by altered physiological conditions. In Progress in Brain Research; Neurobiology of Hyperthermia; Sharma, H.S., Ed.; Elsevier: Amsterdam, The Netherlands, 2007; Volume 162, pp. 433–446. [Google Scholar]
- Hansen, A.; Bi, L.; Saniotis, A.; Nitschke, M. Vulnerability to Extreme Heat and Climate Change: Is Ethnicity a Factor? Glob. Health Action 2013, 6, 21364. [Google Scholar] [CrossRef]
- Madrigano, J.; Ito, K.; Johnson, S.; Kinney, P.L.; Matte, T. A Case-Only Study of Vulnerability to Heat Wave–RelatedMortality in New York City (2000–2011). Environ. Health Perspect. 2015, 123, 672–678. [Google Scholar] [CrossRef]
- O’Neill, M.S. Modifiers of the Temperature and Mortality Association in Seven US Cities. Am. J. Epidemiol. 2003, 157, 1074–1082. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Nitschke, M.; Bi, P. Risk Factors for Direct Heat-Related Hospitalization during the 2009 Adelaide Heatwave: A Case Crossover Study. Sci. Total Environ. 2013, 442, 1–5. [Google Scholar] [CrossRef]
- O’Neill, M.S. Disparities by Race in Heat-Related Mortality in Four US Cities: The Role of Air Conditioning Prevalence. J. Urban Health Bull. N. Y. Acad. Med. 2005, 82, 191–197. [Google Scholar] [CrossRef]
- Kisner, C.; Mulder, K.; VanGessel, B. Assessing Heat Vulnerability and Access to Cooling Centers in Detroit, Michigan; University of Michigan Taubman, College of Architecture & Urban Planning: Ann Arbor, MI, USA, 2012. [Google Scholar]
- Clark, P.J.; Evans, F.C. Distance to Nearest Neighbor as a Measure of Spatial Relationships in Populations. Ecology 1954, 35, 445–453. [Google Scholar] [CrossRef]
- Curriero, F.C.; Heiner, K.S.; Samet, J.M.; Zeger, S.L.; Strug, L.; Patz, J.A. Temperature and Mortality in 11 Cities of the Eastern United States. Am. J. Epidemiol. 2002, 155, 80–87. [Google Scholar] [CrossRef]
- DeVita, P.; Hortobagyi, T. Age Causes a Redistribution of Joint Torques and Powers during Gait. J. Appl. Physiol. 2000, 88, 1804–1811. [Google Scholar] [CrossRef]
- Song, S.; Geyer, H. Predictive Neuromechanical Simulations Indicate Why Walking Performance Declines with Ageing: Computer Simulations of Elderly Gait. J. Physiol. 2018, 596, 1199–1210. [Google Scholar] [CrossRef] [PubMed]
- United Nations (UN). Transforming Our World: The 2030 Agenda for Sustainable Development; Resolution Adopted by the General Assembly on 25 September 2015; UN General Assembly: New York, NY, USA, 2015; Available online: https://sustainabledevelopment.un.org/content/documents/21252030%20Agenda%20for%20Sustainable%20Development%20web.pdf (accessed on 22 April 2021).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| City | Heat Index (°C) | Cooling Center (Count) | Total Population | Age (%) | Black (%) | Hispanic (%) | Insurance (%) | Poverty Level (%) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ≥65 | ≤64 (Ref) | Yes | No (Ref) | Yes | No (Ref) | No | Own (Ref) | Below | Above (Ref) | ||||
| Albuquerque, NM | 28.8 | 45 | 568,755 | 14.7 | 85.3 | 3.2 | 96.8 | 49.9 | 50.1 | 8.1 | 91.9 | 17.0 | 83.0 |
| Baltimore, MD | 27.8 | 11 | 609,032 | 13.6 | 86.4 | 62.4 | 37.6 | 5.3 | 94.7 | 6.6 | 93.4 | 21.2 | 78.8 |
| Chicago, IL | 25.5 | 99 | 2,712,529 | 12.4 | 87.6 | 29.5 | 70.5 | 28.8 | 71.2 | 9.7 | 90.3 | 18.4 | 81.6 |
| Columbus, OH | 27.0 | 29 | 913,582 | 10.5 | 89.5 | 28.1 | 71.9 | 6.1 | 93.9 | 8.8 | 91.2 | 19.0 | 81.0 |
| Dallas, TX | 33.4 | 45 | 1,357,894 | 10.5 | 89.5 | 23.9 | 76.1 | 41.4 | 58.6 | 23.2 | 76.8 | 18.6 | 81.4 |
| Detroit, MI | 26.0 | 24 | 674,841 | 13.6 | 86.4 | 78.3 | 21.7 | 7.7 | 92.3 | 8.4 | 91.6 | 35.0 | 65.0 |
| Fresno, CA | 31.0 | 4 | 549,961 | 11.7 | 88.3 | 7.1 | 92.9 | 49.3 | 50.7 | 8.3 | 91.7 | 25.0 | 75.0 |
| Kansas City, MO | 28.5 | 28 | 505,856 | 12.9 | 87.1 | 27.4 | 72.6 | 10.4 | 89.6 | 11.6 | 88.4 | 15.7 | 84.3 |
| Long Beach, CA | 25.9 | 5 | 469,937 | 11.5 | 88.5 | 12.6 | 87.4 | 42.6 | 57.4 | 8.5 | 91.5 | 16.7 | 83.3 |
| Louisville, KY | 28.9 | 25 | 658,837 | 15.1 | 84.9 | 23.1 | 76.9 | 5.5 | 94.5 | 5.3 | 94.7 | 15.3 | 84.7 |
| Memphis, TN | 31.4 | 18 | 677,513 | 12.6 | 87.4 | 64.0 | 36.0 | 7.0 | 93.0 | 13.7 | 86.3 | 24.5 | 75.5 |
| Mesa, AZ | 35.7 | 7 | 516,705 | 17.0 | 83.0 | 4.0 | 96.0 | 27.6 | 72.4 | 12.2 | 87.8 | 15.0 | 85.0 |
| Milwaukee, WI | 25.2 | 16 | 594,722 | 10.5 | 89.5 | 38.7 | 61.3 | 19.0 | 81.0 | 9.3 | 90.7 | 25.4 | 74.6 |
| Minneapolis, MN | 25.6 | 6 | 420,324 | 10.0 | 90.0 | 19.2 | 80.8 | 9.6 | 90.4 | 6.6 | 93.4 | 19.1 | 80.9 |
| Nashville, TN | 30.2 | 13 | 665,708 | 11.8 | 88.2 | 27.5 | 72.5 | 10.5 | 89.5 | 12.1 | 87.9 | 15.1 | 84.9 |
| Oakland, CA | 24.7 | 5 | 425,097 | 13.1 | 86.9 | 23.8 | 76.2 | 27.0 | 73.0 | 7.9 | 92.1 | 16.7 | 83.3 |
| Philadelphia, PA | 27.6 | 29 | 1,579,075 | 13.4 | 86.6 | 42.1 | 57.9 | 14.7 | 85.3 | 8.1 | 91.9 | 24.3 | 75.7 |
| Phoenix, AZ | 36.1 | 30 | 1,649,286 | 10.7 | 89.3 | 7.1 | 92.9 | 42.5 | 57.5 | 14.0 | 86.0 | 17.9 | 82.1 |
| Portland, OR | 25.4 | 27 | 655,855 | 12.9 | 87.1 | 5.8 | 94.2 | 9.9 | 90.1 | 6.5 | 93.5 | 13.7 | 86.3 |
| Riverside, CA | 29.4 | 7 | 329,396 | 10.7 | 89.3 | 6.1 | 93.9 | 54.2 | 45.8 | 9.5 | 90.5 | 13.9 | 86.1 |
| St. Louis, MO | 28.7 | 37 | 308,174 | 13.1 | 86.9 | 46.4 | 53.6 | 4.0 | 96.0 | 10.8 | 89.2 | 21.8 | 78.2 |
| San Antonio, TX | 33.7 | 25 | 1,589,745 | 11.9 | 88.1 | 7.0 | 93.0 | 63.6 | 36.4 | 16.3 | 83.7 | 17.3 | 82.7 |
| San Jose, CA | 25.9 | 5 | 1,060,954 | 12.5 | 87.5 | 3.0 | 97.0 | 31.5 | 68.5 | 5.1 | 94.9 | 8.7 | 91.3 |
| Stockton, CA | 29.3 | 5 | 329,698 | 12.5 | 87.5 | 10.6 | 89.4 | 43.8 | 56.2 | 6.9 | 93.1 | 18.0 | 82.0 |
| Washington, DC | 28.3 | 79 | 692,683 | 12.1 | 87.9 | 46.3 | 53.7 | 11.0 | 89.0 | 3.7 | 96.3 | 16.2 | 83.8 |
| Average | 28.8 | 25 | 820,646 | 12.3 | 87.7 | 25.9 | 74.1 | 24.9 | 75.1 | 9.6 | 90.4 | 18.8 | 81.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.; Jung, J.; Schollaert, C.; Spector, J.T. A Comparative Assessment of Cooling Center Preparedness across Twenty-Five U.S. Cities. Int. J. Environ. Res. Public Health 2021, 18, 4801. https://doi.org/10.3390/ijerph18094801
Kim K, Jung J, Schollaert C, Spector JT. A Comparative Assessment of Cooling Center Preparedness across Twenty-Five U.S. Cities. International Journal of Environmental Research and Public Health. 2021; 18(9):4801. https://doi.org/10.3390/ijerph18094801
Chicago/Turabian StyleKim, Kyusik, Jihoon Jung, Claire Schollaert, and June T. Spector. 2021. "A Comparative Assessment of Cooling Center Preparedness across Twenty-Five U.S. Cities" International Journal of Environmental Research and Public Health 18, no. 9: 4801. https://doi.org/10.3390/ijerph18094801
APA StyleKim, K., Jung, J., Schollaert, C., & Spector, J. T. (2021). A Comparative Assessment of Cooling Center Preparedness across Twenty-Five U.S. Cities. International Journal of Environmental Research and Public Health, 18(9), 4801. https://doi.org/10.3390/ijerph18094801